- Home
- Motor Behaviour
- Kinesiology/Exercise and Sport Science
- Biomechanics
- Structure and Function of the Musculoskeletal System

Structure and Function of the Musculoskeletal System
408 Pages
An undergraduate-level text for students in sport and exercise science, kinesiology, exercise physiology, biomechanics, or physiotherapy programs; also a reference for graduate students and professionals in the exercise science fields.
Part I. Functional Anatomy of the Musculoskeletal System
Chapter 1. The Musculoskeletal System
Unicellular and Multicellular Organisms
Cellular Organization in Multicellular Organisms
Composition and Function of the Musculoskeletal System Summary
Review Questions
Chapter 2. The Skeleton
Terminology
Axial Skeleton
Appendicular Skeleton
Summary
Review Questions
Chapter 3. Connective Tissues
Functions of Connective Tissues
Ordinary Connective Tissues
Cartilage
Bone
Summary
Review Questions
Chapter 4. The Articular System
Structural Classification of Joints
Joint Movements
Stability-Flexibility Classification of Joints
Synovial Joint Classification
Flexibility, Stability, and Laxity in Synovial Joints
Summary
Review Questions
Chapter 5. Joints of the Axial Skeleton
Joints Between the Vertebrae
Degeneration and Damage in the Vertebral Column
Normal Shape of the Vertebral Column
Abnormal Curvature of the Vertebral Column
Joints of the Pelvis
Summary
Review Questions
Chapter 6. Joints of the Appendicular Skeleton
Joints and Joint Complexes
Shoulder Complex
Elbow Complex
Wrist Complex
Hip Joint
Knee Complex
Rearfoot Complex
Summary
Review Questions
Chapter 7. The Neuromuscular System
Nervous System
Skeletal Muscle Structure
Muscle Fiber Structure and Function
Kinesthetic Sense and Proprioception
Mechanical Characteristics of Musculotendinous Units
Muscle Architecture and Function
Stretch-Shorten Cycle
Summary
Review Questions
Part II. Musculoskeletal Response and Adaptation to Loading
Chapter 8. Elementary Biomechanics
Mechanics and Biomechanics
Center of Gravity
Stability
Center of Pressure
Vector and Scalar Quantities
Moment of a Force
Levers
Summary
Review Questions
Chapter 9. Forces in Muscles and Joints
Selective Recruitment of Motor Units to Match Functional Requirements
Forces Acting on the Head in Upright Postures
Moment of External Forces Versus the Magnitude of Internal Forces
Forces About the Hip Joint in One-Leg Stance
Effect of Squat and Stoop Postures on Forces in the Lumbar Region
Swing and Stabilization Components of Muscle Force
Summary
Review Questions
Chapter 10. Mechanical Characteristics of Musculoskeletal Components
Stress - Strain Relationships in Solids
Work, Strain Energy, and Kinetic Energy
Viscosity and Viscoelasticity
Active and Passive Loading
Impact and Shock
Summary
Review Questions
Chapter 11. Structural Adaptation of the Musculoskeletal System
Adaptation
Biopositive and Bionegative Effects of Loading
Response and Adaptation of Musculoskeletal Components to Loading
Summary
Review Questions
Chapter 12. Etiology of Musculoskeletal Disorders and Injuries
Kinetic Chain
Compensatory Movements
Risk Factors for Musculoskeletal Disorders
Summary
Review Questions
James Watkins, PhD, is a professor of biomechanics in the School of Human Sciences and director of the Sport and Exercise Science Research Centre at the Swansea University in Wales. Watkins spent over 20 years in Glasgow, Scotland, as a lecturer and researcher, and he served as the head of the department of physical education, sport and outdoor education at Jordanhill College and later at the University of Strathclyde, both in Glasgow.
Watkins' main teaching and research specializations are musculoskeletal anatomy and the biomechanics of sport and exercise. He has authored over 80 publications, including three well-known textbooks (An Introduction to the Mechanics of Human Movement, 1983; this text, Structure and Function of the Musculoskeletal System; and An Introduction to Biomechanics of Sport and Exercise, 2007).
Watkins is a fellow of the British Association of Sport and Exercise Sciences (BASES), a fellow of the Physical Education Association of the United Kingdom (PEAUK), and an honorary member of the Association for Physical Education (afPE). He is an advisory board member of the Journal of Sports Sciences and a former chair of the Biomechanics Section of BASES.
In 1975 Watkins received his PhD in biomechanics from the University of Leeds in England. He resides in Swansea, where he enjoys walking, playing golf, and reading about the history of science.
Physical activity helps reduce bone loss
Bone loss begins around age 45 – 50 and moves a at different rates during different phases
Porosity, Osteopenia, and Osteoporosis
Because of the channels and spaces within compact and cancellous bone, any particular region of a bone consists of certain amounts of bone tissue and nonbone tissue. The term porosity describes the proportion of nonbone tissue. At skeletal maturity the porosity of compact and cancellous bone is approximately 2% and 50%, respectively; the density (amount of bone tissue per unit volume) of compact bone is approximately double that of cancellous bone (Radin 1984, Tortora 2004). The density of bone tissue depends on the degree of mineralization. During ossification, the degree of mineralization of bone tissue gradually increases and reaches a maximum level at skeletal maturity (Bailey et al 1986). However, the amount of bone within the skeleton may continue to increase for 5 to 10 years after skeletal maturity, especially in people who are physically active (Stillman et al 1986, Talmage and Anderson 1984, Frost 2003). Consequently, bone mass peaks in males and females between 25 and 30 years of age. In terms of turnover, this means that from skeletal maturity to the age at which peak bone mass occurs, more new bone is formed than old and damaged bone is absorbed.
Following peak bone mass there is usually a stable period in which the amount of bone in the skeleton remains about the same; there is a balance between bone absorption and bone formation. This stable period is followed by a gradual decrease in bone mass for the rest of the person's life; the rate of bone absorption exceeds the rate of bone formation. Bone mass is the product of bone volume and bone density. The loss in bone mass that occurs with age following peak bone mass is the result of decreases in bone volume and bone density. Osteopenia refers to a level of bone density below the normal level for a person's age and sex (Bailey 1995, Frost 1997).
Bone mass starts to decrease earlier and at a greater rate in females than in males. In males, bone loss normally starts between 45 and 50 years of age and proceeds at a rate of 0.4% to 0.75% per year (Bailey et al 1986, Smith 1982). In females, bone loss has three phases. The first phase starts around 30 to 35 years of age and proceeds at a rate of 0.75% to 1% per year until menopause. From menopause until about 5 years after menopause, the rate of bone loss increases to between 2% and 3% per year. During the final phase, the rate of bone loss is approximately 1% per year. Thus, women may lose, on average, about 53% of their peak bone mass by the age of 80 years. In contrast, males may lose, on average, about 18% of their peak bone mass by the age of 80 years (figure 3.32).
Even though body weight tends to decrease with age, the rate of bone loss is usually much greater than the rate at which body weight decreases. Consequently, the effect of bone loss is that the bones, especially weight-bearing bones, become progressively weaker relative to the weight of the rest of the body. In addition to gradually losing strength, the bones also gradually lose their elasticity and become more brittle. In some people, especially women, a loss of bone mass and elasticity is eventually reached when some bones are no longer able to withstand the loads imposed by normal habitual activity. These bones become very susceptible to fracture. This condition, the most common bone disorder in elderly people, is called osteoporosis (Bailey et al 1986, Ferretti et al 2003). Osteoporosis may cause severe disfigurement, especially of the trunk, as a result of fractured or crushed vertebrae. Many deaths in elderly people are due to complications arising from bone fractures that occur as a result of osteoporosis (Kaplan 1983, Kado et al 1999, Cummings and Melton 2002).
Bone loss tends to occur earlier and to proceed at a faster rate in cancellous bone than in compact bone (Bailey et al 1986, Ferretti et al 2003). Consequently, regions of bones with a high proportion of cancellous bone, such as the bodies of the vertebrae, the head and neck of the femur, and the distal end of the radius, are particularly vulnerable to osteoporosis and fracture in elderly people. This vulnerability is reflected in studies that report a rapid increase in the incidence of bone fractures with age, especially in women (Bauer 1960, Chalmers and Ho 1970, Hagino et al 1991, Cummings et al 1993, Court-Brown and Caesar 2006). The results of one study showed that the incidence of fracture to the distal end of the radius was seven times higher in 54-year-old women than in 40-year-old women (Bauer 1960). In another study the incidence of fracture of the neck of the femur was found to be 50 times higher in 70-year-old women than in 40-year-old women (Chalmers and Ho 1970). Bone loss in compact bone occurs mainly on the endosteal surface so that bone width remains relatively unchanged into old age (Smith 1982, Ferretti et al 2003).
Although the cause of osteoporosis is not clear, there is general agreement that four variables are mainly responsible: genetic factors, endocrine status, nutritional factors, and physical activity (Bailey et al 1986, MacKinnon 1988, Ferretti et al 2003). The relative contribution of these variables has not been established, but physical activity seems to be the most important. In the absence of weight-bearing activity, no amount of endocrine or nutritional intervention will prevent rapid bone loss; there must be mechanical stress (Bailey et al 1986, Ferretti et al 2003). Research suggests that regular physical activity throughout life, within the moderate overload range (see chapter 11), can help to prevent osteoporosis in three ways (Bailey 1995, Greene and Naughton 2006, Baxter-Jones et al 2008):
- Peak bone mass is directly related to the level of physical activity prior to peak bone mass; the higher the peak bone mass, the lower the risk of osteoporosis.
- An above-average level of physical activity after peak bone mass will delay the onset of bone loss.
- An above-average level of physical activity after peak bone mass will reduce the rate of bone loss.
Case study 2 discusses whether regular exercise can be used to prevent falls in osteopenic women.

Case Study 2 Using Exercise to Prevent Falls in Osteopenic Women
Hourigan SR, Nitz JC, Brauer S, O'Neill S, Wong J, Richardson CA. 2008. Positive effects of exercise on falls and fracture risk in osteopenic women. Osteoporosis International 19:1077-1086.
The incidence of bone fractures increases with age. As the number of aged people worldwide is increasing, so is the total number of fractures in the aged population (age 65 years and older). Fractures in the aged population are a major health care cost and risk factor for permanent disability and death. Consequently, reducing the risk of fractures in the aged population is a challenge in many countries.
Physical trauma (in particular, falls) and weak bones (due to osteopenia or osteoporosis) are the major causes of fractures in the aged population. Poor balance and weak muscles are risk factors for falls. Osteopenia is defined as bone mineral density (BMD) between 1 and 2.5 standard deviations below the average for young women. Osteoporosis is defined as BMD more than 2.5 standard deviations below the average for young women.
Recent research indicates that muscle strength, bone strength, and balance in the aged population can be improved through properly prescribed physical activity training programs based on resistance exercises involving strength-training machines. The purpose of the present study was to determine the effect of a physical activity program based on weight-bearing activities (rather than strength-training machines) on balance, muscle strength, and bone mineral density in osteopenic women.
Ninety-eight community-dwelling (living more or less independently in their own homes) osteopenic women (age 62.01 ± 8.9; range 41-78 years) were randomly assigned to either a control group (n = 48: no intervention) or an exercise group (n = 50: two 1 hr exercise sessions per week for 20 weeks directed by a trained physiotherapist). Assessments at baseline and post intervention included balance (five measures), strength (quadriceps; hip abductors, adductors, and external rotators; trunk extensors), and BMD (proximal femur and lumbar spine). Baseline assessment showed no significant differences between the exercise and control groups in terms of balance, strength, BMD, or demographics.
The average number of sessions attended by the 42 members of the exercise group who completed the exercise program was 28.2 of a possible 40 sessions (71.2%). Following the intervention, the exercise group showed significantly better performance than the control group in 9 of 11 balance tests (ranging from 10% to 71% better performance) and 7 of 9 strength tests (ranging from 9% to 23% better performance). BMD of the exercise group increased but was not significantly greater than in the control group.
Application
A specific, well-directed program of weight-bearing exercises in a workstation format that emphasizes interaction, discussion, and enjoyment can significantly improve balance and strength in osteopenic women, which in turn is likely to reduce the risk of falling. This type of training may also positively influence BMD, but further research is needed.
Youth sports increase risk of physeal injury
Widespread participation in youth sports increase the risk of physeal injury, resulting in more permanent problems
Case Study 1 Physeal Injuries in Youth Sports
Caine D, DiFiori J, Maffulli N. 2006. Physeal injuries in children's and youth sports: Reasons for concern? British Journal of Sports Medicine 40:749-760.
Participation in children's and youth sports is widespread in Western culture. Many children start year-round training and specialization by 9 years of age. Preteens training at regional centers or with high school and club teams in sports such as gymnastics may train more than 20 hr per week. There is increasing concern, especially among physicians, that the frequency and intensity of training and competition experienced by many participants in children's and youth sports are putting them at risk of serious physeal injury (epiphyseal and apophyseal), which may result in permanent skeletal abnormalities. Unfortunately, detailed information, based on the use of standardized recording systems applied over a long period, on the epidemiology of injuries (incidence, location, type, diagnosis, severity) sustained by participants in children's and youth sports is not available for any sport. The purpose of this study was to systematically review the literature on the frequency and characteristics of physeal injuries in children's and youth sports.
The review was undertaken using Medline and SPORTdiscus. More than 150 reports were obtained, largely case reports or case series investigations. The authors used the reports to determine the number, location, type, diagnosis, and severity of physeal injuries that occur in different sports, but it was not possible to calculate incidence of injury because information was not provided on the total number of participants and exposure time of participants in the various sports.
The review indicates that acute physeal injuries (sudden widening or fracture along or through an epiphyseal or apophyseal plate accompanied by considerable pain) and chronic physeal injuries (progressive widening of an epiphyseal or apophyseal plate associated with a progressive increase in pain, especially during exercise) occur frequently in some sports, including football, baseball, gymnastics, basketball, volleyball, judo, weightlifting, soccer, rugby, tennis, cricket, and long-distance running. The main regions of physeal injuries are the shoulder, elbow, wrist, and knee. Most of the injuries are chronic, and most resolve without complication. However, there are several reports of premature partial or complete physeal closure.
The authors express a number of concerns with current practice, in particular, the paucity of epidemiological data on the distribution and determinants of physeal injuries in children's and youth sports and the apparent lack of knowledge on the part of many coaches of children's and youth sports regarding musculoskeletal growth and development in children in general and physeal injuries in particular.
Application
Coaches should consider the following strategies to reduce the incidence of physeal injuries in children's and youth sports:
- Individualize fitness training and practice for athletes experiencing rapid growth. Assess growth rate by monitoring increases in height and limb segment lengths.
- Use a variety of training and practice drills and avoid excessive volume of training.
- For collision sports, ensure that competition is based on physical maturity rather than chronological age.
- Mandate regular medical assessment to ensure early diagnosis and treatment of epiphyseal and apophyseal plate disorders.
Structure of the knee facilitates extension and flexion
Learn more about the tibiofemoral joint and the ligaments
Capsule of the Knee
The tibiofemoral and patellofemoral joints share a common capsule that has a complicated shape. The capsule is attached above to the femur, below to the tibia, and anteriorly to the patella (figure 6.13). To accommodate the extremes of full flexion and full extension of the tibiofemoral joint, the anterior part of the capsule is folded upward during extension and the posterior part of the capsule is folded downward during flexion. The upward fold, only present in extension, is referred to as the suprapatellar bursa (figure 6.13). The suprapatellar bursa intervenes between the quadriceps tendon and the anterior aspect of the femur just proximal to the patellar surface.
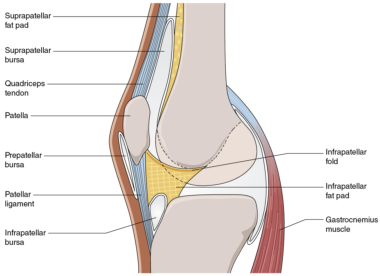
Figure 6.13 Sagittal section through the knee complex showing the shape of the capsule in extension.
The downward fold, only present during flexion, is referred to as the gastrocnemius bursa. The gastrocnemius bursa intervenes between the posterior aspect of the tibial condyles and the gastrocnemius muscle. In general, a bursa is a flattened sac of synovial membrane containing synovial fluid. Bursas minimize friction between structures that slide across each other during normal movement (see chapter 7).
During flexion of the tibiofemoral joint, the suprapatellar bursa becomes progressively smaller and the gastrocnemius bursa becomes progressively larger as synovial fluid is redistributed from the suprapatellar bursa to the gastrocnemius bursa. The movement of synovial fluid is reversed during extension of the tibiofemoral joint; that is, the gastrocnemius bursa becomes progressively smaller and the suprapatellar bursa becomes progressively larger.
The suprapatellar bursa is separated from the femur by a pad of fat called the suprapatellar fat pad. Lying in the space bounded by the upper two thirds of the posterior aspect of the patellar ligament, the anterior intercondylar area of the tibia, and the anterior inferior aspect of the articular surface of the femoral condyles is a pad of fat called the infrapatellar fat pad. It is roughly triangular in sagittal cross section and is suspended superiorly from a fibro-adipose band called the infrapatellar fold. The infrapatellar fold is attached anteriorly to the inferior pole of the patella and posteriorly to the anterior border of the intercondylar notch (figure 6.13). The infrapatellar fat pad is attached anteriorly to the posterior aspect of the patellar ligament and extends at both sides of the patellar ligament. The infrapatellar fat pad also extends narrow branches halfway up each side of the patella; the branches are referred to as alar folds (alar = winglike). The infrapatellar fat pad cushions the patellar ligament and lower part of the patella during movements of the knee.
Knee Ligaments
Four extracapsular ligaments support the tibiofemoral joint. The lateral ligament (also referred to as the lateral collateral ligament and the fibular collateral ligament) is attached superiorly to the lateral epicondyle of the femur and inferiorly to the head of the fibula (figure 6.14a). The medial ligament (also referred to as the medial collateral ligament and the tibial collateral ligament) is attached superiorly to the medial epicondyle of the femur and inferiorly to the medial aspect of the tibia below the tibial condyle (figure 6.14b). The posterior fibers of the medial ligament blend with the joint capsule at the level of the medial meniscus and thus the medial ligament is not completely extracapsular. The arrangement of the medial and lateral ligaments and the curvature of the femoral condyles are such that both ligaments are relatively slack when the knee is flexed but become progressively more taut as the joint extends. In a normal joint the ligaments are fully taut when the joint is fully extended. In this position of the joint both ligaments help to prevent hyperextension and lateral rotation of the tibia relative to the femur. With the knee fully extended, the range of abduction and adduction is normally zero. Because the medial and lateral ligaments are relatively slack when the knee is flexed, a certain amount of axial rotation and abduction and adduction of the lower leg can occur when the knee is in a flexed, non-weight-bearing position. For example, when a person is sitting on a table with his lower leg hanging freely, the ranges of internal and external rotation are normally around 30° and 40°, respectively (Norkin and Levangie 1992). However, the ranges of abduction and adduction are normally very small, approximately 2° to 5°.
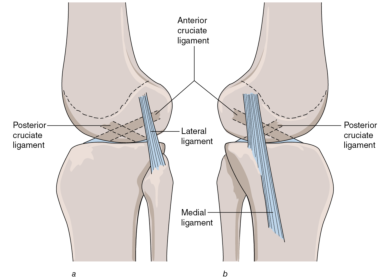
Figure 6.14 Location of the main ligaments of the left knee. (a) Lateral aspect. (b) Medial aspect.
Injuries to the lateral and, in particular, the medial ligaments are common in sports (Reider 1996). The classic cause of medial ligament injury is a blow to the lateral aspect of the knee while the foot in contact with the ground, resulting in abduction of the knee. This situation is common in sports such as American football, soccer, and rugby. The excessive loading on the medial ligament in such situations can result in serious injury (Indelicato 1995). Medial ligament injuries of a less severe but nonetheless persistent nature are common in swimmers, especially breaststroke swimmers. The whip-kick leg action in breaststroke tends to simultaneously abduct and laterally rotate (tibia with respect to femur) the knee, resulting in strain of the medial ligament and associated medial supporting structures (Vizsolyi et al 1987).
Physical activity helps reduce bone loss
Bone loss begins around age 45 – 50 and moves a at different rates during different phases
Porosity, Osteopenia, and Osteoporosis
Because of the channels and spaces within compact and cancellous bone, any particular region of a bone consists of certain amounts of bone tissue and nonbone tissue. The term porosity describes the proportion of nonbone tissue. At skeletal maturity the porosity of compact and cancellous bone is approximately 2% and 50%, respectively; the density (amount of bone tissue per unit volume) of compact bone is approximately double that of cancellous bone (Radin 1984, Tortora 2004). The density of bone tissue depends on the degree of mineralization. During ossification, the degree of mineralization of bone tissue gradually increases and reaches a maximum level at skeletal maturity (Bailey et al 1986). However, the amount of bone within the skeleton may continue to increase for 5 to 10 years after skeletal maturity, especially in people who are physically active (Stillman et al 1986, Talmage and Anderson 1984, Frost 2003). Consequently, bone mass peaks in males and females between 25 and 30 years of age. In terms of turnover, this means that from skeletal maturity to the age at which peak bone mass occurs, more new bone is formed than old and damaged bone is absorbed.
Following peak bone mass there is usually a stable period in which the amount of bone in the skeleton remains about the same; there is a balance between bone absorption and bone formation. This stable period is followed by a gradual decrease in bone mass for the rest of the person's life; the rate of bone absorption exceeds the rate of bone formation. Bone mass is the product of bone volume and bone density. The loss in bone mass that occurs with age following peak bone mass is the result of decreases in bone volume and bone density. Osteopenia refers to a level of bone density below the normal level for a person's age and sex (Bailey 1995, Frost 1997).
Bone mass starts to decrease earlier and at a greater rate in females than in males. In males, bone loss normally starts between 45 and 50 years of age and proceeds at a rate of 0.4% to 0.75% per year (Bailey et al 1986, Smith 1982). In females, bone loss has three phases. The first phase starts around 30 to 35 years of age and proceeds at a rate of 0.75% to 1% per year until menopause. From menopause until about 5 years after menopause, the rate of bone loss increases to between 2% and 3% per year. During the final phase, the rate of bone loss is approximately 1% per year. Thus, women may lose, on average, about 53% of their peak bone mass by the age of 80 years. In contrast, males may lose, on average, about 18% of their peak bone mass by the age of 80 years (figure 3.32).
Even though body weight tends to decrease with age, the rate of bone loss is usually much greater than the rate at which body weight decreases. Consequently, the effect of bone loss is that the bones, especially weight-bearing bones, become progressively weaker relative to the weight of the rest of the body. In addition to gradually losing strength, the bones also gradually lose their elasticity and become more brittle. In some people, especially women, a loss of bone mass and elasticity is eventually reached when some bones are no longer able to withstand the loads imposed by normal habitual activity. These bones become very susceptible to fracture. This condition, the most common bone disorder in elderly people, is called osteoporosis (Bailey et al 1986, Ferretti et al 2003). Osteoporosis may cause severe disfigurement, especially of the trunk, as a result of fractured or crushed vertebrae. Many deaths in elderly people are due to complications arising from bone fractures that occur as a result of osteoporosis (Kaplan 1983, Kado et al 1999, Cummings and Melton 2002).
Bone loss tends to occur earlier and to proceed at a faster rate in cancellous bone than in compact bone (Bailey et al 1986, Ferretti et al 2003). Consequently, regions of bones with a high proportion of cancellous bone, such as the bodies of the vertebrae, the head and neck of the femur, and the distal end of the radius, are particularly vulnerable to osteoporosis and fracture in elderly people. This vulnerability is reflected in studies that report a rapid increase in the incidence of bone fractures with age, especially in women (Bauer 1960, Chalmers and Ho 1970, Hagino et al 1991, Cummings et al 1993, Court-Brown and Caesar 2006). The results of one study showed that the incidence of fracture to the distal end of the radius was seven times higher in 54-year-old women than in 40-year-old women (Bauer 1960). In another study the incidence of fracture of the neck of the femur was found to be 50 times higher in 70-year-old women than in 40-year-old women (Chalmers and Ho 1970). Bone loss in compact bone occurs mainly on the endosteal surface so that bone width remains relatively unchanged into old age (Smith 1982, Ferretti et al 2003).
Although the cause of osteoporosis is not clear, there is general agreement that four variables are mainly responsible: genetic factors, endocrine status, nutritional factors, and physical activity (Bailey et al 1986, MacKinnon 1988, Ferretti et al 2003). The relative contribution of these variables has not been established, but physical activity seems to be the most important. In the absence of weight-bearing activity, no amount of endocrine or nutritional intervention will prevent rapid bone loss; there must be mechanical stress (Bailey et al 1986, Ferretti et al 2003). Research suggests that regular physical activity throughout life, within the moderate overload range (see chapter 11), can help to prevent osteoporosis in three ways (Bailey 1995, Greene and Naughton 2006, Baxter-Jones et al 2008):
- Peak bone mass is directly related to the level of physical activity prior to peak bone mass; the higher the peak bone mass, the lower the risk of osteoporosis.
- An above-average level of physical activity after peak bone mass will delay the onset of bone loss.
- An above-average level of physical activity after peak bone mass will reduce the rate of bone loss.
Case study 2 discusses whether regular exercise can be used to prevent falls in osteopenic women.
Case Study 2 Using Exercise to Prevent Falls in Osteopenic Women
Hourigan SR, Nitz JC, Brauer S, O'Neill S, Wong J, Richardson CA. 2008. Positive effects of exercise on falls and fracture risk in osteopenic women. Osteoporosis International 19:1077-1086.
The incidence of bone fractures increases with age. As the number of aged people worldwide is increasing, so is the total number of fractures in the aged population (age 65 years and older). Fractures in the aged population are a major health care cost and risk factor for permanent disability and death. Consequently, reducing the risk of fractures in the aged population is a challenge in many countries.
Physical trauma (in particular, falls) and weak bones (due to osteopenia or osteoporosis) are the major causes of fractures in the aged population. Poor balance and weak muscles are risk factors for falls. Osteopenia is defined as bone mineral density (BMD) between 1 and 2.5 standard deviations below the average for young women. Osteoporosis is defined as BMD more than 2.5 standard deviations below the average for young women.
Recent research indicates that muscle strength, bone strength, and balance in the aged population can be improved through properly prescribed physical activity training programs based on resistance exercises involving strength-training machines. The purpose of the present study was to determine the effect of a physical activity program based on weight-bearing activities (rather than strength-training machines) on balance, muscle strength, and bone mineral density in osteopenic women.
Ninety-eight community-dwelling (living more or less independently in their own homes) osteopenic women (age 62.01 ± 8.9; range 41-78 years) were randomly assigned to either a control group (n = 48: no intervention) or an exercise group (n = 50: two 1 hr exercise sessions per week for 20 weeks directed by a trained physiotherapist). Assessments at baseline and post intervention included balance (five measures), strength (quadriceps; hip abductors, adductors, and external rotators; trunk extensors), and BMD (proximal femur and lumbar spine). Baseline assessment showed no significant differences between the exercise and control groups in terms of balance, strength, BMD, or demographics.
The average number of sessions attended by the 42 members of the exercise group who completed the exercise program was 28.2 of a possible 40 sessions (71.2%). Following the intervention, the exercise group showed significantly better performance than the control group in 9 of 11 balance tests (ranging from 10% to 71% better performance) and 7 of 9 strength tests (ranging from 9% to 23% better performance). BMD of the exercise group increased but was not significantly greater than in the control group.
Application
A specific, well-directed program of weight-bearing exercises in a workstation format that emphasizes interaction, discussion, and enjoyment can significantly improve balance and strength in osteopenic women, which in turn is likely to reduce the risk of falling. This type of training may also positively influence BMD, but further research is needed.
Youth sports increase risk of physeal injury
Widespread participation in youth sports increase the risk of physeal injury, resulting in more permanent problems
Case Study 1 Physeal Injuries in Youth Sports
Caine D, DiFiori J, Maffulli N. 2006. Physeal injuries in children's and youth sports: Reasons for concern? British Journal of Sports Medicine 40:749-760.
Participation in children's and youth sports is widespread in Western culture. Many children start year-round training and specialization by 9 years of age. Preteens training at regional centers or with high school and club teams in sports such as gymnastics may train more than 20 hr per week. There is increasing concern, especially among physicians, that the frequency and intensity of training and competition experienced by many participants in children's and youth sports are putting them at risk of serious physeal injury (epiphyseal and apophyseal), which may result in permanent skeletal abnormalities. Unfortunately, detailed information, based on the use of standardized recording systems applied over a long period, on the epidemiology of injuries (incidence, location, type, diagnosis, severity) sustained by participants in children's and youth sports is not available for any sport. The purpose of this study was to systematically review the literature on the frequency and characteristics of physeal injuries in children's and youth sports.
The review was undertaken using Medline and SPORTdiscus. More than 150 reports were obtained, largely case reports or case series investigations. The authors used the reports to determine the number, location, type, diagnosis, and severity of physeal injuries that occur in different sports, but it was not possible to calculate incidence of injury because information was not provided on the total number of participants and exposure time of participants in the various sports.
The review indicates that acute physeal injuries (sudden widening or fracture along or through an epiphyseal or apophyseal plate accompanied by considerable pain) and chronic physeal injuries (progressive widening of an epiphyseal or apophyseal plate associated with a progressive increase in pain, especially during exercise) occur frequently in some sports, including football, baseball, gymnastics, basketball, volleyball, judo, weightlifting, soccer, rugby, tennis, cricket, and long-distance running. The main regions of physeal injuries are the shoulder, elbow, wrist, and knee. Most of the injuries are chronic, and most resolve without complication. However, there are several reports of premature partial or complete physeal closure.
The authors express a number of concerns with current practice, in particular, the paucity of epidemiological data on the distribution and determinants of physeal injuries in children's and youth sports and the apparent lack of knowledge on the part of many coaches of children's and youth sports regarding musculoskeletal growth and development in children in general and physeal injuries in particular.
Application
Coaches should consider the following strategies to reduce the incidence of physeal injuries in children's and youth sports:
- Individualize fitness training and practice for athletes experiencing rapid growth. Assess growth rate by monitoring increases in height and limb segment lengths.
- Use a variety of training and practice drills and avoid excessive volume of training.
- For collision sports, ensure that competition is based on physical maturity rather than chronological age.
- Mandate regular medical assessment to ensure early diagnosis and treatment of epiphyseal and apophyseal plate disorders.
Structure of the knee facilitates extension and flexion
Learn more about the tibiofemoral joint and the ligaments
Capsule of the Knee
The tibiofemoral and patellofemoral joints share a common capsule that has a complicated shape. The capsule is attached above to the femur, below to the tibia, and anteriorly to the patella (figure 6.13). To accommodate the extremes of full flexion and full extension of the tibiofemoral joint, the anterior part of the capsule is folded upward during extension and the posterior part of the capsule is folded downward during flexion. The upward fold, only present in extension, is referred to as the suprapatellar bursa (figure 6.13). The suprapatellar bursa intervenes between the quadriceps tendon and the anterior aspect of the femur just proximal to the patellar surface.
Figure 6.13 Sagittal section through the knee complex showing the shape of the capsule in extension.
The downward fold, only present during flexion, is referred to as the gastrocnemius bursa. The gastrocnemius bursa intervenes between the posterior aspect of the tibial condyles and the gastrocnemius muscle. In general, a bursa is a flattened sac of synovial membrane containing synovial fluid. Bursas minimize friction between structures that slide across each other during normal movement (see chapter 7).
During flexion of the tibiofemoral joint, the suprapatellar bursa becomes progressively smaller and the gastrocnemius bursa becomes progressively larger as synovial fluid is redistributed from the suprapatellar bursa to the gastrocnemius bursa. The movement of synovial fluid is reversed during extension of the tibiofemoral joint; that is, the gastrocnemius bursa becomes progressively smaller and the suprapatellar bursa becomes progressively larger.
The suprapatellar bursa is separated from the femur by a pad of fat called the suprapatellar fat pad. Lying in the space bounded by the upper two thirds of the posterior aspect of the patellar ligament, the anterior intercondylar area of the tibia, and the anterior inferior aspect of the articular surface of the femoral condyles is a pad of fat called the infrapatellar fat pad. It is roughly triangular in sagittal cross section and is suspended superiorly from a fibro-adipose band called the infrapatellar fold. The infrapatellar fold is attached anteriorly to the inferior pole of the patella and posteriorly to the anterior border of the intercondylar notch (figure 6.13). The infrapatellar fat pad is attached anteriorly to the posterior aspect of the patellar ligament and extends at both sides of the patellar ligament. The infrapatellar fat pad also extends narrow branches halfway up each side of the patella; the branches are referred to as alar folds (alar = winglike). The infrapatellar fat pad cushions the patellar ligament and lower part of the patella during movements of the knee.
Knee Ligaments
Four extracapsular ligaments support the tibiofemoral joint. The lateral ligament (also referred to as the lateral collateral ligament and the fibular collateral ligament) is attached superiorly to the lateral epicondyle of the femur and inferiorly to the head of the fibula (figure 6.14a). The medial ligament (also referred to as the medial collateral ligament and the tibial collateral ligament) is attached superiorly to the medial epicondyle of the femur and inferiorly to the medial aspect of the tibia below the tibial condyle (figure 6.14b). The posterior fibers of the medial ligament blend with the joint capsule at the level of the medial meniscus and thus the medial ligament is not completely extracapsular. The arrangement of the medial and lateral ligaments and the curvature of the femoral condyles are such that both ligaments are relatively slack when the knee is flexed but become progressively more taut as the joint extends. In a normal joint the ligaments are fully taut when the joint is fully extended. In this position of the joint both ligaments help to prevent hyperextension and lateral rotation of the tibia relative to the femur. With the knee fully extended, the range of abduction and adduction is normally zero. Because the medial and lateral ligaments are relatively slack when the knee is flexed, a certain amount of axial rotation and abduction and adduction of the lower leg can occur when the knee is in a flexed, non-weight-bearing position. For example, when a person is sitting on a table with his lower leg hanging freely, the ranges of internal and external rotation are normally around 30° and 40°, respectively (Norkin and Levangie 1992). However, the ranges of abduction and adduction are normally very small, approximately 2° to 5°.
Figure 6.14 Location of the main ligaments of the left knee. (a) Lateral aspect. (b) Medial aspect.
Injuries to the lateral and, in particular, the medial ligaments are common in sports (Reider 1996). The classic cause of medial ligament injury is a blow to the lateral aspect of the knee while the foot in contact with the ground, resulting in abduction of the knee. This situation is common in sports such as American football, soccer, and rugby. The excessive loading on the medial ligament in such situations can result in serious injury (Indelicato 1995). Medial ligament injuries of a less severe but nonetheless persistent nature are common in swimmers, especially breaststroke swimmers. The whip-kick leg action in breaststroke tends to simultaneously abduct and laterally rotate (tibia with respect to femur) the knee, resulting in strain of the medial ligament and associated medial supporting structures (Vizsolyi et al 1987).
Physical activity helps reduce bone loss
Bone loss begins around age 45 – 50 and moves a at different rates during different phases
Porosity, Osteopenia, and Osteoporosis
Because of the channels and spaces within compact and cancellous bone, any particular region of a bone consists of certain amounts of bone tissue and nonbone tissue. The term porosity describes the proportion of nonbone tissue. At skeletal maturity the porosity of compact and cancellous bone is approximately 2% and 50%, respectively; the density (amount of bone tissue per unit volume) of compact bone is approximately double that of cancellous bone (Radin 1984, Tortora 2004). The density of bone tissue depends on the degree of mineralization. During ossification, the degree of mineralization of bone tissue gradually increases and reaches a maximum level at skeletal maturity (Bailey et al 1986). However, the amount of bone within the skeleton may continue to increase for 5 to 10 years after skeletal maturity, especially in people who are physically active (Stillman et al 1986, Talmage and Anderson 1984, Frost 2003). Consequently, bone mass peaks in males and females between 25 and 30 years of age. In terms of turnover, this means that from skeletal maturity to the age at which peak bone mass occurs, more new bone is formed than old and damaged bone is absorbed.
Following peak bone mass there is usually a stable period in which the amount of bone in the skeleton remains about the same; there is a balance between bone absorption and bone formation. This stable period is followed by a gradual decrease in bone mass for the rest of the person's life; the rate of bone absorption exceeds the rate of bone formation. Bone mass is the product of bone volume and bone density. The loss in bone mass that occurs with age following peak bone mass is the result of decreases in bone volume and bone density. Osteopenia refers to a level of bone density below the normal level for a person's age and sex (Bailey 1995, Frost 1997).
Bone mass starts to decrease earlier and at a greater rate in females than in males. In males, bone loss normally starts between 45 and 50 years of age and proceeds at a rate of 0.4% to 0.75% per year (Bailey et al 1986, Smith 1982). In females, bone loss has three phases. The first phase starts around 30 to 35 years of age and proceeds at a rate of 0.75% to 1% per year until menopause. From menopause until about 5 years after menopause, the rate of bone loss increases to between 2% and 3% per year. During the final phase, the rate of bone loss is approximately 1% per year. Thus, women may lose, on average, about 53% of their peak bone mass by the age of 80 years. In contrast, males may lose, on average, about 18% of their peak bone mass by the age of 80 years (figure 3.32).
Even though body weight tends to decrease with age, the rate of bone loss is usually much greater than the rate at which body weight decreases. Consequently, the effect of bone loss is that the bones, especially weight-bearing bones, become progressively weaker relative to the weight of the rest of the body. In addition to gradually losing strength, the bones also gradually lose their elasticity and become more brittle. In some people, especially women, a loss of bone mass and elasticity is eventually reached when some bones are no longer able to withstand the loads imposed by normal habitual activity. These bones become very susceptible to fracture. This condition, the most common bone disorder in elderly people, is called osteoporosis (Bailey et al 1986, Ferretti et al 2003). Osteoporosis may cause severe disfigurement, especially of the trunk, as a result of fractured or crushed vertebrae. Many deaths in elderly people are due to complications arising from bone fractures that occur as a result of osteoporosis (Kaplan 1983, Kado et al 1999, Cummings and Melton 2002).
Bone loss tends to occur earlier and to proceed at a faster rate in cancellous bone than in compact bone (Bailey et al 1986, Ferretti et al 2003). Consequently, regions of bones with a high proportion of cancellous bone, such as the bodies of the vertebrae, the head and neck of the femur, and the distal end of the radius, are particularly vulnerable to osteoporosis and fracture in elderly people. This vulnerability is reflected in studies that report a rapid increase in the incidence of bone fractures with age, especially in women (Bauer 1960, Chalmers and Ho 1970, Hagino et al 1991, Cummings et al 1993, Court-Brown and Caesar 2006). The results of one study showed that the incidence of fracture to the distal end of the radius was seven times higher in 54-year-old women than in 40-year-old women (Bauer 1960). In another study the incidence of fracture of the neck of the femur was found to be 50 times higher in 70-year-old women than in 40-year-old women (Chalmers and Ho 1970). Bone loss in compact bone occurs mainly on the endosteal surface so that bone width remains relatively unchanged into old age (Smith 1982, Ferretti et al 2003).
Although the cause of osteoporosis is not clear, there is general agreement that four variables are mainly responsible: genetic factors, endocrine status, nutritional factors, and physical activity (Bailey et al 1986, MacKinnon 1988, Ferretti et al 2003). The relative contribution of these variables has not been established, but physical activity seems to be the most important. In the absence of weight-bearing activity, no amount of endocrine or nutritional intervention will prevent rapid bone loss; there must be mechanical stress (Bailey et al 1986, Ferretti et al 2003). Research suggests that regular physical activity throughout life, within the moderate overload range (see chapter 11), can help to prevent osteoporosis in three ways (Bailey 1995, Greene and Naughton 2006, Baxter-Jones et al 2008):
- Peak bone mass is directly related to the level of physical activity prior to peak bone mass; the higher the peak bone mass, the lower the risk of osteoporosis.
- An above-average level of physical activity after peak bone mass will delay the onset of bone loss.
- An above-average level of physical activity after peak bone mass will reduce the rate of bone loss.
Case study 2 discusses whether regular exercise can be used to prevent falls in osteopenic women.
Case Study 2 Using Exercise to Prevent Falls in Osteopenic Women
Hourigan SR, Nitz JC, Brauer S, O'Neill S, Wong J, Richardson CA. 2008. Positive effects of exercise on falls and fracture risk in osteopenic women. Osteoporosis International 19:1077-1086.
The incidence of bone fractures increases with age. As the number of aged people worldwide is increasing, so is the total number of fractures in the aged population (age 65 years and older). Fractures in the aged population are a major health care cost and risk factor for permanent disability and death. Consequently, reducing the risk of fractures in the aged population is a challenge in many countries.
Physical trauma (in particular, falls) and weak bones (due to osteopenia or osteoporosis) are the major causes of fractures in the aged population. Poor balance and weak muscles are risk factors for falls. Osteopenia is defined as bone mineral density (BMD) between 1 and 2.5 standard deviations below the average for young women. Osteoporosis is defined as BMD more than 2.5 standard deviations below the average for young women.
Recent research indicates that muscle strength, bone strength, and balance in the aged population can be improved through properly prescribed physical activity training programs based on resistance exercises involving strength-training machines. The purpose of the present study was to determine the effect of a physical activity program based on weight-bearing activities (rather than strength-training machines) on balance, muscle strength, and bone mineral density in osteopenic women.
Ninety-eight community-dwelling (living more or less independently in their own homes) osteopenic women (age 62.01 ± 8.9; range 41-78 years) were randomly assigned to either a control group (n = 48: no intervention) or an exercise group (n = 50: two 1 hr exercise sessions per week for 20 weeks directed by a trained physiotherapist). Assessments at baseline and post intervention included balance (five measures), strength (quadriceps; hip abductors, adductors, and external rotators; trunk extensors), and BMD (proximal femur and lumbar spine). Baseline assessment showed no significant differences between the exercise and control groups in terms of balance, strength, BMD, or demographics.
The average number of sessions attended by the 42 members of the exercise group who completed the exercise program was 28.2 of a possible 40 sessions (71.2%). Following the intervention, the exercise group showed significantly better performance than the control group in 9 of 11 balance tests (ranging from 10% to 71% better performance) and 7 of 9 strength tests (ranging from 9% to 23% better performance). BMD of the exercise group increased but was not significantly greater than in the control group.
Application
A specific, well-directed program of weight-bearing exercises in a workstation format that emphasizes interaction, discussion, and enjoyment can significantly improve balance and strength in osteopenic women, which in turn is likely to reduce the risk of falling. This type of training may also positively influence BMD, but further research is needed.
Youth sports increase risk of physeal injury
Widespread participation in youth sports increase the risk of physeal injury, resulting in more permanent problems
Case Study 1 Physeal Injuries in Youth Sports
Caine D, DiFiori J, Maffulli N. 2006. Physeal injuries in children's and youth sports: Reasons for concern? British Journal of Sports Medicine 40:749-760.
Participation in children's and youth sports is widespread in Western culture. Many children start year-round training and specialization by 9 years of age. Preteens training at regional centers or with high school and club teams in sports such as gymnastics may train more than 20 hr per week. There is increasing concern, especially among physicians, that the frequency and intensity of training and competition experienced by many participants in children's and youth sports are putting them at risk of serious physeal injury (epiphyseal and apophyseal), which may result in permanent skeletal abnormalities. Unfortunately, detailed information, based on the use of standardized recording systems applied over a long period, on the epidemiology of injuries (incidence, location, type, diagnosis, severity) sustained by participants in children's and youth sports is not available for any sport. The purpose of this study was to systematically review the literature on the frequency and characteristics of physeal injuries in children's and youth sports.
The review was undertaken using Medline and SPORTdiscus. More than 150 reports were obtained, largely case reports or case series investigations. The authors used the reports to determine the number, location, type, diagnosis, and severity of physeal injuries that occur in different sports, but it was not possible to calculate incidence of injury because information was not provided on the total number of participants and exposure time of participants in the various sports.
The review indicates that acute physeal injuries (sudden widening or fracture along or through an epiphyseal or apophyseal plate accompanied by considerable pain) and chronic physeal injuries (progressive widening of an epiphyseal or apophyseal plate associated with a progressive increase in pain, especially during exercise) occur frequently in some sports, including football, baseball, gymnastics, basketball, volleyball, judo, weightlifting, soccer, rugby, tennis, cricket, and long-distance running. The main regions of physeal injuries are the shoulder, elbow, wrist, and knee. Most of the injuries are chronic, and most resolve without complication. However, there are several reports of premature partial or complete physeal closure.
The authors express a number of concerns with current practice, in particular, the paucity of epidemiological data on the distribution and determinants of physeal injuries in children's and youth sports and the apparent lack of knowledge on the part of many coaches of children's and youth sports regarding musculoskeletal growth and development in children in general and physeal injuries in particular.
Application
Coaches should consider the following strategies to reduce the incidence of physeal injuries in children's and youth sports:
- Individualize fitness training and practice for athletes experiencing rapid growth. Assess growth rate by monitoring increases in height and limb segment lengths.
- Use a variety of training and practice drills and avoid excessive volume of training.
- For collision sports, ensure that competition is based on physical maturity rather than chronological age.
- Mandate regular medical assessment to ensure early diagnosis and treatment of epiphyseal and apophyseal plate disorders.
Structure of the knee facilitates extension and flexion
Learn more about the tibiofemoral joint and the ligaments
Capsule of the Knee
The tibiofemoral and patellofemoral joints share a common capsule that has a complicated shape. The capsule is attached above to the femur, below to the tibia, and anteriorly to the patella (figure 6.13). To accommodate the extremes of full flexion and full extension of the tibiofemoral joint, the anterior part of the capsule is folded upward during extension and the posterior part of the capsule is folded downward during flexion. The upward fold, only present in extension, is referred to as the suprapatellar bursa (figure 6.13). The suprapatellar bursa intervenes between the quadriceps tendon and the anterior aspect of the femur just proximal to the patellar surface.
Figure 6.13 Sagittal section through the knee complex showing the shape of the capsule in extension.
The downward fold, only present during flexion, is referred to as the gastrocnemius bursa. The gastrocnemius bursa intervenes between the posterior aspect of the tibial condyles and the gastrocnemius muscle. In general, a bursa is a flattened sac of synovial membrane containing synovial fluid. Bursas minimize friction between structures that slide across each other during normal movement (see chapter 7).
During flexion of the tibiofemoral joint, the suprapatellar bursa becomes progressively smaller and the gastrocnemius bursa becomes progressively larger as synovial fluid is redistributed from the suprapatellar bursa to the gastrocnemius bursa. The movement of synovial fluid is reversed during extension of the tibiofemoral joint; that is, the gastrocnemius bursa becomes progressively smaller and the suprapatellar bursa becomes progressively larger.
The suprapatellar bursa is separated from the femur by a pad of fat called the suprapatellar fat pad. Lying in the space bounded by the upper two thirds of the posterior aspect of the patellar ligament, the anterior intercondylar area of the tibia, and the anterior inferior aspect of the articular surface of the femoral condyles is a pad of fat called the infrapatellar fat pad. It is roughly triangular in sagittal cross section and is suspended superiorly from a fibro-adipose band called the infrapatellar fold. The infrapatellar fold is attached anteriorly to the inferior pole of the patella and posteriorly to the anterior border of the intercondylar notch (figure 6.13). The infrapatellar fat pad is attached anteriorly to the posterior aspect of the patellar ligament and extends at both sides of the patellar ligament. The infrapatellar fat pad also extends narrow branches halfway up each side of the patella; the branches are referred to as alar folds (alar = winglike). The infrapatellar fat pad cushions the patellar ligament and lower part of the patella during movements of the knee.
Knee Ligaments
Four extracapsular ligaments support the tibiofemoral joint. The lateral ligament (also referred to as the lateral collateral ligament and the fibular collateral ligament) is attached superiorly to the lateral epicondyle of the femur and inferiorly to the head of the fibula (figure 6.14a). The medial ligament (also referred to as the medial collateral ligament and the tibial collateral ligament) is attached superiorly to the medial epicondyle of the femur and inferiorly to the medial aspect of the tibia below the tibial condyle (figure 6.14b). The posterior fibers of the medial ligament blend with the joint capsule at the level of the medial meniscus and thus the medial ligament is not completely extracapsular. The arrangement of the medial and lateral ligaments and the curvature of the femoral condyles are such that both ligaments are relatively slack when the knee is flexed but become progressively more taut as the joint extends. In a normal joint the ligaments are fully taut when the joint is fully extended. In this position of the joint both ligaments help to prevent hyperextension and lateral rotation of the tibia relative to the femur. With the knee fully extended, the range of abduction and adduction is normally zero. Because the medial and lateral ligaments are relatively slack when the knee is flexed, a certain amount of axial rotation and abduction and adduction of the lower leg can occur when the knee is in a flexed, non-weight-bearing position. For example, when a person is sitting on a table with his lower leg hanging freely, the ranges of internal and external rotation are normally around 30° and 40°, respectively (Norkin and Levangie 1992). However, the ranges of abduction and adduction are normally very small, approximately 2° to 5°.
Figure 6.14 Location of the main ligaments of the left knee. (a) Lateral aspect. (b) Medial aspect.
Injuries to the lateral and, in particular, the medial ligaments are common in sports (Reider 1996). The classic cause of medial ligament injury is a blow to the lateral aspect of the knee while the foot in contact with the ground, resulting in abduction of the knee. This situation is common in sports such as American football, soccer, and rugby. The excessive loading on the medial ligament in such situations can result in serious injury (Indelicato 1995). Medial ligament injuries of a less severe but nonetheless persistent nature are common in swimmers, especially breaststroke swimmers. The whip-kick leg action in breaststroke tends to simultaneously abduct and laterally rotate (tibia with respect to femur) the knee, resulting in strain of the medial ligament and associated medial supporting structures (Vizsolyi et al 1987).
Physical activity helps reduce bone loss
Bone loss begins around age 45 – 50 and moves a at different rates during different phases
Porosity, Osteopenia, and Osteoporosis
Because of the channels and spaces within compact and cancellous bone, any particular region of a bone consists of certain amounts of bone tissue and nonbone tissue. The term porosity describes the proportion of nonbone tissue. At skeletal maturity the porosity of compact and cancellous bone is approximately 2% and 50%, respectively; the density (amount of bone tissue per unit volume) of compact bone is approximately double that of cancellous bone (Radin 1984, Tortora 2004). The density of bone tissue depends on the degree of mineralization. During ossification, the degree of mineralization of bone tissue gradually increases and reaches a maximum level at skeletal maturity (Bailey et al 1986). However, the amount of bone within the skeleton may continue to increase for 5 to 10 years after skeletal maturity, especially in people who are physically active (Stillman et al 1986, Talmage and Anderson 1984, Frost 2003). Consequently, bone mass peaks in males and females between 25 and 30 years of age. In terms of turnover, this means that from skeletal maturity to the age at which peak bone mass occurs, more new bone is formed than old and damaged bone is absorbed.
Following peak bone mass there is usually a stable period in which the amount of bone in the skeleton remains about the same; there is a balance between bone absorption and bone formation. This stable period is followed by a gradual decrease in bone mass for the rest of the person's life; the rate of bone absorption exceeds the rate of bone formation. Bone mass is the product of bone volume and bone density. The loss in bone mass that occurs with age following peak bone mass is the result of decreases in bone volume and bone density. Osteopenia refers to a level of bone density below the normal level for a person's age and sex (Bailey 1995, Frost 1997).
Bone mass starts to decrease earlier and at a greater rate in females than in males. In males, bone loss normally starts between 45 and 50 years of age and proceeds at a rate of 0.4% to 0.75% per year (Bailey et al 1986, Smith 1982). In females, bone loss has three phases. The first phase starts around 30 to 35 years of age and proceeds at a rate of 0.75% to 1% per year until menopause. From menopause until about 5 years after menopause, the rate of bone loss increases to between 2% and 3% per year. During the final phase, the rate of bone loss is approximately 1% per year. Thus, women may lose, on average, about 53% of their peak bone mass by the age of 80 years. In contrast, males may lose, on average, about 18% of their peak bone mass by the age of 80 years (figure 3.32).
Even though body weight tends to decrease with age, the rate of bone loss is usually much greater than the rate at which body weight decreases. Consequently, the effect of bone loss is that the bones, especially weight-bearing bones, become progressively weaker relative to the weight of the rest of the body. In addition to gradually losing strength, the bones also gradually lose their elasticity and become more brittle. In some people, especially women, a loss of bone mass and elasticity is eventually reached when some bones are no longer able to withstand the loads imposed by normal habitual activity. These bones become very susceptible to fracture. This condition, the most common bone disorder in elderly people, is called osteoporosis (Bailey et al 1986, Ferretti et al 2003). Osteoporosis may cause severe disfigurement, especially of the trunk, as a result of fractured or crushed vertebrae. Many deaths in elderly people are due to complications arising from bone fractures that occur as a result of osteoporosis (Kaplan 1983, Kado et al 1999, Cummings and Melton 2002).
Bone loss tends to occur earlier and to proceed at a faster rate in cancellous bone than in compact bone (Bailey et al 1986, Ferretti et al 2003). Consequently, regions of bones with a high proportion of cancellous bone, such as the bodies of the vertebrae, the head and neck of the femur, and the distal end of the radius, are particularly vulnerable to osteoporosis and fracture in elderly people. This vulnerability is reflected in studies that report a rapid increase in the incidence of bone fractures with age, especially in women (Bauer 1960, Chalmers and Ho 1970, Hagino et al 1991, Cummings et al 1993, Court-Brown and Caesar 2006). The results of one study showed that the incidence of fracture to the distal end of the radius was seven times higher in 54-year-old women than in 40-year-old women (Bauer 1960). In another study the incidence of fracture of the neck of the femur was found to be 50 times higher in 70-year-old women than in 40-year-old women (Chalmers and Ho 1970). Bone loss in compact bone occurs mainly on the endosteal surface so that bone width remains relatively unchanged into old age (Smith 1982, Ferretti et al 2003).
Although the cause of osteoporosis is not clear, there is general agreement that four variables are mainly responsible: genetic factors, endocrine status, nutritional factors, and physical activity (Bailey et al 1986, MacKinnon 1988, Ferretti et al 2003). The relative contribution of these variables has not been established, but physical activity seems to be the most important. In the absence of weight-bearing activity, no amount of endocrine or nutritional intervention will prevent rapid bone loss; there must be mechanical stress (Bailey et al 1986, Ferretti et al 2003). Research suggests that regular physical activity throughout life, within the moderate overload range (see chapter 11), can help to prevent osteoporosis in three ways (Bailey 1995, Greene and Naughton 2006, Baxter-Jones et al 2008):
- Peak bone mass is directly related to the level of physical activity prior to peak bone mass; the higher the peak bone mass, the lower the risk of osteoporosis.
- An above-average level of physical activity after peak bone mass will delay the onset of bone loss.
- An above-average level of physical activity after peak bone mass will reduce the rate of bone loss.
Case study 2 discusses whether regular exercise can be used to prevent falls in osteopenic women.
Case Study 2 Using Exercise to Prevent Falls in Osteopenic Women
Hourigan SR, Nitz JC, Brauer S, O'Neill S, Wong J, Richardson CA. 2008. Positive effects of exercise on falls and fracture risk in osteopenic women. Osteoporosis International 19:1077-1086.
The incidence of bone fractures increases with age. As the number of aged people worldwide is increasing, so is the total number of fractures in the aged population (age 65 years and older). Fractures in the aged population are a major health care cost and risk factor for permanent disability and death. Consequently, reducing the risk of fractures in the aged population is a challenge in many countries.
Physical trauma (in particular, falls) and weak bones (due to osteopenia or osteoporosis) are the major causes of fractures in the aged population. Poor balance and weak muscles are risk factors for falls. Osteopenia is defined as bone mineral density (BMD) between 1 and 2.5 standard deviations below the average for young women. Osteoporosis is defined as BMD more than 2.5 standard deviations below the average for young women.
Recent research indicates that muscle strength, bone strength, and balance in the aged population can be improved through properly prescribed physical activity training programs based on resistance exercises involving strength-training machines. The purpose of the present study was to determine the effect of a physical activity program based on weight-bearing activities (rather than strength-training machines) on balance, muscle strength, and bone mineral density in osteopenic women.
Ninety-eight community-dwelling (living more or less independently in their own homes) osteopenic women (age 62.01 ± 8.9; range 41-78 years) were randomly assigned to either a control group (n = 48: no intervention) or an exercise group (n = 50: two 1 hr exercise sessions per week for 20 weeks directed by a trained physiotherapist). Assessments at baseline and post intervention included balance (five measures), strength (quadriceps; hip abductors, adductors, and external rotators; trunk extensors), and BMD (proximal femur and lumbar spine). Baseline assessment showed no significant differences between the exercise and control groups in terms of balance, strength, BMD, or demographics.
The average number of sessions attended by the 42 members of the exercise group who completed the exercise program was 28.2 of a possible 40 sessions (71.2%). Following the intervention, the exercise group showed significantly better performance than the control group in 9 of 11 balance tests (ranging from 10% to 71% better performance) and 7 of 9 strength tests (ranging from 9% to 23% better performance). BMD of the exercise group increased but was not significantly greater than in the control group.
Application
A specific, well-directed program of weight-bearing exercises in a workstation format that emphasizes interaction, discussion, and enjoyment can significantly improve balance and strength in osteopenic women, which in turn is likely to reduce the risk of falling. This type of training may also positively influence BMD, but further research is needed.
Youth sports increase risk of physeal injury
Widespread participation in youth sports increase the risk of physeal injury, resulting in more permanent problems
Case Study 1 Physeal Injuries in Youth Sports
Caine D, DiFiori J, Maffulli N. 2006. Physeal injuries in children's and youth sports: Reasons for concern? British Journal of Sports Medicine 40:749-760.
Participation in children's and youth sports is widespread in Western culture. Many children start year-round training and specialization by 9 years of age. Preteens training at regional centers or with high school and club teams in sports such as gymnastics may train more than 20 hr per week. There is increasing concern, especially among physicians, that the frequency and intensity of training and competition experienced by many participants in children's and youth sports are putting them at risk of serious physeal injury (epiphyseal and apophyseal), which may result in permanent skeletal abnormalities. Unfortunately, detailed information, based on the use of standardized recording systems applied over a long period, on the epidemiology of injuries (incidence, location, type, diagnosis, severity) sustained by participants in children's and youth sports is not available for any sport. The purpose of this study was to systematically review the literature on the frequency and characteristics of physeal injuries in children's and youth sports.
The review was undertaken using Medline and SPORTdiscus. More than 150 reports were obtained, largely case reports or case series investigations. The authors used the reports to determine the number, location, type, diagnosis, and severity of physeal injuries that occur in different sports, but it was not possible to calculate incidence of injury because information was not provided on the total number of participants and exposure time of participants in the various sports.
The review indicates that acute physeal injuries (sudden widening or fracture along or through an epiphyseal or apophyseal plate accompanied by considerable pain) and chronic physeal injuries (progressive widening of an epiphyseal or apophyseal plate associated with a progressive increase in pain, especially during exercise) occur frequently in some sports, including football, baseball, gymnastics, basketball, volleyball, judo, weightlifting, soccer, rugby, tennis, cricket, and long-distance running. The main regions of physeal injuries are the shoulder, elbow, wrist, and knee. Most of the injuries are chronic, and most resolve without complication. However, there are several reports of premature partial or complete physeal closure.
The authors express a number of concerns with current practice, in particular, the paucity of epidemiological data on the distribution and determinants of physeal injuries in children's and youth sports and the apparent lack of knowledge on the part of many coaches of children's and youth sports regarding musculoskeletal growth and development in children in general and physeal injuries in particular.
Application
Coaches should consider the following strategies to reduce the incidence of physeal injuries in children's and youth sports:
- Individualize fitness training and practice for athletes experiencing rapid growth. Assess growth rate by monitoring increases in height and limb segment lengths.
- Use a variety of training and practice drills and avoid excessive volume of training.
- For collision sports, ensure that competition is based on physical maturity rather than chronological age.
- Mandate regular medical assessment to ensure early diagnosis and treatment of epiphyseal and apophyseal plate disorders.
Structure of the knee facilitates extension and flexion
Learn more about the tibiofemoral joint and the ligaments
Capsule of the Knee
The tibiofemoral and patellofemoral joints share a common capsule that has a complicated shape. The capsule is attached above to the femur, below to the tibia, and anteriorly to the patella (figure 6.13). To accommodate the extremes of full flexion and full extension of the tibiofemoral joint, the anterior part of the capsule is folded upward during extension and the posterior part of the capsule is folded downward during flexion. The upward fold, only present in extension, is referred to as the suprapatellar bursa (figure 6.13). The suprapatellar bursa intervenes between the quadriceps tendon and the anterior aspect of the femur just proximal to the patellar surface.
Figure 6.13 Sagittal section through the knee complex showing the shape of the capsule in extension.
The downward fold, only present during flexion, is referred to as the gastrocnemius bursa. The gastrocnemius bursa intervenes between the posterior aspect of the tibial condyles and the gastrocnemius muscle. In general, a bursa is a flattened sac of synovial membrane containing synovial fluid. Bursas minimize friction between structures that slide across each other during normal movement (see chapter 7).
During flexion of the tibiofemoral joint, the suprapatellar bursa becomes progressively smaller and the gastrocnemius bursa becomes progressively larger as synovial fluid is redistributed from the suprapatellar bursa to the gastrocnemius bursa. The movement of synovial fluid is reversed during extension of the tibiofemoral joint; that is, the gastrocnemius bursa becomes progressively smaller and the suprapatellar bursa becomes progressively larger.
The suprapatellar bursa is separated from the femur by a pad of fat called the suprapatellar fat pad. Lying in the space bounded by the upper two thirds of the posterior aspect of the patellar ligament, the anterior intercondylar area of the tibia, and the anterior inferior aspect of the articular surface of the femoral condyles is a pad of fat called the infrapatellar fat pad. It is roughly triangular in sagittal cross section and is suspended superiorly from a fibro-adipose band called the infrapatellar fold. The infrapatellar fold is attached anteriorly to the inferior pole of the patella and posteriorly to the anterior border of the intercondylar notch (figure 6.13). The infrapatellar fat pad is attached anteriorly to the posterior aspect of the patellar ligament and extends at both sides of the patellar ligament. The infrapatellar fat pad also extends narrow branches halfway up each side of the patella; the branches are referred to as alar folds (alar = winglike). The infrapatellar fat pad cushions the patellar ligament and lower part of the patella during movements of the knee.
Knee Ligaments
Four extracapsular ligaments support the tibiofemoral joint. The lateral ligament (also referred to as the lateral collateral ligament and the fibular collateral ligament) is attached superiorly to the lateral epicondyle of the femur and inferiorly to the head of the fibula (figure 6.14a). The medial ligament (also referred to as the medial collateral ligament and the tibial collateral ligament) is attached superiorly to the medial epicondyle of the femur and inferiorly to the medial aspect of the tibia below the tibial condyle (figure 6.14b). The posterior fibers of the medial ligament blend with the joint capsule at the level of the medial meniscus and thus the medial ligament is not completely extracapsular. The arrangement of the medial and lateral ligaments and the curvature of the femoral condyles are such that both ligaments are relatively slack when the knee is flexed but become progressively more taut as the joint extends. In a normal joint the ligaments are fully taut when the joint is fully extended. In this position of the joint both ligaments help to prevent hyperextension and lateral rotation of the tibia relative to the femur. With the knee fully extended, the range of abduction and adduction is normally zero. Because the medial and lateral ligaments are relatively slack when the knee is flexed, a certain amount of axial rotation and abduction and adduction of the lower leg can occur when the knee is in a flexed, non-weight-bearing position. For example, when a person is sitting on a table with his lower leg hanging freely, the ranges of internal and external rotation are normally around 30° and 40°, respectively (Norkin and Levangie 1992). However, the ranges of abduction and adduction are normally very small, approximately 2° to 5°.
Figure 6.14 Location of the main ligaments of the left knee. (a) Lateral aspect. (b) Medial aspect.
Injuries to the lateral and, in particular, the medial ligaments are common in sports (Reider 1996). The classic cause of medial ligament injury is a blow to the lateral aspect of the knee while the foot in contact with the ground, resulting in abduction of the knee. This situation is common in sports such as American football, soccer, and rugby. The excessive loading on the medial ligament in such situations can result in serious injury (Indelicato 1995). Medial ligament injuries of a less severe but nonetheless persistent nature are common in swimmers, especially breaststroke swimmers. The whip-kick leg action in breaststroke tends to simultaneously abduct and laterally rotate (tibia with respect to femur) the knee, resulting in strain of the medial ligament and associated medial supporting structures (Vizsolyi et al 1987).
Physical activity helps reduce bone loss
Bone loss begins around age 45 – 50 and moves a at different rates during different phases
Porosity, Osteopenia, and Osteoporosis
Because of the channels and spaces within compact and cancellous bone, any particular region of a bone consists of certain amounts of bone tissue and nonbone tissue. The term porosity describes the proportion of nonbone tissue. At skeletal maturity the porosity of compact and cancellous bone is approximately 2% and 50%, respectively; the density (amount of bone tissue per unit volume) of compact bone is approximately double that of cancellous bone (Radin 1984, Tortora 2004). The density of bone tissue depends on the degree of mineralization. During ossification, the degree of mineralization of bone tissue gradually increases and reaches a maximum level at skeletal maturity (Bailey et al 1986). However, the amount of bone within the skeleton may continue to increase for 5 to 10 years after skeletal maturity, especially in people who are physically active (Stillman et al 1986, Talmage and Anderson 1984, Frost 2003). Consequently, bone mass peaks in males and females between 25 and 30 years of age. In terms of turnover, this means that from skeletal maturity to the age at which peak bone mass occurs, more new bone is formed than old and damaged bone is absorbed.
Following peak bone mass there is usually a stable period in which the amount of bone in the skeleton remains about the same; there is a balance between bone absorption and bone formation. This stable period is followed by a gradual decrease in bone mass for the rest of the person's life; the rate of bone absorption exceeds the rate of bone formation. Bone mass is the product of bone volume and bone density. The loss in bone mass that occurs with age following peak bone mass is the result of decreases in bone volume and bone density. Osteopenia refers to a level of bone density below the normal level for a person's age and sex (Bailey 1995, Frost 1997).
Bone mass starts to decrease earlier and at a greater rate in females than in males. In males, bone loss normally starts between 45 and 50 years of age and proceeds at a rate of 0.4% to 0.75% per year (Bailey et al 1986, Smith 1982). In females, bone loss has three phases. The first phase starts around 30 to 35 years of age and proceeds at a rate of 0.75% to 1% per year until menopause. From menopause until about 5 years after menopause, the rate of bone loss increases to between 2% and 3% per year. During the final phase, the rate of bone loss is approximately 1% per year. Thus, women may lose, on average, about 53% of their peak bone mass by the age of 80 years. In contrast, males may lose, on average, about 18% of their peak bone mass by the age of 80 years (figure 3.32).
Even though body weight tends to decrease with age, the rate of bone loss is usually much greater than the rate at which body weight decreases. Consequently, the effect of bone loss is that the bones, especially weight-bearing bones, become progressively weaker relative to the weight of the rest of the body. In addition to gradually losing strength, the bones also gradually lose their elasticity and become more brittle. In some people, especially women, a loss of bone mass and elasticity is eventually reached when some bones are no longer able to withstand the loads imposed by normal habitual activity. These bones become very susceptible to fracture. This condition, the most common bone disorder in elderly people, is called osteoporosis (Bailey et al 1986, Ferretti et al 2003). Osteoporosis may cause severe disfigurement, especially of the trunk, as a result of fractured or crushed vertebrae. Many deaths in elderly people are due to complications arising from bone fractures that occur as a result of osteoporosis (Kaplan 1983, Kado et al 1999, Cummings and Melton 2002).
Bone loss tends to occur earlier and to proceed at a faster rate in cancellous bone than in compact bone (Bailey et al 1986, Ferretti et al 2003). Consequently, regions of bones with a high proportion of cancellous bone, such as the bodies of the vertebrae, the head and neck of the femur, and the distal end of the radius, are particularly vulnerable to osteoporosis and fracture in elderly people. This vulnerability is reflected in studies that report a rapid increase in the incidence of bone fractures with age, especially in women (Bauer 1960, Chalmers and Ho 1970, Hagino et al 1991, Cummings et al 1993, Court-Brown and Caesar 2006). The results of one study showed that the incidence of fracture to the distal end of the radius was seven times higher in 54-year-old women than in 40-year-old women (Bauer 1960). In another study the incidence of fracture of the neck of the femur was found to be 50 times higher in 70-year-old women than in 40-year-old women (Chalmers and Ho 1970). Bone loss in compact bone occurs mainly on the endosteal surface so that bone width remains relatively unchanged into old age (Smith 1982, Ferretti et al 2003).
Although the cause of osteoporosis is not clear, there is general agreement that four variables are mainly responsible: genetic factors, endocrine status, nutritional factors, and physical activity (Bailey et al 1986, MacKinnon 1988, Ferretti et al 2003). The relative contribution of these variables has not been established, but physical activity seems to be the most important. In the absence of weight-bearing activity, no amount of endocrine or nutritional intervention will prevent rapid bone loss; there must be mechanical stress (Bailey et al 1986, Ferretti et al 2003). Research suggests that regular physical activity throughout life, within the moderate overload range (see chapter 11), can help to prevent osteoporosis in three ways (Bailey 1995, Greene and Naughton 2006, Baxter-Jones et al 2008):
- Peak bone mass is directly related to the level of physical activity prior to peak bone mass; the higher the peak bone mass, the lower the risk of osteoporosis.
- An above-average level of physical activity after peak bone mass will delay the onset of bone loss.
- An above-average level of physical activity after peak bone mass will reduce the rate of bone loss.
Case study 2 discusses whether regular exercise can be used to prevent falls in osteopenic women.
Case Study 2 Using Exercise to Prevent Falls in Osteopenic Women
Hourigan SR, Nitz JC, Brauer S, O'Neill S, Wong J, Richardson CA. 2008. Positive effects of exercise on falls and fracture risk in osteopenic women. Osteoporosis International 19:1077-1086.
The incidence of bone fractures increases with age. As the number of aged people worldwide is increasing, so is the total number of fractures in the aged population (age 65 years and older). Fractures in the aged population are a major health care cost and risk factor for permanent disability and death. Consequently, reducing the risk of fractures in the aged population is a challenge in many countries.
Physical trauma (in particular, falls) and weak bones (due to osteopenia or osteoporosis) are the major causes of fractures in the aged population. Poor balance and weak muscles are risk factors for falls. Osteopenia is defined as bone mineral density (BMD) between 1 and 2.5 standard deviations below the average for young women. Osteoporosis is defined as BMD more than 2.5 standard deviations below the average for young women.
Recent research indicates that muscle strength, bone strength, and balance in the aged population can be improved through properly prescribed physical activity training programs based on resistance exercises involving strength-training machines. The purpose of the present study was to determine the effect of a physical activity program based on weight-bearing activities (rather than strength-training machines) on balance, muscle strength, and bone mineral density in osteopenic women.
Ninety-eight community-dwelling (living more or less independently in their own homes) osteopenic women (age 62.01 ± 8.9; range 41-78 years) were randomly assigned to either a control group (n = 48: no intervention) or an exercise group (n = 50: two 1 hr exercise sessions per week for 20 weeks directed by a trained physiotherapist). Assessments at baseline and post intervention included balance (five measures), strength (quadriceps; hip abductors, adductors, and external rotators; trunk extensors), and BMD (proximal femur and lumbar spine). Baseline assessment showed no significant differences between the exercise and control groups in terms of balance, strength, BMD, or demographics.
The average number of sessions attended by the 42 members of the exercise group who completed the exercise program was 28.2 of a possible 40 sessions (71.2%). Following the intervention, the exercise group showed significantly better performance than the control group in 9 of 11 balance tests (ranging from 10% to 71% better performance) and 7 of 9 strength tests (ranging from 9% to 23% better performance). BMD of the exercise group increased but was not significantly greater than in the control group.
Application
A specific, well-directed program of weight-bearing exercises in a workstation format that emphasizes interaction, discussion, and enjoyment can significantly improve balance and strength in osteopenic women, which in turn is likely to reduce the risk of falling. This type of training may also positively influence BMD, but further research is needed.
Youth sports increase risk of physeal injury
Widespread participation in youth sports increase the risk of physeal injury, resulting in more permanent problems
Case Study 1 Physeal Injuries in Youth Sports
Caine D, DiFiori J, Maffulli N. 2006. Physeal injuries in children's and youth sports: Reasons for concern? British Journal of Sports Medicine 40:749-760.
Participation in children's and youth sports is widespread in Western culture. Many children start year-round training and specialization by 9 years of age. Preteens training at regional centers or with high school and club teams in sports such as gymnastics may train more than 20 hr per week. There is increasing concern, especially among physicians, that the frequency and intensity of training and competition experienced by many participants in children's and youth sports are putting them at risk of serious physeal injury (epiphyseal and apophyseal), which may result in permanent skeletal abnormalities. Unfortunately, detailed information, based on the use of standardized recording systems applied over a long period, on the epidemiology of injuries (incidence, location, type, diagnosis, severity) sustained by participants in children's and youth sports is not available for any sport. The purpose of this study was to systematically review the literature on the frequency and characteristics of physeal injuries in children's and youth sports.
The review was undertaken using Medline and SPORTdiscus. More than 150 reports were obtained, largely case reports or case series investigations. The authors used the reports to determine the number, location, type, diagnosis, and severity of physeal injuries that occur in different sports, but it was not possible to calculate incidence of injury because information was not provided on the total number of participants and exposure time of participants in the various sports.
The review indicates that acute physeal injuries (sudden widening or fracture along or through an epiphyseal or apophyseal plate accompanied by considerable pain) and chronic physeal injuries (progressive widening of an epiphyseal or apophyseal plate associated with a progressive increase in pain, especially during exercise) occur frequently in some sports, including football, baseball, gymnastics, basketball, volleyball, judo, weightlifting, soccer, rugby, tennis, cricket, and long-distance running. The main regions of physeal injuries are the shoulder, elbow, wrist, and knee. Most of the injuries are chronic, and most resolve without complication. However, there are several reports of premature partial or complete physeal closure.
The authors express a number of concerns with current practice, in particular, the paucity of epidemiological data on the distribution and determinants of physeal injuries in children's and youth sports and the apparent lack of knowledge on the part of many coaches of children's and youth sports regarding musculoskeletal growth and development in children in general and physeal injuries in particular.
Application
Coaches should consider the following strategies to reduce the incidence of physeal injuries in children's and youth sports:
- Individualize fitness training and practice for athletes experiencing rapid growth. Assess growth rate by monitoring increases in height and limb segment lengths.
- Use a variety of training and practice drills and avoid excessive volume of training.
- For collision sports, ensure that competition is based on physical maturity rather than chronological age.
- Mandate regular medical assessment to ensure early diagnosis and treatment of epiphyseal and apophyseal plate disorders.
Structure of the knee facilitates extension and flexion
Learn more about the tibiofemoral joint and the ligaments
Capsule of the Knee
The tibiofemoral and patellofemoral joints share a common capsule that has a complicated shape. The capsule is attached above to the femur, below to the tibia, and anteriorly to the patella (figure 6.13). To accommodate the extremes of full flexion and full extension of the tibiofemoral joint, the anterior part of the capsule is folded upward during extension and the posterior part of the capsule is folded downward during flexion. The upward fold, only present in extension, is referred to as the suprapatellar bursa (figure 6.13). The suprapatellar bursa intervenes between the quadriceps tendon and the anterior aspect of the femur just proximal to the patellar surface.
Figure 6.13 Sagittal section through the knee complex showing the shape of the capsule in extension.
The downward fold, only present during flexion, is referred to as the gastrocnemius bursa. The gastrocnemius bursa intervenes between the posterior aspect of the tibial condyles and the gastrocnemius muscle. In general, a bursa is a flattened sac of synovial membrane containing synovial fluid. Bursas minimize friction between structures that slide across each other during normal movement (see chapter 7).
During flexion of the tibiofemoral joint, the suprapatellar bursa becomes progressively smaller and the gastrocnemius bursa becomes progressively larger as synovial fluid is redistributed from the suprapatellar bursa to the gastrocnemius bursa. The movement of synovial fluid is reversed during extension of the tibiofemoral joint; that is, the gastrocnemius bursa becomes progressively smaller and the suprapatellar bursa becomes progressively larger.
The suprapatellar bursa is separated from the femur by a pad of fat called the suprapatellar fat pad. Lying in the space bounded by the upper two thirds of the posterior aspect of the patellar ligament, the anterior intercondylar area of the tibia, and the anterior inferior aspect of the articular surface of the femoral condyles is a pad of fat called the infrapatellar fat pad. It is roughly triangular in sagittal cross section and is suspended superiorly from a fibro-adipose band called the infrapatellar fold. The infrapatellar fold is attached anteriorly to the inferior pole of the patella and posteriorly to the anterior border of the intercondylar notch (figure 6.13). The infrapatellar fat pad is attached anteriorly to the posterior aspect of the patellar ligament and extends at both sides of the patellar ligament. The infrapatellar fat pad also extends narrow branches halfway up each side of the patella; the branches are referred to as alar folds (alar = winglike). The infrapatellar fat pad cushions the patellar ligament and lower part of the patella during movements of the knee.
Knee Ligaments
Four extracapsular ligaments support the tibiofemoral joint. The lateral ligament (also referred to as the lateral collateral ligament and the fibular collateral ligament) is attached superiorly to the lateral epicondyle of the femur and inferiorly to the head of the fibula (figure 6.14a). The medial ligament (also referred to as the medial collateral ligament and the tibial collateral ligament) is attached superiorly to the medial epicondyle of the femur and inferiorly to the medial aspect of the tibia below the tibial condyle (figure 6.14b). The posterior fibers of the medial ligament blend with the joint capsule at the level of the medial meniscus and thus the medial ligament is not completely extracapsular. The arrangement of the medial and lateral ligaments and the curvature of the femoral condyles are such that both ligaments are relatively slack when the knee is flexed but become progressively more taut as the joint extends. In a normal joint the ligaments are fully taut when the joint is fully extended. In this position of the joint both ligaments help to prevent hyperextension and lateral rotation of the tibia relative to the femur. With the knee fully extended, the range of abduction and adduction is normally zero. Because the medial and lateral ligaments are relatively slack when the knee is flexed, a certain amount of axial rotation and abduction and adduction of the lower leg can occur when the knee is in a flexed, non-weight-bearing position. For example, when a person is sitting on a table with his lower leg hanging freely, the ranges of internal and external rotation are normally around 30° and 40°, respectively (Norkin and Levangie 1992). However, the ranges of abduction and adduction are normally very small, approximately 2° to 5°.
Figure 6.14 Location of the main ligaments of the left knee. (a) Lateral aspect. (b) Medial aspect.
Injuries to the lateral and, in particular, the medial ligaments are common in sports (Reider 1996). The classic cause of medial ligament injury is a blow to the lateral aspect of the knee while the foot in contact with the ground, resulting in abduction of the knee. This situation is common in sports such as American football, soccer, and rugby. The excessive loading on the medial ligament in such situations can result in serious injury (Indelicato 1995). Medial ligament injuries of a less severe but nonetheless persistent nature are common in swimmers, especially breaststroke swimmers. The whip-kick leg action in breaststroke tends to simultaneously abduct and laterally rotate (tibia with respect to femur) the knee, resulting in strain of the medial ligament and associated medial supporting structures (Vizsolyi et al 1987).
Physical activity helps reduce bone loss
Bone loss begins around age 45 – 50 and moves a at different rates during different phases
Porosity, Osteopenia, and Osteoporosis
Because of the channels and spaces within compact and cancellous bone, any particular region of a bone consists of certain amounts of bone tissue and nonbone tissue. The term porosity describes the proportion of nonbone tissue. At skeletal maturity the porosity of compact and cancellous bone is approximately 2% and 50%, respectively; the density (amount of bone tissue per unit volume) of compact bone is approximately double that of cancellous bone (Radin 1984, Tortora 2004). The density of bone tissue depends on the degree of mineralization. During ossification, the degree of mineralization of bone tissue gradually increases and reaches a maximum level at skeletal maturity (Bailey et al 1986). However, the amount of bone within the skeleton may continue to increase for 5 to 10 years after skeletal maturity, especially in people who are physically active (Stillman et al 1986, Talmage and Anderson 1984, Frost 2003). Consequently, bone mass peaks in males and females between 25 and 30 years of age. In terms of turnover, this means that from skeletal maturity to the age at which peak bone mass occurs, more new bone is formed than old and damaged bone is absorbed.
Following peak bone mass there is usually a stable period in which the amount of bone in the skeleton remains about the same; there is a balance between bone absorption and bone formation. This stable period is followed by a gradual decrease in bone mass for the rest of the person's life; the rate of bone absorption exceeds the rate of bone formation. Bone mass is the product of bone volume and bone density. The loss in bone mass that occurs with age following peak bone mass is the result of decreases in bone volume and bone density. Osteopenia refers to a level of bone density below the normal level for a person's age and sex (Bailey 1995, Frost 1997).
Bone mass starts to decrease earlier and at a greater rate in females than in males. In males, bone loss normally starts between 45 and 50 years of age and proceeds at a rate of 0.4% to 0.75% per year (Bailey et al 1986, Smith 1982). In females, bone loss has three phases. The first phase starts around 30 to 35 years of age and proceeds at a rate of 0.75% to 1% per year until menopause. From menopause until about 5 years after menopause, the rate of bone loss increases to between 2% and 3% per year. During the final phase, the rate of bone loss is approximately 1% per year. Thus, women may lose, on average, about 53% of their peak bone mass by the age of 80 years. In contrast, males may lose, on average, about 18% of their peak bone mass by the age of 80 years (figure 3.32).
Even though body weight tends to decrease with age, the rate of bone loss is usually much greater than the rate at which body weight decreases. Consequently, the effect of bone loss is that the bones, especially weight-bearing bones, become progressively weaker relative to the weight of the rest of the body. In addition to gradually losing strength, the bones also gradually lose their elasticity and become more brittle. In some people, especially women, a loss of bone mass and elasticity is eventually reached when some bones are no longer able to withstand the loads imposed by normal habitual activity. These bones become very susceptible to fracture. This condition, the most common bone disorder in elderly people, is called osteoporosis (Bailey et al 1986, Ferretti et al 2003). Osteoporosis may cause severe disfigurement, especially of the trunk, as a result of fractured or crushed vertebrae. Many deaths in elderly people are due to complications arising from bone fractures that occur as a result of osteoporosis (Kaplan 1983, Kado et al 1999, Cummings and Melton 2002).
Bone loss tends to occur earlier and to proceed at a faster rate in cancellous bone than in compact bone (Bailey et al 1986, Ferretti et al 2003). Consequently, regions of bones with a high proportion of cancellous bone, such as the bodies of the vertebrae, the head and neck of the femur, and the distal end of the radius, are particularly vulnerable to osteoporosis and fracture in elderly people. This vulnerability is reflected in studies that report a rapid increase in the incidence of bone fractures with age, especially in women (Bauer 1960, Chalmers and Ho 1970, Hagino et al 1991, Cummings et al 1993, Court-Brown and Caesar 2006). The results of one study showed that the incidence of fracture to the distal end of the radius was seven times higher in 54-year-old women than in 40-year-old women (Bauer 1960). In another study the incidence of fracture of the neck of the femur was found to be 50 times higher in 70-year-old women than in 40-year-old women (Chalmers and Ho 1970). Bone loss in compact bone occurs mainly on the endosteal surface so that bone width remains relatively unchanged into old age (Smith 1982, Ferretti et al 2003).
Although the cause of osteoporosis is not clear, there is general agreement that four variables are mainly responsible: genetic factors, endocrine status, nutritional factors, and physical activity (Bailey et al 1986, MacKinnon 1988, Ferretti et al 2003). The relative contribution of these variables has not been established, but physical activity seems to be the most important. In the absence of weight-bearing activity, no amount of endocrine or nutritional intervention will prevent rapid bone loss; there must be mechanical stress (Bailey et al 1986, Ferretti et al 2003). Research suggests that regular physical activity throughout life, within the moderate overload range (see chapter 11), can help to prevent osteoporosis in three ways (Bailey 1995, Greene and Naughton 2006, Baxter-Jones et al 2008):
- Peak bone mass is directly related to the level of physical activity prior to peak bone mass; the higher the peak bone mass, the lower the risk of osteoporosis.
- An above-average level of physical activity after peak bone mass will delay the onset of bone loss.
- An above-average level of physical activity after peak bone mass will reduce the rate of bone loss.
Case study 2 discusses whether regular exercise can be used to prevent falls in osteopenic women.
Case Study 2 Using Exercise to Prevent Falls in Osteopenic Women
Hourigan SR, Nitz JC, Brauer S, O'Neill S, Wong J, Richardson CA. 2008. Positive effects of exercise on falls and fracture risk in osteopenic women. Osteoporosis International 19:1077-1086.
The incidence of bone fractures increases with age. As the number of aged people worldwide is increasing, so is the total number of fractures in the aged population (age 65 years and older). Fractures in the aged population are a major health care cost and risk factor for permanent disability and death. Consequently, reducing the risk of fractures in the aged population is a challenge in many countries.
Physical trauma (in particular, falls) and weak bones (due to osteopenia or osteoporosis) are the major causes of fractures in the aged population. Poor balance and weak muscles are risk factors for falls. Osteopenia is defined as bone mineral density (BMD) between 1 and 2.5 standard deviations below the average for young women. Osteoporosis is defined as BMD more than 2.5 standard deviations below the average for young women.
Recent research indicates that muscle strength, bone strength, and balance in the aged population can be improved through properly prescribed physical activity training programs based on resistance exercises involving strength-training machines. The purpose of the present study was to determine the effect of a physical activity program based on weight-bearing activities (rather than strength-training machines) on balance, muscle strength, and bone mineral density in osteopenic women.
Ninety-eight community-dwelling (living more or less independently in their own homes) osteopenic women (age 62.01 ± 8.9; range 41-78 years) were randomly assigned to either a control group (n = 48: no intervention) or an exercise group (n = 50: two 1 hr exercise sessions per week for 20 weeks directed by a trained physiotherapist). Assessments at baseline and post intervention included balance (five measures), strength (quadriceps; hip abductors, adductors, and external rotators; trunk extensors), and BMD (proximal femur and lumbar spine). Baseline assessment showed no significant differences between the exercise and control groups in terms of balance, strength, BMD, or demographics.
The average number of sessions attended by the 42 members of the exercise group who completed the exercise program was 28.2 of a possible 40 sessions (71.2%). Following the intervention, the exercise group showed significantly better performance than the control group in 9 of 11 balance tests (ranging from 10% to 71% better performance) and 7 of 9 strength tests (ranging from 9% to 23% better performance). BMD of the exercise group increased but was not significantly greater than in the control group.
Application
A specific, well-directed program of weight-bearing exercises in a workstation format that emphasizes interaction, discussion, and enjoyment can significantly improve balance and strength in osteopenic women, which in turn is likely to reduce the risk of falling. This type of training may also positively influence BMD, but further research is needed.
Youth sports increase risk of physeal injury
Widespread participation in youth sports increase the risk of physeal injury, resulting in more permanent problems
Case Study 1 Physeal Injuries in Youth Sports
Caine D, DiFiori J, Maffulli N. 2006. Physeal injuries in children's and youth sports: Reasons for concern? British Journal of Sports Medicine 40:749-760.
Participation in children's and youth sports is widespread in Western culture. Many children start year-round training and specialization by 9 years of age. Preteens training at regional centers or with high school and club teams in sports such as gymnastics may train more than 20 hr per week. There is increasing concern, especially among physicians, that the frequency and intensity of training and competition experienced by many participants in children's and youth sports are putting them at risk of serious physeal injury (epiphyseal and apophyseal), which may result in permanent skeletal abnormalities. Unfortunately, detailed information, based on the use of standardized recording systems applied over a long period, on the epidemiology of injuries (incidence, location, type, diagnosis, severity) sustained by participants in children's and youth sports is not available for any sport. The purpose of this study was to systematically review the literature on the frequency and characteristics of physeal injuries in children's and youth sports.
The review was undertaken using Medline and SPORTdiscus. More than 150 reports were obtained, largely case reports or case series investigations. The authors used the reports to determine the number, location, type, diagnosis, and severity of physeal injuries that occur in different sports, but it was not possible to calculate incidence of injury because information was not provided on the total number of participants and exposure time of participants in the various sports.
The review indicates that acute physeal injuries (sudden widening or fracture along or through an epiphyseal or apophyseal plate accompanied by considerable pain) and chronic physeal injuries (progressive widening of an epiphyseal or apophyseal plate associated with a progressive increase in pain, especially during exercise) occur frequently in some sports, including football, baseball, gymnastics, basketball, volleyball, judo, weightlifting, soccer, rugby, tennis, cricket, and long-distance running. The main regions of physeal injuries are the shoulder, elbow, wrist, and knee. Most of the injuries are chronic, and most resolve without complication. However, there are several reports of premature partial or complete physeal closure.
The authors express a number of concerns with current practice, in particular, the paucity of epidemiological data on the distribution and determinants of physeal injuries in children's and youth sports and the apparent lack of knowledge on the part of many coaches of children's and youth sports regarding musculoskeletal growth and development in children in general and physeal injuries in particular.
Application
Coaches should consider the following strategies to reduce the incidence of physeal injuries in children's and youth sports:
- Individualize fitness training and practice for athletes experiencing rapid growth. Assess growth rate by monitoring increases in height and limb segment lengths.
- Use a variety of training and practice drills and avoid excessive volume of training.
- For collision sports, ensure that competition is based on physical maturity rather than chronological age.
- Mandate regular medical assessment to ensure early diagnosis and treatment of epiphyseal and apophyseal plate disorders.
Structure of the knee facilitates extension and flexion
Learn more about the tibiofemoral joint and the ligaments
Capsule of the Knee
The tibiofemoral and patellofemoral joints share a common capsule that has a complicated shape. The capsule is attached above to the femur, below to the tibia, and anteriorly to the patella (figure 6.13). To accommodate the extremes of full flexion and full extension of the tibiofemoral joint, the anterior part of the capsule is folded upward during extension and the posterior part of the capsule is folded downward during flexion. The upward fold, only present in extension, is referred to as the suprapatellar bursa (figure 6.13). The suprapatellar bursa intervenes between the quadriceps tendon and the anterior aspect of the femur just proximal to the patellar surface.
Figure 6.13 Sagittal section through the knee complex showing the shape of the capsule in extension.
The downward fold, only present during flexion, is referred to as the gastrocnemius bursa. The gastrocnemius bursa intervenes between the posterior aspect of the tibial condyles and the gastrocnemius muscle. In general, a bursa is a flattened sac of synovial membrane containing synovial fluid. Bursas minimize friction between structures that slide across each other during normal movement (see chapter 7).
During flexion of the tibiofemoral joint, the suprapatellar bursa becomes progressively smaller and the gastrocnemius bursa becomes progressively larger as synovial fluid is redistributed from the suprapatellar bursa to the gastrocnemius bursa. The movement of synovial fluid is reversed during extension of the tibiofemoral joint; that is, the gastrocnemius bursa becomes progressively smaller and the suprapatellar bursa becomes progressively larger.
The suprapatellar bursa is separated from the femur by a pad of fat called the suprapatellar fat pad. Lying in the space bounded by the upper two thirds of the posterior aspect of the patellar ligament, the anterior intercondylar area of the tibia, and the anterior inferior aspect of the articular surface of the femoral condyles is a pad of fat called the infrapatellar fat pad. It is roughly triangular in sagittal cross section and is suspended superiorly from a fibro-adipose band called the infrapatellar fold. The infrapatellar fold is attached anteriorly to the inferior pole of the patella and posteriorly to the anterior border of the intercondylar notch (figure 6.13). The infrapatellar fat pad is attached anteriorly to the posterior aspect of the patellar ligament and extends at both sides of the patellar ligament. The infrapatellar fat pad also extends narrow branches halfway up each side of the patella; the branches are referred to as alar folds (alar = winglike). The infrapatellar fat pad cushions the patellar ligament and lower part of the patella during movements of the knee.
Knee Ligaments
Four extracapsular ligaments support the tibiofemoral joint. The lateral ligament (also referred to as the lateral collateral ligament and the fibular collateral ligament) is attached superiorly to the lateral epicondyle of the femur and inferiorly to the head of the fibula (figure 6.14a). The medial ligament (also referred to as the medial collateral ligament and the tibial collateral ligament) is attached superiorly to the medial epicondyle of the femur and inferiorly to the medial aspect of the tibia below the tibial condyle (figure 6.14b). The posterior fibers of the medial ligament blend with the joint capsule at the level of the medial meniscus and thus the medial ligament is not completely extracapsular. The arrangement of the medial and lateral ligaments and the curvature of the femoral condyles are such that both ligaments are relatively slack when the knee is flexed but become progressively more taut as the joint extends. In a normal joint the ligaments are fully taut when the joint is fully extended. In this position of the joint both ligaments help to prevent hyperextension and lateral rotation of the tibia relative to the femur. With the knee fully extended, the range of abduction and adduction is normally zero. Because the medial and lateral ligaments are relatively slack when the knee is flexed, a certain amount of axial rotation and abduction and adduction of the lower leg can occur when the knee is in a flexed, non-weight-bearing position. For example, when a person is sitting on a table with his lower leg hanging freely, the ranges of internal and external rotation are normally around 30° and 40°, respectively (Norkin and Levangie 1992). However, the ranges of abduction and adduction are normally very small, approximately 2° to 5°.
Figure 6.14 Location of the main ligaments of the left knee. (a) Lateral aspect. (b) Medial aspect.
Injuries to the lateral and, in particular, the medial ligaments are common in sports (Reider 1996). The classic cause of medial ligament injury is a blow to the lateral aspect of the knee while the foot in contact with the ground, resulting in abduction of the knee. This situation is common in sports such as American football, soccer, and rugby. The excessive loading on the medial ligament in such situations can result in serious injury (Indelicato 1995). Medial ligament injuries of a less severe but nonetheless persistent nature are common in swimmers, especially breaststroke swimmers. The whip-kick leg action in breaststroke tends to simultaneously abduct and laterally rotate (tibia with respect to femur) the knee, resulting in strain of the medial ligament and associated medial supporting structures (Vizsolyi et al 1987).
Physical activity helps reduce bone loss
Bone loss begins around age 45 – 50 and moves a at different rates during different phases
Porosity, Osteopenia, and Osteoporosis
Because of the channels and spaces within compact and cancellous bone, any particular region of a bone consists of certain amounts of bone tissue and nonbone tissue. The term porosity describes the proportion of nonbone tissue. At skeletal maturity the porosity of compact and cancellous bone is approximately 2% and 50%, respectively; the density (amount of bone tissue per unit volume) of compact bone is approximately double that of cancellous bone (Radin 1984, Tortora 2004). The density of bone tissue depends on the degree of mineralization. During ossification, the degree of mineralization of bone tissue gradually increases and reaches a maximum level at skeletal maturity (Bailey et al 1986). However, the amount of bone within the skeleton may continue to increase for 5 to 10 years after skeletal maturity, especially in people who are physically active (Stillman et al 1986, Talmage and Anderson 1984, Frost 2003). Consequently, bone mass peaks in males and females between 25 and 30 years of age. In terms of turnover, this means that from skeletal maturity to the age at which peak bone mass occurs, more new bone is formed than old and damaged bone is absorbed.
Following peak bone mass there is usually a stable period in which the amount of bone in the skeleton remains about the same; there is a balance between bone absorption and bone formation. This stable period is followed by a gradual decrease in bone mass for the rest of the person's life; the rate of bone absorption exceeds the rate of bone formation. Bone mass is the product of bone volume and bone density. The loss in bone mass that occurs with age following peak bone mass is the result of decreases in bone volume and bone density. Osteopenia refers to a level of bone density below the normal level for a person's age and sex (Bailey 1995, Frost 1997).
Bone mass starts to decrease earlier and at a greater rate in females than in males. In males, bone loss normally starts between 45 and 50 years of age and proceeds at a rate of 0.4% to 0.75% per year (Bailey et al 1986, Smith 1982). In females, bone loss has three phases. The first phase starts around 30 to 35 years of age and proceeds at a rate of 0.75% to 1% per year until menopause. From menopause until about 5 years after menopause, the rate of bone loss increases to between 2% and 3% per year. During the final phase, the rate of bone loss is approximately 1% per year. Thus, women may lose, on average, about 53% of their peak bone mass by the age of 80 years. In contrast, males may lose, on average, about 18% of their peak bone mass by the age of 80 years (figure 3.32).
Even though body weight tends to decrease with age, the rate of bone loss is usually much greater than the rate at which body weight decreases. Consequently, the effect of bone loss is that the bones, especially weight-bearing bones, become progressively weaker relative to the weight of the rest of the body. In addition to gradually losing strength, the bones also gradually lose their elasticity and become more brittle. In some people, especially women, a loss of bone mass and elasticity is eventually reached when some bones are no longer able to withstand the loads imposed by normal habitual activity. These bones become very susceptible to fracture. This condition, the most common bone disorder in elderly people, is called osteoporosis (Bailey et al 1986, Ferretti et al 2003). Osteoporosis may cause severe disfigurement, especially of the trunk, as a result of fractured or crushed vertebrae. Many deaths in elderly people are due to complications arising from bone fractures that occur as a result of osteoporosis (Kaplan 1983, Kado et al 1999, Cummings and Melton 2002).
Bone loss tends to occur earlier and to proceed at a faster rate in cancellous bone than in compact bone (Bailey et al 1986, Ferretti et al 2003). Consequently, regions of bones with a high proportion of cancellous bone, such as the bodies of the vertebrae, the head and neck of the femur, and the distal end of the radius, are particularly vulnerable to osteoporosis and fracture in elderly people. This vulnerability is reflected in studies that report a rapid increase in the incidence of bone fractures with age, especially in women (Bauer 1960, Chalmers and Ho 1970, Hagino et al 1991, Cummings et al 1993, Court-Brown and Caesar 2006). The results of one study showed that the incidence of fracture to the distal end of the radius was seven times higher in 54-year-old women than in 40-year-old women (Bauer 1960). In another study the incidence of fracture of the neck of the femur was found to be 50 times higher in 70-year-old women than in 40-year-old women (Chalmers and Ho 1970). Bone loss in compact bone occurs mainly on the endosteal surface so that bone width remains relatively unchanged into old age (Smith 1982, Ferretti et al 2003).
Although the cause of osteoporosis is not clear, there is general agreement that four variables are mainly responsible: genetic factors, endocrine status, nutritional factors, and physical activity (Bailey et al 1986, MacKinnon 1988, Ferretti et al 2003). The relative contribution of these variables has not been established, but physical activity seems to be the most important. In the absence of weight-bearing activity, no amount of endocrine or nutritional intervention will prevent rapid bone loss; there must be mechanical stress (Bailey et al 1986, Ferretti et al 2003). Research suggests that regular physical activity throughout life, within the moderate overload range (see chapter 11), can help to prevent osteoporosis in three ways (Bailey 1995, Greene and Naughton 2006, Baxter-Jones et al 2008):
- Peak bone mass is directly related to the level of physical activity prior to peak bone mass; the higher the peak bone mass, the lower the risk of osteoporosis.
- An above-average level of physical activity after peak bone mass will delay the onset of bone loss.
- An above-average level of physical activity after peak bone mass will reduce the rate of bone loss.
Case study 2 discusses whether regular exercise can be used to prevent falls in osteopenic women.
Case Study 2 Using Exercise to Prevent Falls in Osteopenic Women
Hourigan SR, Nitz JC, Brauer S, O'Neill S, Wong J, Richardson CA. 2008. Positive effects of exercise on falls and fracture risk in osteopenic women. Osteoporosis International 19:1077-1086.
The incidence of bone fractures increases with age. As the number of aged people worldwide is increasing, so is the total number of fractures in the aged population (age 65 years and older). Fractures in the aged population are a major health care cost and risk factor for permanent disability and death. Consequently, reducing the risk of fractures in the aged population is a challenge in many countries.
Physical trauma (in particular, falls) and weak bones (due to osteopenia or osteoporosis) are the major causes of fractures in the aged population. Poor balance and weak muscles are risk factors for falls. Osteopenia is defined as bone mineral density (BMD) between 1 and 2.5 standard deviations below the average for young women. Osteoporosis is defined as BMD more than 2.5 standard deviations below the average for young women.
Recent research indicates that muscle strength, bone strength, and balance in the aged population can be improved through properly prescribed physical activity training programs based on resistance exercises involving strength-training machines. The purpose of the present study was to determine the effect of a physical activity program based on weight-bearing activities (rather than strength-training machines) on balance, muscle strength, and bone mineral density in osteopenic women.
Ninety-eight community-dwelling (living more or less independently in their own homes) osteopenic women (age 62.01 ± 8.9; range 41-78 years) were randomly assigned to either a control group (n = 48: no intervention) or an exercise group (n = 50: two 1 hr exercise sessions per week for 20 weeks directed by a trained physiotherapist). Assessments at baseline and post intervention included balance (five measures), strength (quadriceps; hip abductors, adductors, and external rotators; trunk extensors), and BMD (proximal femur and lumbar spine). Baseline assessment showed no significant differences between the exercise and control groups in terms of balance, strength, BMD, or demographics.
The average number of sessions attended by the 42 members of the exercise group who completed the exercise program was 28.2 of a possible 40 sessions (71.2%). Following the intervention, the exercise group showed significantly better performance than the control group in 9 of 11 balance tests (ranging from 10% to 71% better performance) and 7 of 9 strength tests (ranging from 9% to 23% better performance). BMD of the exercise group increased but was not significantly greater than in the control group.
Application
A specific, well-directed program of weight-bearing exercises in a workstation format that emphasizes interaction, discussion, and enjoyment can significantly improve balance and strength in osteopenic women, which in turn is likely to reduce the risk of falling. This type of training may also positively influence BMD, but further research is needed.
Youth sports increase risk of physeal injury
Widespread participation in youth sports increase the risk of physeal injury, resulting in more permanent problems
Case Study 1 Physeal Injuries in Youth Sports
Caine D, DiFiori J, Maffulli N. 2006. Physeal injuries in children's and youth sports: Reasons for concern? British Journal of Sports Medicine 40:749-760.
Participation in children's and youth sports is widespread in Western culture. Many children start year-round training and specialization by 9 years of age. Preteens training at regional centers or with high school and club teams in sports such as gymnastics may train more than 20 hr per week. There is increasing concern, especially among physicians, that the frequency and intensity of training and competition experienced by many participants in children's and youth sports are putting them at risk of serious physeal injury (epiphyseal and apophyseal), which may result in permanent skeletal abnormalities. Unfortunately, detailed information, based on the use of standardized recording systems applied over a long period, on the epidemiology of injuries (incidence, location, type, diagnosis, severity) sustained by participants in children's and youth sports is not available for any sport. The purpose of this study was to systematically review the literature on the frequency and characteristics of physeal injuries in children's and youth sports.
The review was undertaken using Medline and SPORTdiscus. More than 150 reports were obtained, largely case reports or case series investigations. The authors used the reports to determine the number, location, type, diagnosis, and severity of physeal injuries that occur in different sports, but it was not possible to calculate incidence of injury because information was not provided on the total number of participants and exposure time of participants in the various sports.
The review indicates that acute physeal injuries (sudden widening or fracture along or through an epiphyseal or apophyseal plate accompanied by considerable pain) and chronic physeal injuries (progressive widening of an epiphyseal or apophyseal plate associated with a progressive increase in pain, especially during exercise) occur frequently in some sports, including football, baseball, gymnastics, basketball, volleyball, judo, weightlifting, soccer, rugby, tennis, cricket, and long-distance running. The main regions of physeal injuries are the shoulder, elbow, wrist, and knee. Most of the injuries are chronic, and most resolve without complication. However, there are several reports of premature partial or complete physeal closure.
The authors express a number of concerns with current practice, in particular, the paucity of epidemiological data on the distribution and determinants of physeal injuries in children's and youth sports and the apparent lack of knowledge on the part of many coaches of children's and youth sports regarding musculoskeletal growth and development in children in general and physeal injuries in particular.
Application
Coaches should consider the following strategies to reduce the incidence of physeal injuries in children's and youth sports:
- Individualize fitness training and practice for athletes experiencing rapid growth. Assess growth rate by monitoring increases in height and limb segment lengths.
- Use a variety of training and practice drills and avoid excessive volume of training.
- For collision sports, ensure that competition is based on physical maturity rather than chronological age.
- Mandate regular medical assessment to ensure early diagnosis and treatment of epiphyseal and apophyseal plate disorders.
Structure of the knee facilitates extension and flexion
Learn more about the tibiofemoral joint and the ligaments
Capsule of the Knee
The tibiofemoral and patellofemoral joints share a common capsule that has a complicated shape. The capsule is attached above to the femur, below to the tibia, and anteriorly to the patella (figure 6.13). To accommodate the extremes of full flexion and full extension of the tibiofemoral joint, the anterior part of the capsule is folded upward during extension and the posterior part of the capsule is folded downward during flexion. The upward fold, only present in extension, is referred to as the suprapatellar bursa (figure 6.13). The suprapatellar bursa intervenes between the quadriceps tendon and the anterior aspect of the femur just proximal to the patellar surface.
Figure 6.13 Sagittal section through the knee complex showing the shape of the capsule in extension.
The downward fold, only present during flexion, is referred to as the gastrocnemius bursa. The gastrocnemius bursa intervenes between the posterior aspect of the tibial condyles and the gastrocnemius muscle. In general, a bursa is a flattened sac of synovial membrane containing synovial fluid. Bursas minimize friction between structures that slide across each other during normal movement (see chapter 7).
During flexion of the tibiofemoral joint, the suprapatellar bursa becomes progressively smaller and the gastrocnemius bursa becomes progressively larger as synovial fluid is redistributed from the suprapatellar bursa to the gastrocnemius bursa. The movement of synovial fluid is reversed during extension of the tibiofemoral joint; that is, the gastrocnemius bursa becomes progressively smaller and the suprapatellar bursa becomes progressively larger.
The suprapatellar bursa is separated from the femur by a pad of fat called the suprapatellar fat pad. Lying in the space bounded by the upper two thirds of the posterior aspect of the patellar ligament, the anterior intercondylar area of the tibia, and the anterior inferior aspect of the articular surface of the femoral condyles is a pad of fat called the infrapatellar fat pad. It is roughly triangular in sagittal cross section and is suspended superiorly from a fibro-adipose band called the infrapatellar fold. The infrapatellar fold is attached anteriorly to the inferior pole of the patella and posteriorly to the anterior border of the intercondylar notch (figure 6.13). The infrapatellar fat pad is attached anteriorly to the posterior aspect of the patellar ligament and extends at both sides of the patellar ligament. The infrapatellar fat pad also extends narrow branches halfway up each side of the patella; the branches are referred to as alar folds (alar = winglike). The infrapatellar fat pad cushions the patellar ligament and lower part of the patella during movements of the knee.
Knee Ligaments
Four extracapsular ligaments support the tibiofemoral joint. The lateral ligament (also referred to as the lateral collateral ligament and the fibular collateral ligament) is attached superiorly to the lateral epicondyle of the femur and inferiorly to the head of the fibula (figure 6.14a). The medial ligament (also referred to as the medial collateral ligament and the tibial collateral ligament) is attached superiorly to the medial epicondyle of the femur and inferiorly to the medial aspect of the tibia below the tibial condyle (figure 6.14b). The posterior fibers of the medial ligament blend with the joint capsule at the level of the medial meniscus and thus the medial ligament is not completely extracapsular. The arrangement of the medial and lateral ligaments and the curvature of the femoral condyles are such that both ligaments are relatively slack when the knee is flexed but become progressively more taut as the joint extends. In a normal joint the ligaments are fully taut when the joint is fully extended. In this position of the joint both ligaments help to prevent hyperextension and lateral rotation of the tibia relative to the femur. With the knee fully extended, the range of abduction and adduction is normally zero. Because the medial and lateral ligaments are relatively slack when the knee is flexed, a certain amount of axial rotation and abduction and adduction of the lower leg can occur when the knee is in a flexed, non-weight-bearing position. For example, when a person is sitting on a table with his lower leg hanging freely, the ranges of internal and external rotation are normally around 30° and 40°, respectively (Norkin and Levangie 1992). However, the ranges of abduction and adduction are normally very small, approximately 2° to 5°.
Figure 6.14 Location of the main ligaments of the left knee. (a) Lateral aspect. (b) Medial aspect.
Injuries to the lateral and, in particular, the medial ligaments are common in sports (Reider 1996). The classic cause of medial ligament injury is a blow to the lateral aspect of the knee while the foot in contact with the ground, resulting in abduction of the knee. This situation is common in sports such as American football, soccer, and rugby. The excessive loading on the medial ligament in such situations can result in serious injury (Indelicato 1995). Medial ligament injuries of a less severe but nonetheless persistent nature are common in swimmers, especially breaststroke swimmers. The whip-kick leg action in breaststroke tends to simultaneously abduct and laterally rotate (tibia with respect to femur) the knee, resulting in strain of the medial ligament and associated medial supporting structures (Vizsolyi et al 1987).
Physical activity helps reduce bone loss
Bone loss begins around age 45 – 50 and moves a at different rates during different phases
Porosity, Osteopenia, and Osteoporosis
Because of the channels and spaces within compact and cancellous bone, any particular region of a bone consists of certain amounts of bone tissue and nonbone tissue. The term porosity describes the proportion of nonbone tissue. At skeletal maturity the porosity of compact and cancellous bone is approximately 2% and 50%, respectively; the density (amount of bone tissue per unit volume) of compact bone is approximately double that of cancellous bone (Radin 1984, Tortora 2004). The density of bone tissue depends on the degree of mineralization. During ossification, the degree of mineralization of bone tissue gradually increases and reaches a maximum level at skeletal maturity (Bailey et al 1986). However, the amount of bone within the skeleton may continue to increase for 5 to 10 years after skeletal maturity, especially in people who are physically active (Stillman et al 1986, Talmage and Anderson 1984, Frost 2003). Consequently, bone mass peaks in males and females between 25 and 30 years of age. In terms of turnover, this means that from skeletal maturity to the age at which peak bone mass occurs, more new bone is formed than old and damaged bone is absorbed.
Following peak bone mass there is usually a stable period in which the amount of bone in the skeleton remains about the same; there is a balance between bone absorption and bone formation. This stable period is followed by a gradual decrease in bone mass for the rest of the person's life; the rate of bone absorption exceeds the rate of bone formation. Bone mass is the product of bone volume and bone density. The loss in bone mass that occurs with age following peak bone mass is the result of decreases in bone volume and bone density. Osteopenia refers to a level of bone density below the normal level for a person's age and sex (Bailey 1995, Frost 1997).
Bone mass starts to decrease earlier and at a greater rate in females than in males. In males, bone loss normally starts between 45 and 50 years of age and proceeds at a rate of 0.4% to 0.75% per year (Bailey et al 1986, Smith 1982). In females, bone loss has three phases. The first phase starts around 30 to 35 years of age and proceeds at a rate of 0.75% to 1% per year until menopause. From menopause until about 5 years after menopause, the rate of bone loss increases to between 2% and 3% per year. During the final phase, the rate of bone loss is approximately 1% per year. Thus, women may lose, on average, about 53% of their peak bone mass by the age of 80 years. In contrast, males may lose, on average, about 18% of their peak bone mass by the age of 80 years (figure 3.32).
Even though body weight tends to decrease with age, the rate of bone loss is usually much greater than the rate at which body weight decreases. Consequently, the effect of bone loss is that the bones, especially weight-bearing bones, become progressively weaker relative to the weight of the rest of the body. In addition to gradually losing strength, the bones also gradually lose their elasticity and become more brittle. In some people, especially women, a loss of bone mass and elasticity is eventually reached when some bones are no longer able to withstand the loads imposed by normal habitual activity. These bones become very susceptible to fracture. This condition, the most common bone disorder in elderly people, is called osteoporosis (Bailey et al 1986, Ferretti et al 2003). Osteoporosis may cause severe disfigurement, especially of the trunk, as a result of fractured or crushed vertebrae. Many deaths in elderly people are due to complications arising from bone fractures that occur as a result of osteoporosis (Kaplan 1983, Kado et al 1999, Cummings and Melton 2002).
Bone loss tends to occur earlier and to proceed at a faster rate in cancellous bone than in compact bone (Bailey et al 1986, Ferretti et al 2003). Consequently, regions of bones with a high proportion of cancellous bone, such as the bodies of the vertebrae, the head and neck of the femur, and the distal end of the radius, are particularly vulnerable to osteoporosis and fracture in elderly people. This vulnerability is reflected in studies that report a rapid increase in the incidence of bone fractures with age, especially in women (Bauer 1960, Chalmers and Ho 1970, Hagino et al 1991, Cummings et al 1993, Court-Brown and Caesar 2006). The results of one study showed that the incidence of fracture to the distal end of the radius was seven times higher in 54-year-old women than in 40-year-old women (Bauer 1960). In another study the incidence of fracture of the neck of the femur was found to be 50 times higher in 70-year-old women than in 40-year-old women (Chalmers and Ho 1970). Bone loss in compact bone occurs mainly on the endosteal surface so that bone width remains relatively unchanged into old age (Smith 1982, Ferretti et al 2003).
Although the cause of osteoporosis is not clear, there is general agreement that four variables are mainly responsible: genetic factors, endocrine status, nutritional factors, and physical activity (Bailey et al 1986, MacKinnon 1988, Ferretti et al 2003). The relative contribution of these variables has not been established, but physical activity seems to be the most important. In the absence of weight-bearing activity, no amount of endocrine or nutritional intervention will prevent rapid bone loss; there must be mechanical stress (Bailey et al 1986, Ferretti et al 2003). Research suggests that regular physical activity throughout life, within the moderate overload range (see chapter 11), can help to prevent osteoporosis in three ways (Bailey 1995, Greene and Naughton 2006, Baxter-Jones et al 2008):
- Peak bone mass is directly related to the level of physical activity prior to peak bone mass; the higher the peak bone mass, the lower the risk of osteoporosis.
- An above-average level of physical activity after peak bone mass will delay the onset of bone loss.
- An above-average level of physical activity after peak bone mass will reduce the rate of bone loss.
Case study 2 discusses whether regular exercise can be used to prevent falls in osteopenic women.
Case Study 2 Using Exercise to Prevent Falls in Osteopenic Women
Hourigan SR, Nitz JC, Brauer S, O'Neill S, Wong J, Richardson CA. 2008. Positive effects of exercise on falls and fracture risk in osteopenic women. Osteoporosis International 19:1077-1086.
The incidence of bone fractures increases with age. As the number of aged people worldwide is increasing, so is the total number of fractures in the aged population (age 65 years and older). Fractures in the aged population are a major health care cost and risk factor for permanent disability and death. Consequently, reducing the risk of fractures in the aged population is a challenge in many countries.
Physical trauma (in particular, falls) and weak bones (due to osteopenia or osteoporosis) are the major causes of fractures in the aged population. Poor balance and weak muscles are risk factors for falls. Osteopenia is defined as bone mineral density (BMD) between 1 and 2.5 standard deviations below the average for young women. Osteoporosis is defined as BMD more than 2.5 standard deviations below the average for young women.
Recent research indicates that muscle strength, bone strength, and balance in the aged population can be improved through properly prescribed physical activity training programs based on resistance exercises involving strength-training machines. The purpose of the present study was to determine the effect of a physical activity program based on weight-bearing activities (rather than strength-training machines) on balance, muscle strength, and bone mineral density in osteopenic women.
Ninety-eight community-dwelling (living more or less independently in their own homes) osteopenic women (age 62.01 ± 8.9; range 41-78 years) were randomly assigned to either a control group (n = 48: no intervention) or an exercise group (n = 50: two 1 hr exercise sessions per week for 20 weeks directed by a trained physiotherapist). Assessments at baseline and post intervention included balance (five measures), strength (quadriceps; hip abductors, adductors, and external rotators; trunk extensors), and BMD (proximal femur and lumbar spine). Baseline assessment showed no significant differences between the exercise and control groups in terms of balance, strength, BMD, or demographics.
The average number of sessions attended by the 42 members of the exercise group who completed the exercise program was 28.2 of a possible 40 sessions (71.2%). Following the intervention, the exercise group showed significantly better performance than the control group in 9 of 11 balance tests (ranging from 10% to 71% better performance) and 7 of 9 strength tests (ranging from 9% to 23% better performance). BMD of the exercise group increased but was not significantly greater than in the control group.
Application
A specific, well-directed program of weight-bearing exercises in a workstation format that emphasizes interaction, discussion, and enjoyment can significantly improve balance and strength in osteopenic women, which in turn is likely to reduce the risk of falling. This type of training may also positively influence BMD, but further research is needed.
Youth sports increase risk of physeal injury
Widespread participation in youth sports increase the risk of physeal injury, resulting in more permanent problems
Case Study 1 Physeal Injuries in Youth Sports
Caine D, DiFiori J, Maffulli N. 2006. Physeal injuries in children's and youth sports: Reasons for concern? British Journal of Sports Medicine 40:749-760.
Participation in children's and youth sports is widespread in Western culture. Many children start year-round training and specialization by 9 years of age. Preteens training at regional centers or with high school and club teams in sports such as gymnastics may train more than 20 hr per week. There is increasing concern, especially among physicians, that the frequency and intensity of training and competition experienced by many participants in children's and youth sports are putting them at risk of serious physeal injury (epiphyseal and apophyseal), which may result in permanent skeletal abnormalities. Unfortunately, detailed information, based on the use of standardized recording systems applied over a long period, on the epidemiology of injuries (incidence, location, type, diagnosis, severity) sustained by participants in children's and youth sports is not available for any sport. The purpose of this study was to systematically review the literature on the frequency and characteristics of physeal injuries in children's and youth sports.
The review was undertaken using Medline and SPORTdiscus. More than 150 reports were obtained, largely case reports or case series investigations. The authors used the reports to determine the number, location, type, diagnosis, and severity of physeal injuries that occur in different sports, but it was not possible to calculate incidence of injury because information was not provided on the total number of participants and exposure time of participants in the various sports.
The review indicates that acute physeal injuries (sudden widening or fracture along or through an epiphyseal or apophyseal plate accompanied by considerable pain) and chronic physeal injuries (progressive widening of an epiphyseal or apophyseal plate associated with a progressive increase in pain, especially during exercise) occur frequently in some sports, including football, baseball, gymnastics, basketball, volleyball, judo, weightlifting, soccer, rugby, tennis, cricket, and long-distance running. The main regions of physeal injuries are the shoulder, elbow, wrist, and knee. Most of the injuries are chronic, and most resolve without complication. However, there are several reports of premature partial or complete physeal closure.
The authors express a number of concerns with current practice, in particular, the paucity of epidemiological data on the distribution and determinants of physeal injuries in children's and youth sports and the apparent lack of knowledge on the part of many coaches of children's and youth sports regarding musculoskeletal growth and development in children in general and physeal injuries in particular.
Application
Coaches should consider the following strategies to reduce the incidence of physeal injuries in children's and youth sports:
- Individualize fitness training and practice for athletes experiencing rapid growth. Assess growth rate by monitoring increases in height and limb segment lengths.
- Use a variety of training and practice drills and avoid excessive volume of training.
- For collision sports, ensure that competition is based on physical maturity rather than chronological age.
- Mandate regular medical assessment to ensure early diagnosis and treatment of epiphyseal and apophyseal plate disorders.
Structure of the knee facilitates extension and flexion
Learn more about the tibiofemoral joint and the ligaments
Capsule of the Knee
The tibiofemoral and patellofemoral joints share a common capsule that has a complicated shape. The capsule is attached above to the femur, below to the tibia, and anteriorly to the patella (figure 6.13). To accommodate the extremes of full flexion and full extension of the tibiofemoral joint, the anterior part of the capsule is folded upward during extension and the posterior part of the capsule is folded downward during flexion. The upward fold, only present in extension, is referred to as the suprapatellar bursa (figure 6.13). The suprapatellar bursa intervenes between the quadriceps tendon and the anterior aspect of the femur just proximal to the patellar surface.
Figure 6.13 Sagittal section through the knee complex showing the shape of the capsule in extension.
The downward fold, only present during flexion, is referred to as the gastrocnemius bursa. The gastrocnemius bursa intervenes between the posterior aspect of the tibial condyles and the gastrocnemius muscle. In general, a bursa is a flattened sac of synovial membrane containing synovial fluid. Bursas minimize friction between structures that slide across each other during normal movement (see chapter 7).
During flexion of the tibiofemoral joint, the suprapatellar bursa becomes progressively smaller and the gastrocnemius bursa becomes progressively larger as synovial fluid is redistributed from the suprapatellar bursa to the gastrocnemius bursa. The movement of synovial fluid is reversed during extension of the tibiofemoral joint; that is, the gastrocnemius bursa becomes progressively smaller and the suprapatellar bursa becomes progressively larger.
The suprapatellar bursa is separated from the femur by a pad of fat called the suprapatellar fat pad. Lying in the space bounded by the upper two thirds of the posterior aspect of the patellar ligament, the anterior intercondylar area of the tibia, and the anterior inferior aspect of the articular surface of the femoral condyles is a pad of fat called the infrapatellar fat pad. It is roughly triangular in sagittal cross section and is suspended superiorly from a fibro-adipose band called the infrapatellar fold. The infrapatellar fold is attached anteriorly to the inferior pole of the patella and posteriorly to the anterior border of the intercondylar notch (figure 6.13). The infrapatellar fat pad is attached anteriorly to the posterior aspect of the patellar ligament and extends at both sides of the patellar ligament. The infrapatellar fat pad also extends narrow branches halfway up each side of the patella; the branches are referred to as alar folds (alar = winglike). The infrapatellar fat pad cushions the patellar ligament and lower part of the patella during movements of the knee.
Knee Ligaments
Four extracapsular ligaments support the tibiofemoral joint. The lateral ligament (also referred to as the lateral collateral ligament and the fibular collateral ligament) is attached superiorly to the lateral epicondyle of the femur and inferiorly to the head of the fibula (figure 6.14a). The medial ligament (also referred to as the medial collateral ligament and the tibial collateral ligament) is attached superiorly to the medial epicondyle of the femur and inferiorly to the medial aspect of the tibia below the tibial condyle (figure 6.14b). The posterior fibers of the medial ligament blend with the joint capsule at the level of the medial meniscus and thus the medial ligament is not completely extracapsular. The arrangement of the medial and lateral ligaments and the curvature of the femoral condyles are such that both ligaments are relatively slack when the knee is flexed but become progressively more taut as the joint extends. In a normal joint the ligaments are fully taut when the joint is fully extended. In this position of the joint both ligaments help to prevent hyperextension and lateral rotation of the tibia relative to the femur. With the knee fully extended, the range of abduction and adduction is normally zero. Because the medial and lateral ligaments are relatively slack when the knee is flexed, a certain amount of axial rotation and abduction and adduction of the lower leg can occur when the knee is in a flexed, non-weight-bearing position. For example, when a person is sitting on a table with his lower leg hanging freely, the ranges of internal and external rotation are normally around 30° and 40°, respectively (Norkin and Levangie 1992). However, the ranges of abduction and adduction are normally very small, approximately 2° to 5°.
Figure 6.14 Location of the main ligaments of the left knee. (a) Lateral aspect. (b) Medial aspect.
Injuries to the lateral and, in particular, the medial ligaments are common in sports (Reider 1996). The classic cause of medial ligament injury is a blow to the lateral aspect of the knee while the foot in contact with the ground, resulting in abduction of the knee. This situation is common in sports such as American football, soccer, and rugby. The excessive loading on the medial ligament in such situations can result in serious injury (Indelicato 1995). Medial ligament injuries of a less severe but nonetheless persistent nature are common in swimmers, especially breaststroke swimmers. The whip-kick leg action in breaststroke tends to simultaneously abduct and laterally rotate (tibia with respect to femur) the knee, resulting in strain of the medial ligament and associated medial supporting structures (Vizsolyi et al 1987).
Physical activity helps reduce bone loss
Bone loss begins around age 45 – 50 and moves a at different rates during different phases
Porosity, Osteopenia, and Osteoporosis
Because of the channels and spaces within compact and cancellous bone, any particular region of a bone consists of certain amounts of bone tissue and nonbone tissue. The term porosity describes the proportion of nonbone tissue. At skeletal maturity the porosity of compact and cancellous bone is approximately 2% and 50%, respectively; the density (amount of bone tissue per unit volume) of compact bone is approximately double that of cancellous bone (Radin 1984, Tortora 2004). The density of bone tissue depends on the degree of mineralization. During ossification, the degree of mineralization of bone tissue gradually increases and reaches a maximum level at skeletal maturity (Bailey et al 1986). However, the amount of bone within the skeleton may continue to increase for 5 to 10 years after skeletal maturity, especially in people who are physically active (Stillman et al 1986, Talmage and Anderson 1984, Frost 2003). Consequently, bone mass peaks in males and females between 25 and 30 years of age. In terms of turnover, this means that from skeletal maturity to the age at which peak bone mass occurs, more new bone is formed than old and damaged bone is absorbed.
Following peak bone mass there is usually a stable period in which the amount of bone in the skeleton remains about the same; there is a balance between bone absorption and bone formation. This stable period is followed by a gradual decrease in bone mass for the rest of the person's life; the rate of bone absorption exceeds the rate of bone formation. Bone mass is the product of bone volume and bone density. The loss in bone mass that occurs with age following peak bone mass is the result of decreases in bone volume and bone density. Osteopenia refers to a level of bone density below the normal level for a person's age and sex (Bailey 1995, Frost 1997).
Bone mass starts to decrease earlier and at a greater rate in females than in males. In males, bone loss normally starts between 45 and 50 years of age and proceeds at a rate of 0.4% to 0.75% per year (Bailey et al 1986, Smith 1982). In females, bone loss has three phases. The first phase starts around 30 to 35 years of age and proceeds at a rate of 0.75% to 1% per year until menopause. From menopause until about 5 years after menopause, the rate of bone loss increases to between 2% and 3% per year. During the final phase, the rate of bone loss is approximately 1% per year. Thus, women may lose, on average, about 53% of their peak bone mass by the age of 80 years. In contrast, males may lose, on average, about 18% of their peak bone mass by the age of 80 years (figure 3.32).
Even though body weight tends to decrease with age, the rate of bone loss is usually much greater than the rate at which body weight decreases. Consequently, the effect of bone loss is that the bones, especially weight-bearing bones, become progressively weaker relative to the weight of the rest of the body. In addition to gradually losing strength, the bones also gradually lose their elasticity and become more brittle. In some people, especially women, a loss of bone mass and elasticity is eventually reached when some bones are no longer able to withstand the loads imposed by normal habitual activity. These bones become very susceptible to fracture. This condition, the most common bone disorder in elderly people, is called osteoporosis (Bailey et al 1986, Ferretti et al 2003). Osteoporosis may cause severe disfigurement, especially of the trunk, as a result of fractured or crushed vertebrae. Many deaths in elderly people are due to complications arising from bone fractures that occur as a result of osteoporosis (Kaplan 1983, Kado et al 1999, Cummings and Melton 2002).
Bone loss tends to occur earlier and to proceed at a faster rate in cancellous bone than in compact bone (Bailey et al 1986, Ferretti et al 2003). Consequently, regions of bones with a high proportion of cancellous bone, such as the bodies of the vertebrae, the head and neck of the femur, and the distal end of the radius, are particularly vulnerable to osteoporosis and fracture in elderly people. This vulnerability is reflected in studies that report a rapid increase in the incidence of bone fractures with age, especially in women (Bauer 1960, Chalmers and Ho 1970, Hagino et al 1991, Cummings et al 1993, Court-Brown and Caesar 2006). The results of one study showed that the incidence of fracture to the distal end of the radius was seven times higher in 54-year-old women than in 40-year-old women (Bauer 1960). In another study the incidence of fracture of the neck of the femur was found to be 50 times higher in 70-year-old women than in 40-year-old women (Chalmers and Ho 1970). Bone loss in compact bone occurs mainly on the endosteal surface so that bone width remains relatively unchanged into old age (Smith 1982, Ferretti et al 2003).
Although the cause of osteoporosis is not clear, there is general agreement that four variables are mainly responsible: genetic factors, endocrine status, nutritional factors, and physical activity (Bailey et al 1986, MacKinnon 1988, Ferretti et al 2003). The relative contribution of these variables has not been established, but physical activity seems to be the most important. In the absence of weight-bearing activity, no amount of endocrine or nutritional intervention will prevent rapid bone loss; there must be mechanical stress (Bailey et al 1986, Ferretti et al 2003). Research suggests that regular physical activity throughout life, within the moderate overload range (see chapter 11), can help to prevent osteoporosis in three ways (Bailey 1995, Greene and Naughton 2006, Baxter-Jones et al 2008):
- Peak bone mass is directly related to the level of physical activity prior to peak bone mass; the higher the peak bone mass, the lower the risk of osteoporosis.
- An above-average level of physical activity after peak bone mass will delay the onset of bone loss.
- An above-average level of physical activity after peak bone mass will reduce the rate of bone loss.
Case study 2 discusses whether regular exercise can be used to prevent falls in osteopenic women.
Case Study 2 Using Exercise to Prevent Falls in Osteopenic Women
Hourigan SR, Nitz JC, Brauer S, O'Neill S, Wong J, Richardson CA. 2008. Positive effects of exercise on falls and fracture risk in osteopenic women. Osteoporosis International 19:1077-1086.
The incidence of bone fractures increases with age. As the number of aged people worldwide is increasing, so is the total number of fractures in the aged population (age 65 years and older). Fractures in the aged population are a major health care cost and risk factor for permanent disability and death. Consequently, reducing the risk of fractures in the aged population is a challenge in many countries.
Physical trauma (in particular, falls) and weak bones (due to osteopenia or osteoporosis) are the major causes of fractures in the aged population. Poor balance and weak muscles are risk factors for falls. Osteopenia is defined as bone mineral density (BMD) between 1 and 2.5 standard deviations below the average for young women. Osteoporosis is defined as BMD more than 2.5 standard deviations below the average for young women.
Recent research indicates that muscle strength, bone strength, and balance in the aged population can be improved through properly prescribed physical activity training programs based on resistance exercises involving strength-training machines. The purpose of the present study was to determine the effect of a physical activity program based on weight-bearing activities (rather than strength-training machines) on balance, muscle strength, and bone mineral density in osteopenic women.
Ninety-eight community-dwelling (living more or less independently in their own homes) osteopenic women (age 62.01 ± 8.9; range 41-78 years) were randomly assigned to either a control group (n = 48: no intervention) or an exercise group (n = 50: two 1 hr exercise sessions per week for 20 weeks directed by a trained physiotherapist). Assessments at baseline and post intervention included balance (five measures), strength (quadriceps; hip abductors, adductors, and external rotators; trunk extensors), and BMD (proximal femur and lumbar spine). Baseline assessment showed no significant differences between the exercise and control groups in terms of balance, strength, BMD, or demographics.
The average number of sessions attended by the 42 members of the exercise group who completed the exercise program was 28.2 of a possible 40 sessions (71.2%). Following the intervention, the exercise group showed significantly better performance than the control group in 9 of 11 balance tests (ranging from 10% to 71% better performance) and 7 of 9 strength tests (ranging from 9% to 23% better performance). BMD of the exercise group increased but was not significantly greater than in the control group.
Application
A specific, well-directed program of weight-bearing exercises in a workstation format that emphasizes interaction, discussion, and enjoyment can significantly improve balance and strength in osteopenic women, which in turn is likely to reduce the risk of falling. This type of training may also positively influence BMD, but further research is needed.
Youth sports increase risk of physeal injury
Widespread participation in youth sports increase the risk of physeal injury, resulting in more permanent problems
Case Study 1 Physeal Injuries in Youth Sports
Caine D, DiFiori J, Maffulli N. 2006. Physeal injuries in children's and youth sports: Reasons for concern? British Journal of Sports Medicine 40:749-760.
Participation in children's and youth sports is widespread in Western culture. Many children start year-round training and specialization by 9 years of age. Preteens training at regional centers or with high school and club teams in sports such as gymnastics may train more than 20 hr per week. There is increasing concern, especially among physicians, that the frequency and intensity of training and competition experienced by many participants in children's and youth sports are putting them at risk of serious physeal injury (epiphyseal and apophyseal), which may result in permanent skeletal abnormalities. Unfortunately, detailed information, based on the use of standardized recording systems applied over a long period, on the epidemiology of injuries (incidence, location, type, diagnosis, severity) sustained by participants in children's and youth sports is not available for any sport. The purpose of this study was to systematically review the literature on the frequency and characteristics of physeal injuries in children's and youth sports.
The review was undertaken using Medline and SPORTdiscus. More than 150 reports were obtained, largely case reports or case series investigations. The authors used the reports to determine the number, location, type, diagnosis, and severity of physeal injuries that occur in different sports, but it was not possible to calculate incidence of injury because information was not provided on the total number of participants and exposure time of participants in the various sports.
The review indicates that acute physeal injuries (sudden widening or fracture along or through an epiphyseal or apophyseal plate accompanied by considerable pain) and chronic physeal injuries (progressive widening of an epiphyseal or apophyseal plate associated with a progressive increase in pain, especially during exercise) occur frequently in some sports, including football, baseball, gymnastics, basketball, volleyball, judo, weightlifting, soccer, rugby, tennis, cricket, and long-distance running. The main regions of physeal injuries are the shoulder, elbow, wrist, and knee. Most of the injuries are chronic, and most resolve without complication. However, there are several reports of premature partial or complete physeal closure.
The authors express a number of concerns with current practice, in particular, the paucity of epidemiological data on the distribution and determinants of physeal injuries in children's and youth sports and the apparent lack of knowledge on the part of many coaches of children's and youth sports regarding musculoskeletal growth and development in children in general and physeal injuries in particular.
Application
Coaches should consider the following strategies to reduce the incidence of physeal injuries in children's and youth sports:
- Individualize fitness training and practice for athletes experiencing rapid growth. Assess growth rate by monitoring increases in height and limb segment lengths.
- Use a variety of training and practice drills and avoid excessive volume of training.
- For collision sports, ensure that competition is based on physical maturity rather than chronological age.
- Mandate regular medical assessment to ensure early diagnosis and treatment of epiphyseal and apophyseal plate disorders.
Structure of the knee facilitates extension and flexion
Learn more about the tibiofemoral joint and the ligaments
Capsule of the Knee
The tibiofemoral and patellofemoral joints share a common capsule that has a complicated shape. The capsule is attached above to the femur, below to the tibia, and anteriorly to the patella (figure 6.13). To accommodate the extremes of full flexion and full extension of the tibiofemoral joint, the anterior part of the capsule is folded upward during extension and the posterior part of the capsule is folded downward during flexion. The upward fold, only present in extension, is referred to as the suprapatellar bursa (figure 6.13). The suprapatellar bursa intervenes between the quadriceps tendon and the anterior aspect of the femur just proximal to the patellar surface.
Figure 6.13 Sagittal section through the knee complex showing the shape of the capsule in extension.
The downward fold, only present during flexion, is referred to as the gastrocnemius bursa. The gastrocnemius bursa intervenes between the posterior aspect of the tibial condyles and the gastrocnemius muscle. In general, a bursa is a flattened sac of synovial membrane containing synovial fluid. Bursas minimize friction between structures that slide across each other during normal movement (see chapter 7).
During flexion of the tibiofemoral joint, the suprapatellar bursa becomes progressively smaller and the gastrocnemius bursa becomes progressively larger as synovial fluid is redistributed from the suprapatellar bursa to the gastrocnemius bursa. The movement of synovial fluid is reversed during extension of the tibiofemoral joint; that is, the gastrocnemius bursa becomes progressively smaller and the suprapatellar bursa becomes progressively larger.
The suprapatellar bursa is separated from the femur by a pad of fat called the suprapatellar fat pad. Lying in the space bounded by the upper two thirds of the posterior aspect of the patellar ligament, the anterior intercondylar area of the tibia, and the anterior inferior aspect of the articular surface of the femoral condyles is a pad of fat called the infrapatellar fat pad. It is roughly triangular in sagittal cross section and is suspended superiorly from a fibro-adipose band called the infrapatellar fold. The infrapatellar fold is attached anteriorly to the inferior pole of the patella and posteriorly to the anterior border of the intercondylar notch (figure 6.13). The infrapatellar fat pad is attached anteriorly to the posterior aspect of the patellar ligament and extends at both sides of the patellar ligament. The infrapatellar fat pad also extends narrow branches halfway up each side of the patella; the branches are referred to as alar folds (alar = winglike). The infrapatellar fat pad cushions the patellar ligament and lower part of the patella during movements of the knee.
Knee Ligaments
Four extracapsular ligaments support the tibiofemoral joint. The lateral ligament (also referred to as the lateral collateral ligament and the fibular collateral ligament) is attached superiorly to the lateral epicondyle of the femur and inferiorly to the head of the fibula (figure 6.14a). The medial ligament (also referred to as the medial collateral ligament and the tibial collateral ligament) is attached superiorly to the medial epicondyle of the femur and inferiorly to the medial aspect of the tibia below the tibial condyle (figure 6.14b). The posterior fibers of the medial ligament blend with the joint capsule at the level of the medial meniscus and thus the medial ligament is not completely extracapsular. The arrangement of the medial and lateral ligaments and the curvature of the femoral condyles are such that both ligaments are relatively slack when the knee is flexed but become progressively more taut as the joint extends. In a normal joint the ligaments are fully taut when the joint is fully extended. In this position of the joint both ligaments help to prevent hyperextension and lateral rotation of the tibia relative to the femur. With the knee fully extended, the range of abduction and adduction is normally zero. Because the medial and lateral ligaments are relatively slack when the knee is flexed, a certain amount of axial rotation and abduction and adduction of the lower leg can occur when the knee is in a flexed, non-weight-bearing position. For example, when a person is sitting on a table with his lower leg hanging freely, the ranges of internal and external rotation are normally around 30° and 40°, respectively (Norkin and Levangie 1992). However, the ranges of abduction and adduction are normally very small, approximately 2° to 5°.
Figure 6.14 Location of the main ligaments of the left knee. (a) Lateral aspect. (b) Medial aspect.
Injuries to the lateral and, in particular, the medial ligaments are common in sports (Reider 1996). The classic cause of medial ligament injury is a blow to the lateral aspect of the knee while the foot in contact with the ground, resulting in abduction of the knee. This situation is common in sports such as American football, soccer, and rugby. The excessive loading on the medial ligament in such situations can result in serious injury (Indelicato 1995). Medial ligament injuries of a less severe but nonetheless persistent nature are common in swimmers, especially breaststroke swimmers. The whip-kick leg action in breaststroke tends to simultaneously abduct and laterally rotate (tibia with respect to femur) the knee, resulting in strain of the medial ligament and associated medial supporting structures (Vizsolyi et al 1987).
Physical activity helps reduce bone loss
Bone loss begins around age 45 – 50 and moves a at different rates during different phases
Porosity, Osteopenia, and Osteoporosis
Because of the channels and spaces within compact and cancellous bone, any particular region of a bone consists of certain amounts of bone tissue and nonbone tissue. The term porosity describes the proportion of nonbone tissue. At skeletal maturity the porosity of compact and cancellous bone is approximately 2% and 50%, respectively; the density (amount of bone tissue per unit volume) of compact bone is approximately double that of cancellous bone (Radin 1984, Tortora 2004). The density of bone tissue depends on the degree of mineralization. During ossification, the degree of mineralization of bone tissue gradually increases and reaches a maximum level at skeletal maturity (Bailey et al 1986). However, the amount of bone within the skeleton may continue to increase for 5 to 10 years after skeletal maturity, especially in people who are physically active (Stillman et al 1986, Talmage and Anderson 1984, Frost 2003). Consequently, bone mass peaks in males and females between 25 and 30 years of age. In terms of turnover, this means that from skeletal maturity to the age at which peak bone mass occurs, more new bone is formed than old and damaged bone is absorbed.
Following peak bone mass there is usually a stable period in which the amount of bone in the skeleton remains about the same; there is a balance between bone absorption and bone formation. This stable period is followed by a gradual decrease in bone mass for the rest of the person's life; the rate of bone absorption exceeds the rate of bone formation. Bone mass is the product of bone volume and bone density. The loss in bone mass that occurs with age following peak bone mass is the result of decreases in bone volume and bone density. Osteopenia refers to a level of bone density below the normal level for a person's age and sex (Bailey 1995, Frost 1997).
Bone mass starts to decrease earlier and at a greater rate in females than in males. In males, bone loss normally starts between 45 and 50 years of age and proceeds at a rate of 0.4% to 0.75% per year (Bailey et al 1986, Smith 1982). In females, bone loss has three phases. The first phase starts around 30 to 35 years of age and proceeds at a rate of 0.75% to 1% per year until menopause. From menopause until about 5 years after menopause, the rate of bone loss increases to between 2% and 3% per year. During the final phase, the rate of bone loss is approximately 1% per year. Thus, women may lose, on average, about 53% of their peak bone mass by the age of 80 years. In contrast, males may lose, on average, about 18% of their peak bone mass by the age of 80 years (figure 3.32).
Even though body weight tends to decrease with age, the rate of bone loss is usually much greater than the rate at which body weight decreases. Consequently, the effect of bone loss is that the bones, especially weight-bearing bones, become progressively weaker relative to the weight of the rest of the body. In addition to gradually losing strength, the bones also gradually lose their elasticity and become more brittle. In some people, especially women, a loss of bone mass and elasticity is eventually reached when some bones are no longer able to withstand the loads imposed by normal habitual activity. These bones become very susceptible to fracture. This condition, the most common bone disorder in elderly people, is called osteoporosis (Bailey et al 1986, Ferretti et al 2003). Osteoporosis may cause severe disfigurement, especially of the trunk, as a result of fractured or crushed vertebrae. Many deaths in elderly people are due to complications arising from bone fractures that occur as a result of osteoporosis (Kaplan 1983, Kado et al 1999, Cummings and Melton 2002).
Bone loss tends to occur earlier and to proceed at a faster rate in cancellous bone than in compact bone (Bailey et al 1986, Ferretti et al 2003). Consequently, regions of bones with a high proportion of cancellous bone, such as the bodies of the vertebrae, the head and neck of the femur, and the distal end of the radius, are particularly vulnerable to osteoporosis and fracture in elderly people. This vulnerability is reflected in studies that report a rapid increase in the incidence of bone fractures with age, especially in women (Bauer 1960, Chalmers and Ho 1970, Hagino et al 1991, Cummings et al 1993, Court-Brown and Caesar 2006). The results of one study showed that the incidence of fracture to the distal end of the radius was seven times higher in 54-year-old women than in 40-year-old women (Bauer 1960). In another study the incidence of fracture of the neck of the femur was found to be 50 times higher in 70-year-old women than in 40-year-old women (Chalmers and Ho 1970). Bone loss in compact bone occurs mainly on the endosteal surface so that bone width remains relatively unchanged into old age (Smith 1982, Ferretti et al 2003).
Although the cause of osteoporosis is not clear, there is general agreement that four variables are mainly responsible: genetic factors, endocrine status, nutritional factors, and physical activity (Bailey et al 1986, MacKinnon 1988, Ferretti et al 2003). The relative contribution of these variables has not been established, but physical activity seems to be the most important. In the absence of weight-bearing activity, no amount of endocrine or nutritional intervention will prevent rapid bone loss; there must be mechanical stress (Bailey et al 1986, Ferretti et al 2003). Research suggests that regular physical activity throughout life, within the moderate overload range (see chapter 11), can help to prevent osteoporosis in three ways (Bailey 1995, Greene and Naughton 2006, Baxter-Jones et al 2008):
- Peak bone mass is directly related to the level of physical activity prior to peak bone mass; the higher the peak bone mass, the lower the risk of osteoporosis.
- An above-average level of physical activity after peak bone mass will delay the onset of bone loss.
- An above-average level of physical activity after peak bone mass will reduce the rate of bone loss.
Case study 2 discusses whether regular exercise can be used to prevent falls in osteopenic women.
Case Study 2 Using Exercise to Prevent Falls in Osteopenic Women
Hourigan SR, Nitz JC, Brauer S, O'Neill S, Wong J, Richardson CA. 2008. Positive effects of exercise on falls and fracture risk in osteopenic women. Osteoporosis International 19:1077-1086.
The incidence of bone fractures increases with age. As the number of aged people worldwide is increasing, so is the total number of fractures in the aged population (age 65 years and older). Fractures in the aged population are a major health care cost and risk factor for permanent disability and death. Consequently, reducing the risk of fractures in the aged population is a challenge in many countries.
Physical trauma (in particular, falls) and weak bones (due to osteopenia or osteoporosis) are the major causes of fractures in the aged population. Poor balance and weak muscles are risk factors for falls. Osteopenia is defined as bone mineral density (BMD) between 1 and 2.5 standard deviations below the average for young women. Osteoporosis is defined as BMD more than 2.5 standard deviations below the average for young women.
Recent research indicates that muscle strength, bone strength, and balance in the aged population can be improved through properly prescribed physical activity training programs based on resistance exercises involving strength-training machines. The purpose of the present study was to determine the effect of a physical activity program based on weight-bearing activities (rather than strength-training machines) on balance, muscle strength, and bone mineral density in osteopenic women.
Ninety-eight community-dwelling (living more or less independently in their own homes) osteopenic women (age 62.01 ± 8.9; range 41-78 years) were randomly assigned to either a control group (n = 48: no intervention) or an exercise group (n = 50: two 1 hr exercise sessions per week for 20 weeks directed by a trained physiotherapist). Assessments at baseline and post intervention included balance (five measures), strength (quadriceps; hip abductors, adductors, and external rotators; trunk extensors), and BMD (proximal femur and lumbar spine). Baseline assessment showed no significant differences between the exercise and control groups in terms of balance, strength, BMD, or demographics.
The average number of sessions attended by the 42 members of the exercise group who completed the exercise program was 28.2 of a possible 40 sessions (71.2%). Following the intervention, the exercise group showed significantly better performance than the control group in 9 of 11 balance tests (ranging from 10% to 71% better performance) and 7 of 9 strength tests (ranging from 9% to 23% better performance). BMD of the exercise group increased but was not significantly greater than in the control group.
Application
A specific, well-directed program of weight-bearing exercises in a workstation format that emphasizes interaction, discussion, and enjoyment can significantly improve balance and strength in osteopenic women, which in turn is likely to reduce the risk of falling. This type of training may also positively influence BMD, but further research is needed.
Youth sports increase risk of physeal injury
Widespread participation in youth sports increase the risk of physeal injury, resulting in more permanent problems
Case Study 1 Physeal Injuries in Youth Sports
Caine D, DiFiori J, Maffulli N. 2006. Physeal injuries in children's and youth sports: Reasons for concern? British Journal of Sports Medicine 40:749-760.
Participation in children's and youth sports is widespread in Western culture. Many children start year-round training and specialization by 9 years of age. Preteens training at regional centers or with high school and club teams in sports such as gymnastics may train more than 20 hr per week. There is increasing concern, especially among physicians, that the frequency and intensity of training and competition experienced by many participants in children's and youth sports are putting them at risk of serious physeal injury (epiphyseal and apophyseal), which may result in permanent skeletal abnormalities. Unfortunately, detailed information, based on the use of standardized recording systems applied over a long period, on the epidemiology of injuries (incidence, location, type, diagnosis, severity) sustained by participants in children's and youth sports is not available for any sport. The purpose of this study was to systematically review the literature on the frequency and characteristics of physeal injuries in children's and youth sports.
The review was undertaken using Medline and SPORTdiscus. More than 150 reports were obtained, largely case reports or case series investigations. The authors used the reports to determine the number, location, type, diagnosis, and severity of physeal injuries that occur in different sports, but it was not possible to calculate incidence of injury because information was not provided on the total number of participants and exposure time of participants in the various sports.
The review indicates that acute physeal injuries (sudden widening or fracture along or through an epiphyseal or apophyseal plate accompanied by considerable pain) and chronic physeal injuries (progressive widening of an epiphyseal or apophyseal plate associated with a progressive increase in pain, especially during exercise) occur frequently in some sports, including football, baseball, gymnastics, basketball, volleyball, judo, weightlifting, soccer, rugby, tennis, cricket, and long-distance running. The main regions of physeal injuries are the shoulder, elbow, wrist, and knee. Most of the injuries are chronic, and most resolve without complication. However, there are several reports of premature partial or complete physeal closure.
The authors express a number of concerns with current practice, in particular, the paucity of epidemiological data on the distribution and determinants of physeal injuries in children's and youth sports and the apparent lack of knowledge on the part of many coaches of children's and youth sports regarding musculoskeletal growth and development in children in general and physeal injuries in particular.
Application
Coaches should consider the following strategies to reduce the incidence of physeal injuries in children's and youth sports:
- Individualize fitness training and practice for athletes experiencing rapid growth. Assess growth rate by monitoring increases in height and limb segment lengths.
- Use a variety of training and practice drills and avoid excessive volume of training.
- For collision sports, ensure that competition is based on physical maturity rather than chronological age.
- Mandate regular medical assessment to ensure early diagnosis and treatment of epiphyseal and apophyseal plate disorders.
Structure of the knee facilitates extension and flexion
Learn more about the tibiofemoral joint and the ligaments
Capsule of the Knee
The tibiofemoral and patellofemoral joints share a common capsule that has a complicated shape. The capsule is attached above to the femur, below to the tibia, and anteriorly to the patella (figure 6.13). To accommodate the extremes of full flexion and full extension of the tibiofemoral joint, the anterior part of the capsule is folded upward during extension and the posterior part of the capsule is folded downward during flexion. The upward fold, only present in extension, is referred to as the suprapatellar bursa (figure 6.13). The suprapatellar bursa intervenes between the quadriceps tendon and the anterior aspect of the femur just proximal to the patellar surface.
Figure 6.13 Sagittal section through the knee complex showing the shape of the capsule in extension.
The downward fold, only present during flexion, is referred to as the gastrocnemius bursa. The gastrocnemius bursa intervenes between the posterior aspect of the tibial condyles and the gastrocnemius muscle. In general, a bursa is a flattened sac of synovial membrane containing synovial fluid. Bursas minimize friction between structures that slide across each other during normal movement (see chapter 7).
During flexion of the tibiofemoral joint, the suprapatellar bursa becomes progressively smaller and the gastrocnemius bursa becomes progressively larger as synovial fluid is redistributed from the suprapatellar bursa to the gastrocnemius bursa. The movement of synovial fluid is reversed during extension of the tibiofemoral joint; that is, the gastrocnemius bursa becomes progressively smaller and the suprapatellar bursa becomes progressively larger.
The suprapatellar bursa is separated from the femur by a pad of fat called the suprapatellar fat pad. Lying in the space bounded by the upper two thirds of the posterior aspect of the patellar ligament, the anterior intercondylar area of the tibia, and the anterior inferior aspect of the articular surface of the femoral condyles is a pad of fat called the infrapatellar fat pad. It is roughly triangular in sagittal cross section and is suspended superiorly from a fibro-adipose band called the infrapatellar fold. The infrapatellar fold is attached anteriorly to the inferior pole of the patella and posteriorly to the anterior border of the intercondylar notch (figure 6.13). The infrapatellar fat pad is attached anteriorly to the posterior aspect of the patellar ligament and extends at both sides of the patellar ligament. The infrapatellar fat pad also extends narrow branches halfway up each side of the patella; the branches are referred to as alar folds (alar = winglike). The infrapatellar fat pad cushions the patellar ligament and lower part of the patella during movements of the knee.
Knee Ligaments
Four extracapsular ligaments support the tibiofemoral joint. The lateral ligament (also referred to as the lateral collateral ligament and the fibular collateral ligament) is attached superiorly to the lateral epicondyle of the femur and inferiorly to the head of the fibula (figure 6.14a). The medial ligament (also referred to as the medial collateral ligament and the tibial collateral ligament) is attached superiorly to the medial epicondyle of the femur and inferiorly to the medial aspect of the tibia below the tibial condyle (figure 6.14b). The posterior fibers of the medial ligament blend with the joint capsule at the level of the medial meniscus and thus the medial ligament is not completely extracapsular. The arrangement of the medial and lateral ligaments and the curvature of the femoral condyles are such that both ligaments are relatively slack when the knee is flexed but become progressively more taut as the joint extends. In a normal joint the ligaments are fully taut when the joint is fully extended. In this position of the joint both ligaments help to prevent hyperextension and lateral rotation of the tibia relative to the femur. With the knee fully extended, the range of abduction and adduction is normally zero. Because the medial and lateral ligaments are relatively slack when the knee is flexed, a certain amount of axial rotation and abduction and adduction of the lower leg can occur when the knee is in a flexed, non-weight-bearing position. For example, when a person is sitting on a table with his lower leg hanging freely, the ranges of internal and external rotation are normally around 30° and 40°, respectively (Norkin and Levangie 1992). However, the ranges of abduction and adduction are normally very small, approximately 2° to 5°.
Figure 6.14 Location of the main ligaments of the left knee. (a) Lateral aspect. (b) Medial aspect.
Injuries to the lateral and, in particular, the medial ligaments are common in sports (Reider 1996). The classic cause of medial ligament injury is a blow to the lateral aspect of the knee while the foot in contact with the ground, resulting in abduction of the knee. This situation is common in sports such as American football, soccer, and rugby. The excessive loading on the medial ligament in such situations can result in serious injury (Indelicato 1995). Medial ligament injuries of a less severe but nonetheless persistent nature are common in swimmers, especially breaststroke swimmers. The whip-kick leg action in breaststroke tends to simultaneously abduct and laterally rotate (tibia with respect to femur) the knee, resulting in strain of the medial ligament and associated medial supporting structures (Vizsolyi et al 1987).
Related Books