- Home
- Athletic Training and Therapy
- Health Care in Exercise and Sport
- Medicine in Exercise and Sport
- Physical Therapy/Physiotherapy
- Sport Therapy for the Shoulder

Sport Therapy for the Shoulder
Evaluation, Rehabilitation, and Return to Sport
by Todd S. Ellenbecker and Kevin E. Wilk
Series: Sport Therapy
240 Pages
In Sport Therapy for the Shoulder: Evaluation, Rehabilitation, and Return to Sport, readers will learn about best practices and evidence-based guidelines for assessing and treating patients’ shoulder injuries for re-entry into sport. Written by renowned physical therapists Todd S. Ellenbecker and Kevin E. Wilk, this text is a key resource for physical therapists, athletic trainers, sport chiropractors, massage therapists, strength and conditioning professionals, personal trainers, and other clinicians in sports medicine who work with patients recovering from shoulder injuries.
Sport Therapy for the Shoulder guides readers systematically through functional anatomy and biomechanics of the shoulder, examination techniques and pathology, rehabilitation, and return-to-play progressions. The text provides evidence-based principles to assist clinicians in improving joint stabilization, strength, muscular endurance, and range of motion in the shoulder. Return-to-sport programs feature step-by-step progressions for sports including baseball, softball, golf, swimming, and tennis. Illustrated versions of the Thrower’s Ten and Advanced Thrower’s Ten exercise programs, which were developed by coauthor Kevin E. Wilk and colleagues, are provided in the appendix.
The content is enhanced by more than 200 color photos and detailed illustrations that provide visual support and context for conducting specific evaluation and rehabilitation techniques. Additionally, 21 online video clips are available to complement the highly visual book and demonstrate how to perform specific evaluation tests. An image bank is available free to course adopters and is also available for professionals to purchase separately for use in presentations.
The combination of foundational information, evidence-based guidelines, sport-specific return-to-sport programs, online videos, and colorful visual aids makes Sport Therapy for the Shoulder a must-have resource for clinicians who work with patients who have shoulder injuries. Not only will the book prove to be a valuable learning tool, but it will also be a reference that professionals can use continually in their practice.
Part I. Anatomy and Biomechanics of the Shoulder Complex
Chapter 1. Functional Anatomy of the Shoulder Complex
Joint Structure
Muscle Anatomy
Additional Anatomical Structures
Neurovascular Anatomy
Conclusion
Chapter 2. Mechanics of the Shoulder
Primary Biomechanical Principles
Throwing Mechanics
Tennis Serving and Swinging Mechanics
Volleyball Overheard Motions
Golf Swing Mechanics
Swimming Mechanics
Conclusion
Part II. Examination and Pathology of Shoulder Injuries
Chapter 3. Clinical Examination of the Shoulder
Subjective Evaluation (History)
Posture Evaluation
Scapular Evaluation
Evaluation of Glenohumeral Joint Range of Motion
Strength Evaluation
Functional Evaluation
Special Manual Orthopedic Shoulder Tests
Conclusion
Chapter 4. Injury Pathology of the Shoulder
Rotator Cuff Injury
Shoulder Instability
Labral Lesions and Tears
Conclusion
Part III. Rehabilitation of Shoulder Injuries
Chapter 5. Rehabilitation Progressions
Range of Motion Progression
Scapular Stabilization Methods and Progression
Rotator Cuff Exercise Progression
Conclusion
Chapter 6. Surgical Repair and Rehabilitation Protocols
Rotator Cuff Repair
Labral Repair
Conclusion
Part IV. Return to Sport
Chapter 7. Clinical Decision-Making for Return to Sport
Key Criteria for a Return to Sport Evaluation
Interval Throwing Program
Conclusion
Chapter 8. Interval Return to Sport Programs
Objective Criteria
Tennis Program
Baseball and Softball Program
Swimming Program
Golf Program
Conclusion
Todd S. Ellenbecker, DPT, MS, SCS, OCS, CSCS, is a physical therapist and clinic director for Physiotherapy Associates Scottsdale Sports Clinic in Scottsdale, Arizona, where he is also the national director of clinical research for Physiotherapy Associates. He is the vice president of medical services for the Association of Tennis Professionals (ATP) Tour and current member and past chairman of the United States Tennis Association (USTA) national sport science committee. He is also a certified United States Professional Tennis Association (USPTA) tennis teaching professional. He is a certified sports clinical specialist, orthopaedic clinical specialist, and strength and conditioning specialist.
Ellenbecker, who has more than 30 years of experience in physical therapy, has authored many books and articles in research journals and trade publications and is an international presenter on shoulder and elbow rehabilitation. He has also served on editorial boards for several journals.
Among many other honors, Ellenbecker was named the Sports Medicine Professional of the Year (2003) by the National Strength and Conditional Association and received the Ronald G. Peyton Lecture Award (2007) by the Sports Physical Therapy Section and the Samuel Hardy Educational Merit Award (2008) by the International Tennis Hall of Fame.
Kevin E. Wilk, PT, DPT, FAPTA, is the associate clinical director for Champion Sports Medicine in Birmingham, Alabama, as well as vice president of clinical education for Physiotherapy Associates. He is also the director of rehabilitative research at the American Sports Medicine Institute in Birmingham while also serving as the rehabilitation consultant for Major League Baseball’s Tampa Bay Devil Rays.
Wilk, who has been a physical therapist, researcher, and educator for more than 30 years, has also published many books and articles and book chapters in various medical journals and industry publications. He is an adjunct assistant professor in the physical therapy program at Marquette University and has presented his work and research worldwide.
Wilk received the Catherine Worthingham Fellowship in 2012 by the American Physical Therapy Association, the Turner A. Blackburn Hall of Fame Lifetime Achievement Award in 2012 by the Sports Physical Therapy Section (SPTS), the Ronald G. Peyton Lecture Award in 2004 by SPTS, and the James R. Andrews, MD, Award for Excellence in Baseball Sports Medicine in 1999 by the American Sports Medicine Institute.
What is happening in the shoulder complex during a golf swing?
Similar to the situation with the other sports reviewed in this chapter, to isolate and identify the functions of the major muscles controlling the various body segments during the golf swing, dynamic EMG and high-speed motion analysis has been used and helps to provide a greater understanding of the demands of golf on the shoulder complex.
Golf Swing Mechanics
Similar to the situation with the other sports reviewed in this chapter, to isolate and identify the functions of the major muscles controlling the various body segments during the golf swing, dynamic EMG and high-speed motion analysis has been used and helps to provide a greater understanding of the demands of golf on the shoulder complex. For discussion and analysis purposes, the golf swing has been broken down into the following five phases (Pink et al. 1993):
- Take-away: from address to the ball to the end of the backswing
- Forward swing: from the end of the backswing until the club is horizontal
- Acceleration: from horizontal position of the club to ball contact
- Early follow-through: from ball contact to horizontal club position
- Late follow-through: from horizontal club position to the end of the swing
 |
|
|
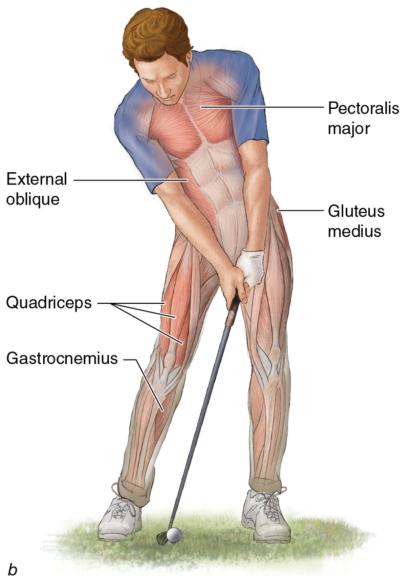
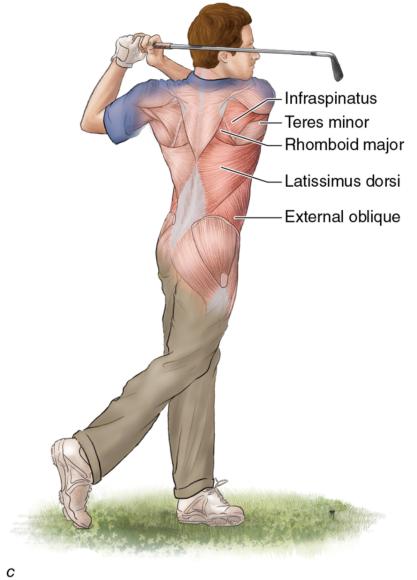
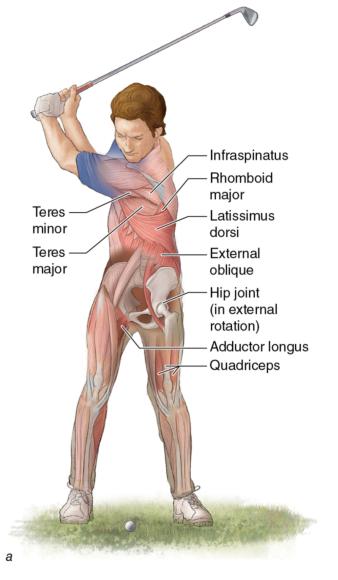
Muscles used in three of the five phases of the golf swing: (a) take-away, (b) acceleration, and (c) follow-through.
This section describes and compares the muscle activity patterns of the primary shoulder and scapular muscles (but note that there are also significant contributions from other body segments during a golf swing).
Take-Away
Before initiation of the backswing, proper setup and ball address must be achieved. This initial posture greatly influences the balance of forces throughout the golf swing and is therefore critical to the achievement of the proper swing plane. The take-away phase has been described as a "coiling" or "loading" of the body in order to enhance the velocity and kinetic energy of the club head (Pink et al. 1990). Electromyographic analysis reveals relatively low activity of the trunk musculature during this segment of the golf swing, as the trunk is simply preparing for the swing (Pink et al. 1990). Electromyographic analysis of the scapular muscles of the trailing arm reveals relatively high activity of the upper, middle, and lower portions of the trapezius during take-away in order to help the scapula retract and upwardly rotate (Kao et al. 1995). Similarly, the levator scapulae and rhomboid muscle of the trailing arm are active during this period to help with such scapular movements (Kao et al. 1995). In the leading arm during take-away, the activity of the scapular stabilizing muscles is relatively low to allow for scapular protraction.
Electromyographic analysis of the rotator cuff muscles exhibits contributions from the supraspinatus and infraspinatus in the trailing arm as they act to approximate and stabilize the shoulder (Jobe et al. 1986, Pink et al. 1990). Of the rotator cuff muscles in the leading arm, only the subscapularis was shown to display marked activity during the take-away phase. It should be noted that the pectoralis major, latissimus dorsi, and the deltoid muscles of both arms are relatively inactive in the backswing of the golf club (Jobe et al. 1986, Pink et al. 1990).
Forward Swing
During forward swing, trunk rotation movement is initiated. Analysis of the trailing arm scapular muscles shows that the three portions of the trapezius have lower activation to allow for scapular protraction (Kao et al. 1995). However, the levator scapulae and rhomboid muscles display marked activity to control scapular protraction and rotation of the trailing arm. Analysis of the serratus anterior muscle in the trailing arm shows increased activity during forward swing to aid in scapular protraction and stabilization (Kao et al. 1995). Electromyographic studies of the lead arm demonstrate high activity of the trapezius, levator scapulae, rhomboids, and serratus anterior as they all contribute to scapular motion and stabilization as the arms move toward the ball (Kao et al. 1995).
Of the trailing shoulder muscles during forward swing, the subscapularis, pectoralis major, and latissimus begin firing at marked levels as the trailing arm increasingly accelerates into the internal rotation and adduction. The lead arm subscapularis and latissimus dorsi are both moderately active during the forward swing phase.
Acceleration
During the acceleration phase, the body segments work together in a coordinated sequence in order to maximize club head speed at ball impact. The serratus anterior is the primary scapular stabilizer that is active in the trailing arm during acceleration (Kao et al. 1995). The serratus has high levels of involvement in order to allow for a strong scapular protraction and contribute to maximizing club head speed. Conversely, EMG analysis reveals strong contractions of the scapular muscles in the lead arm during acceleration (Kao et al. 1995). The trapezius, levator scapulae, and rhomboid muscles are firing to aid in scapular retraction, upward rotation, and elevation. The serratus anterior of the lead arm continues to display high levels of activation throughout. This important muscle is highly involved during the golf swing, similarly to what is seen during throwing and the tennis serve as discussed in earlier sections of this chapter.
Electromyographic investigations display high levels of subscapularis, pectoralis major, and latissimus dorsi activity to provide power to the trailing arm during acceleration (Jobe et al. 1986). These important muscles further increase in activity from forward swing to assist in rotation and forceful adduction of the arm during this phase. The latissimus dorsi contributes most of its power in the forward swing, while the pectoralis major supplies the most power during acceleration (Pink et al. 1990). Similarly, the subscapularis, pectoralis major, and latissimus dorsi of the lead arm fire at high rates during the acceleration phase (Jobe et al. 1986, Pink et al. 1990).
Early Follow-Through
After ball contact has been made, the follow-through phase is initiated. During early follow-through, nearly all the body segments work to decelerate their rotational contributions, often through eccentric muscle contractions (Jobe et al. 1986, Pink et al. 1993). The scapular muscles of both the trailing and lead arms display decreased activity throughout the follow-through phases, allowing for coordinated scapular protraction (Kao et al. 1995). Despite this decrease in scapular activity, the serratus anterior muscles of both arms show fairly consistent muscle firing patterns providing vital scapular stabilization throughout the follow-through phases (Kao et al. 1995).
In the trailing shoulder, marked activity of the subscapularis, pectoralis major, and latissimus dorsi muscles continues into the early follow-through phase (Jobe et al. 1986). For the lead shoulder, the subscapularis continues its high level of activity, while the pectoralis major and latissimus dorsi decrease their contributions (Jobe et al. 1986, Pink et al. 1990).
Late Follow-Through
Activity of the scapular muscles of both arms decreases to lower levels as the swing comes to an end (Kao et al. 1995). The subscapularis of the trailing shoulder is one of the only muscles that remains highly active during this phase (Jobe et al. 1986, Pink et al. 1990). Analysis of the lead arm reveals marked activity of the infraspinatus and the supraspinatus rotator cuff muscles used for glenohumeral stabilization (Pink et al. 1990).
One final discussion regarding the golf swing concerns a common mechanical fault that many golfers have, placing their glenohumeral joints at risk. During take-away, the lead arm is placed into increasing degrees of internal rotation and cross-body adduction. This position may predispose the golfer to impingement-type problems as the rotator cuff tendons and bursae are compressed within the shoulder (Mallon 1996). Additionally, at the end of the backswing, forces on the acromioclavicular joint of the lead arm are shown to be high, contributing to the incidence of pain often seen in the golfer's shoulder. The posterior rotator cuff and scapular muscles of the lead arm are also at risk for injury at the TOB as they are placed under a stretch load to achieve that position (Mallon 1996).
Save
Save
Save
Save
Learn more about Sport Therapy for the Shoulder.
Improve shoulder internal rotation range of motion for throwing athletes
Now that interpretation of glenohumeral joint ROM has been discussed, this section outlines specific techniques to increase IR ROM in the patient with shoulder dysfunction.
Methods to Improve Shoulder Internal Rotation (IR) Range of Motion (ROM) in the Throwing Athlete
Now that interpretation of glenohumeral joint ROM has been discussed, this section outlines specific techniques to increase IR ROM in the patient with shoulder dysfunction. This section, addressing the importance of accurate ROM measurement and clinical decision making based on the latest scientific evidence, can guide the clinician through the rehabilitation process; one can encounter a large spectrum of mobility issues when treating the patient with glenohumeral impingement. To further illustrate the role of ROM and passive stretching during this phase of the rehabilitation, figures 5.4 and 5.5 show versions of clinical IR stretching positions that use the scapular plane and that can be performed in multiple and varied positions of glenohumeral abduction. Each inherently possesses an anterior hand placement, used to exert varying degrees of posterior pressure to minimize scapular compensation and also to provide a checkrein against anterior humeral head translation during the IR stretch because of the effects of obligate translation.

Internal rotation range of motion technique in the scapular plane with 30° of elevation with scapular stabilization.

Internal rotation range of motion technique with scapular stabilization and 45° of glenohumeral joint elevation in the scapular plane. Note that the amount of elevation used with this stretch can be varied from as little as 0⁰ to 10⁰ all the way to 90⁰.
Research by Izumi and colleagues (2008) showed that large strains occurred in the posterior capsule in a stretching position of 30⁰ of elevation in the scapular plane with IR. These researchers compared many positions of shoulder ROM to determine what position optimally placed stress on the posterior capsule. The internally rotated position with the shoulder elevated 30⁰ in the scapular plane produced very acceptable levels of posterior capsular strain and would be highly effective for clinical use. These stretches for the posterior capsule and muscle - tendon unit (posterior shoulder stretches) can be used in a proprioceptive neuromuscular facilitation (PNF) contract - relax format following a low-load prolonged stretch-type paradigm to facilitate the increase in ROM (Sullivan et al. 1982, Zachezewski & Reischl 1986).
Save
Save
Save
Save
Save
Find more stretches to address IR ROM in Sport Therapy for the Shoulder.
Baseball and softball (throwing) program
The interval sport return program for baseball and softball (throwing) is designed to gradually return motion and strength to (and confidence in) the throwing arm after injury or surgery by slowly progressing through graduated throwing distances.
The interval sport return program for baseball and softball (throwing) is designed to gradually return motion and strength to (and confidence in) the throwing arm after injury or surgery by slowly progressing through graduated throwing distances. The program begins upon clearance by the athlete's physician to resume throwing and is performed under the supervision of the rehabilitation team (physician, physical therapist, and athletic trainer). The program is set up to minimize the chance of reinjury and emphasize prethrowing warm-up and stretching. In development of the interval throwing program (ITP), the following factors are considered most important:
- The act of throwing the baseball involves the transfer of energy from the feet through the legs, pelvis, and trunk and out the shoulder through the elbow and hand. Therefore, any return to throwing after injury must include attention to the entire body.
- The chance for reinjury is lessened by a graduated progression of interval throwing.
- Proper warm-up is essential.
- Most injuries occur as the result of fatigue.
- Proper throwing mechanics lessen the incidence of reinjury.
- Baseline requirements for throwing include these:
- Pain-free ROM
- Adequate muscle power
- Adequate muscle resistance to fatigue
Because of individual variability among throwing athletes, there is no set timetable for completion of the program. Most athletes, by nature, are highly competitive individuals and wish to return to competition at the earliest possible moment. While this is a necessary quality in all athletes, the proper channeling of the athlete's energies into a strictly controlled throwing program is essential to lessen the chance of reinjury during the rehabilitation process. The athlete may tend to want to increase the intensity of the throwing program. This will increase the incidence of reinjury and may greatly retard the rehabilitation process. The recommendation is to follow the program exactly, as this is the safest route to return to competition.
During the recovery process the athlete will probably experience soreness and a dull, diffuse aching sensation in the muscles and tendons. If the athlete experiences sharp pain, particularly in the joint, all throwing activity should be stopped until this pain ceases. If the pain continues, he should contact his physician.
Weight Training
The athlete should supplement the ITP with a high-repetition, low-weight exercise program. Strengthening should address a good balance between anterior and posterior musculature so that the shoulder will not be predisposed to injury. Special emphasis must be given to posterior rotator cuff musculature for any strengthening program. Weight training does not increase throwing velocity, but it increases the resistance of the arm to fatigue and injury. The athlete should do weight training on the same day as throwing but after the throwing has been completed; the day in between should be used for flexibility exercises and a recovery period. A weight training pattern or routine should be stressed at this point as a "maintenance program." This pattern can and should accompany the athlete into and throughout the season as a deterrent to further injury. It must be emphasized that weight training is of no benefit unless accompanied by a sound flexibility program.
Individual Variability
The ITP is designed so that each level is achieved without pain or complications before the next level is initiated. This sets up a progression in which the athlete achieves a goal before advancing, rather than advancing according to a specific time frame. Because of this design, the ITP may be used for different levels of skills and abilities compared to those characteristic of high school to professional levels. Progression will vary from person to person throughout the ITP. As an example, one athlete may wish to use alternate days throwing with or without using weights in between; another athlete may have to throw every third or fourth day due to pain or swelling. The athlete should be reminded to listen to her body, since pain signifies when it may be necessary to slow down. Again, completion of the steps of the ITP will vary from person to person. There is no set timetable with regard to days to completion.
Unlock the full program with Sport Therapy for the Shoulder.
What is happening in the shoulder complex during a golf swing?
Similar to the situation with the other sports reviewed in this chapter, to isolate and identify the functions of the major muscles controlling the various body segments during the golf swing, dynamic EMG and high-speed motion analysis has been used and helps to provide a greater understanding of the demands of golf on the shoulder complex.
Golf Swing Mechanics
Similar to the situation with the other sports reviewed in this chapter, to isolate and identify the functions of the major muscles controlling the various body segments during the golf swing, dynamic EMG and high-speed motion analysis has been used and helps to provide a greater understanding of the demands of golf on the shoulder complex. For discussion and analysis purposes, the golf swing has been broken down into the following five phases (Pink et al. 1993):
- Take-away: from address to the ball to the end of the backswing
- Forward swing: from the end of the backswing until the club is horizontal
- Acceleration: from horizontal position of the club to ball contact
- Early follow-through: from ball contact to horizontal club position
- Late follow-through: from horizontal club position to the end of the swing
|
|
|
Muscles used in three of the five phases of the golf swing: (a) take-away, (b) acceleration, and (c) follow-through.
This section describes and compares the muscle activity patterns of the primary shoulder and scapular muscles (but note that there are also significant contributions from other body segments during a golf swing).
Take-Away
Before initiation of the backswing, proper setup and ball address must be achieved. This initial posture greatly influences the balance of forces throughout the golf swing and is therefore critical to the achievement of the proper swing plane. The take-away phase has been described as a "coiling" or "loading" of the body in order to enhance the velocity and kinetic energy of the club head (Pink et al. 1990). Electromyographic analysis reveals relatively low activity of the trunk musculature during this segment of the golf swing, as the trunk is simply preparing for the swing (Pink et al. 1990). Electromyographic analysis of the scapular muscles of the trailing arm reveals relatively high activity of the upper, middle, and lower portions of the trapezius during take-away in order to help the scapula retract and upwardly rotate (Kao et al. 1995). Similarly, the levator scapulae and rhomboid muscle of the trailing arm are active during this period to help with such scapular movements (Kao et al. 1995). In the leading arm during take-away, the activity of the scapular stabilizing muscles is relatively low to allow for scapular protraction.
Electromyographic analysis of the rotator cuff muscles exhibits contributions from the supraspinatus and infraspinatus in the trailing arm as they act to approximate and stabilize the shoulder (Jobe et al. 1986, Pink et al. 1990). Of the rotator cuff muscles in the leading arm, only the subscapularis was shown to display marked activity during the take-away phase. It should be noted that the pectoralis major, latissimus dorsi, and the deltoid muscles of both arms are relatively inactive in the backswing of the golf club (Jobe et al. 1986, Pink et al. 1990).
Forward Swing
During forward swing, trunk rotation movement is initiated. Analysis of the trailing arm scapular muscles shows that the three portions of the trapezius have lower activation to allow for scapular protraction (Kao et al. 1995). However, the levator scapulae and rhomboid muscles display marked activity to control scapular protraction and rotation of the trailing arm. Analysis of the serratus anterior muscle in the trailing arm shows increased activity during forward swing to aid in scapular protraction and stabilization (Kao et al. 1995). Electromyographic studies of the lead arm demonstrate high activity of the trapezius, levator scapulae, rhomboids, and serratus anterior as they all contribute to scapular motion and stabilization as the arms move toward the ball (Kao et al. 1995).
Of the trailing shoulder muscles during forward swing, the subscapularis, pectoralis major, and latissimus begin firing at marked levels as the trailing arm increasingly accelerates into the internal rotation and adduction. The lead arm subscapularis and latissimus dorsi are both moderately active during the forward swing phase.
Acceleration
During the acceleration phase, the body segments work together in a coordinated sequence in order to maximize club head speed at ball impact. The serratus anterior is the primary scapular stabilizer that is active in the trailing arm during acceleration (Kao et al. 1995). The serratus has high levels of involvement in order to allow for a strong scapular protraction and contribute to maximizing club head speed. Conversely, EMG analysis reveals strong contractions of the scapular muscles in the lead arm during acceleration (Kao et al. 1995). The trapezius, levator scapulae, and rhomboid muscles are firing to aid in scapular retraction, upward rotation, and elevation. The serratus anterior of the lead arm continues to display high levels of activation throughout. This important muscle is highly involved during the golf swing, similarly to what is seen during throwing and the tennis serve as discussed in earlier sections of this chapter.
Electromyographic investigations display high levels of subscapularis, pectoralis major, and latissimus dorsi activity to provide power to the trailing arm during acceleration (Jobe et al. 1986). These important muscles further increase in activity from forward swing to assist in rotation and forceful adduction of the arm during this phase. The latissimus dorsi contributes most of its power in the forward swing, while the pectoralis major supplies the most power during acceleration (Pink et al. 1990). Similarly, the subscapularis, pectoralis major, and latissimus dorsi of the lead arm fire at high rates during the acceleration phase (Jobe et al. 1986, Pink et al. 1990).
Early Follow-Through
After ball contact has been made, the follow-through phase is initiated. During early follow-through, nearly all the body segments work to decelerate their rotational contributions, often through eccentric muscle contractions (Jobe et al. 1986, Pink et al. 1993). The scapular muscles of both the trailing and lead arms display decreased activity throughout the follow-through phases, allowing for coordinated scapular protraction (Kao et al. 1995). Despite this decrease in scapular activity, the serratus anterior muscles of both arms show fairly consistent muscle firing patterns providing vital scapular stabilization throughout the follow-through phases (Kao et al. 1995).
In the trailing shoulder, marked activity of the subscapularis, pectoralis major, and latissimus dorsi muscles continues into the early follow-through phase (Jobe et al. 1986). For the lead shoulder, the subscapularis continues its high level of activity, while the pectoralis major and latissimus dorsi decrease their contributions (Jobe et al. 1986, Pink et al. 1990).
Late Follow-Through
Activity of the scapular muscles of both arms decreases to lower levels as the swing comes to an end (Kao et al. 1995). The subscapularis of the trailing shoulder is one of the only muscles that remains highly active during this phase (Jobe et al. 1986, Pink et al. 1990). Analysis of the lead arm reveals marked activity of the infraspinatus and the supraspinatus rotator cuff muscles used for glenohumeral stabilization (Pink et al. 1990).
One final discussion regarding the golf swing concerns a common mechanical fault that many golfers have, placing their glenohumeral joints at risk. During take-away, the lead arm is placed into increasing degrees of internal rotation and cross-body adduction. This position may predispose the golfer to impingement-type problems as the rotator cuff tendons and bursae are compressed within the shoulder (Mallon 1996). Additionally, at the end of the backswing, forces on the acromioclavicular joint of the lead arm are shown to be high, contributing to the incidence of pain often seen in the golfer's shoulder. The posterior rotator cuff and scapular muscles of the lead arm are also at risk for injury at the TOB as they are placed under a stretch load to achieve that position (Mallon 1996).
Save
Save
Save
Save
Learn more about Sport Therapy for the Shoulder.
Improve shoulder internal rotation range of motion for throwing athletes
Now that interpretation of glenohumeral joint ROM has been discussed, this section outlines specific techniques to increase IR ROM in the patient with shoulder dysfunction.
Methods to Improve Shoulder Internal Rotation (IR) Range of Motion (ROM) in the Throwing Athlete
Now that interpretation of glenohumeral joint ROM has been discussed, this section outlines specific techniques to increase IR ROM in the patient with shoulder dysfunction. This section, addressing the importance of accurate ROM measurement and clinical decision making based on the latest scientific evidence, can guide the clinician through the rehabilitation process; one can encounter a large spectrum of mobility issues when treating the patient with glenohumeral impingement. To further illustrate the role of ROM and passive stretching during this phase of the rehabilitation, figures 5.4 and 5.5 show versions of clinical IR stretching positions that use the scapular plane and that can be performed in multiple and varied positions of glenohumeral abduction. Each inherently possesses an anterior hand placement, used to exert varying degrees of posterior pressure to minimize scapular compensation and also to provide a checkrein against anterior humeral head translation during the IR stretch because of the effects of obligate translation.
Internal rotation range of motion technique in the scapular plane with 30° of elevation with scapular stabilization.
Internal rotation range of motion technique with scapular stabilization and 45° of glenohumeral joint elevation in the scapular plane. Note that the amount of elevation used with this stretch can be varied from as little as 0⁰ to 10⁰ all the way to 90⁰.
Research by Izumi and colleagues (2008) showed that large strains occurred in the posterior capsule in a stretching position of 30⁰ of elevation in the scapular plane with IR. These researchers compared many positions of shoulder ROM to determine what position optimally placed stress on the posterior capsule. The internally rotated position with the shoulder elevated 30⁰ in the scapular plane produced very acceptable levels of posterior capsular strain and would be highly effective for clinical use. These stretches for the posterior capsule and muscle - tendon unit (posterior shoulder stretches) can be used in a proprioceptive neuromuscular facilitation (PNF) contract - relax format following a low-load prolonged stretch-type paradigm to facilitate the increase in ROM (Sullivan et al. 1982, Zachezewski & Reischl 1986).
Save
Save
Save
Save
Save
Find more stretches to address IR ROM in Sport Therapy for the Shoulder.
Baseball and softball (throwing) program
The interval sport return program for baseball and softball (throwing) is designed to gradually return motion and strength to (and confidence in) the throwing arm after injury or surgery by slowly progressing through graduated throwing distances.
The interval sport return program for baseball and softball (throwing) is designed to gradually return motion and strength to (and confidence in) the throwing arm after injury or surgery by slowly progressing through graduated throwing distances. The program begins upon clearance by the athlete's physician to resume throwing and is performed under the supervision of the rehabilitation team (physician, physical therapist, and athletic trainer). The program is set up to minimize the chance of reinjury and emphasize prethrowing warm-up and stretching. In development of the interval throwing program (ITP), the following factors are considered most important:
- The act of throwing the baseball involves the transfer of energy from the feet through the legs, pelvis, and trunk and out the shoulder through the elbow and hand. Therefore, any return to throwing after injury must include attention to the entire body.
- The chance for reinjury is lessened by a graduated progression of interval throwing.
- Proper warm-up is essential.
- Most injuries occur as the result of fatigue.
- Proper throwing mechanics lessen the incidence of reinjury.
- Baseline requirements for throwing include these:
- Pain-free ROM
- Adequate muscle power
- Adequate muscle resistance to fatigue
Because of individual variability among throwing athletes, there is no set timetable for completion of the program. Most athletes, by nature, are highly competitive individuals and wish to return to competition at the earliest possible moment. While this is a necessary quality in all athletes, the proper channeling of the athlete's energies into a strictly controlled throwing program is essential to lessen the chance of reinjury during the rehabilitation process. The athlete may tend to want to increase the intensity of the throwing program. This will increase the incidence of reinjury and may greatly retard the rehabilitation process. The recommendation is to follow the program exactly, as this is the safest route to return to competition.
During the recovery process the athlete will probably experience soreness and a dull, diffuse aching sensation in the muscles and tendons. If the athlete experiences sharp pain, particularly in the joint, all throwing activity should be stopped until this pain ceases. If the pain continues, he should contact his physician.
Weight Training
The athlete should supplement the ITP with a high-repetition, low-weight exercise program. Strengthening should address a good balance between anterior and posterior musculature so that the shoulder will not be predisposed to injury. Special emphasis must be given to posterior rotator cuff musculature for any strengthening program. Weight training does not increase throwing velocity, but it increases the resistance of the arm to fatigue and injury. The athlete should do weight training on the same day as throwing but after the throwing has been completed; the day in between should be used for flexibility exercises and a recovery period. A weight training pattern or routine should be stressed at this point as a "maintenance program." This pattern can and should accompany the athlete into and throughout the season as a deterrent to further injury. It must be emphasized that weight training is of no benefit unless accompanied by a sound flexibility program.
Individual Variability
The ITP is designed so that each level is achieved without pain or complications before the next level is initiated. This sets up a progression in which the athlete achieves a goal before advancing, rather than advancing according to a specific time frame. Because of this design, the ITP may be used for different levels of skills and abilities compared to those characteristic of high school to professional levels. Progression will vary from person to person throughout the ITP. As an example, one athlete may wish to use alternate days throwing with or without using weights in between; another athlete may have to throw every third or fourth day due to pain or swelling. The athlete should be reminded to listen to her body, since pain signifies when it may be necessary to slow down. Again, completion of the steps of the ITP will vary from person to person. There is no set timetable with regard to days to completion.
Unlock the full program with Sport Therapy for the Shoulder.
What is happening in the shoulder complex during a golf swing?
Similar to the situation with the other sports reviewed in this chapter, to isolate and identify the functions of the major muscles controlling the various body segments during the golf swing, dynamic EMG and high-speed motion analysis has been used and helps to provide a greater understanding of the demands of golf on the shoulder complex.
Golf Swing Mechanics
Similar to the situation with the other sports reviewed in this chapter, to isolate and identify the functions of the major muscles controlling the various body segments during the golf swing, dynamic EMG and high-speed motion analysis has been used and helps to provide a greater understanding of the demands of golf on the shoulder complex. For discussion and analysis purposes, the golf swing has been broken down into the following five phases (Pink et al. 1993):
- Take-away: from address to the ball to the end of the backswing
- Forward swing: from the end of the backswing until the club is horizontal
- Acceleration: from horizontal position of the club to ball contact
- Early follow-through: from ball contact to horizontal club position
- Late follow-through: from horizontal club position to the end of the swing
|
|
|
Muscles used in three of the five phases of the golf swing: (a) take-away, (b) acceleration, and (c) follow-through.
This section describes and compares the muscle activity patterns of the primary shoulder and scapular muscles (but note that there are also significant contributions from other body segments during a golf swing).
Take-Away
Before initiation of the backswing, proper setup and ball address must be achieved. This initial posture greatly influences the balance of forces throughout the golf swing and is therefore critical to the achievement of the proper swing plane. The take-away phase has been described as a "coiling" or "loading" of the body in order to enhance the velocity and kinetic energy of the club head (Pink et al. 1990). Electromyographic analysis reveals relatively low activity of the trunk musculature during this segment of the golf swing, as the trunk is simply preparing for the swing (Pink et al. 1990). Electromyographic analysis of the scapular muscles of the trailing arm reveals relatively high activity of the upper, middle, and lower portions of the trapezius during take-away in order to help the scapula retract and upwardly rotate (Kao et al. 1995). Similarly, the levator scapulae and rhomboid muscle of the trailing arm are active during this period to help with such scapular movements (Kao et al. 1995). In the leading arm during take-away, the activity of the scapular stabilizing muscles is relatively low to allow for scapular protraction.
Electromyographic analysis of the rotator cuff muscles exhibits contributions from the supraspinatus and infraspinatus in the trailing arm as they act to approximate and stabilize the shoulder (Jobe et al. 1986, Pink et al. 1990). Of the rotator cuff muscles in the leading arm, only the subscapularis was shown to display marked activity during the take-away phase. It should be noted that the pectoralis major, latissimus dorsi, and the deltoid muscles of both arms are relatively inactive in the backswing of the golf club (Jobe et al. 1986, Pink et al. 1990).
Forward Swing
During forward swing, trunk rotation movement is initiated. Analysis of the trailing arm scapular muscles shows that the three portions of the trapezius have lower activation to allow for scapular protraction (Kao et al. 1995). However, the levator scapulae and rhomboid muscles display marked activity to control scapular protraction and rotation of the trailing arm. Analysis of the serratus anterior muscle in the trailing arm shows increased activity during forward swing to aid in scapular protraction and stabilization (Kao et al. 1995). Electromyographic studies of the lead arm demonstrate high activity of the trapezius, levator scapulae, rhomboids, and serratus anterior as they all contribute to scapular motion and stabilization as the arms move toward the ball (Kao et al. 1995).
Of the trailing shoulder muscles during forward swing, the subscapularis, pectoralis major, and latissimus begin firing at marked levels as the trailing arm increasingly accelerates into the internal rotation and adduction. The lead arm subscapularis and latissimus dorsi are both moderately active during the forward swing phase.
Acceleration
During the acceleration phase, the body segments work together in a coordinated sequence in order to maximize club head speed at ball impact. The serratus anterior is the primary scapular stabilizer that is active in the trailing arm during acceleration (Kao et al. 1995). The serratus has high levels of involvement in order to allow for a strong scapular protraction and contribute to maximizing club head speed. Conversely, EMG analysis reveals strong contractions of the scapular muscles in the lead arm during acceleration (Kao et al. 1995). The trapezius, levator scapulae, and rhomboid muscles are firing to aid in scapular retraction, upward rotation, and elevation. The serratus anterior of the lead arm continues to display high levels of activation throughout. This important muscle is highly involved during the golf swing, similarly to what is seen during throwing and the tennis serve as discussed in earlier sections of this chapter.
Electromyographic investigations display high levels of subscapularis, pectoralis major, and latissimus dorsi activity to provide power to the trailing arm during acceleration (Jobe et al. 1986). These important muscles further increase in activity from forward swing to assist in rotation and forceful adduction of the arm during this phase. The latissimus dorsi contributes most of its power in the forward swing, while the pectoralis major supplies the most power during acceleration (Pink et al. 1990). Similarly, the subscapularis, pectoralis major, and latissimus dorsi of the lead arm fire at high rates during the acceleration phase (Jobe et al. 1986, Pink et al. 1990).
Early Follow-Through
After ball contact has been made, the follow-through phase is initiated. During early follow-through, nearly all the body segments work to decelerate their rotational contributions, often through eccentric muscle contractions (Jobe et al. 1986, Pink et al. 1993). The scapular muscles of both the trailing and lead arms display decreased activity throughout the follow-through phases, allowing for coordinated scapular protraction (Kao et al. 1995). Despite this decrease in scapular activity, the serratus anterior muscles of both arms show fairly consistent muscle firing patterns providing vital scapular stabilization throughout the follow-through phases (Kao et al. 1995).
In the trailing shoulder, marked activity of the subscapularis, pectoralis major, and latissimus dorsi muscles continues into the early follow-through phase (Jobe et al. 1986). For the lead shoulder, the subscapularis continues its high level of activity, while the pectoralis major and latissimus dorsi decrease their contributions (Jobe et al. 1986, Pink et al. 1990).
Late Follow-Through
Activity of the scapular muscles of both arms decreases to lower levels as the swing comes to an end (Kao et al. 1995). The subscapularis of the trailing shoulder is one of the only muscles that remains highly active during this phase (Jobe et al. 1986, Pink et al. 1990). Analysis of the lead arm reveals marked activity of the infraspinatus and the supraspinatus rotator cuff muscles used for glenohumeral stabilization (Pink et al. 1990).
One final discussion regarding the golf swing concerns a common mechanical fault that many golfers have, placing their glenohumeral joints at risk. During take-away, the lead arm is placed into increasing degrees of internal rotation and cross-body adduction. This position may predispose the golfer to impingement-type problems as the rotator cuff tendons and bursae are compressed within the shoulder (Mallon 1996). Additionally, at the end of the backswing, forces on the acromioclavicular joint of the lead arm are shown to be high, contributing to the incidence of pain often seen in the golfer's shoulder. The posterior rotator cuff and scapular muscles of the lead arm are also at risk for injury at the TOB as they are placed under a stretch load to achieve that position (Mallon 1996).
Save
Save
Save
Save
Learn more about Sport Therapy for the Shoulder.
Improve shoulder internal rotation range of motion for throwing athletes
Now that interpretation of glenohumeral joint ROM has been discussed, this section outlines specific techniques to increase IR ROM in the patient with shoulder dysfunction.
Methods to Improve Shoulder Internal Rotation (IR) Range of Motion (ROM) in the Throwing Athlete
Now that interpretation of glenohumeral joint ROM has been discussed, this section outlines specific techniques to increase IR ROM in the patient with shoulder dysfunction. This section, addressing the importance of accurate ROM measurement and clinical decision making based on the latest scientific evidence, can guide the clinician through the rehabilitation process; one can encounter a large spectrum of mobility issues when treating the patient with glenohumeral impingement. To further illustrate the role of ROM and passive stretching during this phase of the rehabilitation, figures 5.4 and 5.5 show versions of clinical IR stretching positions that use the scapular plane and that can be performed in multiple and varied positions of glenohumeral abduction. Each inherently possesses an anterior hand placement, used to exert varying degrees of posterior pressure to minimize scapular compensation and also to provide a checkrein against anterior humeral head translation during the IR stretch because of the effects of obligate translation.
Internal rotation range of motion technique in the scapular plane with 30° of elevation with scapular stabilization.
Internal rotation range of motion technique with scapular stabilization and 45° of glenohumeral joint elevation in the scapular plane. Note that the amount of elevation used with this stretch can be varied from as little as 0⁰ to 10⁰ all the way to 90⁰.
Research by Izumi and colleagues (2008) showed that large strains occurred in the posterior capsule in a stretching position of 30⁰ of elevation in the scapular plane with IR. These researchers compared many positions of shoulder ROM to determine what position optimally placed stress on the posterior capsule. The internally rotated position with the shoulder elevated 30⁰ in the scapular plane produced very acceptable levels of posterior capsular strain and would be highly effective for clinical use. These stretches for the posterior capsule and muscle - tendon unit (posterior shoulder stretches) can be used in a proprioceptive neuromuscular facilitation (PNF) contract - relax format following a low-load prolonged stretch-type paradigm to facilitate the increase in ROM (Sullivan et al. 1982, Zachezewski & Reischl 1986).
Save
Save
Save
Save
Save
Find more stretches to address IR ROM in Sport Therapy for the Shoulder.
Baseball and softball (throwing) program
The interval sport return program for baseball and softball (throwing) is designed to gradually return motion and strength to (and confidence in) the throwing arm after injury or surgery by slowly progressing through graduated throwing distances.
The interval sport return program for baseball and softball (throwing) is designed to gradually return motion and strength to (and confidence in) the throwing arm after injury or surgery by slowly progressing through graduated throwing distances. The program begins upon clearance by the athlete's physician to resume throwing and is performed under the supervision of the rehabilitation team (physician, physical therapist, and athletic trainer). The program is set up to minimize the chance of reinjury and emphasize prethrowing warm-up and stretching. In development of the interval throwing program (ITP), the following factors are considered most important:
- The act of throwing the baseball involves the transfer of energy from the feet through the legs, pelvis, and trunk and out the shoulder through the elbow and hand. Therefore, any return to throwing after injury must include attention to the entire body.
- The chance for reinjury is lessened by a graduated progression of interval throwing.
- Proper warm-up is essential.
- Most injuries occur as the result of fatigue.
- Proper throwing mechanics lessen the incidence of reinjury.
- Baseline requirements for throwing include these:
- Pain-free ROM
- Adequate muscle power
- Adequate muscle resistance to fatigue
Because of individual variability among throwing athletes, there is no set timetable for completion of the program. Most athletes, by nature, are highly competitive individuals and wish to return to competition at the earliest possible moment. While this is a necessary quality in all athletes, the proper channeling of the athlete's energies into a strictly controlled throwing program is essential to lessen the chance of reinjury during the rehabilitation process. The athlete may tend to want to increase the intensity of the throwing program. This will increase the incidence of reinjury and may greatly retard the rehabilitation process. The recommendation is to follow the program exactly, as this is the safest route to return to competition.
During the recovery process the athlete will probably experience soreness and a dull, diffuse aching sensation in the muscles and tendons. If the athlete experiences sharp pain, particularly in the joint, all throwing activity should be stopped until this pain ceases. If the pain continues, he should contact his physician.
Weight Training
The athlete should supplement the ITP with a high-repetition, low-weight exercise program. Strengthening should address a good balance between anterior and posterior musculature so that the shoulder will not be predisposed to injury. Special emphasis must be given to posterior rotator cuff musculature for any strengthening program. Weight training does not increase throwing velocity, but it increases the resistance of the arm to fatigue and injury. The athlete should do weight training on the same day as throwing but after the throwing has been completed; the day in between should be used for flexibility exercises and a recovery period. A weight training pattern or routine should be stressed at this point as a "maintenance program." This pattern can and should accompany the athlete into and throughout the season as a deterrent to further injury. It must be emphasized that weight training is of no benefit unless accompanied by a sound flexibility program.
Individual Variability
The ITP is designed so that each level is achieved without pain or complications before the next level is initiated. This sets up a progression in which the athlete achieves a goal before advancing, rather than advancing according to a specific time frame. Because of this design, the ITP may be used for different levels of skills and abilities compared to those characteristic of high school to professional levels. Progression will vary from person to person throughout the ITP. As an example, one athlete may wish to use alternate days throwing with or without using weights in between; another athlete may have to throw every third or fourth day due to pain or swelling. The athlete should be reminded to listen to her body, since pain signifies when it may be necessary to slow down. Again, completion of the steps of the ITP will vary from person to person. There is no set timetable with regard to days to completion.
Unlock the full program with Sport Therapy for the Shoulder.
What is happening in the shoulder complex during a golf swing?
Similar to the situation with the other sports reviewed in this chapter, to isolate and identify the functions of the major muscles controlling the various body segments during the golf swing, dynamic EMG and high-speed motion analysis has been used and helps to provide a greater understanding of the demands of golf on the shoulder complex.
Golf Swing Mechanics
Similar to the situation with the other sports reviewed in this chapter, to isolate and identify the functions of the major muscles controlling the various body segments during the golf swing, dynamic EMG and high-speed motion analysis has been used and helps to provide a greater understanding of the demands of golf on the shoulder complex. For discussion and analysis purposes, the golf swing has been broken down into the following five phases (Pink et al. 1993):
- Take-away: from address to the ball to the end of the backswing
- Forward swing: from the end of the backswing until the club is horizontal
- Acceleration: from horizontal position of the club to ball contact
- Early follow-through: from ball contact to horizontal club position
- Late follow-through: from horizontal club position to the end of the swing
|
|
|
Muscles used in three of the five phases of the golf swing: (a) take-away, (b) acceleration, and (c) follow-through.
This section describes and compares the muscle activity patterns of the primary shoulder and scapular muscles (but note that there are also significant contributions from other body segments during a golf swing).
Take-Away
Before initiation of the backswing, proper setup and ball address must be achieved. This initial posture greatly influences the balance of forces throughout the golf swing and is therefore critical to the achievement of the proper swing plane. The take-away phase has been described as a "coiling" or "loading" of the body in order to enhance the velocity and kinetic energy of the club head (Pink et al. 1990). Electromyographic analysis reveals relatively low activity of the trunk musculature during this segment of the golf swing, as the trunk is simply preparing for the swing (Pink et al. 1990). Electromyographic analysis of the scapular muscles of the trailing arm reveals relatively high activity of the upper, middle, and lower portions of the trapezius during take-away in order to help the scapula retract and upwardly rotate (Kao et al. 1995). Similarly, the levator scapulae and rhomboid muscle of the trailing arm are active during this period to help with such scapular movements (Kao et al. 1995). In the leading arm during take-away, the activity of the scapular stabilizing muscles is relatively low to allow for scapular protraction.
Electromyographic analysis of the rotator cuff muscles exhibits contributions from the supraspinatus and infraspinatus in the trailing arm as they act to approximate and stabilize the shoulder (Jobe et al. 1986, Pink et al. 1990). Of the rotator cuff muscles in the leading arm, only the subscapularis was shown to display marked activity during the take-away phase. It should be noted that the pectoralis major, latissimus dorsi, and the deltoid muscles of both arms are relatively inactive in the backswing of the golf club (Jobe et al. 1986, Pink et al. 1990).
Forward Swing
During forward swing, trunk rotation movement is initiated. Analysis of the trailing arm scapular muscles shows that the three portions of the trapezius have lower activation to allow for scapular protraction (Kao et al. 1995). However, the levator scapulae and rhomboid muscles display marked activity to control scapular protraction and rotation of the trailing arm. Analysis of the serratus anterior muscle in the trailing arm shows increased activity during forward swing to aid in scapular protraction and stabilization (Kao et al. 1995). Electromyographic studies of the lead arm demonstrate high activity of the trapezius, levator scapulae, rhomboids, and serratus anterior as they all contribute to scapular motion and stabilization as the arms move toward the ball (Kao et al. 1995).
Of the trailing shoulder muscles during forward swing, the subscapularis, pectoralis major, and latissimus begin firing at marked levels as the trailing arm increasingly accelerates into the internal rotation and adduction. The lead arm subscapularis and latissimus dorsi are both moderately active during the forward swing phase.
Acceleration
During the acceleration phase, the body segments work together in a coordinated sequence in order to maximize club head speed at ball impact. The serratus anterior is the primary scapular stabilizer that is active in the trailing arm during acceleration (Kao et al. 1995). The serratus has high levels of involvement in order to allow for a strong scapular protraction and contribute to maximizing club head speed. Conversely, EMG analysis reveals strong contractions of the scapular muscles in the lead arm during acceleration (Kao et al. 1995). The trapezius, levator scapulae, and rhomboid muscles are firing to aid in scapular retraction, upward rotation, and elevation. The serratus anterior of the lead arm continues to display high levels of activation throughout. This important muscle is highly involved during the golf swing, similarly to what is seen during throwing and the tennis serve as discussed in earlier sections of this chapter.
Electromyographic investigations display high levels of subscapularis, pectoralis major, and latissimus dorsi activity to provide power to the trailing arm during acceleration (Jobe et al. 1986). These important muscles further increase in activity from forward swing to assist in rotation and forceful adduction of the arm during this phase. The latissimus dorsi contributes most of its power in the forward swing, while the pectoralis major supplies the most power during acceleration (Pink et al. 1990). Similarly, the subscapularis, pectoralis major, and latissimus dorsi of the lead arm fire at high rates during the acceleration phase (Jobe et al. 1986, Pink et al. 1990).
Early Follow-Through
After ball contact has been made, the follow-through phase is initiated. During early follow-through, nearly all the body segments work to decelerate their rotational contributions, often through eccentric muscle contractions (Jobe et al. 1986, Pink et al. 1993). The scapular muscles of both the trailing and lead arms display decreased activity throughout the follow-through phases, allowing for coordinated scapular protraction (Kao et al. 1995). Despite this decrease in scapular activity, the serratus anterior muscles of both arms show fairly consistent muscle firing patterns providing vital scapular stabilization throughout the follow-through phases (Kao et al. 1995).
In the trailing shoulder, marked activity of the subscapularis, pectoralis major, and latissimus dorsi muscles continues into the early follow-through phase (Jobe et al. 1986). For the lead shoulder, the subscapularis continues its high level of activity, while the pectoralis major and latissimus dorsi decrease their contributions (Jobe et al. 1986, Pink et al. 1990).
Late Follow-Through
Activity of the scapular muscles of both arms decreases to lower levels as the swing comes to an end (Kao et al. 1995). The subscapularis of the trailing shoulder is one of the only muscles that remains highly active during this phase (Jobe et al. 1986, Pink et al. 1990). Analysis of the lead arm reveals marked activity of the infraspinatus and the supraspinatus rotator cuff muscles used for glenohumeral stabilization (Pink et al. 1990).
One final discussion regarding the golf swing concerns a common mechanical fault that many golfers have, placing their glenohumeral joints at risk. During take-away, the lead arm is placed into increasing degrees of internal rotation and cross-body adduction. This position may predispose the golfer to impingement-type problems as the rotator cuff tendons and bursae are compressed within the shoulder (Mallon 1996). Additionally, at the end of the backswing, forces on the acromioclavicular joint of the lead arm are shown to be high, contributing to the incidence of pain often seen in the golfer's shoulder. The posterior rotator cuff and scapular muscles of the lead arm are also at risk for injury at the TOB as they are placed under a stretch load to achieve that position (Mallon 1996).
Save
Save
Save
Save
Learn more about Sport Therapy for the Shoulder.
Improve shoulder internal rotation range of motion for throwing athletes
Now that interpretation of glenohumeral joint ROM has been discussed, this section outlines specific techniques to increase IR ROM in the patient with shoulder dysfunction.
Methods to Improve Shoulder Internal Rotation (IR) Range of Motion (ROM) in the Throwing Athlete
Now that interpretation of glenohumeral joint ROM has been discussed, this section outlines specific techniques to increase IR ROM in the patient with shoulder dysfunction. This section, addressing the importance of accurate ROM measurement and clinical decision making based on the latest scientific evidence, can guide the clinician through the rehabilitation process; one can encounter a large spectrum of mobility issues when treating the patient with glenohumeral impingement. To further illustrate the role of ROM and passive stretching during this phase of the rehabilitation, figures 5.4 and 5.5 show versions of clinical IR stretching positions that use the scapular plane and that can be performed in multiple and varied positions of glenohumeral abduction. Each inherently possesses an anterior hand placement, used to exert varying degrees of posterior pressure to minimize scapular compensation and also to provide a checkrein against anterior humeral head translation during the IR stretch because of the effects of obligate translation.
Internal rotation range of motion technique in the scapular plane with 30° of elevation with scapular stabilization.
Internal rotation range of motion technique with scapular stabilization and 45° of glenohumeral joint elevation in the scapular plane. Note that the amount of elevation used with this stretch can be varied from as little as 0⁰ to 10⁰ all the way to 90⁰.
Research by Izumi and colleagues (2008) showed that large strains occurred in the posterior capsule in a stretching position of 30⁰ of elevation in the scapular plane with IR. These researchers compared many positions of shoulder ROM to determine what position optimally placed stress on the posterior capsule. The internally rotated position with the shoulder elevated 30⁰ in the scapular plane produced very acceptable levels of posterior capsular strain and would be highly effective for clinical use. These stretches for the posterior capsule and muscle - tendon unit (posterior shoulder stretches) can be used in a proprioceptive neuromuscular facilitation (PNF) contract - relax format following a low-load prolonged stretch-type paradigm to facilitate the increase in ROM (Sullivan et al. 1982, Zachezewski & Reischl 1986).
Save
Save
Save
Save
Save
Find more stretches to address IR ROM in Sport Therapy for the Shoulder.
Baseball and softball (throwing) program
The interval sport return program for baseball and softball (throwing) is designed to gradually return motion and strength to (and confidence in) the throwing arm after injury or surgery by slowly progressing through graduated throwing distances.
The interval sport return program for baseball and softball (throwing) is designed to gradually return motion and strength to (and confidence in) the throwing arm after injury or surgery by slowly progressing through graduated throwing distances. The program begins upon clearance by the athlete's physician to resume throwing and is performed under the supervision of the rehabilitation team (physician, physical therapist, and athletic trainer). The program is set up to minimize the chance of reinjury and emphasize prethrowing warm-up and stretching. In development of the interval throwing program (ITP), the following factors are considered most important:
- The act of throwing the baseball involves the transfer of energy from the feet through the legs, pelvis, and trunk and out the shoulder through the elbow and hand. Therefore, any return to throwing after injury must include attention to the entire body.
- The chance for reinjury is lessened by a graduated progression of interval throwing.
- Proper warm-up is essential.
- Most injuries occur as the result of fatigue.
- Proper throwing mechanics lessen the incidence of reinjury.
- Baseline requirements for throwing include these:
- Pain-free ROM
- Adequate muscle power
- Adequate muscle resistance to fatigue
Because of individual variability among throwing athletes, there is no set timetable for completion of the program. Most athletes, by nature, are highly competitive individuals and wish to return to competition at the earliest possible moment. While this is a necessary quality in all athletes, the proper channeling of the athlete's energies into a strictly controlled throwing program is essential to lessen the chance of reinjury during the rehabilitation process. The athlete may tend to want to increase the intensity of the throwing program. This will increase the incidence of reinjury and may greatly retard the rehabilitation process. The recommendation is to follow the program exactly, as this is the safest route to return to competition.
During the recovery process the athlete will probably experience soreness and a dull, diffuse aching sensation in the muscles and tendons. If the athlete experiences sharp pain, particularly in the joint, all throwing activity should be stopped until this pain ceases. If the pain continues, he should contact his physician.
Weight Training
The athlete should supplement the ITP with a high-repetition, low-weight exercise program. Strengthening should address a good balance between anterior and posterior musculature so that the shoulder will not be predisposed to injury. Special emphasis must be given to posterior rotator cuff musculature for any strengthening program. Weight training does not increase throwing velocity, but it increases the resistance of the arm to fatigue and injury. The athlete should do weight training on the same day as throwing but after the throwing has been completed; the day in between should be used for flexibility exercises and a recovery period. A weight training pattern or routine should be stressed at this point as a "maintenance program." This pattern can and should accompany the athlete into and throughout the season as a deterrent to further injury. It must be emphasized that weight training is of no benefit unless accompanied by a sound flexibility program.
Individual Variability
The ITP is designed so that each level is achieved without pain or complications before the next level is initiated. This sets up a progression in which the athlete achieves a goal before advancing, rather than advancing according to a specific time frame. Because of this design, the ITP may be used for different levels of skills and abilities compared to those characteristic of high school to professional levels. Progression will vary from person to person throughout the ITP. As an example, one athlete may wish to use alternate days throwing with or without using weights in between; another athlete may have to throw every third or fourth day due to pain or swelling. The athlete should be reminded to listen to her body, since pain signifies when it may be necessary to slow down. Again, completion of the steps of the ITP will vary from person to person. There is no set timetable with regard to days to completion.
Unlock the full program with Sport Therapy for the Shoulder.
What is happening in the shoulder complex during a golf swing?
Similar to the situation with the other sports reviewed in this chapter, to isolate and identify the functions of the major muscles controlling the various body segments during the golf swing, dynamic EMG and high-speed motion analysis has been used and helps to provide a greater understanding of the demands of golf on the shoulder complex.
Golf Swing Mechanics
Similar to the situation with the other sports reviewed in this chapter, to isolate and identify the functions of the major muscles controlling the various body segments during the golf swing, dynamic EMG and high-speed motion analysis has been used and helps to provide a greater understanding of the demands of golf on the shoulder complex. For discussion and analysis purposes, the golf swing has been broken down into the following five phases (Pink et al. 1993):
- Take-away: from address to the ball to the end of the backswing
- Forward swing: from the end of the backswing until the club is horizontal
- Acceleration: from horizontal position of the club to ball contact
- Early follow-through: from ball contact to horizontal club position
- Late follow-through: from horizontal club position to the end of the swing
|
|
|
Muscles used in three of the five phases of the golf swing: (a) take-away, (b) acceleration, and (c) follow-through.
This section describes and compares the muscle activity patterns of the primary shoulder and scapular muscles (but note that there are also significant contributions from other body segments during a golf swing).
Take-Away
Before initiation of the backswing, proper setup and ball address must be achieved. This initial posture greatly influences the balance of forces throughout the golf swing and is therefore critical to the achievement of the proper swing plane. The take-away phase has been described as a "coiling" or "loading" of the body in order to enhance the velocity and kinetic energy of the club head (Pink et al. 1990). Electromyographic analysis reveals relatively low activity of the trunk musculature during this segment of the golf swing, as the trunk is simply preparing for the swing (Pink et al. 1990). Electromyographic analysis of the scapular muscles of the trailing arm reveals relatively high activity of the upper, middle, and lower portions of the trapezius during take-away in order to help the scapula retract and upwardly rotate (Kao et al. 1995). Similarly, the levator scapulae and rhomboid muscle of the trailing arm are active during this period to help with such scapular movements (Kao et al. 1995). In the leading arm during take-away, the activity of the scapular stabilizing muscles is relatively low to allow for scapular protraction.
Electromyographic analysis of the rotator cuff muscles exhibits contributions from the supraspinatus and infraspinatus in the trailing arm as they act to approximate and stabilize the shoulder (Jobe et al. 1986, Pink et al. 1990). Of the rotator cuff muscles in the leading arm, only the subscapularis was shown to display marked activity during the take-away phase. It should be noted that the pectoralis major, latissimus dorsi, and the deltoid muscles of both arms are relatively inactive in the backswing of the golf club (Jobe et al. 1986, Pink et al. 1990).
Forward Swing
During forward swing, trunk rotation movement is initiated. Analysis of the trailing arm scapular muscles shows that the three portions of the trapezius have lower activation to allow for scapular protraction (Kao et al. 1995). However, the levator scapulae and rhomboid muscles display marked activity to control scapular protraction and rotation of the trailing arm. Analysis of the serratus anterior muscle in the trailing arm shows increased activity during forward swing to aid in scapular protraction and stabilization (Kao et al. 1995). Electromyographic studies of the lead arm demonstrate high activity of the trapezius, levator scapulae, rhomboids, and serratus anterior as they all contribute to scapular motion and stabilization as the arms move toward the ball (Kao et al. 1995).
Of the trailing shoulder muscles during forward swing, the subscapularis, pectoralis major, and latissimus begin firing at marked levels as the trailing arm increasingly accelerates into the internal rotation and adduction. The lead arm subscapularis and latissimus dorsi are both moderately active during the forward swing phase.
Acceleration
During the acceleration phase, the body segments work together in a coordinated sequence in order to maximize club head speed at ball impact. The serratus anterior is the primary scapular stabilizer that is active in the trailing arm during acceleration (Kao et al. 1995). The serratus has high levels of involvement in order to allow for a strong scapular protraction and contribute to maximizing club head speed. Conversely, EMG analysis reveals strong contractions of the scapular muscles in the lead arm during acceleration (Kao et al. 1995). The trapezius, levator scapulae, and rhomboid muscles are firing to aid in scapular retraction, upward rotation, and elevation. The serratus anterior of the lead arm continues to display high levels of activation throughout. This important muscle is highly involved during the golf swing, similarly to what is seen during throwing and the tennis serve as discussed in earlier sections of this chapter.
Electromyographic investigations display high levels of subscapularis, pectoralis major, and latissimus dorsi activity to provide power to the trailing arm during acceleration (Jobe et al. 1986). These important muscles further increase in activity from forward swing to assist in rotation and forceful adduction of the arm during this phase. The latissimus dorsi contributes most of its power in the forward swing, while the pectoralis major supplies the most power during acceleration (Pink et al. 1990). Similarly, the subscapularis, pectoralis major, and latissimus dorsi of the lead arm fire at high rates during the acceleration phase (Jobe et al. 1986, Pink et al. 1990).
Early Follow-Through
After ball contact has been made, the follow-through phase is initiated. During early follow-through, nearly all the body segments work to decelerate their rotational contributions, often through eccentric muscle contractions (Jobe et al. 1986, Pink et al. 1993). The scapular muscles of both the trailing and lead arms display decreased activity throughout the follow-through phases, allowing for coordinated scapular protraction (Kao et al. 1995). Despite this decrease in scapular activity, the serratus anterior muscles of both arms show fairly consistent muscle firing patterns providing vital scapular stabilization throughout the follow-through phases (Kao et al. 1995).
In the trailing shoulder, marked activity of the subscapularis, pectoralis major, and latissimus dorsi muscles continues into the early follow-through phase (Jobe et al. 1986). For the lead shoulder, the subscapularis continues its high level of activity, while the pectoralis major and latissimus dorsi decrease their contributions (Jobe et al. 1986, Pink et al. 1990).
Late Follow-Through
Activity of the scapular muscles of both arms decreases to lower levels as the swing comes to an end (Kao et al. 1995). The subscapularis of the trailing shoulder is one of the only muscles that remains highly active during this phase (Jobe et al. 1986, Pink et al. 1990). Analysis of the lead arm reveals marked activity of the infraspinatus and the supraspinatus rotator cuff muscles used for glenohumeral stabilization (Pink et al. 1990).
One final discussion regarding the golf swing concerns a common mechanical fault that many golfers have, placing their glenohumeral joints at risk. During take-away, the lead arm is placed into increasing degrees of internal rotation and cross-body adduction. This position may predispose the golfer to impingement-type problems as the rotator cuff tendons and bursae are compressed within the shoulder (Mallon 1996). Additionally, at the end of the backswing, forces on the acromioclavicular joint of the lead arm are shown to be high, contributing to the incidence of pain often seen in the golfer's shoulder. The posterior rotator cuff and scapular muscles of the lead arm are also at risk for injury at the TOB as they are placed under a stretch load to achieve that position (Mallon 1996).
Save
Save
Save
Save
Learn more about Sport Therapy for the Shoulder.
Improve shoulder internal rotation range of motion for throwing athletes
Now that interpretation of glenohumeral joint ROM has been discussed, this section outlines specific techniques to increase IR ROM in the patient with shoulder dysfunction.
Methods to Improve Shoulder Internal Rotation (IR) Range of Motion (ROM) in the Throwing Athlete
Now that interpretation of glenohumeral joint ROM has been discussed, this section outlines specific techniques to increase IR ROM in the patient with shoulder dysfunction. This section, addressing the importance of accurate ROM measurement and clinical decision making based on the latest scientific evidence, can guide the clinician through the rehabilitation process; one can encounter a large spectrum of mobility issues when treating the patient with glenohumeral impingement. To further illustrate the role of ROM and passive stretching during this phase of the rehabilitation, figures 5.4 and 5.5 show versions of clinical IR stretching positions that use the scapular plane and that can be performed in multiple and varied positions of glenohumeral abduction. Each inherently possesses an anterior hand placement, used to exert varying degrees of posterior pressure to minimize scapular compensation and also to provide a checkrein against anterior humeral head translation during the IR stretch because of the effects of obligate translation.
Internal rotation range of motion technique in the scapular plane with 30° of elevation with scapular stabilization.
Internal rotation range of motion technique with scapular stabilization and 45° of glenohumeral joint elevation in the scapular plane. Note that the amount of elevation used with this stretch can be varied from as little as 0⁰ to 10⁰ all the way to 90⁰.
Research by Izumi and colleagues (2008) showed that large strains occurred in the posterior capsule in a stretching position of 30⁰ of elevation in the scapular plane with IR. These researchers compared many positions of shoulder ROM to determine what position optimally placed stress on the posterior capsule. The internally rotated position with the shoulder elevated 30⁰ in the scapular plane produced very acceptable levels of posterior capsular strain and would be highly effective for clinical use. These stretches for the posterior capsule and muscle - tendon unit (posterior shoulder stretches) can be used in a proprioceptive neuromuscular facilitation (PNF) contract - relax format following a low-load prolonged stretch-type paradigm to facilitate the increase in ROM (Sullivan et al. 1982, Zachezewski & Reischl 1986).
Save
Save
Save
Save
Save
Find more stretches to address IR ROM in Sport Therapy for the Shoulder.
Baseball and softball (throwing) program
The interval sport return program for baseball and softball (throwing) is designed to gradually return motion and strength to (and confidence in) the throwing arm after injury or surgery by slowly progressing through graduated throwing distances.
The interval sport return program for baseball and softball (throwing) is designed to gradually return motion and strength to (and confidence in) the throwing arm after injury or surgery by slowly progressing through graduated throwing distances. The program begins upon clearance by the athlete's physician to resume throwing and is performed under the supervision of the rehabilitation team (physician, physical therapist, and athletic trainer). The program is set up to minimize the chance of reinjury and emphasize prethrowing warm-up and stretching. In development of the interval throwing program (ITP), the following factors are considered most important:
- The act of throwing the baseball involves the transfer of energy from the feet through the legs, pelvis, and trunk and out the shoulder through the elbow and hand. Therefore, any return to throwing after injury must include attention to the entire body.
- The chance for reinjury is lessened by a graduated progression of interval throwing.
- Proper warm-up is essential.
- Most injuries occur as the result of fatigue.
- Proper throwing mechanics lessen the incidence of reinjury.
- Baseline requirements for throwing include these:
- Pain-free ROM
- Adequate muscle power
- Adequate muscle resistance to fatigue
Because of individual variability among throwing athletes, there is no set timetable for completion of the program. Most athletes, by nature, are highly competitive individuals and wish to return to competition at the earliest possible moment. While this is a necessary quality in all athletes, the proper channeling of the athlete's energies into a strictly controlled throwing program is essential to lessen the chance of reinjury during the rehabilitation process. The athlete may tend to want to increase the intensity of the throwing program. This will increase the incidence of reinjury and may greatly retard the rehabilitation process. The recommendation is to follow the program exactly, as this is the safest route to return to competition.
During the recovery process the athlete will probably experience soreness and a dull, diffuse aching sensation in the muscles and tendons. If the athlete experiences sharp pain, particularly in the joint, all throwing activity should be stopped until this pain ceases. If the pain continues, he should contact his physician.
Weight Training
The athlete should supplement the ITP with a high-repetition, low-weight exercise program. Strengthening should address a good balance between anterior and posterior musculature so that the shoulder will not be predisposed to injury. Special emphasis must be given to posterior rotator cuff musculature for any strengthening program. Weight training does not increase throwing velocity, but it increases the resistance of the arm to fatigue and injury. The athlete should do weight training on the same day as throwing but after the throwing has been completed; the day in between should be used for flexibility exercises and a recovery period. A weight training pattern or routine should be stressed at this point as a "maintenance program." This pattern can and should accompany the athlete into and throughout the season as a deterrent to further injury. It must be emphasized that weight training is of no benefit unless accompanied by a sound flexibility program.
Individual Variability
The ITP is designed so that each level is achieved without pain or complications before the next level is initiated. This sets up a progression in which the athlete achieves a goal before advancing, rather than advancing according to a specific time frame. Because of this design, the ITP may be used for different levels of skills and abilities compared to those characteristic of high school to professional levels. Progression will vary from person to person throughout the ITP. As an example, one athlete may wish to use alternate days throwing with or without using weights in between; another athlete may have to throw every third or fourth day due to pain or swelling. The athlete should be reminded to listen to her body, since pain signifies when it may be necessary to slow down. Again, completion of the steps of the ITP will vary from person to person. There is no set timetable with regard to days to completion.
Unlock the full program with Sport Therapy for the Shoulder.
What is happening in the shoulder complex during a golf swing?
Similar to the situation with the other sports reviewed in this chapter, to isolate and identify the functions of the major muscles controlling the various body segments during the golf swing, dynamic EMG and high-speed motion analysis has been used and helps to provide a greater understanding of the demands of golf on the shoulder complex.
Golf Swing Mechanics
Similar to the situation with the other sports reviewed in this chapter, to isolate and identify the functions of the major muscles controlling the various body segments during the golf swing, dynamic EMG and high-speed motion analysis has been used and helps to provide a greater understanding of the demands of golf on the shoulder complex. For discussion and analysis purposes, the golf swing has been broken down into the following five phases (Pink et al. 1993):
- Take-away: from address to the ball to the end of the backswing
- Forward swing: from the end of the backswing until the club is horizontal
- Acceleration: from horizontal position of the club to ball contact
- Early follow-through: from ball contact to horizontal club position
- Late follow-through: from horizontal club position to the end of the swing
|
|
|
Muscles used in three of the five phases of the golf swing: (a) take-away, (b) acceleration, and (c) follow-through.
This section describes and compares the muscle activity patterns of the primary shoulder and scapular muscles (but note that there are also significant contributions from other body segments during a golf swing).
Take-Away
Before initiation of the backswing, proper setup and ball address must be achieved. This initial posture greatly influences the balance of forces throughout the golf swing and is therefore critical to the achievement of the proper swing plane. The take-away phase has been described as a "coiling" or "loading" of the body in order to enhance the velocity and kinetic energy of the club head (Pink et al. 1990). Electromyographic analysis reveals relatively low activity of the trunk musculature during this segment of the golf swing, as the trunk is simply preparing for the swing (Pink et al. 1990). Electromyographic analysis of the scapular muscles of the trailing arm reveals relatively high activity of the upper, middle, and lower portions of the trapezius during take-away in order to help the scapula retract and upwardly rotate (Kao et al. 1995). Similarly, the levator scapulae and rhomboid muscle of the trailing arm are active during this period to help with such scapular movements (Kao et al. 1995). In the leading arm during take-away, the activity of the scapular stabilizing muscles is relatively low to allow for scapular protraction.
Electromyographic analysis of the rotator cuff muscles exhibits contributions from the supraspinatus and infraspinatus in the trailing arm as they act to approximate and stabilize the shoulder (Jobe et al. 1986, Pink et al. 1990). Of the rotator cuff muscles in the leading arm, only the subscapularis was shown to display marked activity during the take-away phase. It should be noted that the pectoralis major, latissimus dorsi, and the deltoid muscles of both arms are relatively inactive in the backswing of the golf club (Jobe et al. 1986, Pink et al. 1990).
Forward Swing
During forward swing, trunk rotation movement is initiated. Analysis of the trailing arm scapular muscles shows that the three portions of the trapezius have lower activation to allow for scapular protraction (Kao et al. 1995). However, the levator scapulae and rhomboid muscles display marked activity to control scapular protraction and rotation of the trailing arm. Analysis of the serratus anterior muscle in the trailing arm shows increased activity during forward swing to aid in scapular protraction and stabilization (Kao et al. 1995). Electromyographic studies of the lead arm demonstrate high activity of the trapezius, levator scapulae, rhomboids, and serratus anterior as they all contribute to scapular motion and stabilization as the arms move toward the ball (Kao et al. 1995).
Of the trailing shoulder muscles during forward swing, the subscapularis, pectoralis major, and latissimus begin firing at marked levels as the trailing arm increasingly accelerates into the internal rotation and adduction. The lead arm subscapularis and latissimus dorsi are both moderately active during the forward swing phase.
Acceleration
During the acceleration phase, the body segments work together in a coordinated sequence in order to maximize club head speed at ball impact. The serratus anterior is the primary scapular stabilizer that is active in the trailing arm during acceleration (Kao et al. 1995). The serratus has high levels of involvement in order to allow for a strong scapular protraction and contribute to maximizing club head speed. Conversely, EMG analysis reveals strong contractions of the scapular muscles in the lead arm during acceleration (Kao et al. 1995). The trapezius, levator scapulae, and rhomboid muscles are firing to aid in scapular retraction, upward rotation, and elevation. The serratus anterior of the lead arm continues to display high levels of activation throughout. This important muscle is highly involved during the golf swing, similarly to what is seen during throwing and the tennis serve as discussed in earlier sections of this chapter.
Electromyographic investigations display high levels of subscapularis, pectoralis major, and latissimus dorsi activity to provide power to the trailing arm during acceleration (Jobe et al. 1986). These important muscles further increase in activity from forward swing to assist in rotation and forceful adduction of the arm during this phase. The latissimus dorsi contributes most of its power in the forward swing, while the pectoralis major supplies the most power during acceleration (Pink et al. 1990). Similarly, the subscapularis, pectoralis major, and latissimus dorsi of the lead arm fire at high rates during the acceleration phase (Jobe et al. 1986, Pink et al. 1990).
Early Follow-Through
After ball contact has been made, the follow-through phase is initiated. During early follow-through, nearly all the body segments work to decelerate their rotational contributions, often through eccentric muscle contractions (Jobe et al. 1986, Pink et al. 1993). The scapular muscles of both the trailing and lead arms display decreased activity throughout the follow-through phases, allowing for coordinated scapular protraction (Kao et al. 1995). Despite this decrease in scapular activity, the serratus anterior muscles of both arms show fairly consistent muscle firing patterns providing vital scapular stabilization throughout the follow-through phases (Kao et al. 1995).
In the trailing shoulder, marked activity of the subscapularis, pectoralis major, and latissimus dorsi muscles continues into the early follow-through phase (Jobe et al. 1986). For the lead shoulder, the subscapularis continues its high level of activity, while the pectoralis major and latissimus dorsi decrease their contributions (Jobe et al. 1986, Pink et al. 1990).
Late Follow-Through
Activity of the scapular muscles of both arms decreases to lower levels as the swing comes to an end (Kao et al. 1995). The subscapularis of the trailing shoulder is one of the only muscles that remains highly active during this phase (Jobe et al. 1986, Pink et al. 1990). Analysis of the lead arm reveals marked activity of the infraspinatus and the supraspinatus rotator cuff muscles used for glenohumeral stabilization (Pink et al. 1990).
One final discussion regarding the golf swing concerns a common mechanical fault that many golfers have, placing their glenohumeral joints at risk. During take-away, the lead arm is placed into increasing degrees of internal rotation and cross-body adduction. This position may predispose the golfer to impingement-type problems as the rotator cuff tendons and bursae are compressed within the shoulder (Mallon 1996). Additionally, at the end of the backswing, forces on the acromioclavicular joint of the lead arm are shown to be high, contributing to the incidence of pain often seen in the golfer's shoulder. The posterior rotator cuff and scapular muscles of the lead arm are also at risk for injury at the TOB as they are placed under a stretch load to achieve that position (Mallon 1996).
Save
Save
Save
Save
Learn more about Sport Therapy for the Shoulder.
Improve shoulder internal rotation range of motion for throwing athletes
Now that interpretation of glenohumeral joint ROM has been discussed, this section outlines specific techniques to increase IR ROM in the patient with shoulder dysfunction.
Methods to Improve Shoulder Internal Rotation (IR) Range of Motion (ROM) in the Throwing Athlete
Now that interpretation of glenohumeral joint ROM has been discussed, this section outlines specific techniques to increase IR ROM in the patient with shoulder dysfunction. This section, addressing the importance of accurate ROM measurement and clinical decision making based on the latest scientific evidence, can guide the clinician through the rehabilitation process; one can encounter a large spectrum of mobility issues when treating the patient with glenohumeral impingement. To further illustrate the role of ROM and passive stretching during this phase of the rehabilitation, figures 5.4 and 5.5 show versions of clinical IR stretching positions that use the scapular plane and that can be performed in multiple and varied positions of glenohumeral abduction. Each inherently possesses an anterior hand placement, used to exert varying degrees of posterior pressure to minimize scapular compensation and also to provide a checkrein against anterior humeral head translation during the IR stretch because of the effects of obligate translation.
Internal rotation range of motion technique in the scapular plane with 30° of elevation with scapular stabilization.
Internal rotation range of motion technique with scapular stabilization and 45° of glenohumeral joint elevation in the scapular plane. Note that the amount of elevation used with this stretch can be varied from as little as 0⁰ to 10⁰ all the way to 90⁰.
Research by Izumi and colleagues (2008) showed that large strains occurred in the posterior capsule in a stretching position of 30⁰ of elevation in the scapular plane with IR. These researchers compared many positions of shoulder ROM to determine what position optimally placed stress on the posterior capsule. The internally rotated position with the shoulder elevated 30⁰ in the scapular plane produced very acceptable levels of posterior capsular strain and would be highly effective for clinical use. These stretches for the posterior capsule and muscle - tendon unit (posterior shoulder stretches) can be used in a proprioceptive neuromuscular facilitation (PNF) contract - relax format following a low-load prolonged stretch-type paradigm to facilitate the increase in ROM (Sullivan et al. 1982, Zachezewski & Reischl 1986).
Save
Save
Save
Save
Save
Find more stretches to address IR ROM in Sport Therapy for the Shoulder.
Baseball and softball (throwing) program
The interval sport return program for baseball and softball (throwing) is designed to gradually return motion and strength to (and confidence in) the throwing arm after injury or surgery by slowly progressing through graduated throwing distances.
The interval sport return program for baseball and softball (throwing) is designed to gradually return motion and strength to (and confidence in) the throwing arm after injury or surgery by slowly progressing through graduated throwing distances. The program begins upon clearance by the athlete's physician to resume throwing and is performed under the supervision of the rehabilitation team (physician, physical therapist, and athletic trainer). The program is set up to minimize the chance of reinjury and emphasize prethrowing warm-up and stretching. In development of the interval throwing program (ITP), the following factors are considered most important:
- The act of throwing the baseball involves the transfer of energy from the feet through the legs, pelvis, and trunk and out the shoulder through the elbow and hand. Therefore, any return to throwing after injury must include attention to the entire body.
- The chance for reinjury is lessened by a graduated progression of interval throwing.
- Proper warm-up is essential.
- Most injuries occur as the result of fatigue.
- Proper throwing mechanics lessen the incidence of reinjury.
- Baseline requirements for throwing include these:
- Pain-free ROM
- Adequate muscle power
- Adequate muscle resistance to fatigue
Because of individual variability among throwing athletes, there is no set timetable for completion of the program. Most athletes, by nature, are highly competitive individuals and wish to return to competition at the earliest possible moment. While this is a necessary quality in all athletes, the proper channeling of the athlete's energies into a strictly controlled throwing program is essential to lessen the chance of reinjury during the rehabilitation process. The athlete may tend to want to increase the intensity of the throwing program. This will increase the incidence of reinjury and may greatly retard the rehabilitation process. The recommendation is to follow the program exactly, as this is the safest route to return to competition.
During the recovery process the athlete will probably experience soreness and a dull, diffuse aching sensation in the muscles and tendons. If the athlete experiences sharp pain, particularly in the joint, all throwing activity should be stopped until this pain ceases. If the pain continues, he should contact his physician.
Weight Training
The athlete should supplement the ITP with a high-repetition, low-weight exercise program. Strengthening should address a good balance between anterior and posterior musculature so that the shoulder will not be predisposed to injury. Special emphasis must be given to posterior rotator cuff musculature for any strengthening program. Weight training does not increase throwing velocity, but it increases the resistance of the arm to fatigue and injury. The athlete should do weight training on the same day as throwing but after the throwing has been completed; the day in between should be used for flexibility exercises and a recovery period. A weight training pattern or routine should be stressed at this point as a "maintenance program." This pattern can and should accompany the athlete into and throughout the season as a deterrent to further injury. It must be emphasized that weight training is of no benefit unless accompanied by a sound flexibility program.
Individual Variability
The ITP is designed so that each level is achieved without pain or complications before the next level is initiated. This sets up a progression in which the athlete achieves a goal before advancing, rather than advancing according to a specific time frame. Because of this design, the ITP may be used for different levels of skills and abilities compared to those characteristic of high school to professional levels. Progression will vary from person to person throughout the ITP. As an example, one athlete may wish to use alternate days throwing with or without using weights in between; another athlete may have to throw every third or fourth day due to pain or swelling. The athlete should be reminded to listen to her body, since pain signifies when it may be necessary to slow down. Again, completion of the steps of the ITP will vary from person to person. There is no set timetable with regard to days to completion.
Unlock the full program with Sport Therapy for the Shoulder.
What is happening in the shoulder complex during a golf swing?
Similar to the situation with the other sports reviewed in this chapter, to isolate and identify the functions of the major muscles controlling the various body segments during the golf swing, dynamic EMG and high-speed motion analysis has been used and helps to provide a greater understanding of the demands of golf on the shoulder complex.
Golf Swing Mechanics
Similar to the situation with the other sports reviewed in this chapter, to isolate and identify the functions of the major muscles controlling the various body segments during the golf swing, dynamic EMG and high-speed motion analysis has been used and helps to provide a greater understanding of the demands of golf on the shoulder complex. For discussion and analysis purposes, the golf swing has been broken down into the following five phases (Pink et al. 1993):
- Take-away: from address to the ball to the end of the backswing
- Forward swing: from the end of the backswing until the club is horizontal
- Acceleration: from horizontal position of the club to ball contact
- Early follow-through: from ball contact to horizontal club position
- Late follow-through: from horizontal club position to the end of the swing
|
|
|
Muscles used in three of the five phases of the golf swing: (a) take-away, (b) acceleration, and (c) follow-through.
This section describes and compares the muscle activity patterns of the primary shoulder and scapular muscles (but note that there are also significant contributions from other body segments during a golf swing).
Take-Away
Before initiation of the backswing, proper setup and ball address must be achieved. This initial posture greatly influences the balance of forces throughout the golf swing and is therefore critical to the achievement of the proper swing plane. The take-away phase has been described as a "coiling" or "loading" of the body in order to enhance the velocity and kinetic energy of the club head (Pink et al. 1990). Electromyographic analysis reveals relatively low activity of the trunk musculature during this segment of the golf swing, as the trunk is simply preparing for the swing (Pink et al. 1990). Electromyographic analysis of the scapular muscles of the trailing arm reveals relatively high activity of the upper, middle, and lower portions of the trapezius during take-away in order to help the scapula retract and upwardly rotate (Kao et al. 1995). Similarly, the levator scapulae and rhomboid muscle of the trailing arm are active during this period to help with such scapular movements (Kao et al. 1995). In the leading arm during take-away, the activity of the scapular stabilizing muscles is relatively low to allow for scapular protraction.
Electromyographic analysis of the rotator cuff muscles exhibits contributions from the supraspinatus and infraspinatus in the trailing arm as they act to approximate and stabilize the shoulder (Jobe et al. 1986, Pink et al. 1990). Of the rotator cuff muscles in the leading arm, only the subscapularis was shown to display marked activity during the take-away phase. It should be noted that the pectoralis major, latissimus dorsi, and the deltoid muscles of both arms are relatively inactive in the backswing of the golf club (Jobe et al. 1986, Pink et al. 1990).
Forward Swing
During forward swing, trunk rotation movement is initiated. Analysis of the trailing arm scapular muscles shows that the three portions of the trapezius have lower activation to allow for scapular protraction (Kao et al. 1995). However, the levator scapulae and rhomboid muscles display marked activity to control scapular protraction and rotation of the trailing arm. Analysis of the serratus anterior muscle in the trailing arm shows increased activity during forward swing to aid in scapular protraction and stabilization (Kao et al. 1995). Electromyographic studies of the lead arm demonstrate high activity of the trapezius, levator scapulae, rhomboids, and serratus anterior as they all contribute to scapular motion and stabilization as the arms move toward the ball (Kao et al. 1995).
Of the trailing shoulder muscles during forward swing, the subscapularis, pectoralis major, and latissimus begin firing at marked levels as the trailing arm increasingly accelerates into the internal rotation and adduction. The lead arm subscapularis and latissimus dorsi are both moderately active during the forward swing phase.
Acceleration
During the acceleration phase, the body segments work together in a coordinated sequence in order to maximize club head speed at ball impact. The serratus anterior is the primary scapular stabilizer that is active in the trailing arm during acceleration (Kao et al. 1995). The serratus has high levels of involvement in order to allow for a strong scapular protraction and contribute to maximizing club head speed. Conversely, EMG analysis reveals strong contractions of the scapular muscles in the lead arm during acceleration (Kao et al. 1995). The trapezius, levator scapulae, and rhomboid muscles are firing to aid in scapular retraction, upward rotation, and elevation. The serratus anterior of the lead arm continues to display high levels of activation throughout. This important muscle is highly involved during the golf swing, similarly to what is seen during throwing and the tennis serve as discussed in earlier sections of this chapter.
Electromyographic investigations display high levels of subscapularis, pectoralis major, and latissimus dorsi activity to provide power to the trailing arm during acceleration (Jobe et al. 1986). These important muscles further increase in activity from forward swing to assist in rotation and forceful adduction of the arm during this phase. The latissimus dorsi contributes most of its power in the forward swing, while the pectoralis major supplies the most power during acceleration (Pink et al. 1990). Similarly, the subscapularis, pectoralis major, and latissimus dorsi of the lead arm fire at high rates during the acceleration phase (Jobe et al. 1986, Pink et al. 1990).
Early Follow-Through
After ball contact has been made, the follow-through phase is initiated. During early follow-through, nearly all the body segments work to decelerate their rotational contributions, often through eccentric muscle contractions (Jobe et al. 1986, Pink et al. 1993). The scapular muscles of both the trailing and lead arms display decreased activity throughout the follow-through phases, allowing for coordinated scapular protraction (Kao et al. 1995). Despite this decrease in scapular activity, the serratus anterior muscles of both arms show fairly consistent muscle firing patterns providing vital scapular stabilization throughout the follow-through phases (Kao et al. 1995).
In the trailing shoulder, marked activity of the subscapularis, pectoralis major, and latissimus dorsi muscles continues into the early follow-through phase (Jobe et al. 1986). For the lead shoulder, the subscapularis continues its high level of activity, while the pectoralis major and latissimus dorsi decrease their contributions (Jobe et al. 1986, Pink et al. 1990).
Late Follow-Through
Activity of the scapular muscles of both arms decreases to lower levels as the swing comes to an end (Kao et al. 1995). The subscapularis of the trailing shoulder is one of the only muscles that remains highly active during this phase (Jobe et al. 1986, Pink et al. 1990). Analysis of the lead arm reveals marked activity of the infraspinatus and the supraspinatus rotator cuff muscles used for glenohumeral stabilization (Pink et al. 1990).
One final discussion regarding the golf swing concerns a common mechanical fault that many golfers have, placing their glenohumeral joints at risk. During take-away, the lead arm is placed into increasing degrees of internal rotation and cross-body adduction. This position may predispose the golfer to impingement-type problems as the rotator cuff tendons and bursae are compressed within the shoulder (Mallon 1996). Additionally, at the end of the backswing, forces on the acromioclavicular joint of the lead arm are shown to be high, contributing to the incidence of pain often seen in the golfer's shoulder. The posterior rotator cuff and scapular muscles of the lead arm are also at risk for injury at the TOB as they are placed under a stretch load to achieve that position (Mallon 1996).
Save
Save
Save
Save
Learn more about Sport Therapy for the Shoulder.
Improve shoulder internal rotation range of motion for throwing athletes
Now that interpretation of glenohumeral joint ROM has been discussed, this section outlines specific techniques to increase IR ROM in the patient with shoulder dysfunction.
Methods to Improve Shoulder Internal Rotation (IR) Range of Motion (ROM) in the Throwing Athlete
Now that interpretation of glenohumeral joint ROM has been discussed, this section outlines specific techniques to increase IR ROM in the patient with shoulder dysfunction. This section, addressing the importance of accurate ROM measurement and clinical decision making based on the latest scientific evidence, can guide the clinician through the rehabilitation process; one can encounter a large spectrum of mobility issues when treating the patient with glenohumeral impingement. To further illustrate the role of ROM and passive stretching during this phase of the rehabilitation, figures 5.4 and 5.5 show versions of clinical IR stretching positions that use the scapular plane and that can be performed in multiple and varied positions of glenohumeral abduction. Each inherently possesses an anterior hand placement, used to exert varying degrees of posterior pressure to minimize scapular compensation and also to provide a checkrein against anterior humeral head translation during the IR stretch because of the effects of obligate translation.
Internal rotation range of motion technique in the scapular plane with 30° of elevation with scapular stabilization.
Internal rotation range of motion technique with scapular stabilization and 45° of glenohumeral joint elevation in the scapular plane. Note that the amount of elevation used with this stretch can be varied from as little as 0⁰ to 10⁰ all the way to 90⁰.
Research by Izumi and colleagues (2008) showed that large strains occurred in the posterior capsule in a stretching position of 30⁰ of elevation in the scapular plane with IR. These researchers compared many positions of shoulder ROM to determine what position optimally placed stress on the posterior capsule. The internally rotated position with the shoulder elevated 30⁰ in the scapular plane produced very acceptable levels of posterior capsular strain and would be highly effective for clinical use. These stretches for the posterior capsule and muscle - tendon unit (posterior shoulder stretches) can be used in a proprioceptive neuromuscular facilitation (PNF) contract - relax format following a low-load prolonged stretch-type paradigm to facilitate the increase in ROM (Sullivan et al. 1982, Zachezewski & Reischl 1986).
Save
Save
Save
Save
Save
Find more stretches to address IR ROM in Sport Therapy for the Shoulder.
Baseball and softball (throwing) program
The interval sport return program for baseball and softball (throwing) is designed to gradually return motion and strength to (and confidence in) the throwing arm after injury or surgery by slowly progressing through graduated throwing distances.
The interval sport return program for baseball and softball (throwing) is designed to gradually return motion and strength to (and confidence in) the throwing arm after injury or surgery by slowly progressing through graduated throwing distances. The program begins upon clearance by the athlete's physician to resume throwing and is performed under the supervision of the rehabilitation team (physician, physical therapist, and athletic trainer). The program is set up to minimize the chance of reinjury and emphasize prethrowing warm-up and stretching. In development of the interval throwing program (ITP), the following factors are considered most important:
- The act of throwing the baseball involves the transfer of energy from the feet through the legs, pelvis, and trunk and out the shoulder through the elbow and hand. Therefore, any return to throwing after injury must include attention to the entire body.
- The chance for reinjury is lessened by a graduated progression of interval throwing.
- Proper warm-up is essential.
- Most injuries occur as the result of fatigue.
- Proper throwing mechanics lessen the incidence of reinjury.
- Baseline requirements for throwing include these:
- Pain-free ROM
- Adequate muscle power
- Adequate muscle resistance to fatigue
Because of individual variability among throwing athletes, there is no set timetable for completion of the program. Most athletes, by nature, are highly competitive individuals and wish to return to competition at the earliest possible moment. While this is a necessary quality in all athletes, the proper channeling of the athlete's energies into a strictly controlled throwing program is essential to lessen the chance of reinjury during the rehabilitation process. The athlete may tend to want to increase the intensity of the throwing program. This will increase the incidence of reinjury and may greatly retard the rehabilitation process. The recommendation is to follow the program exactly, as this is the safest route to return to competition.
During the recovery process the athlete will probably experience soreness and a dull, diffuse aching sensation in the muscles and tendons. If the athlete experiences sharp pain, particularly in the joint, all throwing activity should be stopped until this pain ceases. If the pain continues, he should contact his physician.
Weight Training
The athlete should supplement the ITP with a high-repetition, low-weight exercise program. Strengthening should address a good balance between anterior and posterior musculature so that the shoulder will not be predisposed to injury. Special emphasis must be given to posterior rotator cuff musculature for any strengthening program. Weight training does not increase throwing velocity, but it increases the resistance of the arm to fatigue and injury. The athlete should do weight training on the same day as throwing but after the throwing has been completed; the day in between should be used for flexibility exercises and a recovery period. A weight training pattern or routine should be stressed at this point as a "maintenance program." This pattern can and should accompany the athlete into and throughout the season as a deterrent to further injury. It must be emphasized that weight training is of no benefit unless accompanied by a sound flexibility program.
Individual Variability
The ITP is designed so that each level is achieved without pain or complications before the next level is initiated. This sets up a progression in which the athlete achieves a goal before advancing, rather than advancing according to a specific time frame. Because of this design, the ITP may be used for different levels of skills and abilities compared to those characteristic of high school to professional levels. Progression will vary from person to person throughout the ITP. As an example, one athlete may wish to use alternate days throwing with or without using weights in between; another athlete may have to throw every third or fourth day due to pain or swelling. The athlete should be reminded to listen to her body, since pain signifies when it may be necessary to slow down. Again, completion of the steps of the ITP will vary from person to person. There is no set timetable with regard to days to completion.
Unlock the full program with Sport Therapy for the Shoulder.
What is happening in the shoulder complex during a golf swing?
Similar to the situation with the other sports reviewed in this chapter, to isolate and identify the functions of the major muscles controlling the various body segments during the golf swing, dynamic EMG and high-speed motion analysis has been used and helps to provide a greater understanding of the demands of golf on the shoulder complex.
Golf Swing Mechanics
Similar to the situation with the other sports reviewed in this chapter, to isolate and identify the functions of the major muscles controlling the various body segments during the golf swing, dynamic EMG and high-speed motion analysis has been used and helps to provide a greater understanding of the demands of golf on the shoulder complex. For discussion and analysis purposes, the golf swing has been broken down into the following five phases (Pink et al. 1993):
- Take-away: from address to the ball to the end of the backswing
- Forward swing: from the end of the backswing until the club is horizontal
- Acceleration: from horizontal position of the club to ball contact
- Early follow-through: from ball contact to horizontal club position
- Late follow-through: from horizontal club position to the end of the swing
|
|
|
Muscles used in three of the five phases of the golf swing: (a) take-away, (b) acceleration, and (c) follow-through.
This section describes and compares the muscle activity patterns of the primary shoulder and scapular muscles (but note that there are also significant contributions from other body segments during a golf swing).
Take-Away
Before initiation of the backswing, proper setup and ball address must be achieved. This initial posture greatly influences the balance of forces throughout the golf swing and is therefore critical to the achievement of the proper swing plane. The take-away phase has been described as a "coiling" or "loading" of the body in order to enhance the velocity and kinetic energy of the club head (Pink et al. 1990). Electromyographic analysis reveals relatively low activity of the trunk musculature during this segment of the golf swing, as the trunk is simply preparing for the swing (Pink et al. 1990). Electromyographic analysis of the scapular muscles of the trailing arm reveals relatively high activity of the upper, middle, and lower portions of the trapezius during take-away in order to help the scapula retract and upwardly rotate (Kao et al. 1995). Similarly, the levator scapulae and rhomboid muscle of the trailing arm are active during this period to help with such scapular movements (Kao et al. 1995). In the leading arm during take-away, the activity of the scapular stabilizing muscles is relatively low to allow for scapular protraction.
Electromyographic analysis of the rotator cuff muscles exhibits contributions from the supraspinatus and infraspinatus in the trailing arm as they act to approximate and stabilize the shoulder (Jobe et al. 1986, Pink et al. 1990). Of the rotator cuff muscles in the leading arm, only the subscapularis was shown to display marked activity during the take-away phase. It should be noted that the pectoralis major, latissimus dorsi, and the deltoid muscles of both arms are relatively inactive in the backswing of the golf club (Jobe et al. 1986, Pink et al. 1990).
Forward Swing
During forward swing, trunk rotation movement is initiated. Analysis of the trailing arm scapular muscles shows that the three portions of the trapezius have lower activation to allow for scapular protraction (Kao et al. 1995). However, the levator scapulae and rhomboid muscles display marked activity to control scapular protraction and rotation of the trailing arm. Analysis of the serratus anterior muscle in the trailing arm shows increased activity during forward swing to aid in scapular protraction and stabilization (Kao et al. 1995). Electromyographic studies of the lead arm demonstrate high activity of the trapezius, levator scapulae, rhomboids, and serratus anterior as they all contribute to scapular motion and stabilization as the arms move toward the ball (Kao et al. 1995).
Of the trailing shoulder muscles during forward swing, the subscapularis, pectoralis major, and latissimus begin firing at marked levels as the trailing arm increasingly accelerates into the internal rotation and adduction. The lead arm subscapularis and latissimus dorsi are both moderately active during the forward swing phase.
Acceleration
During the acceleration phase, the body segments work together in a coordinated sequence in order to maximize club head speed at ball impact. The serratus anterior is the primary scapular stabilizer that is active in the trailing arm during acceleration (Kao et al. 1995). The serratus has high levels of involvement in order to allow for a strong scapular protraction and contribute to maximizing club head speed. Conversely, EMG analysis reveals strong contractions of the scapular muscles in the lead arm during acceleration (Kao et al. 1995). The trapezius, levator scapulae, and rhomboid muscles are firing to aid in scapular retraction, upward rotation, and elevation. The serratus anterior of the lead arm continues to display high levels of activation throughout. This important muscle is highly involved during the golf swing, similarly to what is seen during throwing and the tennis serve as discussed in earlier sections of this chapter.
Electromyographic investigations display high levels of subscapularis, pectoralis major, and latissimus dorsi activity to provide power to the trailing arm during acceleration (Jobe et al. 1986). These important muscles further increase in activity from forward swing to assist in rotation and forceful adduction of the arm during this phase. The latissimus dorsi contributes most of its power in the forward swing, while the pectoralis major supplies the most power during acceleration (Pink et al. 1990). Similarly, the subscapularis, pectoralis major, and latissimus dorsi of the lead arm fire at high rates during the acceleration phase (Jobe et al. 1986, Pink et al. 1990).
Early Follow-Through
After ball contact has been made, the follow-through phase is initiated. During early follow-through, nearly all the body segments work to decelerate their rotational contributions, often through eccentric muscle contractions (Jobe et al. 1986, Pink et al. 1993). The scapular muscles of both the trailing and lead arms display decreased activity throughout the follow-through phases, allowing for coordinated scapular protraction (Kao et al. 1995). Despite this decrease in scapular activity, the serratus anterior muscles of both arms show fairly consistent muscle firing patterns providing vital scapular stabilization throughout the follow-through phases (Kao et al. 1995).
In the trailing shoulder, marked activity of the subscapularis, pectoralis major, and latissimus dorsi muscles continues into the early follow-through phase (Jobe et al. 1986). For the lead shoulder, the subscapularis continues its high level of activity, while the pectoralis major and latissimus dorsi decrease their contributions (Jobe et al. 1986, Pink et al. 1990).
Late Follow-Through
Activity of the scapular muscles of both arms decreases to lower levels as the swing comes to an end (Kao et al. 1995). The subscapularis of the trailing shoulder is one of the only muscles that remains highly active during this phase (Jobe et al. 1986, Pink et al. 1990). Analysis of the lead arm reveals marked activity of the infraspinatus and the supraspinatus rotator cuff muscles used for glenohumeral stabilization (Pink et al. 1990).
One final discussion regarding the golf swing concerns a common mechanical fault that many golfers have, placing their glenohumeral joints at risk. During take-away, the lead arm is placed into increasing degrees of internal rotation and cross-body adduction. This position may predispose the golfer to impingement-type problems as the rotator cuff tendons and bursae are compressed within the shoulder (Mallon 1996). Additionally, at the end of the backswing, forces on the acromioclavicular joint of the lead arm are shown to be high, contributing to the incidence of pain often seen in the golfer's shoulder. The posterior rotator cuff and scapular muscles of the lead arm are also at risk for injury at the TOB as they are placed under a stretch load to achieve that position (Mallon 1996).
Save
Save
Save
Save
Learn more about Sport Therapy for the Shoulder.
Improve shoulder internal rotation range of motion for throwing athletes
Now that interpretation of glenohumeral joint ROM has been discussed, this section outlines specific techniques to increase IR ROM in the patient with shoulder dysfunction.
Methods to Improve Shoulder Internal Rotation (IR) Range of Motion (ROM) in the Throwing Athlete
Now that interpretation of glenohumeral joint ROM has been discussed, this section outlines specific techniques to increase IR ROM in the patient with shoulder dysfunction. This section, addressing the importance of accurate ROM measurement and clinical decision making based on the latest scientific evidence, can guide the clinician through the rehabilitation process; one can encounter a large spectrum of mobility issues when treating the patient with glenohumeral impingement. To further illustrate the role of ROM and passive stretching during this phase of the rehabilitation, figures 5.4 and 5.5 show versions of clinical IR stretching positions that use the scapular plane and that can be performed in multiple and varied positions of glenohumeral abduction. Each inherently possesses an anterior hand placement, used to exert varying degrees of posterior pressure to minimize scapular compensation and also to provide a checkrein against anterior humeral head translation during the IR stretch because of the effects of obligate translation.
Internal rotation range of motion technique in the scapular plane with 30° of elevation with scapular stabilization.
Internal rotation range of motion technique with scapular stabilization and 45° of glenohumeral joint elevation in the scapular plane. Note that the amount of elevation used with this stretch can be varied from as little as 0⁰ to 10⁰ all the way to 90⁰.
Research by Izumi and colleagues (2008) showed that large strains occurred in the posterior capsule in a stretching position of 30⁰ of elevation in the scapular plane with IR. These researchers compared many positions of shoulder ROM to determine what position optimally placed stress on the posterior capsule. The internally rotated position with the shoulder elevated 30⁰ in the scapular plane produced very acceptable levels of posterior capsular strain and would be highly effective for clinical use. These stretches for the posterior capsule and muscle - tendon unit (posterior shoulder stretches) can be used in a proprioceptive neuromuscular facilitation (PNF) contract - relax format following a low-load prolonged stretch-type paradigm to facilitate the increase in ROM (Sullivan et al. 1982, Zachezewski & Reischl 1986).
Save
Save
Save
Save
Save
Find more stretches to address IR ROM in Sport Therapy for the Shoulder.
Baseball and softball (throwing) program
The interval sport return program for baseball and softball (throwing) is designed to gradually return motion and strength to (and confidence in) the throwing arm after injury or surgery by slowly progressing through graduated throwing distances.
The interval sport return program for baseball and softball (throwing) is designed to gradually return motion and strength to (and confidence in) the throwing arm after injury or surgery by slowly progressing through graduated throwing distances. The program begins upon clearance by the athlete's physician to resume throwing and is performed under the supervision of the rehabilitation team (physician, physical therapist, and athletic trainer). The program is set up to minimize the chance of reinjury and emphasize prethrowing warm-up and stretching. In development of the interval throwing program (ITP), the following factors are considered most important:
- The act of throwing the baseball involves the transfer of energy from the feet through the legs, pelvis, and trunk and out the shoulder through the elbow and hand. Therefore, any return to throwing after injury must include attention to the entire body.
- The chance for reinjury is lessened by a graduated progression of interval throwing.
- Proper warm-up is essential.
- Most injuries occur as the result of fatigue.
- Proper throwing mechanics lessen the incidence of reinjury.
- Baseline requirements for throwing include these:
- Pain-free ROM
- Adequate muscle power
- Adequate muscle resistance to fatigue
Because of individual variability among throwing athletes, there is no set timetable for completion of the program. Most athletes, by nature, are highly competitive individuals and wish to return to competition at the earliest possible moment. While this is a necessary quality in all athletes, the proper channeling of the athlete's energies into a strictly controlled throwing program is essential to lessen the chance of reinjury during the rehabilitation process. The athlete may tend to want to increase the intensity of the throwing program. This will increase the incidence of reinjury and may greatly retard the rehabilitation process. The recommendation is to follow the program exactly, as this is the safest route to return to competition.
During the recovery process the athlete will probably experience soreness and a dull, diffuse aching sensation in the muscles and tendons. If the athlete experiences sharp pain, particularly in the joint, all throwing activity should be stopped until this pain ceases. If the pain continues, he should contact his physician.
Weight Training
The athlete should supplement the ITP with a high-repetition, low-weight exercise program. Strengthening should address a good balance between anterior and posterior musculature so that the shoulder will not be predisposed to injury. Special emphasis must be given to posterior rotator cuff musculature for any strengthening program. Weight training does not increase throwing velocity, but it increases the resistance of the arm to fatigue and injury. The athlete should do weight training on the same day as throwing but after the throwing has been completed; the day in between should be used for flexibility exercises and a recovery period. A weight training pattern or routine should be stressed at this point as a "maintenance program." This pattern can and should accompany the athlete into and throughout the season as a deterrent to further injury. It must be emphasized that weight training is of no benefit unless accompanied by a sound flexibility program.
Individual Variability
The ITP is designed so that each level is achieved without pain or complications before the next level is initiated. This sets up a progression in which the athlete achieves a goal before advancing, rather than advancing according to a specific time frame. Because of this design, the ITP may be used for different levels of skills and abilities compared to those characteristic of high school to professional levels. Progression will vary from person to person throughout the ITP. As an example, one athlete may wish to use alternate days throwing with or without using weights in between; another athlete may have to throw every third or fourth day due to pain or swelling. The athlete should be reminded to listen to her body, since pain signifies when it may be necessary to slow down. Again, completion of the steps of the ITP will vary from person to person. There is no set timetable with regard to days to completion.
Unlock the full program with Sport Therapy for the Shoulder.
What is happening in the shoulder complex during a golf swing?
Similar to the situation with the other sports reviewed in this chapter, to isolate and identify the functions of the major muscles controlling the various body segments during the golf swing, dynamic EMG and high-speed motion analysis has been used and helps to provide a greater understanding of the demands of golf on the shoulder complex.
Golf Swing Mechanics
Similar to the situation with the other sports reviewed in this chapter, to isolate and identify the functions of the major muscles controlling the various body segments during the golf swing, dynamic EMG and high-speed motion analysis has been used and helps to provide a greater understanding of the demands of golf on the shoulder complex. For discussion and analysis purposes, the golf swing has been broken down into the following five phases (Pink et al. 1993):
- Take-away: from address to the ball to the end of the backswing
- Forward swing: from the end of the backswing until the club is horizontal
- Acceleration: from horizontal position of the club to ball contact
- Early follow-through: from ball contact to horizontal club position
- Late follow-through: from horizontal club position to the end of the swing
|
|
|
Muscles used in three of the five phases of the golf swing: (a) take-away, (b) acceleration, and (c) follow-through.
This section describes and compares the muscle activity patterns of the primary shoulder and scapular muscles (but note that there are also significant contributions from other body segments during a golf swing).
Take-Away
Before initiation of the backswing, proper setup and ball address must be achieved. This initial posture greatly influences the balance of forces throughout the golf swing and is therefore critical to the achievement of the proper swing plane. The take-away phase has been described as a "coiling" or "loading" of the body in order to enhance the velocity and kinetic energy of the club head (Pink et al. 1990). Electromyographic analysis reveals relatively low activity of the trunk musculature during this segment of the golf swing, as the trunk is simply preparing for the swing (Pink et al. 1990). Electromyographic analysis of the scapular muscles of the trailing arm reveals relatively high activity of the upper, middle, and lower portions of the trapezius during take-away in order to help the scapula retract and upwardly rotate (Kao et al. 1995). Similarly, the levator scapulae and rhomboid muscle of the trailing arm are active during this period to help with such scapular movements (Kao et al. 1995). In the leading arm during take-away, the activity of the scapular stabilizing muscles is relatively low to allow for scapular protraction.
Electromyographic analysis of the rotator cuff muscles exhibits contributions from the supraspinatus and infraspinatus in the trailing arm as they act to approximate and stabilize the shoulder (Jobe et al. 1986, Pink et al. 1990). Of the rotator cuff muscles in the leading arm, only the subscapularis was shown to display marked activity during the take-away phase. It should be noted that the pectoralis major, latissimus dorsi, and the deltoid muscles of both arms are relatively inactive in the backswing of the golf club (Jobe et al. 1986, Pink et al. 1990).
Forward Swing
During forward swing, trunk rotation movement is initiated. Analysis of the trailing arm scapular muscles shows that the three portions of the trapezius have lower activation to allow for scapular protraction (Kao et al. 1995). However, the levator scapulae and rhomboid muscles display marked activity to control scapular protraction and rotation of the trailing arm. Analysis of the serratus anterior muscle in the trailing arm shows increased activity during forward swing to aid in scapular protraction and stabilization (Kao et al. 1995). Electromyographic studies of the lead arm demonstrate high activity of the trapezius, levator scapulae, rhomboids, and serratus anterior as they all contribute to scapular motion and stabilization as the arms move toward the ball (Kao et al. 1995).
Of the trailing shoulder muscles during forward swing, the subscapularis, pectoralis major, and latissimus begin firing at marked levels as the trailing arm increasingly accelerates into the internal rotation and adduction. The lead arm subscapularis and latissimus dorsi are both moderately active during the forward swing phase.
Acceleration
During the acceleration phase, the body segments work together in a coordinated sequence in order to maximize club head speed at ball impact. The serratus anterior is the primary scapular stabilizer that is active in the trailing arm during acceleration (Kao et al. 1995). The serratus has high levels of involvement in order to allow for a strong scapular protraction and contribute to maximizing club head speed. Conversely, EMG analysis reveals strong contractions of the scapular muscles in the lead arm during acceleration (Kao et al. 1995). The trapezius, levator scapulae, and rhomboid muscles are firing to aid in scapular retraction, upward rotation, and elevation. The serratus anterior of the lead arm continues to display high levels of activation throughout. This important muscle is highly involved during the golf swing, similarly to what is seen during throwing and the tennis serve as discussed in earlier sections of this chapter.
Electromyographic investigations display high levels of subscapularis, pectoralis major, and latissimus dorsi activity to provide power to the trailing arm during acceleration (Jobe et al. 1986). These important muscles further increase in activity from forward swing to assist in rotation and forceful adduction of the arm during this phase. The latissimus dorsi contributes most of its power in the forward swing, while the pectoralis major supplies the most power during acceleration (Pink et al. 1990). Similarly, the subscapularis, pectoralis major, and latissimus dorsi of the lead arm fire at high rates during the acceleration phase (Jobe et al. 1986, Pink et al. 1990).
Early Follow-Through
After ball contact has been made, the follow-through phase is initiated. During early follow-through, nearly all the body segments work to decelerate their rotational contributions, often through eccentric muscle contractions (Jobe et al. 1986, Pink et al. 1993). The scapular muscles of both the trailing and lead arms display decreased activity throughout the follow-through phases, allowing for coordinated scapular protraction (Kao et al. 1995). Despite this decrease in scapular activity, the serratus anterior muscles of both arms show fairly consistent muscle firing patterns providing vital scapular stabilization throughout the follow-through phases (Kao et al. 1995).
In the trailing shoulder, marked activity of the subscapularis, pectoralis major, and latissimus dorsi muscles continues into the early follow-through phase (Jobe et al. 1986). For the lead shoulder, the subscapularis continues its high level of activity, while the pectoralis major and latissimus dorsi decrease their contributions (Jobe et al. 1986, Pink et al. 1990).
Late Follow-Through
Activity of the scapular muscles of both arms decreases to lower levels as the swing comes to an end (Kao et al. 1995). The subscapularis of the trailing shoulder is one of the only muscles that remains highly active during this phase (Jobe et al. 1986, Pink et al. 1990). Analysis of the lead arm reveals marked activity of the infraspinatus and the supraspinatus rotator cuff muscles used for glenohumeral stabilization (Pink et al. 1990).
One final discussion regarding the golf swing concerns a common mechanical fault that many golfers have, placing their glenohumeral joints at risk. During take-away, the lead arm is placed into increasing degrees of internal rotation and cross-body adduction. This position may predispose the golfer to impingement-type problems as the rotator cuff tendons and bursae are compressed within the shoulder (Mallon 1996). Additionally, at the end of the backswing, forces on the acromioclavicular joint of the lead arm are shown to be high, contributing to the incidence of pain often seen in the golfer's shoulder. The posterior rotator cuff and scapular muscles of the lead arm are also at risk for injury at the TOB as they are placed under a stretch load to achieve that position (Mallon 1996).
Save
Save
Save
Save
Learn more about Sport Therapy for the Shoulder.
Improve shoulder internal rotation range of motion for throwing athletes
Now that interpretation of glenohumeral joint ROM has been discussed, this section outlines specific techniques to increase IR ROM in the patient with shoulder dysfunction.
Methods to Improve Shoulder Internal Rotation (IR) Range of Motion (ROM) in the Throwing Athlete
Now that interpretation of glenohumeral joint ROM has been discussed, this section outlines specific techniques to increase IR ROM in the patient with shoulder dysfunction. This section, addressing the importance of accurate ROM measurement and clinical decision making based on the latest scientific evidence, can guide the clinician through the rehabilitation process; one can encounter a large spectrum of mobility issues when treating the patient with glenohumeral impingement. To further illustrate the role of ROM and passive stretching during this phase of the rehabilitation, figures 5.4 and 5.5 show versions of clinical IR stretching positions that use the scapular plane and that can be performed in multiple and varied positions of glenohumeral abduction. Each inherently possesses an anterior hand placement, used to exert varying degrees of posterior pressure to minimize scapular compensation and also to provide a checkrein against anterior humeral head translation during the IR stretch because of the effects of obligate translation.
Internal rotation range of motion technique in the scapular plane with 30° of elevation with scapular stabilization.
Internal rotation range of motion technique with scapular stabilization and 45° of glenohumeral joint elevation in the scapular plane. Note that the amount of elevation used with this stretch can be varied from as little as 0⁰ to 10⁰ all the way to 90⁰.
Research by Izumi and colleagues (2008) showed that large strains occurred in the posterior capsule in a stretching position of 30⁰ of elevation in the scapular plane with IR. These researchers compared many positions of shoulder ROM to determine what position optimally placed stress on the posterior capsule. The internally rotated position with the shoulder elevated 30⁰ in the scapular plane produced very acceptable levels of posterior capsular strain and would be highly effective for clinical use. These stretches for the posterior capsule and muscle - tendon unit (posterior shoulder stretches) can be used in a proprioceptive neuromuscular facilitation (PNF) contract - relax format following a low-load prolonged stretch-type paradigm to facilitate the increase in ROM (Sullivan et al. 1982, Zachezewski & Reischl 1986).
Save
Save
Save
Save
Save
Find more stretches to address IR ROM in Sport Therapy for the Shoulder.
Baseball and softball (throwing) program
The interval sport return program for baseball and softball (throwing) is designed to gradually return motion and strength to (and confidence in) the throwing arm after injury or surgery by slowly progressing through graduated throwing distances.
The interval sport return program for baseball and softball (throwing) is designed to gradually return motion and strength to (and confidence in) the throwing arm after injury or surgery by slowly progressing through graduated throwing distances. The program begins upon clearance by the athlete's physician to resume throwing and is performed under the supervision of the rehabilitation team (physician, physical therapist, and athletic trainer). The program is set up to minimize the chance of reinjury and emphasize prethrowing warm-up and stretching. In development of the interval throwing program (ITP), the following factors are considered most important:
- The act of throwing the baseball involves the transfer of energy from the feet through the legs, pelvis, and trunk and out the shoulder through the elbow and hand. Therefore, any return to throwing after injury must include attention to the entire body.
- The chance for reinjury is lessened by a graduated progression of interval throwing.
- Proper warm-up is essential.
- Most injuries occur as the result of fatigue.
- Proper throwing mechanics lessen the incidence of reinjury.
- Baseline requirements for throwing include these:
- Pain-free ROM
- Adequate muscle power
- Adequate muscle resistance to fatigue
Because of individual variability among throwing athletes, there is no set timetable for completion of the program. Most athletes, by nature, are highly competitive individuals and wish to return to competition at the earliest possible moment. While this is a necessary quality in all athletes, the proper channeling of the athlete's energies into a strictly controlled throwing program is essential to lessen the chance of reinjury during the rehabilitation process. The athlete may tend to want to increase the intensity of the throwing program. This will increase the incidence of reinjury and may greatly retard the rehabilitation process. The recommendation is to follow the program exactly, as this is the safest route to return to competition.
During the recovery process the athlete will probably experience soreness and a dull, diffuse aching sensation in the muscles and tendons. If the athlete experiences sharp pain, particularly in the joint, all throwing activity should be stopped until this pain ceases. If the pain continues, he should contact his physician.
Weight Training
The athlete should supplement the ITP with a high-repetition, low-weight exercise program. Strengthening should address a good balance between anterior and posterior musculature so that the shoulder will not be predisposed to injury. Special emphasis must be given to posterior rotator cuff musculature for any strengthening program. Weight training does not increase throwing velocity, but it increases the resistance of the arm to fatigue and injury. The athlete should do weight training on the same day as throwing but after the throwing has been completed; the day in between should be used for flexibility exercises and a recovery period. A weight training pattern or routine should be stressed at this point as a "maintenance program." This pattern can and should accompany the athlete into and throughout the season as a deterrent to further injury. It must be emphasized that weight training is of no benefit unless accompanied by a sound flexibility program.
Individual Variability
The ITP is designed so that each level is achieved without pain or complications before the next level is initiated. This sets up a progression in which the athlete achieves a goal before advancing, rather than advancing according to a specific time frame. Because of this design, the ITP may be used for different levels of skills and abilities compared to those characteristic of high school to professional levels. Progression will vary from person to person throughout the ITP. As an example, one athlete may wish to use alternate days throwing with or without using weights in between; another athlete may have to throw every third or fourth day due to pain or swelling. The athlete should be reminded to listen to her body, since pain signifies when it may be necessary to slow down. Again, completion of the steps of the ITP will vary from person to person. There is no set timetable with regard to days to completion.
Unlock the full program with Sport Therapy for the Shoulder.
What is happening in the shoulder complex during a golf swing?
Similar to the situation with the other sports reviewed in this chapter, to isolate and identify the functions of the major muscles controlling the various body segments during the golf swing, dynamic EMG and high-speed motion analysis has been used and helps to provide a greater understanding of the demands of golf on the shoulder complex.
Golf Swing Mechanics
Similar to the situation with the other sports reviewed in this chapter, to isolate and identify the functions of the major muscles controlling the various body segments during the golf swing, dynamic EMG and high-speed motion analysis has been used and helps to provide a greater understanding of the demands of golf on the shoulder complex. For discussion and analysis purposes, the golf swing has been broken down into the following five phases (Pink et al. 1993):
- Take-away: from address to the ball to the end of the backswing
- Forward swing: from the end of the backswing until the club is horizontal
- Acceleration: from horizontal position of the club to ball contact
- Early follow-through: from ball contact to horizontal club position
- Late follow-through: from horizontal club position to the end of the swing
|
|
|
Muscles used in three of the five phases of the golf swing: (a) take-away, (b) acceleration, and (c) follow-through.
This section describes and compares the muscle activity patterns of the primary shoulder and scapular muscles (but note that there are also significant contributions from other body segments during a golf swing).
Take-Away
Before initiation of the backswing, proper setup and ball address must be achieved. This initial posture greatly influences the balance of forces throughout the golf swing and is therefore critical to the achievement of the proper swing plane. The take-away phase has been described as a "coiling" or "loading" of the body in order to enhance the velocity and kinetic energy of the club head (Pink et al. 1990). Electromyographic analysis reveals relatively low activity of the trunk musculature during this segment of the golf swing, as the trunk is simply preparing for the swing (Pink et al. 1990). Electromyographic analysis of the scapular muscles of the trailing arm reveals relatively high activity of the upper, middle, and lower portions of the trapezius during take-away in order to help the scapula retract and upwardly rotate (Kao et al. 1995). Similarly, the levator scapulae and rhomboid muscle of the trailing arm are active during this period to help with such scapular movements (Kao et al. 1995). In the leading arm during take-away, the activity of the scapular stabilizing muscles is relatively low to allow for scapular protraction.
Electromyographic analysis of the rotator cuff muscles exhibits contributions from the supraspinatus and infraspinatus in the trailing arm as they act to approximate and stabilize the shoulder (Jobe et al. 1986, Pink et al. 1990). Of the rotator cuff muscles in the leading arm, only the subscapularis was shown to display marked activity during the take-away phase. It should be noted that the pectoralis major, latissimus dorsi, and the deltoid muscles of both arms are relatively inactive in the backswing of the golf club (Jobe et al. 1986, Pink et al. 1990).
Forward Swing
During forward swing, trunk rotation movement is initiated. Analysis of the trailing arm scapular muscles shows that the three portions of the trapezius have lower activation to allow for scapular protraction (Kao et al. 1995). However, the levator scapulae and rhomboid muscles display marked activity to control scapular protraction and rotation of the trailing arm. Analysis of the serratus anterior muscle in the trailing arm shows increased activity during forward swing to aid in scapular protraction and stabilization (Kao et al. 1995). Electromyographic studies of the lead arm demonstrate high activity of the trapezius, levator scapulae, rhomboids, and serratus anterior as they all contribute to scapular motion and stabilization as the arms move toward the ball (Kao et al. 1995).
Of the trailing shoulder muscles during forward swing, the subscapularis, pectoralis major, and latissimus begin firing at marked levels as the trailing arm increasingly accelerates into the internal rotation and adduction. The lead arm subscapularis and latissimus dorsi are both moderately active during the forward swing phase.
Acceleration
During the acceleration phase, the body segments work together in a coordinated sequence in order to maximize club head speed at ball impact. The serratus anterior is the primary scapular stabilizer that is active in the trailing arm during acceleration (Kao et al. 1995). The serratus has high levels of involvement in order to allow for a strong scapular protraction and contribute to maximizing club head speed. Conversely, EMG analysis reveals strong contractions of the scapular muscles in the lead arm during acceleration (Kao et al. 1995). The trapezius, levator scapulae, and rhomboid muscles are firing to aid in scapular retraction, upward rotation, and elevation. The serratus anterior of the lead arm continues to display high levels of activation throughout. This important muscle is highly involved during the golf swing, similarly to what is seen during throwing and the tennis serve as discussed in earlier sections of this chapter.
Electromyographic investigations display high levels of subscapularis, pectoralis major, and latissimus dorsi activity to provide power to the trailing arm during acceleration (Jobe et al. 1986). These important muscles further increase in activity from forward swing to assist in rotation and forceful adduction of the arm during this phase. The latissimus dorsi contributes most of its power in the forward swing, while the pectoralis major supplies the most power during acceleration (Pink et al. 1990). Similarly, the subscapularis, pectoralis major, and latissimus dorsi of the lead arm fire at high rates during the acceleration phase (Jobe et al. 1986, Pink et al. 1990).
Early Follow-Through
After ball contact has been made, the follow-through phase is initiated. During early follow-through, nearly all the body segments work to decelerate their rotational contributions, often through eccentric muscle contractions (Jobe et al. 1986, Pink et al. 1993). The scapular muscles of both the trailing and lead arms display decreased activity throughout the follow-through phases, allowing for coordinated scapular protraction (Kao et al. 1995). Despite this decrease in scapular activity, the serratus anterior muscles of both arms show fairly consistent muscle firing patterns providing vital scapular stabilization throughout the follow-through phases (Kao et al. 1995).
In the trailing shoulder, marked activity of the subscapularis, pectoralis major, and latissimus dorsi muscles continues into the early follow-through phase (Jobe et al. 1986). For the lead shoulder, the subscapularis continues its high level of activity, while the pectoralis major and latissimus dorsi decrease their contributions (Jobe et al. 1986, Pink et al. 1990).
Late Follow-Through
Activity of the scapular muscles of both arms decreases to lower levels as the swing comes to an end (Kao et al. 1995). The subscapularis of the trailing shoulder is one of the only muscles that remains highly active during this phase (Jobe et al. 1986, Pink et al. 1990). Analysis of the lead arm reveals marked activity of the infraspinatus and the supraspinatus rotator cuff muscles used for glenohumeral stabilization (Pink et al. 1990).
One final discussion regarding the golf swing concerns a common mechanical fault that many golfers have, placing their glenohumeral joints at risk. During take-away, the lead arm is placed into increasing degrees of internal rotation and cross-body adduction. This position may predispose the golfer to impingement-type problems as the rotator cuff tendons and bursae are compressed within the shoulder (Mallon 1996). Additionally, at the end of the backswing, forces on the acromioclavicular joint of the lead arm are shown to be high, contributing to the incidence of pain often seen in the golfer's shoulder. The posterior rotator cuff and scapular muscles of the lead arm are also at risk for injury at the TOB as they are placed under a stretch load to achieve that position (Mallon 1996).
Save
Save
Save
Save
Learn more about Sport Therapy for the Shoulder.
Improve shoulder internal rotation range of motion for throwing athletes
Now that interpretation of glenohumeral joint ROM has been discussed, this section outlines specific techniques to increase IR ROM in the patient with shoulder dysfunction.
Methods to Improve Shoulder Internal Rotation (IR) Range of Motion (ROM) in the Throwing Athlete
Now that interpretation of glenohumeral joint ROM has been discussed, this section outlines specific techniques to increase IR ROM in the patient with shoulder dysfunction. This section, addressing the importance of accurate ROM measurement and clinical decision making based on the latest scientific evidence, can guide the clinician through the rehabilitation process; one can encounter a large spectrum of mobility issues when treating the patient with glenohumeral impingement. To further illustrate the role of ROM and passive stretching during this phase of the rehabilitation, figures 5.4 and 5.5 show versions of clinical IR stretching positions that use the scapular plane and that can be performed in multiple and varied positions of glenohumeral abduction. Each inherently possesses an anterior hand placement, used to exert varying degrees of posterior pressure to minimize scapular compensation and also to provide a checkrein against anterior humeral head translation during the IR stretch because of the effects of obligate translation.
Internal rotation range of motion technique in the scapular plane with 30° of elevation with scapular stabilization.
Internal rotation range of motion technique with scapular stabilization and 45° of glenohumeral joint elevation in the scapular plane. Note that the amount of elevation used with this stretch can be varied from as little as 0⁰ to 10⁰ all the way to 90⁰.
Research by Izumi and colleagues (2008) showed that large strains occurred in the posterior capsule in a stretching position of 30⁰ of elevation in the scapular plane with IR. These researchers compared many positions of shoulder ROM to determine what position optimally placed stress on the posterior capsule. The internally rotated position with the shoulder elevated 30⁰ in the scapular plane produced very acceptable levels of posterior capsular strain and would be highly effective for clinical use. These stretches for the posterior capsule and muscle - tendon unit (posterior shoulder stretches) can be used in a proprioceptive neuromuscular facilitation (PNF) contract - relax format following a low-load prolonged stretch-type paradigm to facilitate the increase in ROM (Sullivan et al. 1982, Zachezewski & Reischl 1986).
Save
Save
Save
Save
Save
Find more stretches to address IR ROM in Sport Therapy for the Shoulder.
Baseball and softball (throwing) program
The interval sport return program for baseball and softball (throwing) is designed to gradually return motion and strength to (and confidence in) the throwing arm after injury or surgery by slowly progressing through graduated throwing distances.
The interval sport return program for baseball and softball (throwing) is designed to gradually return motion and strength to (and confidence in) the throwing arm after injury or surgery by slowly progressing through graduated throwing distances. The program begins upon clearance by the athlete's physician to resume throwing and is performed under the supervision of the rehabilitation team (physician, physical therapist, and athletic trainer). The program is set up to minimize the chance of reinjury and emphasize prethrowing warm-up and stretching. In development of the interval throwing program (ITP), the following factors are considered most important:
- The act of throwing the baseball involves the transfer of energy from the feet through the legs, pelvis, and trunk and out the shoulder through the elbow and hand. Therefore, any return to throwing after injury must include attention to the entire body.
- The chance for reinjury is lessened by a graduated progression of interval throwing.
- Proper warm-up is essential.
- Most injuries occur as the result of fatigue.
- Proper throwing mechanics lessen the incidence of reinjury.
- Baseline requirements for throwing include these:
- Pain-free ROM
- Adequate muscle power
- Adequate muscle resistance to fatigue
Because of individual variability among throwing athletes, there is no set timetable for completion of the program. Most athletes, by nature, are highly competitive individuals and wish to return to competition at the earliest possible moment. While this is a necessary quality in all athletes, the proper channeling of the athlete's energies into a strictly controlled throwing program is essential to lessen the chance of reinjury during the rehabilitation process. The athlete may tend to want to increase the intensity of the throwing program. This will increase the incidence of reinjury and may greatly retard the rehabilitation process. The recommendation is to follow the program exactly, as this is the safest route to return to competition.
During the recovery process the athlete will probably experience soreness and a dull, diffuse aching sensation in the muscles and tendons. If the athlete experiences sharp pain, particularly in the joint, all throwing activity should be stopped until this pain ceases. If the pain continues, he should contact his physician.
Weight Training
The athlete should supplement the ITP with a high-repetition, low-weight exercise program. Strengthening should address a good balance between anterior and posterior musculature so that the shoulder will not be predisposed to injury. Special emphasis must be given to posterior rotator cuff musculature for any strengthening program. Weight training does not increase throwing velocity, but it increases the resistance of the arm to fatigue and injury. The athlete should do weight training on the same day as throwing but after the throwing has been completed; the day in between should be used for flexibility exercises and a recovery period. A weight training pattern or routine should be stressed at this point as a "maintenance program." This pattern can and should accompany the athlete into and throughout the season as a deterrent to further injury. It must be emphasized that weight training is of no benefit unless accompanied by a sound flexibility program.
Individual Variability
The ITP is designed so that each level is achieved without pain or complications before the next level is initiated. This sets up a progression in which the athlete achieves a goal before advancing, rather than advancing according to a specific time frame. Because of this design, the ITP may be used for different levels of skills and abilities compared to those characteristic of high school to professional levels. Progression will vary from person to person throughout the ITP. As an example, one athlete may wish to use alternate days throwing with or without using weights in between; another athlete may have to throw every third or fourth day due to pain or swelling. The athlete should be reminded to listen to her body, since pain signifies when it may be necessary to slow down. Again, completion of the steps of the ITP will vary from person to person. There is no set timetable with regard to days to completion.
Unlock the full program with Sport Therapy for the Shoulder.
Related Books