
- Home
- Stretching and Flexibility
- Physical Activity and Health
- Health Education
- Health Care for Special Conditions
- Fitness and Health
- Physical Activity and Health Guidelines
Physical Activity and Health Guidelines
Recommendations for Various Ages, Fitness Levels, and Conditions from 57 Authoritative Sources
by Riva Rahl
368 Pages, 8.5
Sifting through the numerous guidelines on physical activity and health published by government agencies, professional organizations, and associations can be a daunting task. Information exists in all types of formats and locations—including government documents, press releases, and Web sites—so simply finding those guidelines can be an ordeal. PhysicalActivity and Health Guidelines puts the current information in one place—at your fingertips.
Physical Activity and Health Guidelines compiles the latest recommendations from various leading sources and organizations into a single text. This one-of-kind resource provides quick reference to physical activity and health recommendations for healthy people and for those with chronic conditions across all age groups. All readers—physicians, physical therapists, fitness professionals, and general fitness enthusiasts—will be able to locate individualized recommendations regarding appropriate levels and types of physical activity.
Specific activity recommendations for people with diabetes, asthma, osteoarthritis, and cerebral palsy are detailed in this text. Other guidelines for the prevention of common chronic diseases such as cancer, coronary artery disease, osteoporosis, and metabolic syndrome are also shared.
This text also includes the following information:
• The components of exercise program design, which will assist readers in preparing to implement individual and group exercise programs
• How physical activity recommendations can help people meet weight-management guidelines
• Information on purchasing and using exercise equipment such as treadmills, heart rate monitors, weight training machines, and exercise videos
• Guidelines for cardiac testing and other exercise testing to assist in the implementation and evaluation of physical activity programs as well as the assessment of the safety of these programs for people with chronic conditions
For ease of use, Physical Activity and Health Guidelines presents information in a consistent format for each entry, including the date issued or most recently updated, the issuing organization, appropriate population, and location of the guidelines (with Web sites when available). Recommendations are given for aerobic, resistance, and flexibility training; further specifications regarding the frequency, intensity, duration, and type of activity are included. An appendix lists additional resources divided by topic and includes Web addresses of key organizations, statements, and other physical activity and health-related tools.
Physical Activity and Health Guidelines is the first text to gather the wealth of information regarding physical activity, exercise, and health needs and recommendations into a single source. Convenient and easy to use, this unique text will help readers understand the requirements for safe and effective physical activity for all people regardless of health conditions, and it offers the basic knowledge and tools for designing and implementing appropriate physical activity programs.
Part I: General Health and Fitness Guidelines
Chapter 1: Exploring the Relationship Between Physical Activity and Health
History and Development of Physical Activity Guidelines
Basic Concepts and Definitions
Changes and Benefits Resulting From Physical Activity
Risks of Physical Activity
Patterns in Physical Activity Participation
Summary
Chapter 2: Exercise Guidelines for Physical Fitness and Health
Most Recent National Guidelines in the United States
Significant Historical Guidelines
Specialized Guidelines
State and International Guidelines
Summary
Chapter 3: Guidelines for Personal Exercise Programs
Basic Definitions and the FITT Principle
Components of Physical Fitness
Guidelines for Individualized Exercise Prescription
Summary
Part II: Physical Activity Guidelines by Population
Chapter 4: Infants and Toddlers
Guidelines From the American Academy of Pediatrics
Guidelines From Other Organizations
Guidelines for Prevention of Obesity and Chronic Disease
Physical Activity as Play and Nutritional Goals for Children
Summary
Chapter 5: School-Aged Children
Basic Facts About Physical Activity and Health in Children
Establishment of the Earliest Guidelines for Children
Landmark Guidelines
School and Community Health Guidelines
Guidelines Outside of the School Environment
International and State Guidelines
Guidelines Focused on Specific Health Goals
Summary
Chapter 6: Pregnant and Postpartum Women
Encouraging Pregnant Women to Be Physically Active
Benefits and Risks of Physical Activity for Pregnant Women
Primary Concerns of Exercise and Physical Activity During Pregnancy
Guidelines for General Exercise Prescription
Important National and International Guidelines
Benefits and Risks of Physical Activity During the Postpartum Period
Summary
Chapter 7: Older Adults
Benefits of Physical Activity for Older Adults
Major National Guidelines
Other National Guidelines
International and State Guidelines
Guidelines for Adults Who Are Frail or at Risk for Falling
Contraindications to Exercise
Summary
Part III: Physical Activity Guidelines by Disease States
Chapter 8: Cancer Prevention and Optimal Cardiometabolic Health
How Exercise Reduces the Risks of Cancer
General Cancer Prevention Guidelines
Guidelines for Specific Types of Cancer
Metabolic Syndrome
Type 2 Diabetes
Summary
Chapter 9: Cancer
Benefits of Physical Activity
American Cancer Society Guidelines
Other Notable Guidelines
Guidelines for Specific Cancers
Side Effects of Cancer Affecting Physical Activity
Summary
Chapter 10: Hypertension and Cardiovascular Disease
Benefits of Exercise for Hypertension
American College of Sports Medicine Guidelines
International Guidelines
Guidelines for Coronary Artery Disease
Summary
Chapter 11: Arthritis and Osteoporosis
Rheumatoid Arthritis
Osteoarthritis
General Arthritis Guidelines
Osteoarthritis Guidelines
Osteoporosis
Guidelines for Prevention of Osteoporosis
Guidelines for Individuals With Osteoporosis
Summary
Chapter 12: Diabetes
Benefits of Physical Activity for Preventing and Managing Diabetes
Potential Concerns Regarding Physical Activity
Guidelines for Individuals With Type 2 Diabetes
Guidelines for Individuals With Type 1 Diabetes
Summary
Chapter 13: Neuromuscular Disorders
Benefits of Physical Activity
General Recommendations From Physical Activity Guidelines for Americans
Guidelines for Cerebral Palsy
Guidelines for Parkinson’s Disease
Guidelines for Muscular Dystrophy
Guidelines for Multiple Sclerosis
Guidelines for Spinal Cord Injury and Disability
Guidelines for Stroke and Brain Injury
Summary
Chapter 14: Asthma
Exercise-Induced Asthma
General Guidelines for People With Asthma
Guidelines for Children With Asthma
Summary
Part IV: Guidelines for Exercise Testing and Prescription and Beyond
Chapter 15: Exercise Testing and Prescription
Standards for Exercise Testing in Adults
Benefits of Exercise Testing for Children
Summary
Chapter 16: Cardiac Exercise Testing and Prescription
Candidates for Testing Utility of Information Acquired From Exercise Testing
Protocols for Exercise Testing
Exercise Testing Procedures
Other Methods of Cardiac Testing
Summary
Chapter 17: Dietary and Weight Management Guidelines
Basic Facts About Body Weight
Dietary Guidelines From National Organizations
International Dietary Guidelines
Hydration, Energy, and Supplementation During Activity
Dietary Guidelines for Special Populations
Dietary Guidelines for Various Diseases
Summary
Chapter 18: Exercise Equipment and Facilities
Aerobic Exercise Machines
Weights
Tools for Monitoring Physical Activity
Exercising at Home
Exercising in a Workout Facility
Summary
Riva L. Rahl, MD, is medical director of the Cooper Wellness Program at the Cooper Aerobics Center in Dallas, Texas, where she counsels patients and clients regarding appropriate physical activity programs.
Board certified in both internal and emergency medicine, Rahl is a staff physician at the Cooper Clinic in Dallas and was previously chief resident in emergency medicine at the University of Texas Southwestern (Parkland) Hospital. She is a member of the American College of Sports Medicine, the American College of Physicians, and USA Track and Field. She received her medical doctorate from the University of California at San Francisco in 1999.
Now a competitive marathoner, Rahl was a four-year varsity athlete in cross country and track and field at Rice University (Division I), where she studied biochemistry and exercise science. She has won several races, including the Dallas White Rock Marathon in 2000 and the Fort Worth Cowtown Marathon in 2000, 2002, and 2008.
Rahl and her husband, Brian, and two young sons reside in Dallas. Rahl enjoys training for race day, caring for her children, and traveling internationally.
Physical activity as play and nutritional goals for children
Because infants and young children are not autonomous, guidelines for this population are aimed at parents, caregivers, schools, and the community.
Because infants and young children are not autonomous, guidelines for this population are aimed at parents, caregivers, schools, and the community. In fact, the next chapter outlines multiple sets of guidelines focusing on community or school policy as a way of promoting physical activity for youths. For preschoolers, it is extremely important that age-appropriate opportunities for physical activity and play be available. Playgrounds offer a variety of activities that may be acceptable for a range of ages, making them a sound option for children. Starting with toddlers and extending through older school-aged children, playground equipment allows for independent play with multiple opportunities to challenge the musculoskeletal, neurological, and psychosocial systems. Many of the guidelines for young children include a call to action for communities to continue to provide ample opportunities for outdoor play in the form of playgrounds and outdoor environments. One author summed up the benefits of playgrounds and physical play as allowing children to BECOME FIT (adapted from Clements 2007).
In addition to physical activity, healthy diet and proper nutrition should begin at an early age. The connection between food and fitness is clearly known; parents and caregivers again have an opportunity to play role model for their children by following healthy eating patterns. Sitting down to meals as a family—particularly breakfast—has been shown to improve communication as well as emotional and psychosocial development. Schoolchildren who eat breakfast perform better academically and have a better chance of meeting all their nutritional needs. Getting adequate amounts of macronutrients, vitamins, minerals, and fiber enables children to have the proper energy to live the active lifestyle that is so important for their present and future health status. Recommendations for appropriate activity and nutrition in children appear in both the IOM report on DRIs and the Dietary Guidelines for Americans. While the 2005 Dietary Guidelines for Americans specifically states that its recommendations apply to children aged 2 y and older, the report on DRIs does not make specific reference to the age at which the youth guidelines apply.
SUMMARY
Guidelines for infants and toddlers are important in that they establish the foundation for a lifetime of physical activity and good health. Although exercise per se is not recommended for very young children, there is an emphasis on developmentally appropriate and enjoyable physical activity. Children in this age group use physical activity to build motor skills that will ultimately pave the way for more formalized physical activity as they grow. Properly supervised opportunities for activity, an avoidance of sedentary time, and the ability to observe and pattern healthy physical activity behaviors in parents and caregivers are key components of guidelines for this age group.
Benefits and risks of physical activity for pregnant women
The goals of physical activity during pregnancy include maintaining a sense of maternal well-being, avoiding fetal harm, and establishing a pattern of regular activity.
The goals of physical activity during pregnancy include maintaining a sense of maternal well-being, avoiding fetal harm, and establishing a pattern of regular activity that will ultimately prevent the onset of chronic disease associated with a sedentary lifestyle. Most women can participate in a wide range of recreational activities and maintain an active lifestyle during pregnancy, although those with medical or obstetrical complications may require modifications. Modifications may also be necessary for women who regularly participated in strenuous recreational or competitive physical activities before their pregnancies. In addition, women who are active before pregnancy may choose to modify their exercise programs somewhat; for example, weight gain or joint laxity may prompt women to walk instead of jog or to exercise indoors instead of outdoors because of improved environmental control. Because of all the physiological changes that occur during pregnancy, activity recommendations for pregnant women are subject to modifications. Finally, concerns for fetal health dictate other changes in order to optimize fetal outcomes.
Nevertheless, the benefits of regular physical activity throughout pregnancy generally outweigh the risks. Women who exercise routinely in the prenatal period have a lower incidence of babies with low birth weight. Starting with the first trimester, regular activity may help ease nausea and lessen fatigue. Body image and mood—both during pregnancy and in the postpartum period—are positively influenced by regular physical activity. Although there are not yet disorder-specific guidelines, it is felt that regular physical activity during pregnancy benefits preeclampsia, hypertension, and gestational diabetes, as mentioned earlier. It is not yet clear whether a regular physical activity program affects gestational length, quality or duration of labor, or incidence of chronic disease in the offspring.
Although the benefits of physical activity for pregnant women are significant, there are still precautions to take and health risks to keep in mind. Because of the increased metabolic rate during pregnancy, thermoregulation during exercise and the potential effect on fetal temperature are a concern. It is important for pregnant exercisers to stay well hydrated in order to improve cooling and maintain blood volume. While the benefits of chronic exercise belong to the mother, the risk of overexercise predominantly affects the fetus (Whaley 2005).

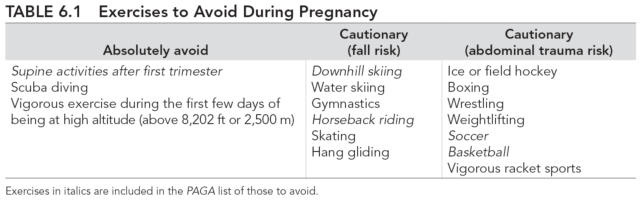
Starting with the second trimester, supine exercises are not recommended, as these can cause the uterus to compress the inferior vena cava and result in decreased cardiac output. Also, prolonged isometric exercise during weightlifting may decrease uterine perfusion. Because of the shift in the expecting mother's center of gravity, exercises that require balance should be avoided later in pregnancy; other anatomical changes of pregnancy are presented in the sidebar. Contact sports and activities that have an increased risk for falls should also be avoided. The new PAGA lists several exercises to avoid; table 6.1 includes these as well as others with risk for maternal or fetal harm. Motionless standing results in venous pooling and a significant decrease in cardiac output and thus should be avoided. In fact, one large study of 7,722 pregnancies found that mothers who had jobs requiring predominantly standing had babies with lower birth weights (Naeye and Peters 1982).
Exercise has beneficial effect on hypertension, cardiovascular disease
Currently more than 50 million Americans—and more than 50% of the American population over the age of 60—have hypertension, or high blood pressure (Hagberg 2005).
Currently more than 50 million Americans—and more than 50% of the American population over the age of 60—have hypertension, or high blood pressure (Hagberg2005). Worldwide, the number of people with hypertension is estimated to be 1 billion! Furthermore, because blood pressure tends to increase with age, the number of people with hypertension is likely to rise significantly as the U.S. population continues to age. Unfortunately, due to a lack of symptoms a large number of individuals are unaware that they have the silent killer, as hypertension is called, and do not realize their hypertension is placing them at a higher risk for a heart attack or stroke. Although hypertension affects nearly every organ, its lack of symptoms means that many individuals do not realize the damage that may be occurring even at modest elevations of blood pressure.
Physical activity is considered one of the mainstays in the nonpharmacological treatment of hypertension. This chapter discusses the current definition of hypertension and introduces the physiological relationship between exercise and blood pressure, as well as provides some background and mechanistic details. Then it presents both nationally and internationally issued activity guidelines for individuals with hypertension. Also, because of the close and causal relationship between hypertension and CAD, this chapter also includes guidelines that pertain to CAD.
Benefits of Exercise for Hypertension
The definition of hypertension has changed over time. Currently, the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7: NHBPEP 2003) defines normal blood pressure as a pressure less than 120/80 mmHg (see table 10.1). Elevated blood pressure, which at one time was diagnosed only when in excess of 160/100 mmHg, is a primary cardiac risk factor and also increases the risk for stroke, type 2 diabetes, kidney disease, and vascular disease. According to the JNC 7, the risk of CVD begins at only 115/75 mmHg and doubles with each incremental increase of 20/10 mmHg. People who are classified as prehyper-tensive have twice the risk of developing hypertension. Even individuals with normal blood pressure have a high lifetime risk of developing hypertension—an estimated 90% risk for individuals with normal blood pressure at age 55 (Vasan and others 2002)!
For people with prehypertension, exercise is one of the primary recommended lifestyle changes that can lower blood pressure to a normal level. In fact, even in individuals who have a normal blood pressure, regular aerobic exercise may lower resting blood pressure, although the extent of lowering is less than that seen in individuals with frank hypertension. In the JNC 7, physical activity compares favorably with the other recommended lifestyle changes when it comes to reducing resting blood pressure—table 10.2 gives examples of these changes and their relative effects. Also, physical activity may contribute to weight loss, which can reduce blood pressure even further.

So, although the distensibility or pliability of blood vessels decreases with age and makes hypertension more likely, hypertension is not necessarily an unavoidable consequence of aging, because regular physical activity is clearly effective in preventing hypertension and reducing its intensity. A single session of aerobic exercise creates a sustained hypotensive response that lasts up to 24 h (Hagberg and others 2000), and over time participation in regular physical activity can have long-term benefits. Postulated mechanisms for the reduction of both systolic and diastolic blood pressure that occurs with regular exercise training include the following:
- Reduced visceral fat
- Improved sodium elimination due to altered renal function
- Reduced plasma renin and catecholamine activity
- Reduced sympathetic and increased parasympathetic tone
Because physical activity decreases hypertension, it also reduces the potential contribution of hypertension to cardiovascular risk. In addition to lowering blood pressure, physical activity generally causes a regression of left ventricular hypertrophy, improves lipid profiles, and lowers the risk for type 2 diabetes. This combination of risk reduction has a substantial long-term benefit on cardiovascular risk. There are also notable benefits to other health parameters. Individuals with hypertension may not necessarily achieve normal blood pressure through exercise, but they will likely see improvements in lean body mass, glycemic control, and inflammatory biomarkers.
Overall, a regular physical activity program lowers both systolic and diastolic blood pressure. However, during aerobic exercise, the normal physiological response is a gradually rising systolic blood pressure with a stable or slightly decreasing diastolic blood pressure. In addition, during resistance training and particularly during high-intensity efforts, blood pressure may rise significantly. These natural responses to exercise necessitate guidelines for people with hypertension so that they may receive the benefits of activity safely without increasing their risk for injury or disease.
The use of antihypertensive medications also necessitates physical activity guidelines. Exercise is recommended as an adjunct to antihypertensive medication as there appears to be an additive effect of physical activity with most antihypertensive medications. Beta-blockers, however, may interfere with the antihypertensive effect of exercise (Ades and others 1988). For hypertensive individuals who regularly participate in physical activity, beta-blockers also blunt the peak heart rate and blood pressure; the former effect requires using an alternative to target heart rate for measuring exercise intensity.
Physical activity as play and nutritional goals for children
Because infants and young children are not autonomous, guidelines for this population are aimed at parents, caregivers, schools, and the community.
Because infants and young children are not autonomous, guidelines for this population are aimed at parents, caregivers, schools, and the community. In fact, the next chapter outlines multiple sets of guidelines focusing on community or school policy as a way of promoting physical activity for youths. For preschoolers, it is extremely important that age-appropriate opportunities for physical activity and play be available. Playgrounds offer a variety of activities that may be acceptable for a range of ages, making them a sound option for children. Starting with toddlers and extending through older school-aged children, playground equipment allows for independent play with multiple opportunities to challenge the musculoskeletal, neurological, and psychosocial systems. Many of the guidelines for young children include a call to action for communities to continue to provide ample opportunities for outdoor play in the form of playgrounds and outdoor environments. One author summed up the benefits of playgrounds and physical play as allowing children to BECOME FIT (adapted from Clements 2007).
In addition to physical activity, healthy diet and proper nutrition should begin at an early age. The connection between food and fitness is clearly known; parents and caregivers again have an opportunity to play role model for their children by following healthy eating patterns. Sitting down to meals as a family—particularly breakfast—has been shown to improve communication as well as emotional and psychosocial development. Schoolchildren who eat breakfast perform better academically and have a better chance of meeting all their nutritional needs. Getting adequate amounts of macronutrients, vitamins, minerals, and fiber enables children to have the proper energy to live the active lifestyle that is so important for their present and future health status. Recommendations for appropriate activity and nutrition in children appear in both the IOM report on DRIs and the Dietary Guidelines for Americans. While the 2005 Dietary Guidelines for Americans specifically states that its recommendations apply to children aged 2 y and older, the report on DRIs does not make specific reference to the age at which the youth guidelines apply.
SUMMARY
Guidelines for infants and toddlers are important in that they establish the foundation for a lifetime of physical activity and good health. Although exercise per se is not recommended for very young children, there is an emphasis on developmentally appropriate and enjoyable physical activity. Children in this age group use physical activity to build motor skills that will ultimately pave the way for more formalized physical activity as they grow. Properly supervised opportunities for activity, an avoidance of sedentary time, and the ability to observe and pattern healthy physical activity behaviors in parents and caregivers are key components of guidelines for this age group.
Benefits and risks of physical activity for pregnant women
The goals of physical activity during pregnancy include maintaining a sense of maternal well-being, avoiding fetal harm, and establishing a pattern of regular activity.
The goals of physical activity during pregnancy include maintaining a sense of maternal well-being, avoiding fetal harm, and establishing a pattern of regular activity that will ultimately prevent the onset of chronic disease associated with a sedentary lifestyle. Most women can participate in a wide range of recreational activities and maintain an active lifestyle during pregnancy, although those with medical or obstetrical complications may require modifications. Modifications may also be necessary for women who regularly participated in strenuous recreational or competitive physical activities before their pregnancies. In addition, women who are active before pregnancy may choose to modify their exercise programs somewhat; for example, weight gain or joint laxity may prompt women to walk instead of jog or to exercise indoors instead of outdoors because of improved environmental control. Because of all the physiological changes that occur during pregnancy, activity recommendations for pregnant women are subject to modifications. Finally, concerns for fetal health dictate other changes in order to optimize fetal outcomes.
Nevertheless, the benefits of regular physical activity throughout pregnancy generally outweigh the risks. Women who exercise routinely in the prenatal period have a lower incidence of babies with low birth weight. Starting with the first trimester, regular activity may help ease nausea and lessen fatigue. Body image and mood—both during pregnancy and in the postpartum period—are positively influenced by regular physical activity. Although there are not yet disorder-specific guidelines, it is felt that regular physical activity during pregnancy benefits preeclampsia, hypertension, and gestational diabetes, as mentioned earlier. It is not yet clear whether a regular physical activity program affects gestational length, quality or duration of labor, or incidence of chronic disease in the offspring.
Although the benefits of physical activity for pregnant women are significant, there are still precautions to take and health risks to keep in mind. Because of the increased metabolic rate during pregnancy, thermoregulation during exercise and the potential effect on fetal temperature are a concern. It is important for pregnant exercisers to stay well hydrated in order to improve cooling and maintain blood volume. While the benefits of chronic exercise belong to the mother, the risk of overexercise predominantly affects the fetus (Whaley 2005).
Starting with the second trimester, supine exercises are not recommended, as these can cause the uterus to compress the inferior vena cava and result in decreased cardiac output. Also, prolonged isometric exercise during weightlifting may decrease uterine perfusion. Because of the shift in the expecting mother's center of gravity, exercises that require balance should be avoided later in pregnancy; other anatomical changes of pregnancy are presented in the sidebar. Contact sports and activities that have an increased risk for falls should also be avoided. The new PAGA lists several exercises to avoid; table 6.1 includes these as well as others with risk for maternal or fetal harm. Motionless standing results in venous pooling and a significant decrease in cardiac output and thus should be avoided. In fact, one large study of 7,722 pregnancies found that mothers who had jobs requiring predominantly standing had babies with lower birth weights (Naeye and Peters 1982).
Exercise has beneficial effect on hypertension, cardiovascular disease
Currently more than 50 million Americans—and more than 50% of the American population over the age of 60—have hypertension, or high blood pressure (Hagberg 2005).
Currently more than 50 million Americans—and more than 50% of the American population over the age of 60—have hypertension, or high blood pressure (Hagberg2005). Worldwide, the number of people with hypertension is estimated to be 1 billion! Furthermore, because blood pressure tends to increase with age, the number of people with hypertension is likely to rise significantly as the U.S. population continues to age. Unfortunately, due to a lack of symptoms a large number of individuals are unaware that they have the silent killer, as hypertension is called, and do not realize their hypertension is placing them at a higher risk for a heart attack or stroke. Although hypertension affects nearly every organ, its lack of symptoms means that many individuals do not realize the damage that may be occurring even at modest elevations of blood pressure.
Physical activity is considered one of the mainstays in the nonpharmacological treatment of hypertension. This chapter discusses the current definition of hypertension and introduces the physiological relationship between exercise and blood pressure, as well as provides some background and mechanistic details. Then it presents both nationally and internationally issued activity guidelines for individuals with hypertension. Also, because of the close and causal relationship between hypertension and CAD, this chapter also includes guidelines that pertain to CAD.
Benefits of Exercise for Hypertension
The definition of hypertension has changed over time. Currently, the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7: NHBPEP 2003) defines normal blood pressure as a pressure less than 120/80 mmHg (see table 10.1). Elevated blood pressure, which at one time was diagnosed only when in excess of 160/100 mmHg, is a primary cardiac risk factor and also increases the risk for stroke, type 2 diabetes, kidney disease, and vascular disease. According to the JNC 7, the risk of CVD begins at only 115/75 mmHg and doubles with each incremental increase of 20/10 mmHg. People who are classified as prehyper-tensive have twice the risk of developing hypertension. Even individuals with normal blood pressure have a high lifetime risk of developing hypertension—an estimated 90% risk for individuals with normal blood pressure at age 55 (Vasan and others 2002)!
For people with prehypertension, exercise is one of the primary recommended lifestyle changes that can lower blood pressure to a normal level. In fact, even in individuals who have a normal blood pressure, regular aerobic exercise may lower resting blood pressure, although the extent of lowering is less than that seen in individuals with frank hypertension. In the JNC 7, physical activity compares favorably with the other recommended lifestyle changes when it comes to reducing resting blood pressure—table 10.2 gives examples of these changes and their relative effects. Also, physical activity may contribute to weight loss, which can reduce blood pressure even further.
So, although the distensibility or pliability of blood vessels decreases with age and makes hypertension more likely, hypertension is not necessarily an unavoidable consequence of aging, because regular physical activity is clearly effective in preventing hypertension and reducing its intensity. A single session of aerobic exercise creates a sustained hypotensive response that lasts up to 24 h (Hagberg and others 2000), and over time participation in regular physical activity can have long-term benefits. Postulated mechanisms for the reduction of both systolic and diastolic blood pressure that occurs with regular exercise training include the following:
- Reduced visceral fat
- Improved sodium elimination due to altered renal function
- Reduced plasma renin and catecholamine activity
- Reduced sympathetic and increased parasympathetic tone
Because physical activity decreases hypertension, it also reduces the potential contribution of hypertension to cardiovascular risk. In addition to lowering blood pressure, physical activity generally causes a regression of left ventricular hypertrophy, improves lipid profiles, and lowers the risk for type 2 diabetes. This combination of risk reduction has a substantial long-term benefit on cardiovascular risk. There are also notable benefits to other health parameters. Individuals with hypertension may not necessarily achieve normal blood pressure through exercise, but they will likely see improvements in lean body mass, glycemic control, and inflammatory biomarkers.
Overall, a regular physical activity program lowers both systolic and diastolic blood pressure. However, during aerobic exercise, the normal physiological response is a gradually rising systolic blood pressure with a stable or slightly decreasing diastolic blood pressure. In addition, during resistance training and particularly during high-intensity efforts, blood pressure may rise significantly. These natural responses to exercise necessitate guidelines for people with hypertension so that they may receive the benefits of activity safely without increasing their risk for injury or disease.
The use of antihypertensive medications also necessitates physical activity guidelines. Exercise is recommended as an adjunct to antihypertensive medication as there appears to be an additive effect of physical activity with most antihypertensive medications. Beta-blockers, however, may interfere with the antihypertensive effect of exercise (Ades and others 1988). For hypertensive individuals who regularly participate in physical activity, beta-blockers also blunt the peak heart rate and blood pressure; the former effect requires using an alternative to target heart rate for measuring exercise intensity.
Physical activity as play and nutritional goals for children
Because infants and young children are not autonomous, guidelines for this population are aimed at parents, caregivers, schools, and the community.
Because infants and young children are not autonomous, guidelines for this population are aimed at parents, caregivers, schools, and the community. In fact, the next chapter outlines multiple sets of guidelines focusing on community or school policy as a way of promoting physical activity for youths. For preschoolers, it is extremely important that age-appropriate opportunities for physical activity and play be available. Playgrounds offer a variety of activities that may be acceptable for a range of ages, making them a sound option for children. Starting with toddlers and extending through older school-aged children, playground equipment allows for independent play with multiple opportunities to challenge the musculoskeletal, neurological, and psychosocial systems. Many of the guidelines for young children include a call to action for communities to continue to provide ample opportunities for outdoor play in the form of playgrounds and outdoor environments. One author summed up the benefits of playgrounds and physical play as allowing children to BECOME FIT (adapted from Clements 2007).
In addition to physical activity, healthy diet and proper nutrition should begin at an early age. The connection between food and fitness is clearly known; parents and caregivers again have an opportunity to play role model for their children by following healthy eating patterns. Sitting down to meals as a family—particularly breakfast—has been shown to improve communication as well as emotional and psychosocial development. Schoolchildren who eat breakfast perform better academically and have a better chance of meeting all their nutritional needs. Getting adequate amounts of macronutrients, vitamins, minerals, and fiber enables children to have the proper energy to live the active lifestyle that is so important for their present and future health status. Recommendations for appropriate activity and nutrition in children appear in both the IOM report on DRIs and the Dietary Guidelines for Americans. While the 2005 Dietary Guidelines for Americans specifically states that its recommendations apply to children aged 2 y and older, the report on DRIs does not make specific reference to the age at which the youth guidelines apply.
SUMMARY
Guidelines for infants and toddlers are important in that they establish the foundation for a lifetime of physical activity and good health. Although exercise per se is not recommended for very young children, there is an emphasis on developmentally appropriate and enjoyable physical activity. Children in this age group use physical activity to build motor skills that will ultimately pave the way for more formalized physical activity as they grow. Properly supervised opportunities for activity, an avoidance of sedentary time, and the ability to observe and pattern healthy physical activity behaviors in parents and caregivers are key components of guidelines for this age group.
Benefits and risks of physical activity for pregnant women
The goals of physical activity during pregnancy include maintaining a sense of maternal well-being, avoiding fetal harm, and establishing a pattern of regular activity.
The goals of physical activity during pregnancy include maintaining a sense of maternal well-being, avoiding fetal harm, and establishing a pattern of regular activity that will ultimately prevent the onset of chronic disease associated with a sedentary lifestyle. Most women can participate in a wide range of recreational activities and maintain an active lifestyle during pregnancy, although those with medical or obstetrical complications may require modifications. Modifications may also be necessary for women who regularly participated in strenuous recreational or competitive physical activities before their pregnancies. In addition, women who are active before pregnancy may choose to modify their exercise programs somewhat; for example, weight gain or joint laxity may prompt women to walk instead of jog or to exercise indoors instead of outdoors because of improved environmental control. Because of all the physiological changes that occur during pregnancy, activity recommendations for pregnant women are subject to modifications. Finally, concerns for fetal health dictate other changes in order to optimize fetal outcomes.
Nevertheless, the benefits of regular physical activity throughout pregnancy generally outweigh the risks. Women who exercise routinely in the prenatal period have a lower incidence of babies with low birth weight. Starting with the first trimester, regular activity may help ease nausea and lessen fatigue. Body image and mood—both during pregnancy and in the postpartum period—are positively influenced by regular physical activity. Although there are not yet disorder-specific guidelines, it is felt that regular physical activity during pregnancy benefits preeclampsia, hypertension, and gestational diabetes, as mentioned earlier. It is not yet clear whether a regular physical activity program affects gestational length, quality or duration of labor, or incidence of chronic disease in the offspring.
Although the benefits of physical activity for pregnant women are significant, there are still precautions to take and health risks to keep in mind. Because of the increased metabolic rate during pregnancy, thermoregulation during exercise and the potential effect on fetal temperature are a concern. It is important for pregnant exercisers to stay well hydrated in order to improve cooling and maintain blood volume. While the benefits of chronic exercise belong to the mother, the risk of overexercise predominantly affects the fetus (Whaley 2005).
Starting with the second trimester, supine exercises are not recommended, as these can cause the uterus to compress the inferior vena cava and result in decreased cardiac output. Also, prolonged isometric exercise during weightlifting may decrease uterine perfusion. Because of the shift in the expecting mother's center of gravity, exercises that require balance should be avoided later in pregnancy; other anatomical changes of pregnancy are presented in the sidebar. Contact sports and activities that have an increased risk for falls should also be avoided. The new PAGA lists several exercises to avoid; table 6.1 includes these as well as others with risk for maternal or fetal harm. Motionless standing results in venous pooling and a significant decrease in cardiac output and thus should be avoided. In fact, one large study of 7,722 pregnancies found that mothers who had jobs requiring predominantly standing had babies with lower birth weights (Naeye and Peters 1982).
Exercise has beneficial effect on hypertension, cardiovascular disease
Currently more than 50 million Americans—and more than 50% of the American population over the age of 60—have hypertension, or high blood pressure (Hagberg 2005).
Currently more than 50 million Americans—and more than 50% of the American population over the age of 60—have hypertension, or high blood pressure (Hagberg2005). Worldwide, the number of people with hypertension is estimated to be 1 billion! Furthermore, because blood pressure tends to increase with age, the number of people with hypertension is likely to rise significantly as the U.S. population continues to age. Unfortunately, due to a lack of symptoms a large number of individuals are unaware that they have the silent killer, as hypertension is called, and do not realize their hypertension is placing them at a higher risk for a heart attack or stroke. Although hypertension affects nearly every organ, its lack of symptoms means that many individuals do not realize the damage that may be occurring even at modest elevations of blood pressure.
Physical activity is considered one of the mainstays in the nonpharmacological treatment of hypertension. This chapter discusses the current definition of hypertension and introduces the physiological relationship between exercise and blood pressure, as well as provides some background and mechanistic details. Then it presents both nationally and internationally issued activity guidelines for individuals with hypertension. Also, because of the close and causal relationship between hypertension and CAD, this chapter also includes guidelines that pertain to CAD.
Benefits of Exercise for Hypertension
The definition of hypertension has changed over time. Currently, the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7: NHBPEP 2003) defines normal blood pressure as a pressure less than 120/80 mmHg (see table 10.1). Elevated blood pressure, which at one time was diagnosed only when in excess of 160/100 mmHg, is a primary cardiac risk factor and also increases the risk for stroke, type 2 diabetes, kidney disease, and vascular disease. According to the JNC 7, the risk of CVD begins at only 115/75 mmHg and doubles with each incremental increase of 20/10 mmHg. People who are classified as prehyper-tensive have twice the risk of developing hypertension. Even individuals with normal blood pressure have a high lifetime risk of developing hypertension—an estimated 90% risk for individuals with normal blood pressure at age 55 (Vasan and others 2002)!
For people with prehypertension, exercise is one of the primary recommended lifestyle changes that can lower blood pressure to a normal level. In fact, even in individuals who have a normal blood pressure, regular aerobic exercise may lower resting blood pressure, although the extent of lowering is less than that seen in individuals with frank hypertension. In the JNC 7, physical activity compares favorably with the other recommended lifestyle changes when it comes to reducing resting blood pressure—table 10.2 gives examples of these changes and their relative effects. Also, physical activity may contribute to weight loss, which can reduce blood pressure even further.
So, although the distensibility or pliability of blood vessels decreases with age and makes hypertension more likely, hypertension is not necessarily an unavoidable consequence of aging, because regular physical activity is clearly effective in preventing hypertension and reducing its intensity. A single session of aerobic exercise creates a sustained hypotensive response that lasts up to 24 h (Hagberg and others 2000), and over time participation in regular physical activity can have long-term benefits. Postulated mechanisms for the reduction of both systolic and diastolic blood pressure that occurs with regular exercise training include the following:
- Reduced visceral fat
- Improved sodium elimination due to altered renal function
- Reduced plasma renin and catecholamine activity
- Reduced sympathetic and increased parasympathetic tone
Because physical activity decreases hypertension, it also reduces the potential contribution of hypertension to cardiovascular risk. In addition to lowering blood pressure, physical activity generally causes a regression of left ventricular hypertrophy, improves lipid profiles, and lowers the risk for type 2 diabetes. This combination of risk reduction has a substantial long-term benefit on cardiovascular risk. There are also notable benefits to other health parameters. Individuals with hypertension may not necessarily achieve normal blood pressure through exercise, but they will likely see improvements in lean body mass, glycemic control, and inflammatory biomarkers.
Overall, a regular physical activity program lowers both systolic and diastolic blood pressure. However, during aerobic exercise, the normal physiological response is a gradually rising systolic blood pressure with a stable or slightly decreasing diastolic blood pressure. In addition, during resistance training and particularly during high-intensity efforts, blood pressure may rise significantly. These natural responses to exercise necessitate guidelines for people with hypertension so that they may receive the benefits of activity safely without increasing their risk for injury or disease.
The use of antihypertensive medications also necessitates physical activity guidelines. Exercise is recommended as an adjunct to antihypertensive medication as there appears to be an additive effect of physical activity with most antihypertensive medications. Beta-blockers, however, may interfere with the antihypertensive effect of exercise (Ades and others 1988). For hypertensive individuals who regularly participate in physical activity, beta-blockers also blunt the peak heart rate and blood pressure; the former effect requires using an alternative to target heart rate for measuring exercise intensity.
Physical activity as play and nutritional goals for children
Because infants and young children are not autonomous, guidelines for this population are aimed at parents, caregivers, schools, and the community.
Because infants and young children are not autonomous, guidelines for this population are aimed at parents, caregivers, schools, and the community. In fact, the next chapter outlines multiple sets of guidelines focusing on community or school policy as a way of promoting physical activity for youths. For preschoolers, it is extremely important that age-appropriate opportunities for physical activity and play be available. Playgrounds offer a variety of activities that may be acceptable for a range of ages, making them a sound option for children. Starting with toddlers and extending through older school-aged children, playground equipment allows for independent play with multiple opportunities to challenge the musculoskeletal, neurological, and psychosocial systems. Many of the guidelines for young children include a call to action for communities to continue to provide ample opportunities for outdoor play in the form of playgrounds and outdoor environments. One author summed up the benefits of playgrounds and physical play as allowing children to BECOME FIT (adapted from Clements 2007).
In addition to physical activity, healthy diet and proper nutrition should begin at an early age. The connection between food and fitness is clearly known; parents and caregivers again have an opportunity to play role model for their children by following healthy eating patterns. Sitting down to meals as a family—particularly breakfast—has been shown to improve communication as well as emotional and psychosocial development. Schoolchildren who eat breakfast perform better academically and have a better chance of meeting all their nutritional needs. Getting adequate amounts of macronutrients, vitamins, minerals, and fiber enables children to have the proper energy to live the active lifestyle that is so important for their present and future health status. Recommendations for appropriate activity and nutrition in children appear in both the IOM report on DRIs and the Dietary Guidelines for Americans. While the 2005 Dietary Guidelines for Americans specifically states that its recommendations apply to children aged 2 y and older, the report on DRIs does not make specific reference to the age at which the youth guidelines apply.
SUMMARY
Guidelines for infants and toddlers are important in that they establish the foundation for a lifetime of physical activity and good health. Although exercise per se is not recommended for very young children, there is an emphasis on developmentally appropriate and enjoyable physical activity. Children in this age group use physical activity to build motor skills that will ultimately pave the way for more formalized physical activity as they grow. Properly supervised opportunities for activity, an avoidance of sedentary time, and the ability to observe and pattern healthy physical activity behaviors in parents and caregivers are key components of guidelines for this age group.
Benefits and risks of physical activity for pregnant women
The goals of physical activity during pregnancy include maintaining a sense of maternal well-being, avoiding fetal harm, and establishing a pattern of regular activity.
The goals of physical activity during pregnancy include maintaining a sense of maternal well-being, avoiding fetal harm, and establishing a pattern of regular activity that will ultimately prevent the onset of chronic disease associated with a sedentary lifestyle. Most women can participate in a wide range of recreational activities and maintain an active lifestyle during pregnancy, although those with medical or obstetrical complications may require modifications. Modifications may also be necessary for women who regularly participated in strenuous recreational or competitive physical activities before their pregnancies. In addition, women who are active before pregnancy may choose to modify their exercise programs somewhat; for example, weight gain or joint laxity may prompt women to walk instead of jog or to exercise indoors instead of outdoors because of improved environmental control. Because of all the physiological changes that occur during pregnancy, activity recommendations for pregnant women are subject to modifications. Finally, concerns for fetal health dictate other changes in order to optimize fetal outcomes.
Nevertheless, the benefits of regular physical activity throughout pregnancy generally outweigh the risks. Women who exercise routinely in the prenatal period have a lower incidence of babies with low birth weight. Starting with the first trimester, regular activity may help ease nausea and lessen fatigue. Body image and mood—both during pregnancy and in the postpartum period—are positively influenced by regular physical activity. Although there are not yet disorder-specific guidelines, it is felt that regular physical activity during pregnancy benefits preeclampsia, hypertension, and gestational diabetes, as mentioned earlier. It is not yet clear whether a regular physical activity program affects gestational length, quality or duration of labor, or incidence of chronic disease in the offspring.
Although the benefits of physical activity for pregnant women are significant, there are still precautions to take and health risks to keep in mind. Because of the increased metabolic rate during pregnancy, thermoregulation during exercise and the potential effect on fetal temperature are a concern. It is important for pregnant exercisers to stay well hydrated in order to improve cooling and maintain blood volume. While the benefits of chronic exercise belong to the mother, the risk of overexercise predominantly affects the fetus (Whaley 2005).
Starting with the second trimester, supine exercises are not recommended, as these can cause the uterus to compress the inferior vena cava and result in decreased cardiac output. Also, prolonged isometric exercise during weightlifting may decrease uterine perfusion. Because of the shift in the expecting mother's center of gravity, exercises that require balance should be avoided later in pregnancy; other anatomical changes of pregnancy are presented in the sidebar. Contact sports and activities that have an increased risk for falls should also be avoided. The new PAGA lists several exercises to avoid; table 6.1 includes these as well as others with risk for maternal or fetal harm. Motionless standing results in venous pooling and a significant decrease in cardiac output and thus should be avoided. In fact, one large study of 7,722 pregnancies found that mothers who had jobs requiring predominantly standing had babies with lower birth weights (Naeye and Peters 1982).
Exercise has beneficial effect on hypertension, cardiovascular disease
Currently more than 50 million Americans—and more than 50% of the American population over the age of 60—have hypertension, or high blood pressure (Hagberg 2005).
Currently more than 50 million Americans—and more than 50% of the American population over the age of 60—have hypertension, or high blood pressure (Hagberg2005). Worldwide, the number of people with hypertension is estimated to be 1 billion! Furthermore, because blood pressure tends to increase with age, the number of people with hypertension is likely to rise significantly as the U.S. population continues to age. Unfortunately, due to a lack of symptoms a large number of individuals are unaware that they have the silent killer, as hypertension is called, and do not realize their hypertension is placing them at a higher risk for a heart attack or stroke. Although hypertension affects nearly every organ, its lack of symptoms means that many individuals do not realize the damage that may be occurring even at modest elevations of blood pressure.
Physical activity is considered one of the mainstays in the nonpharmacological treatment of hypertension. This chapter discusses the current definition of hypertension and introduces the physiological relationship between exercise and blood pressure, as well as provides some background and mechanistic details. Then it presents both nationally and internationally issued activity guidelines for individuals with hypertension. Also, because of the close and causal relationship between hypertension and CAD, this chapter also includes guidelines that pertain to CAD.
Benefits of Exercise for Hypertension
The definition of hypertension has changed over time. Currently, the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7: NHBPEP 2003) defines normal blood pressure as a pressure less than 120/80 mmHg (see table 10.1). Elevated blood pressure, which at one time was diagnosed only when in excess of 160/100 mmHg, is a primary cardiac risk factor and also increases the risk for stroke, type 2 diabetes, kidney disease, and vascular disease. According to the JNC 7, the risk of CVD begins at only 115/75 mmHg and doubles with each incremental increase of 20/10 mmHg. People who are classified as prehyper-tensive have twice the risk of developing hypertension. Even individuals with normal blood pressure have a high lifetime risk of developing hypertension—an estimated 90% risk for individuals with normal blood pressure at age 55 (Vasan and others 2002)!
For people with prehypertension, exercise is one of the primary recommended lifestyle changes that can lower blood pressure to a normal level. In fact, even in individuals who have a normal blood pressure, regular aerobic exercise may lower resting blood pressure, although the extent of lowering is less than that seen in individuals with frank hypertension. In the JNC 7, physical activity compares favorably with the other recommended lifestyle changes when it comes to reducing resting blood pressure—table 10.2 gives examples of these changes and their relative effects. Also, physical activity may contribute to weight loss, which can reduce blood pressure even further.
So, although the distensibility or pliability of blood vessels decreases with age and makes hypertension more likely, hypertension is not necessarily an unavoidable consequence of aging, because regular physical activity is clearly effective in preventing hypertension and reducing its intensity. A single session of aerobic exercise creates a sustained hypotensive response that lasts up to 24 h (Hagberg and others 2000), and over time participation in regular physical activity can have long-term benefits. Postulated mechanisms for the reduction of both systolic and diastolic blood pressure that occurs with regular exercise training include the following:
- Reduced visceral fat
- Improved sodium elimination due to altered renal function
- Reduced plasma renin and catecholamine activity
- Reduced sympathetic and increased parasympathetic tone
Because physical activity decreases hypertension, it also reduces the potential contribution of hypertension to cardiovascular risk. In addition to lowering blood pressure, physical activity generally causes a regression of left ventricular hypertrophy, improves lipid profiles, and lowers the risk for type 2 diabetes. This combination of risk reduction has a substantial long-term benefit on cardiovascular risk. There are also notable benefits to other health parameters. Individuals with hypertension may not necessarily achieve normal blood pressure through exercise, but they will likely see improvements in lean body mass, glycemic control, and inflammatory biomarkers.
Overall, a regular physical activity program lowers both systolic and diastolic blood pressure. However, during aerobic exercise, the normal physiological response is a gradually rising systolic blood pressure with a stable or slightly decreasing diastolic blood pressure. In addition, during resistance training and particularly during high-intensity efforts, blood pressure may rise significantly. These natural responses to exercise necessitate guidelines for people with hypertension so that they may receive the benefits of activity safely without increasing their risk for injury or disease.
The use of antihypertensive medications also necessitates physical activity guidelines. Exercise is recommended as an adjunct to antihypertensive medication as there appears to be an additive effect of physical activity with most antihypertensive medications. Beta-blockers, however, may interfere with the antihypertensive effect of exercise (Ades and others 1988). For hypertensive individuals who regularly participate in physical activity, beta-blockers also blunt the peak heart rate and blood pressure; the former effect requires using an alternative to target heart rate for measuring exercise intensity.
Physical activity as play and nutritional goals for children
Because infants and young children are not autonomous, guidelines for this population are aimed at parents, caregivers, schools, and the community.
Because infants and young children are not autonomous, guidelines for this population are aimed at parents, caregivers, schools, and the community. In fact, the next chapter outlines multiple sets of guidelines focusing on community or school policy as a way of promoting physical activity for youths. For preschoolers, it is extremely important that age-appropriate opportunities for physical activity and play be available. Playgrounds offer a variety of activities that may be acceptable for a range of ages, making them a sound option for children. Starting with toddlers and extending through older school-aged children, playground equipment allows for independent play with multiple opportunities to challenge the musculoskeletal, neurological, and psychosocial systems. Many of the guidelines for young children include a call to action for communities to continue to provide ample opportunities for outdoor play in the form of playgrounds and outdoor environments. One author summed up the benefits of playgrounds and physical play as allowing children to BECOME FIT (adapted from Clements 2007).
In addition to physical activity, healthy diet and proper nutrition should begin at an early age. The connection between food and fitness is clearly known; parents and caregivers again have an opportunity to play role model for their children by following healthy eating patterns. Sitting down to meals as a family—particularly breakfast—has been shown to improve communication as well as emotional and psychosocial development. Schoolchildren who eat breakfast perform better academically and have a better chance of meeting all their nutritional needs. Getting adequate amounts of macronutrients, vitamins, minerals, and fiber enables children to have the proper energy to live the active lifestyle that is so important for their present and future health status. Recommendations for appropriate activity and nutrition in children appear in both the IOM report on DRIs and the Dietary Guidelines for Americans. While the 2005 Dietary Guidelines for Americans specifically states that its recommendations apply to children aged 2 y and older, the report on DRIs does not make specific reference to the age at which the youth guidelines apply.
SUMMARY
Guidelines for infants and toddlers are important in that they establish the foundation for a lifetime of physical activity and good health. Although exercise per se is not recommended for very young children, there is an emphasis on developmentally appropriate and enjoyable physical activity. Children in this age group use physical activity to build motor skills that will ultimately pave the way for more formalized physical activity as they grow. Properly supervised opportunities for activity, an avoidance of sedentary time, and the ability to observe and pattern healthy physical activity behaviors in parents and caregivers are key components of guidelines for this age group.
Benefits and risks of physical activity for pregnant women
The goals of physical activity during pregnancy include maintaining a sense of maternal well-being, avoiding fetal harm, and establishing a pattern of regular activity.
The goals of physical activity during pregnancy include maintaining a sense of maternal well-being, avoiding fetal harm, and establishing a pattern of regular activity that will ultimately prevent the onset of chronic disease associated with a sedentary lifestyle. Most women can participate in a wide range of recreational activities and maintain an active lifestyle during pregnancy, although those with medical or obstetrical complications may require modifications. Modifications may also be necessary for women who regularly participated in strenuous recreational or competitive physical activities before their pregnancies. In addition, women who are active before pregnancy may choose to modify their exercise programs somewhat; for example, weight gain or joint laxity may prompt women to walk instead of jog or to exercise indoors instead of outdoors because of improved environmental control. Because of all the physiological changes that occur during pregnancy, activity recommendations for pregnant women are subject to modifications. Finally, concerns for fetal health dictate other changes in order to optimize fetal outcomes.
Nevertheless, the benefits of regular physical activity throughout pregnancy generally outweigh the risks. Women who exercise routinely in the prenatal period have a lower incidence of babies with low birth weight. Starting with the first trimester, regular activity may help ease nausea and lessen fatigue. Body image and mood—both during pregnancy and in the postpartum period—are positively influenced by regular physical activity. Although there are not yet disorder-specific guidelines, it is felt that regular physical activity during pregnancy benefits preeclampsia, hypertension, and gestational diabetes, as mentioned earlier. It is not yet clear whether a regular physical activity program affects gestational length, quality or duration of labor, or incidence of chronic disease in the offspring.
Although the benefits of physical activity for pregnant women are significant, there are still precautions to take and health risks to keep in mind. Because of the increased metabolic rate during pregnancy, thermoregulation during exercise and the potential effect on fetal temperature are a concern. It is important for pregnant exercisers to stay well hydrated in order to improve cooling and maintain blood volume. While the benefits of chronic exercise belong to the mother, the risk of overexercise predominantly affects the fetus (Whaley 2005).
Starting with the second trimester, supine exercises are not recommended, as these can cause the uterus to compress the inferior vena cava and result in decreased cardiac output. Also, prolonged isometric exercise during weightlifting may decrease uterine perfusion. Because of the shift in the expecting mother's center of gravity, exercises that require balance should be avoided later in pregnancy; other anatomical changes of pregnancy are presented in the sidebar. Contact sports and activities that have an increased risk for falls should also be avoided. The new PAGA lists several exercises to avoid; table 6.1 includes these as well as others with risk for maternal or fetal harm. Motionless standing results in venous pooling and a significant decrease in cardiac output and thus should be avoided. In fact, one large study of 7,722 pregnancies found that mothers who had jobs requiring predominantly standing had babies with lower birth weights (Naeye and Peters 1982).
Exercise has beneficial effect on hypertension, cardiovascular disease
Currently more than 50 million Americans—and more than 50% of the American population over the age of 60—have hypertension, or high blood pressure (Hagberg 2005).
Currently more than 50 million Americans—and more than 50% of the American population over the age of 60—have hypertension, or high blood pressure (Hagberg2005). Worldwide, the number of people with hypertension is estimated to be 1 billion! Furthermore, because blood pressure tends to increase with age, the number of people with hypertension is likely to rise significantly as the U.S. population continues to age. Unfortunately, due to a lack of symptoms a large number of individuals are unaware that they have the silent killer, as hypertension is called, and do not realize their hypertension is placing them at a higher risk for a heart attack or stroke. Although hypertension affects nearly every organ, its lack of symptoms means that many individuals do not realize the damage that may be occurring even at modest elevations of blood pressure.
Physical activity is considered one of the mainstays in the nonpharmacological treatment of hypertension. This chapter discusses the current definition of hypertension and introduces the physiological relationship between exercise and blood pressure, as well as provides some background and mechanistic details. Then it presents both nationally and internationally issued activity guidelines for individuals with hypertension. Also, because of the close and causal relationship between hypertension and CAD, this chapter also includes guidelines that pertain to CAD.
Benefits of Exercise for Hypertension
The definition of hypertension has changed over time. Currently, the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7: NHBPEP 2003) defines normal blood pressure as a pressure less than 120/80 mmHg (see table 10.1). Elevated blood pressure, which at one time was diagnosed only when in excess of 160/100 mmHg, is a primary cardiac risk factor and also increases the risk for stroke, type 2 diabetes, kidney disease, and vascular disease. According to the JNC 7, the risk of CVD begins at only 115/75 mmHg and doubles with each incremental increase of 20/10 mmHg. People who are classified as prehyper-tensive have twice the risk of developing hypertension. Even individuals with normal blood pressure have a high lifetime risk of developing hypertension—an estimated 90% risk for individuals with normal blood pressure at age 55 (Vasan and others 2002)!
For people with prehypertension, exercise is one of the primary recommended lifestyle changes that can lower blood pressure to a normal level. In fact, even in individuals who have a normal blood pressure, regular aerobic exercise may lower resting blood pressure, although the extent of lowering is less than that seen in individuals with frank hypertension. In the JNC 7, physical activity compares favorably with the other recommended lifestyle changes when it comes to reducing resting blood pressure—table 10.2 gives examples of these changes and their relative effects. Also, physical activity may contribute to weight loss, which can reduce blood pressure even further.
So, although the distensibility or pliability of blood vessels decreases with age and makes hypertension more likely, hypertension is not necessarily an unavoidable consequence of aging, because regular physical activity is clearly effective in preventing hypertension and reducing its intensity. A single session of aerobic exercise creates a sustained hypotensive response that lasts up to 24 h (Hagberg and others 2000), and over time participation in regular physical activity can have long-term benefits. Postulated mechanisms for the reduction of both systolic and diastolic blood pressure that occurs with regular exercise training include the following:
- Reduced visceral fat
- Improved sodium elimination due to altered renal function
- Reduced plasma renin and catecholamine activity
- Reduced sympathetic and increased parasympathetic tone
Because physical activity decreases hypertension, it also reduces the potential contribution of hypertension to cardiovascular risk. In addition to lowering blood pressure, physical activity generally causes a regression of left ventricular hypertrophy, improves lipid profiles, and lowers the risk for type 2 diabetes. This combination of risk reduction has a substantial long-term benefit on cardiovascular risk. There are also notable benefits to other health parameters. Individuals with hypertension may not necessarily achieve normal blood pressure through exercise, but they will likely see improvements in lean body mass, glycemic control, and inflammatory biomarkers.
Overall, a regular physical activity program lowers both systolic and diastolic blood pressure. However, during aerobic exercise, the normal physiological response is a gradually rising systolic blood pressure with a stable or slightly decreasing diastolic blood pressure. In addition, during resistance training and particularly during high-intensity efforts, blood pressure may rise significantly. These natural responses to exercise necessitate guidelines for people with hypertension so that they may receive the benefits of activity safely without increasing their risk for injury or disease.
The use of antihypertensive medications also necessitates physical activity guidelines. Exercise is recommended as an adjunct to antihypertensive medication as there appears to be an additive effect of physical activity with most antihypertensive medications. Beta-blockers, however, may interfere with the antihypertensive effect of exercise (Ades and others 1988). For hypertensive individuals who regularly participate in physical activity, beta-blockers also blunt the peak heart rate and blood pressure; the former effect requires using an alternative to target heart rate for measuring exercise intensity.
Physical activity as play and nutritional goals for children
Because infants and young children are not autonomous, guidelines for this population are aimed at parents, caregivers, schools, and the community.
Because infants and young children are not autonomous, guidelines for this population are aimed at parents, caregivers, schools, and the community. In fact, the next chapter outlines multiple sets of guidelines focusing on community or school policy as a way of promoting physical activity for youths. For preschoolers, it is extremely important that age-appropriate opportunities for physical activity and play be available. Playgrounds offer a variety of activities that may be acceptable for a range of ages, making them a sound option for children. Starting with toddlers and extending through older school-aged children, playground equipment allows for independent play with multiple opportunities to challenge the musculoskeletal, neurological, and psychosocial systems. Many of the guidelines for young children include a call to action for communities to continue to provide ample opportunities for outdoor play in the form of playgrounds and outdoor environments. One author summed up the benefits of playgrounds and physical play as allowing children to BECOME FIT (adapted from Clements 2007).
In addition to physical activity, healthy diet and proper nutrition should begin at an early age. The connection between food and fitness is clearly known; parents and caregivers again have an opportunity to play role model for their children by following healthy eating patterns. Sitting down to meals as a family—particularly breakfast—has been shown to improve communication as well as emotional and psychosocial development. Schoolchildren who eat breakfast perform better academically and have a better chance of meeting all their nutritional needs. Getting adequate amounts of macronutrients, vitamins, minerals, and fiber enables children to have the proper energy to live the active lifestyle that is so important for their present and future health status. Recommendations for appropriate activity and nutrition in children appear in both the IOM report on DRIs and the Dietary Guidelines for Americans. While the 2005 Dietary Guidelines for Americans specifically states that its recommendations apply to children aged 2 y and older, the report on DRIs does not make specific reference to the age at which the youth guidelines apply.
SUMMARY
Guidelines for infants and toddlers are important in that they establish the foundation for a lifetime of physical activity and good health. Although exercise per se is not recommended for very young children, there is an emphasis on developmentally appropriate and enjoyable physical activity. Children in this age group use physical activity to build motor skills that will ultimately pave the way for more formalized physical activity as they grow. Properly supervised opportunities for activity, an avoidance of sedentary time, and the ability to observe and pattern healthy physical activity behaviors in parents and caregivers are key components of guidelines for this age group.
Benefits and risks of physical activity for pregnant women
The goals of physical activity during pregnancy include maintaining a sense of maternal well-being, avoiding fetal harm, and establishing a pattern of regular activity.
The goals of physical activity during pregnancy include maintaining a sense of maternal well-being, avoiding fetal harm, and establishing a pattern of regular activity that will ultimately prevent the onset of chronic disease associated with a sedentary lifestyle. Most women can participate in a wide range of recreational activities and maintain an active lifestyle during pregnancy, although those with medical or obstetrical complications may require modifications. Modifications may also be necessary for women who regularly participated in strenuous recreational or competitive physical activities before their pregnancies. In addition, women who are active before pregnancy may choose to modify their exercise programs somewhat; for example, weight gain or joint laxity may prompt women to walk instead of jog or to exercise indoors instead of outdoors because of improved environmental control. Because of all the physiological changes that occur during pregnancy, activity recommendations for pregnant women are subject to modifications. Finally, concerns for fetal health dictate other changes in order to optimize fetal outcomes.
Nevertheless, the benefits of regular physical activity throughout pregnancy generally outweigh the risks. Women who exercise routinely in the prenatal period have a lower incidence of babies with low birth weight. Starting with the first trimester, regular activity may help ease nausea and lessen fatigue. Body image and mood—both during pregnancy and in the postpartum period—are positively influenced by regular physical activity. Although there are not yet disorder-specific guidelines, it is felt that regular physical activity during pregnancy benefits preeclampsia, hypertension, and gestational diabetes, as mentioned earlier. It is not yet clear whether a regular physical activity program affects gestational length, quality or duration of labor, or incidence of chronic disease in the offspring.
Although the benefits of physical activity for pregnant women are significant, there are still precautions to take and health risks to keep in mind. Because of the increased metabolic rate during pregnancy, thermoregulation during exercise and the potential effect on fetal temperature are a concern. It is important for pregnant exercisers to stay well hydrated in order to improve cooling and maintain blood volume. While the benefits of chronic exercise belong to the mother, the risk of overexercise predominantly affects the fetus (Whaley 2005).
Starting with the second trimester, supine exercises are not recommended, as these can cause the uterus to compress the inferior vena cava and result in decreased cardiac output. Also, prolonged isometric exercise during weightlifting may decrease uterine perfusion. Because of the shift in the expecting mother's center of gravity, exercises that require balance should be avoided later in pregnancy; other anatomical changes of pregnancy are presented in the sidebar. Contact sports and activities that have an increased risk for falls should also be avoided. The new PAGA lists several exercises to avoid; table 6.1 includes these as well as others with risk for maternal or fetal harm. Motionless standing results in venous pooling and a significant decrease in cardiac output and thus should be avoided. In fact, one large study of 7,722 pregnancies found that mothers who had jobs requiring predominantly standing had babies with lower birth weights (Naeye and Peters 1982).
Exercise has beneficial effect on hypertension, cardiovascular disease
Currently more than 50 million Americans—and more than 50% of the American population over the age of 60—have hypertension, or high blood pressure (Hagberg 2005).
Currently more than 50 million Americans—and more than 50% of the American population over the age of 60—have hypertension, or high blood pressure (Hagberg2005). Worldwide, the number of people with hypertension is estimated to be 1 billion! Furthermore, because blood pressure tends to increase with age, the number of people with hypertension is likely to rise significantly as the U.S. population continues to age. Unfortunately, due to a lack of symptoms a large number of individuals are unaware that they have the silent killer, as hypertension is called, and do not realize their hypertension is placing them at a higher risk for a heart attack or stroke. Although hypertension affects nearly every organ, its lack of symptoms means that many individuals do not realize the damage that may be occurring even at modest elevations of blood pressure.
Physical activity is considered one of the mainstays in the nonpharmacological treatment of hypertension. This chapter discusses the current definition of hypertension and introduces the physiological relationship between exercise and blood pressure, as well as provides some background and mechanistic details. Then it presents both nationally and internationally issued activity guidelines for individuals with hypertension. Also, because of the close and causal relationship between hypertension and CAD, this chapter also includes guidelines that pertain to CAD.
Benefits of Exercise for Hypertension
The definition of hypertension has changed over time. Currently, the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7: NHBPEP 2003) defines normal blood pressure as a pressure less than 120/80 mmHg (see table 10.1). Elevated blood pressure, which at one time was diagnosed only when in excess of 160/100 mmHg, is a primary cardiac risk factor and also increases the risk for stroke, type 2 diabetes, kidney disease, and vascular disease. According to the JNC 7, the risk of CVD begins at only 115/75 mmHg and doubles with each incremental increase of 20/10 mmHg. People who are classified as prehyper-tensive have twice the risk of developing hypertension. Even individuals with normal blood pressure have a high lifetime risk of developing hypertension—an estimated 90% risk for individuals with normal blood pressure at age 55 (Vasan and others 2002)!
For people with prehypertension, exercise is one of the primary recommended lifestyle changes that can lower blood pressure to a normal level. In fact, even in individuals who have a normal blood pressure, regular aerobic exercise may lower resting blood pressure, although the extent of lowering is less than that seen in individuals with frank hypertension. In the JNC 7, physical activity compares favorably with the other recommended lifestyle changes when it comes to reducing resting blood pressure—table 10.2 gives examples of these changes and their relative effects. Also, physical activity may contribute to weight loss, which can reduce blood pressure even further.
So, although the distensibility or pliability of blood vessels decreases with age and makes hypertension more likely, hypertension is not necessarily an unavoidable consequence of aging, because regular physical activity is clearly effective in preventing hypertension and reducing its intensity. A single session of aerobic exercise creates a sustained hypotensive response that lasts up to 24 h (Hagberg and others 2000), and over time participation in regular physical activity can have long-term benefits. Postulated mechanisms for the reduction of both systolic and diastolic blood pressure that occurs with regular exercise training include the following:
- Reduced visceral fat
- Improved sodium elimination due to altered renal function
- Reduced plasma renin and catecholamine activity
- Reduced sympathetic and increased parasympathetic tone
Because physical activity decreases hypertension, it also reduces the potential contribution of hypertension to cardiovascular risk. In addition to lowering blood pressure, physical activity generally causes a regression of left ventricular hypertrophy, improves lipid profiles, and lowers the risk for type 2 diabetes. This combination of risk reduction has a substantial long-term benefit on cardiovascular risk. There are also notable benefits to other health parameters. Individuals with hypertension may not necessarily achieve normal blood pressure through exercise, but they will likely see improvements in lean body mass, glycemic control, and inflammatory biomarkers.
Overall, a regular physical activity program lowers both systolic and diastolic blood pressure. However, during aerobic exercise, the normal physiological response is a gradually rising systolic blood pressure with a stable or slightly decreasing diastolic blood pressure. In addition, during resistance training and particularly during high-intensity efforts, blood pressure may rise significantly. These natural responses to exercise necessitate guidelines for people with hypertension so that they may receive the benefits of activity safely without increasing their risk for injury or disease.
The use of antihypertensive medications also necessitates physical activity guidelines. Exercise is recommended as an adjunct to antihypertensive medication as there appears to be an additive effect of physical activity with most antihypertensive medications. Beta-blockers, however, may interfere with the antihypertensive effect of exercise (Ades and others 1988). For hypertensive individuals who regularly participate in physical activity, beta-blockers also blunt the peak heart rate and blood pressure; the former effect requires using an alternative to target heart rate for measuring exercise intensity.
Physical activity as play and nutritional goals for children
Because infants and young children are not autonomous, guidelines for this population are aimed at parents, caregivers, schools, and the community.
Because infants and young children are not autonomous, guidelines for this population are aimed at parents, caregivers, schools, and the community. In fact, the next chapter outlines multiple sets of guidelines focusing on community or school policy as a way of promoting physical activity for youths. For preschoolers, it is extremely important that age-appropriate opportunities for physical activity and play be available. Playgrounds offer a variety of activities that may be acceptable for a range of ages, making them a sound option for children. Starting with toddlers and extending through older school-aged children, playground equipment allows for independent play with multiple opportunities to challenge the musculoskeletal, neurological, and psychosocial systems. Many of the guidelines for young children include a call to action for communities to continue to provide ample opportunities for outdoor play in the form of playgrounds and outdoor environments. One author summed up the benefits of playgrounds and physical play as allowing children to BECOME FIT (adapted from Clements 2007).
In addition to physical activity, healthy diet and proper nutrition should begin at an early age. The connection between food and fitness is clearly known; parents and caregivers again have an opportunity to play role model for their children by following healthy eating patterns. Sitting down to meals as a family—particularly breakfast—has been shown to improve communication as well as emotional and psychosocial development. Schoolchildren who eat breakfast perform better academically and have a better chance of meeting all their nutritional needs. Getting adequate amounts of macronutrients, vitamins, minerals, and fiber enables children to have the proper energy to live the active lifestyle that is so important for their present and future health status. Recommendations for appropriate activity and nutrition in children appear in both the IOM report on DRIs and the Dietary Guidelines for Americans. While the 2005 Dietary Guidelines for Americans specifically states that its recommendations apply to children aged 2 y and older, the report on DRIs does not make specific reference to the age at which the youth guidelines apply.
SUMMARY
Guidelines for infants and toddlers are important in that they establish the foundation for a lifetime of physical activity and good health. Although exercise per se is not recommended for very young children, there is an emphasis on developmentally appropriate and enjoyable physical activity. Children in this age group use physical activity to build motor skills that will ultimately pave the way for more formalized physical activity as they grow. Properly supervised opportunities for activity, an avoidance of sedentary time, and the ability to observe and pattern healthy physical activity behaviors in parents and caregivers are key components of guidelines for this age group.
Benefits and risks of physical activity for pregnant women
The goals of physical activity during pregnancy include maintaining a sense of maternal well-being, avoiding fetal harm, and establishing a pattern of regular activity.
The goals of physical activity during pregnancy include maintaining a sense of maternal well-being, avoiding fetal harm, and establishing a pattern of regular activity that will ultimately prevent the onset of chronic disease associated with a sedentary lifestyle. Most women can participate in a wide range of recreational activities and maintain an active lifestyle during pregnancy, although those with medical or obstetrical complications may require modifications. Modifications may also be necessary for women who regularly participated in strenuous recreational or competitive physical activities before their pregnancies. In addition, women who are active before pregnancy may choose to modify their exercise programs somewhat; for example, weight gain or joint laxity may prompt women to walk instead of jog or to exercise indoors instead of outdoors because of improved environmental control. Because of all the physiological changes that occur during pregnancy, activity recommendations for pregnant women are subject to modifications. Finally, concerns for fetal health dictate other changes in order to optimize fetal outcomes.
Nevertheless, the benefits of regular physical activity throughout pregnancy generally outweigh the risks. Women who exercise routinely in the prenatal period have a lower incidence of babies with low birth weight. Starting with the first trimester, regular activity may help ease nausea and lessen fatigue. Body image and mood—both during pregnancy and in the postpartum period—are positively influenced by regular physical activity. Although there are not yet disorder-specific guidelines, it is felt that regular physical activity during pregnancy benefits preeclampsia, hypertension, and gestational diabetes, as mentioned earlier. It is not yet clear whether a regular physical activity program affects gestational length, quality or duration of labor, or incidence of chronic disease in the offspring.
Although the benefits of physical activity for pregnant women are significant, there are still precautions to take and health risks to keep in mind. Because of the increased metabolic rate during pregnancy, thermoregulation during exercise and the potential effect on fetal temperature are a concern. It is important for pregnant exercisers to stay well hydrated in order to improve cooling and maintain blood volume. While the benefits of chronic exercise belong to the mother, the risk of overexercise predominantly affects the fetus (Whaley 2005).
Starting with the second trimester, supine exercises are not recommended, as these can cause the uterus to compress the inferior vena cava and result in decreased cardiac output. Also, prolonged isometric exercise during weightlifting may decrease uterine perfusion. Because of the shift in the expecting mother's center of gravity, exercises that require balance should be avoided later in pregnancy; other anatomical changes of pregnancy are presented in the sidebar. Contact sports and activities that have an increased risk for falls should also be avoided. The new PAGA lists several exercises to avoid; table 6.1 includes these as well as others with risk for maternal or fetal harm. Motionless standing results in venous pooling and a significant decrease in cardiac output and thus should be avoided. In fact, one large study of 7,722 pregnancies found that mothers who had jobs requiring predominantly standing had babies with lower birth weights (Naeye and Peters 1982).
Exercise has beneficial effect on hypertension, cardiovascular disease
Currently more than 50 million Americans—and more than 50% of the American population over the age of 60—have hypertension, or high blood pressure (Hagberg 2005).
Currently more than 50 million Americans—and more than 50% of the American population over the age of 60—have hypertension, or high blood pressure (Hagberg2005). Worldwide, the number of people with hypertension is estimated to be 1 billion! Furthermore, because blood pressure tends to increase with age, the number of people with hypertension is likely to rise significantly as the U.S. population continues to age. Unfortunately, due to a lack of symptoms a large number of individuals are unaware that they have the silent killer, as hypertension is called, and do not realize their hypertension is placing them at a higher risk for a heart attack or stroke. Although hypertension affects nearly every organ, its lack of symptoms means that many individuals do not realize the damage that may be occurring even at modest elevations of blood pressure.
Physical activity is considered one of the mainstays in the nonpharmacological treatment of hypertension. This chapter discusses the current definition of hypertension and introduces the physiological relationship between exercise and blood pressure, as well as provides some background and mechanistic details. Then it presents both nationally and internationally issued activity guidelines for individuals with hypertension. Also, because of the close and causal relationship between hypertension and CAD, this chapter also includes guidelines that pertain to CAD.
Benefits of Exercise for Hypertension
The definition of hypertension has changed over time. Currently, the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7: NHBPEP 2003) defines normal blood pressure as a pressure less than 120/80 mmHg (see table 10.1). Elevated blood pressure, which at one time was diagnosed only when in excess of 160/100 mmHg, is a primary cardiac risk factor and also increases the risk for stroke, type 2 diabetes, kidney disease, and vascular disease. According to the JNC 7, the risk of CVD begins at only 115/75 mmHg and doubles with each incremental increase of 20/10 mmHg. People who are classified as prehyper-tensive have twice the risk of developing hypertension. Even individuals with normal blood pressure have a high lifetime risk of developing hypertension—an estimated 90% risk for individuals with normal blood pressure at age 55 (Vasan and others 2002)!
For people with prehypertension, exercise is one of the primary recommended lifestyle changes that can lower blood pressure to a normal level. In fact, even in individuals who have a normal blood pressure, regular aerobic exercise may lower resting blood pressure, although the extent of lowering is less than that seen in individuals with frank hypertension. In the JNC 7, physical activity compares favorably with the other recommended lifestyle changes when it comes to reducing resting blood pressure—table 10.2 gives examples of these changes and their relative effects. Also, physical activity may contribute to weight loss, which can reduce blood pressure even further.
So, although the distensibility or pliability of blood vessels decreases with age and makes hypertension more likely, hypertension is not necessarily an unavoidable consequence of aging, because regular physical activity is clearly effective in preventing hypertension and reducing its intensity. A single session of aerobic exercise creates a sustained hypotensive response that lasts up to 24 h (Hagberg and others 2000), and over time participation in regular physical activity can have long-term benefits. Postulated mechanisms for the reduction of both systolic and diastolic blood pressure that occurs with regular exercise training include the following:
- Reduced visceral fat
- Improved sodium elimination due to altered renal function
- Reduced plasma renin and catecholamine activity
- Reduced sympathetic and increased parasympathetic tone
Because physical activity decreases hypertension, it also reduces the potential contribution of hypertension to cardiovascular risk. In addition to lowering blood pressure, physical activity generally causes a regression of left ventricular hypertrophy, improves lipid profiles, and lowers the risk for type 2 diabetes. This combination of risk reduction has a substantial long-term benefit on cardiovascular risk. There are also notable benefits to other health parameters. Individuals with hypertension may not necessarily achieve normal blood pressure through exercise, but they will likely see improvements in lean body mass, glycemic control, and inflammatory biomarkers.
Overall, a regular physical activity program lowers both systolic and diastolic blood pressure. However, during aerobic exercise, the normal physiological response is a gradually rising systolic blood pressure with a stable or slightly decreasing diastolic blood pressure. In addition, during resistance training and particularly during high-intensity efforts, blood pressure may rise significantly. These natural responses to exercise necessitate guidelines for people with hypertension so that they may receive the benefits of activity safely without increasing their risk for injury or disease.
The use of antihypertensive medications also necessitates physical activity guidelines. Exercise is recommended as an adjunct to antihypertensive medication as there appears to be an additive effect of physical activity with most antihypertensive medications. Beta-blockers, however, may interfere with the antihypertensive effect of exercise (Ades and others 1988). For hypertensive individuals who regularly participate in physical activity, beta-blockers also blunt the peak heart rate and blood pressure; the former effect requires using an alternative to target heart rate for measuring exercise intensity.
Physical activity as play and nutritional goals for children
Because infants and young children are not autonomous, guidelines for this population are aimed at parents, caregivers, schools, and the community.
Because infants and young children are not autonomous, guidelines for this population are aimed at parents, caregivers, schools, and the community. In fact, the next chapter outlines multiple sets of guidelines focusing on community or school policy as a way of promoting physical activity for youths. For preschoolers, it is extremely important that age-appropriate opportunities for physical activity and play be available. Playgrounds offer a variety of activities that may be acceptable for a range of ages, making them a sound option for children. Starting with toddlers and extending through older school-aged children, playground equipment allows for independent play with multiple opportunities to challenge the musculoskeletal, neurological, and psychosocial systems. Many of the guidelines for young children include a call to action for communities to continue to provide ample opportunities for outdoor play in the form of playgrounds and outdoor environments. One author summed up the benefits of playgrounds and physical play as allowing children to BECOME FIT (adapted from Clements 2007).
In addition to physical activity, healthy diet and proper nutrition should begin at an early age. The connection between food and fitness is clearly known; parents and caregivers again have an opportunity to play role model for their children by following healthy eating patterns. Sitting down to meals as a family—particularly breakfast—has been shown to improve communication as well as emotional and psychosocial development. Schoolchildren who eat breakfast perform better academically and have a better chance of meeting all their nutritional needs. Getting adequate amounts of macronutrients, vitamins, minerals, and fiber enables children to have the proper energy to live the active lifestyle that is so important for their present and future health status. Recommendations for appropriate activity and nutrition in children appear in both the IOM report on DRIs and the Dietary Guidelines for Americans. While the 2005 Dietary Guidelines for Americans specifically states that its recommendations apply to children aged 2 y and older, the report on DRIs does not make specific reference to the age at which the youth guidelines apply.
SUMMARY
Guidelines for infants and toddlers are important in that they establish the foundation for a lifetime of physical activity and good health. Although exercise per se is not recommended for very young children, there is an emphasis on developmentally appropriate and enjoyable physical activity. Children in this age group use physical activity to build motor skills that will ultimately pave the way for more formalized physical activity as they grow. Properly supervised opportunities for activity, an avoidance of sedentary time, and the ability to observe and pattern healthy physical activity behaviors in parents and caregivers are key components of guidelines for this age group.
Benefits and risks of physical activity for pregnant women
The goals of physical activity during pregnancy include maintaining a sense of maternal well-being, avoiding fetal harm, and establishing a pattern of regular activity.
The goals of physical activity during pregnancy include maintaining a sense of maternal well-being, avoiding fetal harm, and establishing a pattern of regular activity that will ultimately prevent the onset of chronic disease associated with a sedentary lifestyle. Most women can participate in a wide range of recreational activities and maintain an active lifestyle during pregnancy, although those with medical or obstetrical complications may require modifications. Modifications may also be necessary for women who regularly participated in strenuous recreational or competitive physical activities before their pregnancies. In addition, women who are active before pregnancy may choose to modify their exercise programs somewhat; for example, weight gain or joint laxity may prompt women to walk instead of jog or to exercise indoors instead of outdoors because of improved environmental control. Because of all the physiological changes that occur during pregnancy, activity recommendations for pregnant women are subject to modifications. Finally, concerns for fetal health dictate other changes in order to optimize fetal outcomes.
Nevertheless, the benefits of regular physical activity throughout pregnancy generally outweigh the risks. Women who exercise routinely in the prenatal period have a lower incidence of babies with low birth weight. Starting with the first trimester, regular activity may help ease nausea and lessen fatigue. Body image and mood—both during pregnancy and in the postpartum period—are positively influenced by regular physical activity. Although there are not yet disorder-specific guidelines, it is felt that regular physical activity during pregnancy benefits preeclampsia, hypertension, and gestational diabetes, as mentioned earlier. It is not yet clear whether a regular physical activity program affects gestational length, quality or duration of labor, or incidence of chronic disease in the offspring.
Although the benefits of physical activity for pregnant women are significant, there are still precautions to take and health risks to keep in mind. Because of the increased metabolic rate during pregnancy, thermoregulation during exercise and the potential effect on fetal temperature are a concern. It is important for pregnant exercisers to stay well hydrated in order to improve cooling and maintain blood volume. While the benefits of chronic exercise belong to the mother, the risk of overexercise predominantly affects the fetus (Whaley 2005).
Starting with the second trimester, supine exercises are not recommended, as these can cause the uterus to compress the inferior vena cava and result in decreased cardiac output. Also, prolonged isometric exercise during weightlifting may decrease uterine perfusion. Because of the shift in the expecting mother's center of gravity, exercises that require balance should be avoided later in pregnancy; other anatomical changes of pregnancy are presented in the sidebar. Contact sports and activities that have an increased risk for falls should also be avoided. The new PAGA lists several exercises to avoid; table 6.1 includes these as well as others with risk for maternal or fetal harm. Motionless standing results in venous pooling and a significant decrease in cardiac output and thus should be avoided. In fact, one large study of 7,722 pregnancies found that mothers who had jobs requiring predominantly standing had babies with lower birth weights (Naeye and Peters 1982).
Exercise has beneficial effect on hypertension, cardiovascular disease
Currently more than 50 million Americans—and more than 50% of the American population over the age of 60—have hypertension, or high blood pressure (Hagberg 2005).
Currently more than 50 million Americans—and more than 50% of the American population over the age of 60—have hypertension, or high blood pressure (Hagberg2005). Worldwide, the number of people with hypertension is estimated to be 1 billion! Furthermore, because blood pressure tends to increase with age, the number of people with hypertension is likely to rise significantly as the U.S. population continues to age. Unfortunately, due to a lack of symptoms a large number of individuals are unaware that they have the silent killer, as hypertension is called, and do not realize their hypertension is placing them at a higher risk for a heart attack or stroke. Although hypertension affects nearly every organ, its lack of symptoms means that many individuals do not realize the damage that may be occurring even at modest elevations of blood pressure.
Physical activity is considered one of the mainstays in the nonpharmacological treatment of hypertension. This chapter discusses the current definition of hypertension and introduces the physiological relationship between exercise and blood pressure, as well as provides some background and mechanistic details. Then it presents both nationally and internationally issued activity guidelines for individuals with hypertension. Also, because of the close and causal relationship between hypertension and CAD, this chapter also includes guidelines that pertain to CAD.
Benefits of Exercise for Hypertension
The definition of hypertension has changed over time. Currently, the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7: NHBPEP 2003) defines normal blood pressure as a pressure less than 120/80 mmHg (see table 10.1). Elevated blood pressure, which at one time was diagnosed only when in excess of 160/100 mmHg, is a primary cardiac risk factor and also increases the risk for stroke, type 2 diabetes, kidney disease, and vascular disease. According to the JNC 7, the risk of CVD begins at only 115/75 mmHg and doubles with each incremental increase of 20/10 mmHg. People who are classified as prehyper-tensive have twice the risk of developing hypertension. Even individuals with normal blood pressure have a high lifetime risk of developing hypertension—an estimated 90% risk for individuals with normal blood pressure at age 55 (Vasan and others 2002)!
For people with prehypertension, exercise is one of the primary recommended lifestyle changes that can lower blood pressure to a normal level. In fact, even in individuals who have a normal blood pressure, regular aerobic exercise may lower resting blood pressure, although the extent of lowering is less than that seen in individuals with frank hypertension. In the JNC 7, physical activity compares favorably with the other recommended lifestyle changes when it comes to reducing resting blood pressure—table 10.2 gives examples of these changes and their relative effects. Also, physical activity may contribute to weight loss, which can reduce blood pressure even further.
So, although the distensibility or pliability of blood vessels decreases with age and makes hypertension more likely, hypertension is not necessarily an unavoidable consequence of aging, because regular physical activity is clearly effective in preventing hypertension and reducing its intensity. A single session of aerobic exercise creates a sustained hypotensive response that lasts up to 24 h (Hagberg and others 2000), and over time participation in regular physical activity can have long-term benefits. Postulated mechanisms for the reduction of both systolic and diastolic blood pressure that occurs with regular exercise training include the following:
- Reduced visceral fat
- Improved sodium elimination due to altered renal function
- Reduced plasma renin and catecholamine activity
- Reduced sympathetic and increased parasympathetic tone
Because physical activity decreases hypertension, it also reduces the potential contribution of hypertension to cardiovascular risk. In addition to lowering blood pressure, physical activity generally causes a regression of left ventricular hypertrophy, improves lipid profiles, and lowers the risk for type 2 diabetes. This combination of risk reduction has a substantial long-term benefit on cardiovascular risk. There are also notable benefits to other health parameters. Individuals with hypertension may not necessarily achieve normal blood pressure through exercise, but they will likely see improvements in lean body mass, glycemic control, and inflammatory biomarkers.
Overall, a regular physical activity program lowers both systolic and diastolic blood pressure. However, during aerobic exercise, the normal physiological response is a gradually rising systolic blood pressure with a stable or slightly decreasing diastolic blood pressure. In addition, during resistance training and particularly during high-intensity efforts, blood pressure may rise significantly. These natural responses to exercise necessitate guidelines for people with hypertension so that they may receive the benefits of activity safely without increasing their risk for injury or disease.
The use of antihypertensive medications also necessitates physical activity guidelines. Exercise is recommended as an adjunct to antihypertensive medication as there appears to be an additive effect of physical activity with most antihypertensive medications. Beta-blockers, however, may interfere with the antihypertensive effect of exercise (Ades and others 1988). For hypertensive individuals who regularly participate in physical activity, beta-blockers also blunt the peak heart rate and blood pressure; the former effect requires using an alternative to target heart rate for measuring exercise intensity.
Physical activity as play and nutritional goals for children
Because infants and young children are not autonomous, guidelines for this population are aimed at parents, caregivers, schools, and the community.
Because infants and young children are not autonomous, guidelines for this population are aimed at parents, caregivers, schools, and the community. In fact, the next chapter outlines multiple sets of guidelines focusing on community or school policy as a way of promoting physical activity for youths. For preschoolers, it is extremely important that age-appropriate opportunities for physical activity and play be available. Playgrounds offer a variety of activities that may be acceptable for a range of ages, making them a sound option for children. Starting with toddlers and extending through older school-aged children, playground equipment allows for independent play with multiple opportunities to challenge the musculoskeletal, neurological, and psychosocial systems. Many of the guidelines for young children include a call to action for communities to continue to provide ample opportunities for outdoor play in the form of playgrounds and outdoor environments. One author summed up the benefits of playgrounds and physical play as allowing children to BECOME FIT (adapted from Clements 2007).
In addition to physical activity, healthy diet and proper nutrition should begin at an early age. The connection between food and fitness is clearly known; parents and caregivers again have an opportunity to play role model for their children by following healthy eating patterns. Sitting down to meals as a family—particularly breakfast—has been shown to improve communication as well as emotional and psychosocial development. Schoolchildren who eat breakfast perform better academically and have a better chance of meeting all their nutritional needs. Getting adequate amounts of macronutrients, vitamins, minerals, and fiber enables children to have the proper energy to live the active lifestyle that is so important for their present and future health status. Recommendations for appropriate activity and nutrition in children appear in both the IOM report on DRIs and the Dietary Guidelines for Americans. While the 2005 Dietary Guidelines for Americans specifically states that its recommendations apply to children aged 2 y and older, the report on DRIs does not make specific reference to the age at which the youth guidelines apply.
SUMMARY
Guidelines for infants and toddlers are important in that they establish the foundation for a lifetime of physical activity and good health. Although exercise per se is not recommended for very young children, there is an emphasis on developmentally appropriate and enjoyable physical activity. Children in this age group use physical activity to build motor skills that will ultimately pave the way for more formalized physical activity as they grow. Properly supervised opportunities for activity, an avoidance of sedentary time, and the ability to observe and pattern healthy physical activity behaviors in parents and caregivers are key components of guidelines for this age group.
Benefits and risks of physical activity for pregnant women
The goals of physical activity during pregnancy include maintaining a sense of maternal well-being, avoiding fetal harm, and establishing a pattern of regular activity.
The goals of physical activity during pregnancy include maintaining a sense of maternal well-being, avoiding fetal harm, and establishing a pattern of regular activity that will ultimately prevent the onset of chronic disease associated with a sedentary lifestyle. Most women can participate in a wide range of recreational activities and maintain an active lifestyle during pregnancy, although those with medical or obstetrical complications may require modifications. Modifications may also be necessary for women who regularly participated in strenuous recreational or competitive physical activities before their pregnancies. In addition, women who are active before pregnancy may choose to modify their exercise programs somewhat; for example, weight gain or joint laxity may prompt women to walk instead of jog or to exercise indoors instead of outdoors because of improved environmental control. Because of all the physiological changes that occur during pregnancy, activity recommendations for pregnant women are subject to modifications. Finally, concerns for fetal health dictate other changes in order to optimize fetal outcomes.
Nevertheless, the benefits of regular physical activity throughout pregnancy generally outweigh the risks. Women who exercise routinely in the prenatal period have a lower incidence of babies with low birth weight. Starting with the first trimester, regular activity may help ease nausea and lessen fatigue. Body image and mood—both during pregnancy and in the postpartum period—are positively influenced by regular physical activity. Although there are not yet disorder-specific guidelines, it is felt that regular physical activity during pregnancy benefits preeclampsia, hypertension, and gestational diabetes, as mentioned earlier. It is not yet clear whether a regular physical activity program affects gestational length, quality or duration of labor, or incidence of chronic disease in the offspring.
Although the benefits of physical activity for pregnant women are significant, there are still precautions to take and health risks to keep in mind. Because of the increased metabolic rate during pregnancy, thermoregulation during exercise and the potential effect on fetal temperature are a concern. It is important for pregnant exercisers to stay well hydrated in order to improve cooling and maintain blood volume. While the benefits of chronic exercise belong to the mother, the risk of overexercise predominantly affects the fetus (Whaley 2005).
Starting with the second trimester, supine exercises are not recommended, as these can cause the uterus to compress the inferior vena cava and result in decreased cardiac output. Also, prolonged isometric exercise during weightlifting may decrease uterine perfusion. Because of the shift in the expecting mother's center of gravity, exercises that require balance should be avoided later in pregnancy; other anatomical changes of pregnancy are presented in the sidebar. Contact sports and activities that have an increased risk for falls should also be avoided. The new PAGA lists several exercises to avoid; table 6.1 includes these as well as others with risk for maternal or fetal harm. Motionless standing results in venous pooling and a significant decrease in cardiac output and thus should be avoided. In fact, one large study of 7,722 pregnancies found that mothers who had jobs requiring predominantly standing had babies with lower birth weights (Naeye and Peters 1982).
Exercise has beneficial effect on hypertension, cardiovascular disease
Currently more than 50 million Americans—and more than 50% of the American population over the age of 60—have hypertension, or high blood pressure (Hagberg 2005).
Currently more than 50 million Americans—and more than 50% of the American population over the age of 60—have hypertension, or high blood pressure (Hagberg2005). Worldwide, the number of people with hypertension is estimated to be 1 billion! Furthermore, because blood pressure tends to increase with age, the number of people with hypertension is likely to rise significantly as the U.S. population continues to age. Unfortunately, due to a lack of symptoms a large number of individuals are unaware that they have the silent killer, as hypertension is called, and do not realize their hypertension is placing them at a higher risk for a heart attack or stroke. Although hypertension affects nearly every organ, its lack of symptoms means that many individuals do not realize the damage that may be occurring even at modest elevations of blood pressure.
Physical activity is considered one of the mainstays in the nonpharmacological treatment of hypertension. This chapter discusses the current definition of hypertension and introduces the physiological relationship between exercise and blood pressure, as well as provides some background and mechanistic details. Then it presents both nationally and internationally issued activity guidelines for individuals with hypertension. Also, because of the close and causal relationship between hypertension and CAD, this chapter also includes guidelines that pertain to CAD.
Benefits of Exercise for Hypertension
The definition of hypertension has changed over time. Currently, the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7: NHBPEP 2003) defines normal blood pressure as a pressure less than 120/80 mmHg (see table 10.1). Elevated blood pressure, which at one time was diagnosed only when in excess of 160/100 mmHg, is a primary cardiac risk factor and also increases the risk for stroke, type 2 diabetes, kidney disease, and vascular disease. According to the JNC 7, the risk of CVD begins at only 115/75 mmHg and doubles with each incremental increase of 20/10 mmHg. People who are classified as prehyper-tensive have twice the risk of developing hypertension. Even individuals with normal blood pressure have a high lifetime risk of developing hypertension—an estimated 90% risk for individuals with normal blood pressure at age 55 (Vasan and others 2002)!
For people with prehypertension, exercise is one of the primary recommended lifestyle changes that can lower blood pressure to a normal level. In fact, even in individuals who have a normal blood pressure, regular aerobic exercise may lower resting blood pressure, although the extent of lowering is less than that seen in individuals with frank hypertension. In the JNC 7, physical activity compares favorably with the other recommended lifestyle changes when it comes to reducing resting blood pressure—table 10.2 gives examples of these changes and their relative effects. Also, physical activity may contribute to weight loss, which can reduce blood pressure even further.
So, although the distensibility or pliability of blood vessels decreases with age and makes hypertension more likely, hypertension is not necessarily an unavoidable consequence of aging, because regular physical activity is clearly effective in preventing hypertension and reducing its intensity. A single session of aerobic exercise creates a sustained hypotensive response that lasts up to 24 h (Hagberg and others 2000), and over time participation in regular physical activity can have long-term benefits. Postulated mechanisms for the reduction of both systolic and diastolic blood pressure that occurs with regular exercise training include the following:
- Reduced visceral fat
- Improved sodium elimination due to altered renal function
- Reduced plasma renin and catecholamine activity
- Reduced sympathetic and increased parasympathetic tone
Because physical activity decreases hypertension, it also reduces the potential contribution of hypertension to cardiovascular risk. In addition to lowering blood pressure, physical activity generally causes a regression of left ventricular hypertrophy, improves lipid profiles, and lowers the risk for type 2 diabetes. This combination of risk reduction has a substantial long-term benefit on cardiovascular risk. There are also notable benefits to other health parameters. Individuals with hypertension may not necessarily achieve normal blood pressure through exercise, but they will likely see improvements in lean body mass, glycemic control, and inflammatory biomarkers.
Overall, a regular physical activity program lowers both systolic and diastolic blood pressure. However, during aerobic exercise, the normal physiological response is a gradually rising systolic blood pressure with a stable or slightly decreasing diastolic blood pressure. In addition, during resistance training and particularly during high-intensity efforts, blood pressure may rise significantly. These natural responses to exercise necessitate guidelines for people with hypertension so that they may receive the benefits of activity safely without increasing their risk for injury or disease.
The use of antihypertensive medications also necessitates physical activity guidelines. Exercise is recommended as an adjunct to antihypertensive medication as there appears to be an additive effect of physical activity with most antihypertensive medications. Beta-blockers, however, may interfere with the antihypertensive effect of exercise (Ades and others 1988). For hypertensive individuals who regularly participate in physical activity, beta-blockers also blunt the peak heart rate and blood pressure; the former effect requires using an alternative to target heart rate for measuring exercise intensity.
Related Books









