

Sedentary Behavior and Health
Concepts, Assessments, and Interventions
by Weimo Zhu
Edited by Neville Owen
456 Pages
From office jobs and long commutes to passive entertainment like television and video games, humans are sitting more than ever. Though lack of exercise has major health consequences, researchers are now examining the additional and widespread health risk of the simple act of sitting for extended periods. With research from leading scientists, Sedentary Behavior and Health: Concepts, Assessments, and Interventions presents evidence on sedentary behavior, its apparent health risks, and suggestions on measuring and altering this behavior.
The highly respected international author team provides an interdisciplinary review of current research, examining scientific, public health, and broader social questions about the implications of sedentary behavior. These topics include humans’ physiological predispositions, exacerbation of current health conditions like obesity and diabetes, and the design and ergonomics of offices and chairs.
To examine the many facets of this developing area of study, Sedentary Behavior and Health is divided into five parts:
• “Sedentary Behavior Concepts and Context” reviews the physiology of sedentary behavior, investigating current habits from the perspectives of evolution, industrial engineering, and design.
• “Sedentary Behavior and Health” explores the relationship between sedentary behavior and several major chronic diseases, including obesity, cardiovascular disease, and low-back pain.
• “Measuring and Analyzing Sedentary Behavior” explains research methods for understanding and measuring sedentary behavior in order to recognize patterns and design interventions.
• “Sedentary Behavior and Subpopulations” covers issues, risks, and behaviors in groups such as children, working adults, older adults, and minorities.
• “Changing Sedentary Behavior” provides methods and recommendations for improvement with environmental, social, community, worksite, and technology-based interventions.
Included in this groundbreaking text are learning objectives, key concepts, and study questions to focus attention on key issues and reinforce concepts. Reviews of the literature in the field are presented, many with comparisons in table form, to provide the full scope of research. Sidebars throughout the text apply theoretical concepts to real-world scenarios.
Inactivity is mismatched with many aspects of humans’ genetic makeup. While it is becoming the new norm, the consequences of this behavior are emerging as a public health threat. Sedentary Behavior and Health will serve as a key reference for the rapidly emerging research area of sedentary behavior.
Part I. Sedentary Behavior Concepts and Context
Chapter 1. Emergence of Research on Sedentary Behavior and Health
Neville Owen
Contemporary Sedentary Behavior Research and Concepts
Sedentary Behavior and Health
Sedentary Research Agenda
Sedentary Behavior Research Priorities
Summary
Chapter 2. Gravity, Sitting, and Health
Joan Vernikos
Gravity and Spaceflight
Head Down Bed Rest Studies
Gravity Deprivation Syndrome
Health Consequences of Prolonged Sitting and Gravity
Perceiving Gravity
Gravity Intervention Design and Implementation
Summary
Chapter 3. Physiological Effects of Reducing and Breaking Up Sitting Time
David W. Dunstan, Bethany J. Howard, Audrey Bergouignan, Bronwyn A. Kingwell, and Neville Owen
Methodological Considerations for Studies of Sedentary Behavior
Metabolic Effects of Reduced Sitting and the Postprandial State
Cardio Metabolic Effects Following Exposure to Reduced Sitting
Cardiometabolic Effects of Repeated-Day Exposure to Reduced Sitting
Public Health and Clinical Guidelines
Summary
Chapter 4. Rethinking the Chair and Sitting
Galen Cranz
Problems with Sitting in Chairs
Chair Designer Response
Postural Education
Summary
Chapter 5. Children and Screen Time
Jorge A. Banda and Thomas N. Robinson
Screen Time Exposure
Mobile Devices and Screen Time Changes
Influences on Media Use
Screen Time and Body Weight
Screen Time and Cardiometabolic Risk Factors
Screen Time, Physical Activity, and Cardiorespiratory Fitness
Screen Time and Dietary Habits
Experimental Studies of Reducing Screen Time
Summary
Part II. Sedentary Behavior and Health
Chapter 6. Economics of Sedentary Occupations
Kenneth A. Glover
Economic Sectors
Economics of Inactivity
Worksite Health Promotion
Regulation and Innovation
Choice Architecture
Summary
Chapter 7. Sedentary Behavior and Obesity
Michael L. Power
Role of Fat
Adipose Tissue and Endocrine Function
Mismatch Paradigm
Obesity and Inflammation
Central Versus Peripheral Obesity
Sex Differences in Fat Storage and Mobilization
Vitamin D, Adipose Tissue, and Sedentary Behavior
Obesity Prevalence
Summary
Chapter 8. Sedentary Behavior and Incident Diabetes
Carl J. Caspersen and G. Darlene Thomas
Diabetes Statistics
Key Risk Factors
Epidemiological Diabetes Research
Research Limitations
Six Criteria to Assess a Causal Inference for Sedentary Behavior and Diabetes
Summary
Chapter 9. Sedentary Behavior and Cardiovascular Disease
Edward Archer, Enrique G. Artero, and Steven N. Blair
Cardiovascular Diseases
Occupational Physical Activity and CVD
Physical Activity and CVD
Summary
Chapter 10. Sedentary Behavior and Cancer
Brigid M. Lynch and Christine M. Friedenreich
Cancer Epidemiology
Key Risk Factors
Sedentary Behavior and Cancer Research
Sedentary Behavior and Cancer Survivorship
Proposed Biological Mechanisms
Summary
Chapter 11. Sedentary Behavior and Low Back Pain
Marco S. Boscolo and Weimo Zhu
Low Back Pain and Its Impact
Spine Anatomy
Spine Stability
Known Risk Factors of Low Back Pain
Relationship Between Low Back Pain and Sedentary Behavior
Prevention of Low Back Pain
Summary
Chapter 12. Sedentary behavior and psychological well-being
Stuart J.H. Biddle and Stephan Bandelow
Sedentary Behavior and Depression
Sedentary Behavior and Cognitive Functioning
Sedentary Behavior and Health-Related Quality of Life
Summary
Part III. Measuring and Analyzing Sedentary Behavior
Chapter 13. Assessing Sedentary Behavior Using Questionnaires
Barbara E. Ainsworth, Alberto Flórez Pregonero, and Fabien Rivière
Key Components of Questionnaires
Measurement Principles of Questionnaires
Practical Guidelines
Summary
Chapter 14. Assessing Sedentary Behavior Using Motion Sensors
Kong Y. Chen and Richard P. Troiano
Key Components of Motion Sensors
Measurement Principles of Motion Transducers
Accelerometers
Practical Guidelines
Potential of Raw Accelerometer Data
Summary
Chapter 15. Assessing Sedentary Behavior Using Physiological Sensors
David Bassett and Dinesh John
Key Components of Physiological Sensors
Measurement Principles of Physiological Sensors
Practical Guidelines
Summary
Chapter 16. Assessing Sedentary Behavior Using New Technology
Dinesh John and Stephen Intille
Existing Technology for Measuring Sedentary Behavior
Sedentary Behavior Measurement Goals
Improvements and Emerging Technology for Measuring Sedentary Behavior
Data Collection, Storage, and Open Source Processing
Summary
Chapter 17. Critical Measurement and Research Issues in Analyzing Sedentary Behavior
Weimo Zhu
Sedentary Behavior Data Characteristics
Challenges and Solutions in the Analysis of Sedentary Behavior Data
Summary
Part IV. Sedentary Behavior and Subpopulations
Chapter 18. Sedentary Behavior in Children
Gregory J. Welk and Youngwon Kim
Measures of Sedentary Behavior in Youth
Health Effects of Sedentary Behavior in Youth
Epidemiology of Sedentary Behavior in Youth
Differences in Sedentary Behavior by Age and Gender
Social and Cultural Differences in Sedentary Behavior in Youth
Correlates of Youth Sedentary Behavior
Patterns of Youth Physical Activity and Sedentary Behavior
Intervention Approaches for Sedentary Behavior in Youth
Summary
Chapter 19. Occupational Sedentary Behavior in Adults
Wendy J. Brown
Most Sedentary Occupations
Characteristics of Sitting at Work
Health Effects of Occupational Sitting
Changing Sitting at Work to Improve Health Outcomes
Summary
Chapter 20. Sedentary Behavior of Older Adults
Jorge A. Banda, Sandra J. Winter, and Abby C. King
Measuring Sedentary Behavior in Older Adults
Health and Functional Outcomes of Sedentary Behavior
Putative Drivers of Sedentary Behavior
Possible Contexts of Sedentary Behavior
Interventions Aimed at Reducing Sedentary Behavior
Summary
Chapter 21. Sedentary Behavior in Racial/Ethnic Minority Groups
Melicia C. Whitt-Glover and Tyrone G. Ceaser
Statistics
Correlates of Sedentary Behavior
Interventions to Reduce Sedentary Behavior in Racial/Ethnic Minorities
Summary
Part V. Changing Sedentary Behavior
Chapter 22. Psychological and Behavior-Based Interventions
Kevin Moran and John P. Elder
Theories of Reasoned Action and Planned Behavior
Social Cognitive Theory
Health Belief Model
Transtheoretical Model
Operant Conditioning, Contingency Management and Positivistic Models
Socioecological Models
Summary
Chapter 23. Environment and Policy Interventions
Jordan A. Carlson and James F. Sallis
Comprehensive Multi-Level Approaches
Evaluating Environment and Policy Interventions
Integrating Environment and Policy Interventions with Other Approaches
Practical Guidelines
Summary
Chapter 24. Sedentary Behavior and Worksite Interventions
Nicolaas P. Pronk
Characteristics of Worksite Interventions
Applications of Worksite Interventions
Practical Guidelines
Summary
Chapter 25. Community Based Interventions
Adrian Bauman and Josephine Y. Chau
Framework for Assessing Sedentary Behavior-Reducing Interventions
Evaluating Community-Based Interventions
Practical Guidelines
Summary
Chapter 26. Ergonomics of Redesigning Sitting
John B. Shea
Characteristics and Impact of Chair Designs and Positional Behaviors
Applications of Sitting Redesign
Practical Guidelines
Summary
Chapter 27. Emerging Communication Systems to Curb Physical Inactivity
Dolores Albarracin, Vera Liao, Jessica Yi, and Cheng Zhai
Determinants of Exposure and Attitude
Determinants of Attitude and Behavior Change
Information Systems
Summary
Weimo Zhu, PhD, is currently a tenured full professor in the department of kinesiology and community health at the University of Illinois at Urbana-Champaign. His major area of research is in kinesmetrics (i.e., measurement and evaluation in kinesiology).
Dr. Zhu’s primary research interests are the study and application of new measurement theories (e.g., item response theory) and models to the field of kinesiology. His research works have earned him international recognition. He is the editor in chief of the Research Quarterly for Exercise and Sport and a fellow of the American Academy of Kinesiology, American College of Sports Medicine, and Research Consortium of SHAPE America. He is a member of the Fitnessgram/Activitygram Advisory Committee. He is also a member of the editorial board for various academic journals and serves on the executive committees of several national and international professional organizations. Dr. Zhu was the chair of the Measurement and Evaluation Council of SHAPE America. Currently, Dr. Zhu is examining the application of advanced measurement and statistical techniques to several measurement issues in public health. A practical application of Zhu’s theoretical work has been in the assessment of physical activity and sedentary behavior, and he is exploring a new idea and technologies to solve the problems raised.
Neville Owen, PhD, is head of the Behavioural Epidemiology Laboratory at the Baker IDI Heart and Diabetes Institute, a National Health and Medical Research Council of Australia (NHMRC) senior principal research fellow, adjunct professor in the School of Public Health at the University of Queensland, honorary professorial fellow in the School of Population and Global Health at the University of Melbourne, and adjunct professor in medicine at Monash University. He was foundation professor of Human Movement Science and inaugural head of the School of Human Movement at Deakin University (1995-99) and director of the Cancer Prevention Research Centre at the University of Queensland (2002-11). His research deals with the prevention and management of diabetes, heart disease, and cancer through identifying health consequences, environmental determinants, and behavior-change strategies for physical inactivity and sedentary behavior.
Owen has published more than 450 peer-reviewed papers and the book Physical Activity and Behavioral Medicine with James F Sallis. Thomson Reuters (2015) identified him as a highly cited researcher and among the world’s most influential minds in the social sciences. He has been supported by grants from the NHMRC since 1992, including two grants for five-year programs (Physical Activity and Public Health; Sitting Less and Moving More: Population Health Research to Understand and Influence Sedentary Behaviour) and a grant from Centres of Research Excellence (Sitting Time and Chronic Disease Prevention: Measurement, Mechanisms and Interventions).
Sedentary Behavior and Depression
Teychenne, Ball, and Salmon (2008) conducted a systematic review on depression and sedentary behavior in adults. Seven observational (5 cross-sectional and 2 longitudinal) and four intervention studies were included.
Teychenne, Ball, and Salmon (2008) conducted a systematic review on depression and sedentary behavior in adults. Seven observational (5 cross-sectional and 2 longitudinal) and four intervention studies were included. Of the observational studies, 6 of 7 showed a positive association between sedentary behavior and depression; that is, higher sedentary behavior was associated with greater depression. The other study also showed this for time spent surfing the Internet, but reported negative associations for depression with hours spent e-mailing and using chat rooms. This suggests that the type of sedentary behavior may be an important moderator of any association between sedentary behavior and depression. More is said on this subject later in the chapter.
The four intervention studies reviewed by Teychenne et al. (2008) showed mixed results: one study showed no effect and one showed an increase in depression after the introduction of free computer and Internet use, while two showed that the risk of depression was reduced during the intervention. One provided extra computer and Internet use while the other used extra chat sessions. The latter may have boosted well-being through social interaction. It is important to note that the authors of the review concluded that at the time, no interventions had attempted to reduce sedentary behavior in an effort to assess changes in depression.
Since the review by Teychenne et al. (2008), there have been several large-scale epidemiological studies published on this topic. Vallance and colleagues (2011) analyzed data from 2,862 adults from the National Health and Nutrition Examination Survey (NHANES) for 2005-2006. This is a national survey of U.S. adults that, for this time period, assessed physical activity and sedentary behavior objectively using accelerometers. Depression was assessed using the Patient Health Questionnaire-9.
Results showed that in comparison to the least sedentary quartile (the reference group), there was a trend for a greater risk of depression for those with higher levels of sedentary behavior. This was most clearly shown in the most sedentary quartile. This is shown in figure 12.1 for data from model 1 (odds ratios adjusted for gender, ethnicity, and age) and for model 2 with additional adjustment for other sociodemographic factors, health status, and moderate- to vigorous-intensity physical activity (MVPA). Although model 2 shows some attenuation of the odds for depression, the same trend is evident, and the most sedentary group has a twofold elevated risk of depression over those in the lowest sedentary quartile.
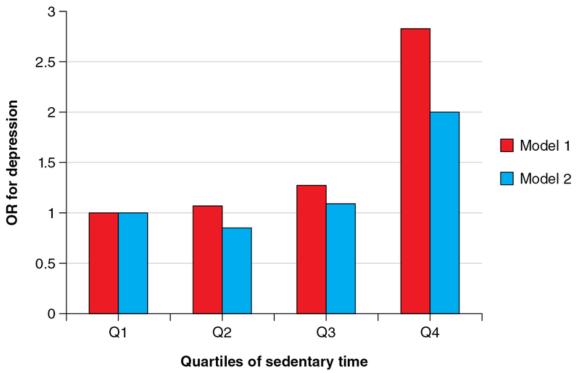
Odds ratios (OR) for depression across quartiles of objectively assessed sedentary time from the NHANES study. Model 1 is the least adjusted model and model 2 is the most adjusted.
Data from Vallance et al. 2011.
Save
Learn more about Sedentary Behavior and Health.
Metabolic Effects of Reduced Sitting and the Postprandial State
Several studies have investigated the effects on cardiometabolic biomarkers of short episodes (2- to 9-hr, single-day experiment) of prolonged uninterrupted sitting versus various manipulations of reduced sitting during the postprandial period.
Several studies have investigated the effects on cardiometabolic biomarkers of short episodes (2- to 9-hr, single-day experiment) of prolonged uninterrupted sitting versus various manipulations of reduced sitting during the postprandial period. Although the findings from the experimental studies that have specifically addressed the cardiometabolic consequences of prolonged sitting and reduced sitting are promising, there is still a clear need for the development of further high-quality research evidence. In addition to examining the effect of longer-term exposures (i.e., weeks or months), the various perturbations in the frequency (high versus low), length (short versus long), and type (ambulation versus standing) of activity interruptions to prolonged sitting and interactions with moderate- to vigorous-intensity physical activity, dietary intake, and meal patterns need to be examined.
Furthermore, there are likely to be effects of reducing and breaking up sitting time on multiple body tissues, organs, and systems (e.g., vascular and hemodynamic mechanisms, cognitive function, musculoskeletal adaptations). Establishing the dose - response relationships among interrupting sitting, risk markers, and physiological adaptations also has the potential to inform further work in specific disease groups - for example, among patients with hypertension, peripheral artery disease, osteoarthritis, overweight and obesity, metabolic syndrome and diabetes, and cognitive impairment, and among those with elevated thrombotic risk.
Prolonged Slow Walking Post Meal
Within the work-office setting, a randomized crossover trial by Nygaard and colleagues (2009) investigated the capillary (finger-prick) blood glucose response to a carbohydrate-rich meal over a 2-hour period (see table 3.1). The study compared, in healthy women aged >50 years, uninterrupted sitting to reduced sitting achieved through initial 15- and 40-minute bouts of slow, very light walking followed by sitting. The 40-minute walking condition, but not the 15-minute walking condition, induced a significant decrease in the 2-hour incremental glucose area under the curve (AUC), leading the authors to suggest that a dose response between the duration of slow walking (and the resultant increase in energy expenditure) and reductions in postprandial glycemia may exist. However, a subsequent study by Lunde and others (2012) using a similar study design and methodologies in female Pakistani immigrants (most of whom had abnormal glucose tolerance) demonstrated reductions in the 2-hour incremental area under the curve for both the 20-minute (by 30.6%) and 40-minute (by 39.0%) walking conditions relative to the control day. A significant reduction in systolic blood pressure was also observed after the 40-minute walking condition. The discrepancies between the results in these two studies suggest that a greater workload in terms of duration of the bout of activity or in terms of energy expenditure is required in metabolically unhealthy people. An interaction between extrinsic factors (i.e., physical activity) and genetic background (Caucasians versus Asians) may also influence the dose - response relationship between physical activity and metabolic health.

Save
Learn more about Sedentary Behavior and Health.
Screen Time and Cardiometabolic Risk Factors
In addition to the relationships with overweight and obesity, there is mounting evidence that screen time is associated with other cardiometabolic risk factors such as hypertension, high cholesterol levels, insulin resistance and type 2 diabetes mellitus, and metabolic syndrome (Council on Communications and Media 2011).
In addition to the relationships with overweight and obesity, there is mounting evidence that screen time is associated with other cardiometabolic risk factors such as hypertension, high cholesterol levels, insulin resistance and type 2 diabetes mellitus, and metabolic syndrome (Council on Communications and Media 2011). A study of 6- to 19-year-olds in the 2003-2004 and 2005-2006 NHANES found that the odds of having a higher cardiometabolic risk score (calculated from waist circumference, resting systolic blood pressure, non-high-density lipoprotein cholesterol, and C-reactive protein) were significantly higher for children who viewed 4 or more hours per day of television than for children who viewed less than 1 hour per day, adjusting for demographic characteristics, smoking, total calories from fat, total calories from saturated fat, dietary cholesterol intake, sodium intake, and physical activity (Carson and Janssen 2011). Similar results were found in a population-based sample of Portuguese 2- to 12-year-olds in the 2009 and 2010 Portuguese Prevalence Study of Obesity in Childhood, which found that higher television viewing time was significantly associated with an unfavorable cardiometabolic risk score (calculated from resting heart rate, resting diastolic blood pressure, resting systolic blood pressure, BMI, and skinfold thickness), adjusting for age, gender, parental education, parental BMI, perceptions of crime in the area, sleep duration, birth weight, duration of breastfeeding, a "bad diet" score, number of fruit portions eaten per week, and physical activity. This study also found significant positive associations between television viewing and resting systolic blood pressure and resting diastolic blood pressure (Stamatakis et al. 2013). In addition, a cross-sectional study of overweight and obese 14- to 18-year-olds found a significant positive association between television viewing and fasting insulin and HOMA-IR (indicators of insulin resistance), adjusting for demographic characteristics, waist-to-hip ratio, total caloric intake, percent of caloric intake from carbohydrate, and physical activity (Goldfield et al. 2013).
Although more limited than the television viewing research literature, studies provide some evidence for associations between computer use and video game playing with cardiometabolic risk factors. A cross-sectional study of overweight and obese 12- to 18-year-olds found a significant positive association between computer use and total cholesterol and low-density-lipoprotein cholesterol, adjusting for age, gender, pubertal stage, race/ethnicity, and physical activity (Altenburg et al. 2012). Another cross-sectional study of overweight and obese 14- to 18-year-olds found a significant positive association between video game playing and systolic blood pressure and ratio of total cholesterol to high-density lipoprotein, adjusting for demographic characteristics, BMI, sexual maturity, total caloric intake, percent of caloric intake from dietary fat, and physical activity (Goldfield et al. 2011).
Mechanisms Linking Screen Time and Obesity and Other Cardiometabolic Risks
Five mechanisms have been hypothesized to explain screen media viewing's contribution to obesity and other cardiometabolic risk factors (Council on Communications and Media 2011; Robinson 2001):
- Screen media viewing decreases metabolic rate.
- Screen media viewing displaces sleep or disturbs sleep patterns.
- Screen media viewing displaces physical activity, resulting in reduced energy expenditure.
- Dietary energy intake increases and dietary quality decreases during screen media viewing.
- Dietary energy intake increases and dietary practices worsen in response to advertising.
Although all of these mechanisms may be playing at least some role in the development of obesity and other cardiometabolic risk factors, limited evidence exists for the first three mechanisms. To date, the bulk of epidemiological and experimental studies are providing the greatest support for the fourth and fifth mechanisms.
Learn more about Sedentary Behavior and Health.
Sedentary Behavior and Depression
Teychenne, Ball, and Salmon (2008) conducted a systematic review on depression and sedentary behavior in adults. Seven observational (5 cross-sectional and 2 longitudinal) and four intervention studies were included.
Teychenne, Ball, and Salmon (2008) conducted a systematic review on depression and sedentary behavior in adults. Seven observational (5 cross-sectional and 2 longitudinal) and four intervention studies were included. Of the observational studies, 6 of 7 showed a positive association between sedentary behavior and depression; that is, higher sedentary behavior was associated with greater depression. The other study also showed this for time spent surfing the Internet, but reported negative associations for depression with hours spent e-mailing and using chat rooms. This suggests that the type of sedentary behavior may be an important moderator of any association between sedentary behavior and depression. More is said on this subject later in the chapter.
The four intervention studies reviewed by Teychenne et al. (2008) showed mixed results: one study showed no effect and one showed an increase in depression after the introduction of free computer and Internet use, while two showed that the risk of depression was reduced during the intervention. One provided extra computer and Internet use while the other used extra chat sessions. The latter may have boosted well-being through social interaction. It is important to note that the authors of the review concluded that at the time, no interventions had attempted to reduce sedentary behavior in an effort to assess changes in depression.
Since the review by Teychenne et al. (2008), there have been several large-scale epidemiological studies published on this topic. Vallance and colleagues (2011) analyzed data from 2,862 adults from the National Health and Nutrition Examination Survey (NHANES) for 2005-2006. This is a national survey of U.S. adults that, for this time period, assessed physical activity and sedentary behavior objectively using accelerometers. Depression was assessed using the Patient Health Questionnaire-9.
Results showed that in comparison to the least sedentary quartile (the reference group), there was a trend for a greater risk of depression for those with higher levels of sedentary behavior. This was most clearly shown in the most sedentary quartile. This is shown in figure 12.1 for data from model 1 (odds ratios adjusted for gender, ethnicity, and age) and for model 2 with additional adjustment for other sociodemographic factors, health status, and moderate- to vigorous-intensity physical activity (MVPA). Although model 2 shows some attenuation of the odds for depression, the same trend is evident, and the most sedentary group has a twofold elevated risk of depression over those in the lowest sedentary quartile.
Odds ratios (OR) for depression across quartiles of objectively assessed sedentary time from the NHANES study. Model 1 is the least adjusted model and model 2 is the most adjusted.
Data from Vallance et al. 2011.
Save
Learn more about Sedentary Behavior and Health.
Metabolic Effects of Reduced Sitting and the Postprandial State
Several studies have investigated the effects on cardiometabolic biomarkers of short episodes (2- to 9-hr, single-day experiment) of prolonged uninterrupted sitting versus various manipulations of reduced sitting during the postprandial period.
Several studies have investigated the effects on cardiometabolic biomarkers of short episodes (2- to 9-hr, single-day experiment) of prolonged uninterrupted sitting versus various manipulations of reduced sitting during the postprandial period. Although the findings from the experimental studies that have specifically addressed the cardiometabolic consequences of prolonged sitting and reduced sitting are promising, there is still a clear need for the development of further high-quality research evidence. In addition to examining the effect of longer-term exposures (i.e., weeks or months), the various perturbations in the frequency (high versus low), length (short versus long), and type (ambulation versus standing) of activity interruptions to prolonged sitting and interactions with moderate- to vigorous-intensity physical activity, dietary intake, and meal patterns need to be examined.
Furthermore, there are likely to be effects of reducing and breaking up sitting time on multiple body tissues, organs, and systems (e.g., vascular and hemodynamic mechanisms, cognitive function, musculoskeletal adaptations). Establishing the dose - response relationships among interrupting sitting, risk markers, and physiological adaptations also has the potential to inform further work in specific disease groups - for example, among patients with hypertension, peripheral artery disease, osteoarthritis, overweight and obesity, metabolic syndrome and diabetes, and cognitive impairment, and among those with elevated thrombotic risk.
Prolonged Slow Walking Post Meal
Within the work-office setting, a randomized crossover trial by Nygaard and colleagues (2009) investigated the capillary (finger-prick) blood glucose response to a carbohydrate-rich meal over a 2-hour period (see table 3.1). The study compared, in healthy women aged >50 years, uninterrupted sitting to reduced sitting achieved through initial 15- and 40-minute bouts of slow, very light walking followed by sitting. The 40-minute walking condition, but not the 15-minute walking condition, induced a significant decrease in the 2-hour incremental glucose area under the curve (AUC), leading the authors to suggest that a dose response between the duration of slow walking (and the resultant increase in energy expenditure) and reductions in postprandial glycemia may exist. However, a subsequent study by Lunde and others (2012) using a similar study design and methodologies in female Pakistani immigrants (most of whom had abnormal glucose tolerance) demonstrated reductions in the 2-hour incremental area under the curve for both the 20-minute (by 30.6%) and 40-minute (by 39.0%) walking conditions relative to the control day. A significant reduction in systolic blood pressure was also observed after the 40-minute walking condition. The discrepancies between the results in these two studies suggest that a greater workload in terms of duration of the bout of activity or in terms of energy expenditure is required in metabolically unhealthy people. An interaction between extrinsic factors (i.e., physical activity) and genetic background (Caucasians versus Asians) may also influence the dose - response relationship between physical activity and metabolic health.
Save
Learn more about Sedentary Behavior and Health.
Screen Time and Cardiometabolic Risk Factors
In addition to the relationships with overweight and obesity, there is mounting evidence that screen time is associated with other cardiometabolic risk factors such as hypertension, high cholesterol levels, insulin resistance and type 2 diabetes mellitus, and metabolic syndrome (Council on Communications and Media 2011).
In addition to the relationships with overweight and obesity, there is mounting evidence that screen time is associated with other cardiometabolic risk factors such as hypertension, high cholesterol levels, insulin resistance and type 2 diabetes mellitus, and metabolic syndrome (Council on Communications and Media 2011). A study of 6- to 19-year-olds in the 2003-2004 and 2005-2006 NHANES found that the odds of having a higher cardiometabolic risk score (calculated from waist circumference, resting systolic blood pressure, non-high-density lipoprotein cholesterol, and C-reactive protein) were significantly higher for children who viewed 4 or more hours per day of television than for children who viewed less than 1 hour per day, adjusting for demographic characteristics, smoking, total calories from fat, total calories from saturated fat, dietary cholesterol intake, sodium intake, and physical activity (Carson and Janssen 2011). Similar results were found in a population-based sample of Portuguese 2- to 12-year-olds in the 2009 and 2010 Portuguese Prevalence Study of Obesity in Childhood, which found that higher television viewing time was significantly associated with an unfavorable cardiometabolic risk score (calculated from resting heart rate, resting diastolic blood pressure, resting systolic blood pressure, BMI, and skinfold thickness), adjusting for age, gender, parental education, parental BMI, perceptions of crime in the area, sleep duration, birth weight, duration of breastfeeding, a "bad diet" score, number of fruit portions eaten per week, and physical activity. This study also found significant positive associations between television viewing and resting systolic blood pressure and resting diastolic blood pressure (Stamatakis et al. 2013). In addition, a cross-sectional study of overweight and obese 14- to 18-year-olds found a significant positive association between television viewing and fasting insulin and HOMA-IR (indicators of insulin resistance), adjusting for demographic characteristics, waist-to-hip ratio, total caloric intake, percent of caloric intake from carbohydrate, and physical activity (Goldfield et al. 2013).
Although more limited than the television viewing research literature, studies provide some evidence for associations between computer use and video game playing with cardiometabolic risk factors. A cross-sectional study of overweight and obese 12- to 18-year-olds found a significant positive association between computer use and total cholesterol and low-density-lipoprotein cholesterol, adjusting for age, gender, pubertal stage, race/ethnicity, and physical activity (Altenburg et al. 2012). Another cross-sectional study of overweight and obese 14- to 18-year-olds found a significant positive association between video game playing and systolic blood pressure and ratio of total cholesterol to high-density lipoprotein, adjusting for demographic characteristics, BMI, sexual maturity, total caloric intake, percent of caloric intake from dietary fat, and physical activity (Goldfield et al. 2011).
Mechanisms Linking Screen Time and Obesity and Other Cardiometabolic Risks
Five mechanisms have been hypothesized to explain screen media viewing's contribution to obesity and other cardiometabolic risk factors (Council on Communications and Media 2011; Robinson 2001):
- Screen media viewing decreases metabolic rate.
- Screen media viewing displaces sleep or disturbs sleep patterns.
- Screen media viewing displaces physical activity, resulting in reduced energy expenditure.
- Dietary energy intake increases and dietary quality decreases during screen media viewing.
- Dietary energy intake increases and dietary practices worsen in response to advertising.
Although all of these mechanisms may be playing at least some role in the development of obesity and other cardiometabolic risk factors, limited evidence exists for the first three mechanisms. To date, the bulk of epidemiological and experimental studies are providing the greatest support for the fourth and fifth mechanisms.
Learn more about Sedentary Behavior and Health.
Sedentary Behavior and Depression
Teychenne, Ball, and Salmon (2008) conducted a systematic review on depression and sedentary behavior in adults. Seven observational (5 cross-sectional and 2 longitudinal) and four intervention studies were included.
Teychenne, Ball, and Salmon (2008) conducted a systematic review on depression and sedentary behavior in adults. Seven observational (5 cross-sectional and 2 longitudinal) and four intervention studies were included. Of the observational studies, 6 of 7 showed a positive association between sedentary behavior and depression; that is, higher sedentary behavior was associated with greater depression. The other study also showed this for time spent surfing the Internet, but reported negative associations for depression with hours spent e-mailing and using chat rooms. This suggests that the type of sedentary behavior may be an important moderator of any association between sedentary behavior and depression. More is said on this subject later in the chapter.
The four intervention studies reviewed by Teychenne et al. (2008) showed mixed results: one study showed no effect and one showed an increase in depression after the introduction of free computer and Internet use, while two showed that the risk of depression was reduced during the intervention. One provided extra computer and Internet use while the other used extra chat sessions. The latter may have boosted well-being through social interaction. It is important to note that the authors of the review concluded that at the time, no interventions had attempted to reduce sedentary behavior in an effort to assess changes in depression.
Since the review by Teychenne et al. (2008), there have been several large-scale epidemiological studies published on this topic. Vallance and colleagues (2011) analyzed data from 2,862 adults from the National Health and Nutrition Examination Survey (NHANES) for 2005-2006. This is a national survey of U.S. adults that, for this time period, assessed physical activity and sedentary behavior objectively using accelerometers. Depression was assessed using the Patient Health Questionnaire-9.
Results showed that in comparison to the least sedentary quartile (the reference group), there was a trend for a greater risk of depression for those with higher levels of sedentary behavior. This was most clearly shown in the most sedentary quartile. This is shown in figure 12.1 for data from model 1 (odds ratios adjusted for gender, ethnicity, and age) and for model 2 with additional adjustment for other sociodemographic factors, health status, and moderate- to vigorous-intensity physical activity (MVPA). Although model 2 shows some attenuation of the odds for depression, the same trend is evident, and the most sedentary group has a twofold elevated risk of depression over those in the lowest sedentary quartile.
Odds ratios (OR) for depression across quartiles of objectively assessed sedentary time from the NHANES study. Model 1 is the least adjusted model and model 2 is the most adjusted.
Data from Vallance et al. 2011.
Save
Learn more about Sedentary Behavior and Health.
Metabolic Effects of Reduced Sitting and the Postprandial State
Several studies have investigated the effects on cardiometabolic biomarkers of short episodes (2- to 9-hr, single-day experiment) of prolonged uninterrupted sitting versus various manipulations of reduced sitting during the postprandial period.
Several studies have investigated the effects on cardiometabolic biomarkers of short episodes (2- to 9-hr, single-day experiment) of prolonged uninterrupted sitting versus various manipulations of reduced sitting during the postprandial period. Although the findings from the experimental studies that have specifically addressed the cardiometabolic consequences of prolonged sitting and reduced sitting are promising, there is still a clear need for the development of further high-quality research evidence. In addition to examining the effect of longer-term exposures (i.e., weeks or months), the various perturbations in the frequency (high versus low), length (short versus long), and type (ambulation versus standing) of activity interruptions to prolonged sitting and interactions with moderate- to vigorous-intensity physical activity, dietary intake, and meal patterns need to be examined.
Furthermore, there are likely to be effects of reducing and breaking up sitting time on multiple body tissues, organs, and systems (e.g., vascular and hemodynamic mechanisms, cognitive function, musculoskeletal adaptations). Establishing the dose - response relationships among interrupting sitting, risk markers, and physiological adaptations also has the potential to inform further work in specific disease groups - for example, among patients with hypertension, peripheral artery disease, osteoarthritis, overweight and obesity, metabolic syndrome and diabetes, and cognitive impairment, and among those with elevated thrombotic risk.
Prolonged Slow Walking Post Meal
Within the work-office setting, a randomized crossover trial by Nygaard and colleagues (2009) investigated the capillary (finger-prick) blood glucose response to a carbohydrate-rich meal over a 2-hour period (see table 3.1). The study compared, in healthy women aged >50 years, uninterrupted sitting to reduced sitting achieved through initial 15- and 40-minute bouts of slow, very light walking followed by sitting. The 40-minute walking condition, but not the 15-minute walking condition, induced a significant decrease in the 2-hour incremental glucose area under the curve (AUC), leading the authors to suggest that a dose response between the duration of slow walking (and the resultant increase in energy expenditure) and reductions in postprandial glycemia may exist. However, a subsequent study by Lunde and others (2012) using a similar study design and methodologies in female Pakistani immigrants (most of whom had abnormal glucose tolerance) demonstrated reductions in the 2-hour incremental area under the curve for both the 20-minute (by 30.6%) and 40-minute (by 39.0%) walking conditions relative to the control day. A significant reduction in systolic blood pressure was also observed after the 40-minute walking condition. The discrepancies between the results in these two studies suggest that a greater workload in terms of duration of the bout of activity or in terms of energy expenditure is required in metabolically unhealthy people. An interaction between extrinsic factors (i.e., physical activity) and genetic background (Caucasians versus Asians) may also influence the dose - response relationship between physical activity and metabolic health.
Save
Learn more about Sedentary Behavior and Health.
Screen Time and Cardiometabolic Risk Factors
In addition to the relationships with overweight and obesity, there is mounting evidence that screen time is associated with other cardiometabolic risk factors such as hypertension, high cholesterol levels, insulin resistance and type 2 diabetes mellitus, and metabolic syndrome (Council on Communications and Media 2011).
In addition to the relationships with overweight and obesity, there is mounting evidence that screen time is associated with other cardiometabolic risk factors such as hypertension, high cholesterol levels, insulin resistance and type 2 diabetes mellitus, and metabolic syndrome (Council on Communications and Media 2011). A study of 6- to 19-year-olds in the 2003-2004 and 2005-2006 NHANES found that the odds of having a higher cardiometabolic risk score (calculated from waist circumference, resting systolic blood pressure, non-high-density lipoprotein cholesterol, and C-reactive protein) were significantly higher for children who viewed 4 or more hours per day of television than for children who viewed less than 1 hour per day, adjusting for demographic characteristics, smoking, total calories from fat, total calories from saturated fat, dietary cholesterol intake, sodium intake, and physical activity (Carson and Janssen 2011). Similar results were found in a population-based sample of Portuguese 2- to 12-year-olds in the 2009 and 2010 Portuguese Prevalence Study of Obesity in Childhood, which found that higher television viewing time was significantly associated with an unfavorable cardiometabolic risk score (calculated from resting heart rate, resting diastolic blood pressure, resting systolic blood pressure, BMI, and skinfold thickness), adjusting for age, gender, parental education, parental BMI, perceptions of crime in the area, sleep duration, birth weight, duration of breastfeeding, a "bad diet" score, number of fruit portions eaten per week, and physical activity. This study also found significant positive associations between television viewing and resting systolic blood pressure and resting diastolic blood pressure (Stamatakis et al. 2013). In addition, a cross-sectional study of overweight and obese 14- to 18-year-olds found a significant positive association between television viewing and fasting insulin and HOMA-IR (indicators of insulin resistance), adjusting for demographic characteristics, waist-to-hip ratio, total caloric intake, percent of caloric intake from carbohydrate, and physical activity (Goldfield et al. 2013).
Although more limited than the television viewing research literature, studies provide some evidence for associations between computer use and video game playing with cardiometabolic risk factors. A cross-sectional study of overweight and obese 12- to 18-year-olds found a significant positive association between computer use and total cholesterol and low-density-lipoprotein cholesterol, adjusting for age, gender, pubertal stage, race/ethnicity, and physical activity (Altenburg et al. 2012). Another cross-sectional study of overweight and obese 14- to 18-year-olds found a significant positive association between video game playing and systolic blood pressure and ratio of total cholesterol to high-density lipoprotein, adjusting for demographic characteristics, BMI, sexual maturity, total caloric intake, percent of caloric intake from dietary fat, and physical activity (Goldfield et al. 2011).
Mechanisms Linking Screen Time and Obesity and Other Cardiometabolic Risks
Five mechanisms have been hypothesized to explain screen media viewing's contribution to obesity and other cardiometabolic risk factors (Council on Communications and Media 2011; Robinson 2001):
- Screen media viewing decreases metabolic rate.
- Screen media viewing displaces sleep or disturbs sleep patterns.
- Screen media viewing displaces physical activity, resulting in reduced energy expenditure.
- Dietary energy intake increases and dietary quality decreases during screen media viewing.
- Dietary energy intake increases and dietary practices worsen in response to advertising.
Although all of these mechanisms may be playing at least some role in the development of obesity and other cardiometabolic risk factors, limited evidence exists for the first three mechanisms. To date, the bulk of epidemiological and experimental studies are providing the greatest support for the fourth and fifth mechanisms.
Learn more about Sedentary Behavior and Health.
Sedentary Behavior and Depression
Teychenne, Ball, and Salmon (2008) conducted a systematic review on depression and sedentary behavior in adults. Seven observational (5 cross-sectional and 2 longitudinal) and four intervention studies were included.
Teychenne, Ball, and Salmon (2008) conducted a systematic review on depression and sedentary behavior in adults. Seven observational (5 cross-sectional and 2 longitudinal) and four intervention studies were included. Of the observational studies, 6 of 7 showed a positive association between sedentary behavior and depression; that is, higher sedentary behavior was associated with greater depression. The other study also showed this for time spent surfing the Internet, but reported negative associations for depression with hours spent e-mailing and using chat rooms. This suggests that the type of sedentary behavior may be an important moderator of any association between sedentary behavior and depression. More is said on this subject later in the chapter.
The four intervention studies reviewed by Teychenne et al. (2008) showed mixed results: one study showed no effect and one showed an increase in depression after the introduction of free computer and Internet use, while two showed that the risk of depression was reduced during the intervention. One provided extra computer and Internet use while the other used extra chat sessions. The latter may have boosted well-being through social interaction. It is important to note that the authors of the review concluded that at the time, no interventions had attempted to reduce sedentary behavior in an effort to assess changes in depression.
Since the review by Teychenne et al. (2008), there have been several large-scale epidemiological studies published on this topic. Vallance and colleagues (2011) analyzed data from 2,862 adults from the National Health and Nutrition Examination Survey (NHANES) for 2005-2006. This is a national survey of U.S. adults that, for this time period, assessed physical activity and sedentary behavior objectively using accelerometers. Depression was assessed using the Patient Health Questionnaire-9.
Results showed that in comparison to the least sedentary quartile (the reference group), there was a trend for a greater risk of depression for those with higher levels of sedentary behavior. This was most clearly shown in the most sedentary quartile. This is shown in figure 12.1 for data from model 1 (odds ratios adjusted for gender, ethnicity, and age) and for model 2 with additional adjustment for other sociodemographic factors, health status, and moderate- to vigorous-intensity physical activity (MVPA). Although model 2 shows some attenuation of the odds for depression, the same trend is evident, and the most sedentary group has a twofold elevated risk of depression over those in the lowest sedentary quartile.
Odds ratios (OR) for depression across quartiles of objectively assessed sedentary time from the NHANES study. Model 1 is the least adjusted model and model 2 is the most adjusted.
Data from Vallance et al. 2011.
Save
Learn more about Sedentary Behavior and Health.
Metabolic Effects of Reduced Sitting and the Postprandial State
Several studies have investigated the effects on cardiometabolic biomarkers of short episodes (2- to 9-hr, single-day experiment) of prolonged uninterrupted sitting versus various manipulations of reduced sitting during the postprandial period.
Several studies have investigated the effects on cardiometabolic biomarkers of short episodes (2- to 9-hr, single-day experiment) of prolonged uninterrupted sitting versus various manipulations of reduced sitting during the postprandial period. Although the findings from the experimental studies that have specifically addressed the cardiometabolic consequences of prolonged sitting and reduced sitting are promising, there is still a clear need for the development of further high-quality research evidence. In addition to examining the effect of longer-term exposures (i.e., weeks or months), the various perturbations in the frequency (high versus low), length (short versus long), and type (ambulation versus standing) of activity interruptions to prolonged sitting and interactions with moderate- to vigorous-intensity physical activity, dietary intake, and meal patterns need to be examined.
Furthermore, there are likely to be effects of reducing and breaking up sitting time on multiple body tissues, organs, and systems (e.g., vascular and hemodynamic mechanisms, cognitive function, musculoskeletal adaptations). Establishing the dose - response relationships among interrupting sitting, risk markers, and physiological adaptations also has the potential to inform further work in specific disease groups - for example, among patients with hypertension, peripheral artery disease, osteoarthritis, overweight and obesity, metabolic syndrome and diabetes, and cognitive impairment, and among those with elevated thrombotic risk.
Prolonged Slow Walking Post Meal
Within the work-office setting, a randomized crossover trial by Nygaard and colleagues (2009) investigated the capillary (finger-prick) blood glucose response to a carbohydrate-rich meal over a 2-hour period (see table 3.1). The study compared, in healthy women aged >50 years, uninterrupted sitting to reduced sitting achieved through initial 15- and 40-minute bouts of slow, very light walking followed by sitting. The 40-minute walking condition, but not the 15-minute walking condition, induced a significant decrease in the 2-hour incremental glucose area under the curve (AUC), leading the authors to suggest that a dose response between the duration of slow walking (and the resultant increase in energy expenditure) and reductions in postprandial glycemia may exist. However, a subsequent study by Lunde and others (2012) using a similar study design and methodologies in female Pakistani immigrants (most of whom had abnormal glucose tolerance) demonstrated reductions in the 2-hour incremental area under the curve for both the 20-minute (by 30.6%) and 40-minute (by 39.0%) walking conditions relative to the control day. A significant reduction in systolic blood pressure was also observed after the 40-minute walking condition. The discrepancies between the results in these two studies suggest that a greater workload in terms of duration of the bout of activity or in terms of energy expenditure is required in metabolically unhealthy people. An interaction between extrinsic factors (i.e., physical activity) and genetic background (Caucasians versus Asians) may also influence the dose - response relationship between physical activity and metabolic health.
Save
Learn more about Sedentary Behavior and Health.
Screen Time and Cardiometabolic Risk Factors
In addition to the relationships with overweight and obesity, there is mounting evidence that screen time is associated with other cardiometabolic risk factors such as hypertension, high cholesterol levels, insulin resistance and type 2 diabetes mellitus, and metabolic syndrome (Council on Communications and Media 2011).
In addition to the relationships with overweight and obesity, there is mounting evidence that screen time is associated with other cardiometabolic risk factors such as hypertension, high cholesterol levels, insulin resistance and type 2 diabetes mellitus, and metabolic syndrome (Council on Communications and Media 2011). A study of 6- to 19-year-olds in the 2003-2004 and 2005-2006 NHANES found that the odds of having a higher cardiometabolic risk score (calculated from waist circumference, resting systolic blood pressure, non-high-density lipoprotein cholesterol, and C-reactive protein) were significantly higher for children who viewed 4 or more hours per day of television than for children who viewed less than 1 hour per day, adjusting for demographic characteristics, smoking, total calories from fat, total calories from saturated fat, dietary cholesterol intake, sodium intake, and physical activity (Carson and Janssen 2011). Similar results were found in a population-based sample of Portuguese 2- to 12-year-olds in the 2009 and 2010 Portuguese Prevalence Study of Obesity in Childhood, which found that higher television viewing time was significantly associated with an unfavorable cardiometabolic risk score (calculated from resting heart rate, resting diastolic blood pressure, resting systolic blood pressure, BMI, and skinfold thickness), adjusting for age, gender, parental education, parental BMI, perceptions of crime in the area, sleep duration, birth weight, duration of breastfeeding, a "bad diet" score, number of fruit portions eaten per week, and physical activity. This study also found significant positive associations between television viewing and resting systolic blood pressure and resting diastolic blood pressure (Stamatakis et al. 2013). In addition, a cross-sectional study of overweight and obese 14- to 18-year-olds found a significant positive association between television viewing and fasting insulin and HOMA-IR (indicators of insulin resistance), adjusting for demographic characteristics, waist-to-hip ratio, total caloric intake, percent of caloric intake from carbohydrate, and physical activity (Goldfield et al. 2013).
Although more limited than the television viewing research literature, studies provide some evidence for associations between computer use and video game playing with cardiometabolic risk factors. A cross-sectional study of overweight and obese 12- to 18-year-olds found a significant positive association between computer use and total cholesterol and low-density-lipoprotein cholesterol, adjusting for age, gender, pubertal stage, race/ethnicity, and physical activity (Altenburg et al. 2012). Another cross-sectional study of overweight and obese 14- to 18-year-olds found a significant positive association between video game playing and systolic blood pressure and ratio of total cholesterol to high-density lipoprotein, adjusting for demographic characteristics, BMI, sexual maturity, total caloric intake, percent of caloric intake from dietary fat, and physical activity (Goldfield et al. 2011).
Mechanisms Linking Screen Time and Obesity and Other Cardiometabolic Risks
Five mechanisms have been hypothesized to explain screen media viewing's contribution to obesity and other cardiometabolic risk factors (Council on Communications and Media 2011; Robinson 2001):
- Screen media viewing decreases metabolic rate.
- Screen media viewing displaces sleep or disturbs sleep patterns.
- Screen media viewing displaces physical activity, resulting in reduced energy expenditure.
- Dietary energy intake increases and dietary quality decreases during screen media viewing.
- Dietary energy intake increases and dietary practices worsen in response to advertising.
Although all of these mechanisms may be playing at least some role in the development of obesity and other cardiometabolic risk factors, limited evidence exists for the first three mechanisms. To date, the bulk of epidemiological and experimental studies are providing the greatest support for the fourth and fifth mechanisms.
Learn more about Sedentary Behavior and Health.
Sedentary Behavior and Depression
Teychenne, Ball, and Salmon (2008) conducted a systematic review on depression and sedentary behavior in adults. Seven observational (5 cross-sectional and 2 longitudinal) and four intervention studies were included.
Teychenne, Ball, and Salmon (2008) conducted a systematic review on depression and sedentary behavior in adults. Seven observational (5 cross-sectional and 2 longitudinal) and four intervention studies were included. Of the observational studies, 6 of 7 showed a positive association between sedentary behavior and depression; that is, higher sedentary behavior was associated with greater depression. The other study also showed this for time spent surfing the Internet, but reported negative associations for depression with hours spent e-mailing and using chat rooms. This suggests that the type of sedentary behavior may be an important moderator of any association between sedentary behavior and depression. More is said on this subject later in the chapter.
The four intervention studies reviewed by Teychenne et al. (2008) showed mixed results: one study showed no effect and one showed an increase in depression after the introduction of free computer and Internet use, while two showed that the risk of depression was reduced during the intervention. One provided extra computer and Internet use while the other used extra chat sessions. The latter may have boosted well-being through social interaction. It is important to note that the authors of the review concluded that at the time, no interventions had attempted to reduce sedentary behavior in an effort to assess changes in depression.
Since the review by Teychenne et al. (2008), there have been several large-scale epidemiological studies published on this topic. Vallance and colleagues (2011) analyzed data from 2,862 adults from the National Health and Nutrition Examination Survey (NHANES) for 2005-2006. This is a national survey of U.S. adults that, for this time period, assessed physical activity and sedentary behavior objectively using accelerometers. Depression was assessed using the Patient Health Questionnaire-9.
Results showed that in comparison to the least sedentary quartile (the reference group), there was a trend for a greater risk of depression for those with higher levels of sedentary behavior. This was most clearly shown in the most sedentary quartile. This is shown in figure 12.1 for data from model 1 (odds ratios adjusted for gender, ethnicity, and age) and for model 2 with additional adjustment for other sociodemographic factors, health status, and moderate- to vigorous-intensity physical activity (MVPA). Although model 2 shows some attenuation of the odds for depression, the same trend is evident, and the most sedentary group has a twofold elevated risk of depression over those in the lowest sedentary quartile.
Odds ratios (OR) for depression across quartiles of objectively assessed sedentary time from the NHANES study. Model 1 is the least adjusted model and model 2 is the most adjusted.
Data from Vallance et al. 2011.
Save
Learn more about Sedentary Behavior and Health.
Metabolic Effects of Reduced Sitting and the Postprandial State
Several studies have investigated the effects on cardiometabolic biomarkers of short episodes (2- to 9-hr, single-day experiment) of prolonged uninterrupted sitting versus various manipulations of reduced sitting during the postprandial period.
Several studies have investigated the effects on cardiometabolic biomarkers of short episodes (2- to 9-hr, single-day experiment) of prolonged uninterrupted sitting versus various manipulations of reduced sitting during the postprandial period. Although the findings from the experimental studies that have specifically addressed the cardiometabolic consequences of prolonged sitting and reduced sitting are promising, there is still a clear need for the development of further high-quality research evidence. In addition to examining the effect of longer-term exposures (i.e., weeks or months), the various perturbations in the frequency (high versus low), length (short versus long), and type (ambulation versus standing) of activity interruptions to prolonged sitting and interactions with moderate- to vigorous-intensity physical activity, dietary intake, and meal patterns need to be examined.
Furthermore, there are likely to be effects of reducing and breaking up sitting time on multiple body tissues, organs, and systems (e.g., vascular and hemodynamic mechanisms, cognitive function, musculoskeletal adaptations). Establishing the dose - response relationships among interrupting sitting, risk markers, and physiological adaptations also has the potential to inform further work in specific disease groups - for example, among patients with hypertension, peripheral artery disease, osteoarthritis, overweight and obesity, metabolic syndrome and diabetes, and cognitive impairment, and among those with elevated thrombotic risk.
Prolonged Slow Walking Post Meal
Within the work-office setting, a randomized crossover trial by Nygaard and colleagues (2009) investigated the capillary (finger-prick) blood glucose response to a carbohydrate-rich meal over a 2-hour period (see table 3.1). The study compared, in healthy women aged >50 years, uninterrupted sitting to reduced sitting achieved through initial 15- and 40-minute bouts of slow, very light walking followed by sitting. The 40-minute walking condition, but not the 15-minute walking condition, induced a significant decrease in the 2-hour incremental glucose area under the curve (AUC), leading the authors to suggest that a dose response between the duration of slow walking (and the resultant increase in energy expenditure) and reductions in postprandial glycemia may exist. However, a subsequent study by Lunde and others (2012) using a similar study design and methodologies in female Pakistani immigrants (most of whom had abnormal glucose tolerance) demonstrated reductions in the 2-hour incremental area under the curve for both the 20-minute (by 30.6%) and 40-minute (by 39.0%) walking conditions relative to the control day. A significant reduction in systolic blood pressure was also observed after the 40-minute walking condition. The discrepancies between the results in these two studies suggest that a greater workload in terms of duration of the bout of activity or in terms of energy expenditure is required in metabolically unhealthy people. An interaction between extrinsic factors (i.e., physical activity) and genetic background (Caucasians versus Asians) may also influence the dose - response relationship between physical activity and metabolic health.
Save
Learn more about Sedentary Behavior and Health.
Screen Time and Cardiometabolic Risk Factors
In addition to the relationships with overweight and obesity, there is mounting evidence that screen time is associated with other cardiometabolic risk factors such as hypertension, high cholesterol levels, insulin resistance and type 2 diabetes mellitus, and metabolic syndrome (Council on Communications and Media 2011).
In addition to the relationships with overweight and obesity, there is mounting evidence that screen time is associated with other cardiometabolic risk factors such as hypertension, high cholesterol levels, insulin resistance and type 2 diabetes mellitus, and metabolic syndrome (Council on Communications and Media 2011). A study of 6- to 19-year-olds in the 2003-2004 and 2005-2006 NHANES found that the odds of having a higher cardiometabolic risk score (calculated from waist circumference, resting systolic blood pressure, non-high-density lipoprotein cholesterol, and C-reactive protein) were significantly higher for children who viewed 4 or more hours per day of television than for children who viewed less than 1 hour per day, adjusting for demographic characteristics, smoking, total calories from fat, total calories from saturated fat, dietary cholesterol intake, sodium intake, and physical activity (Carson and Janssen 2011). Similar results were found in a population-based sample of Portuguese 2- to 12-year-olds in the 2009 and 2010 Portuguese Prevalence Study of Obesity in Childhood, which found that higher television viewing time was significantly associated with an unfavorable cardiometabolic risk score (calculated from resting heart rate, resting diastolic blood pressure, resting systolic blood pressure, BMI, and skinfold thickness), adjusting for age, gender, parental education, parental BMI, perceptions of crime in the area, sleep duration, birth weight, duration of breastfeeding, a "bad diet" score, number of fruit portions eaten per week, and physical activity. This study also found significant positive associations between television viewing and resting systolic blood pressure and resting diastolic blood pressure (Stamatakis et al. 2013). In addition, a cross-sectional study of overweight and obese 14- to 18-year-olds found a significant positive association between television viewing and fasting insulin and HOMA-IR (indicators of insulin resistance), adjusting for demographic characteristics, waist-to-hip ratio, total caloric intake, percent of caloric intake from carbohydrate, and physical activity (Goldfield et al. 2013).
Although more limited than the television viewing research literature, studies provide some evidence for associations between computer use and video game playing with cardiometabolic risk factors. A cross-sectional study of overweight and obese 12- to 18-year-olds found a significant positive association between computer use and total cholesterol and low-density-lipoprotein cholesterol, adjusting for age, gender, pubertal stage, race/ethnicity, and physical activity (Altenburg et al. 2012). Another cross-sectional study of overweight and obese 14- to 18-year-olds found a significant positive association between video game playing and systolic blood pressure and ratio of total cholesterol to high-density lipoprotein, adjusting for demographic characteristics, BMI, sexual maturity, total caloric intake, percent of caloric intake from dietary fat, and physical activity (Goldfield et al. 2011).
Mechanisms Linking Screen Time and Obesity and Other Cardiometabolic Risks
Five mechanisms have been hypothesized to explain screen media viewing's contribution to obesity and other cardiometabolic risk factors (Council on Communications and Media 2011; Robinson 2001):
- Screen media viewing decreases metabolic rate.
- Screen media viewing displaces sleep or disturbs sleep patterns.
- Screen media viewing displaces physical activity, resulting in reduced energy expenditure.
- Dietary energy intake increases and dietary quality decreases during screen media viewing.
- Dietary energy intake increases and dietary practices worsen in response to advertising.
Although all of these mechanisms may be playing at least some role in the development of obesity and other cardiometabolic risk factors, limited evidence exists for the first three mechanisms. To date, the bulk of epidemiological and experimental studies are providing the greatest support for the fourth and fifth mechanisms.
Learn more about Sedentary Behavior and Health.
Sedentary Behavior and Depression
Teychenne, Ball, and Salmon (2008) conducted a systematic review on depression and sedentary behavior in adults. Seven observational (5 cross-sectional and 2 longitudinal) and four intervention studies were included.
Teychenne, Ball, and Salmon (2008) conducted a systematic review on depression and sedentary behavior in adults. Seven observational (5 cross-sectional and 2 longitudinal) and four intervention studies were included. Of the observational studies, 6 of 7 showed a positive association between sedentary behavior and depression; that is, higher sedentary behavior was associated with greater depression. The other study also showed this for time spent surfing the Internet, but reported negative associations for depression with hours spent e-mailing and using chat rooms. This suggests that the type of sedentary behavior may be an important moderator of any association between sedentary behavior and depression. More is said on this subject later in the chapter.
The four intervention studies reviewed by Teychenne et al. (2008) showed mixed results: one study showed no effect and one showed an increase in depression after the introduction of free computer and Internet use, while two showed that the risk of depression was reduced during the intervention. One provided extra computer and Internet use while the other used extra chat sessions. The latter may have boosted well-being through social interaction. It is important to note that the authors of the review concluded that at the time, no interventions had attempted to reduce sedentary behavior in an effort to assess changes in depression.
Since the review by Teychenne et al. (2008), there have been several large-scale epidemiological studies published on this topic. Vallance and colleagues (2011) analyzed data from 2,862 adults from the National Health and Nutrition Examination Survey (NHANES) for 2005-2006. This is a national survey of U.S. adults that, for this time period, assessed physical activity and sedentary behavior objectively using accelerometers. Depression was assessed using the Patient Health Questionnaire-9.
Results showed that in comparison to the least sedentary quartile (the reference group), there was a trend for a greater risk of depression for those with higher levels of sedentary behavior. This was most clearly shown in the most sedentary quartile. This is shown in figure 12.1 for data from model 1 (odds ratios adjusted for gender, ethnicity, and age) and for model 2 with additional adjustment for other sociodemographic factors, health status, and moderate- to vigorous-intensity physical activity (MVPA). Although model 2 shows some attenuation of the odds for depression, the same trend is evident, and the most sedentary group has a twofold elevated risk of depression over those in the lowest sedentary quartile.
Odds ratios (OR) for depression across quartiles of objectively assessed sedentary time from the NHANES study. Model 1 is the least adjusted model and model 2 is the most adjusted.
Data from Vallance et al. 2011.
Save
Learn more about Sedentary Behavior and Health.
Metabolic Effects of Reduced Sitting and the Postprandial State
Several studies have investigated the effects on cardiometabolic biomarkers of short episodes (2- to 9-hr, single-day experiment) of prolonged uninterrupted sitting versus various manipulations of reduced sitting during the postprandial period.
Several studies have investigated the effects on cardiometabolic biomarkers of short episodes (2- to 9-hr, single-day experiment) of prolonged uninterrupted sitting versus various manipulations of reduced sitting during the postprandial period. Although the findings from the experimental studies that have specifically addressed the cardiometabolic consequences of prolonged sitting and reduced sitting are promising, there is still a clear need for the development of further high-quality research evidence. In addition to examining the effect of longer-term exposures (i.e., weeks or months), the various perturbations in the frequency (high versus low), length (short versus long), and type (ambulation versus standing) of activity interruptions to prolonged sitting and interactions with moderate- to vigorous-intensity physical activity, dietary intake, and meal patterns need to be examined.
Furthermore, there are likely to be effects of reducing and breaking up sitting time on multiple body tissues, organs, and systems (e.g., vascular and hemodynamic mechanisms, cognitive function, musculoskeletal adaptations). Establishing the dose - response relationships among interrupting sitting, risk markers, and physiological adaptations also has the potential to inform further work in specific disease groups - for example, among patients with hypertension, peripheral artery disease, osteoarthritis, overweight and obesity, metabolic syndrome and diabetes, and cognitive impairment, and among those with elevated thrombotic risk.
Prolonged Slow Walking Post Meal
Within the work-office setting, a randomized crossover trial by Nygaard and colleagues (2009) investigated the capillary (finger-prick) blood glucose response to a carbohydrate-rich meal over a 2-hour period (see table 3.1). The study compared, in healthy women aged >50 years, uninterrupted sitting to reduced sitting achieved through initial 15- and 40-minute bouts of slow, very light walking followed by sitting. The 40-minute walking condition, but not the 15-minute walking condition, induced a significant decrease in the 2-hour incremental glucose area under the curve (AUC), leading the authors to suggest that a dose response between the duration of slow walking (and the resultant increase in energy expenditure) and reductions in postprandial glycemia may exist. However, a subsequent study by Lunde and others (2012) using a similar study design and methodologies in female Pakistani immigrants (most of whom had abnormal glucose tolerance) demonstrated reductions in the 2-hour incremental area under the curve for both the 20-minute (by 30.6%) and 40-minute (by 39.0%) walking conditions relative to the control day. A significant reduction in systolic blood pressure was also observed after the 40-minute walking condition. The discrepancies between the results in these two studies suggest that a greater workload in terms of duration of the bout of activity or in terms of energy expenditure is required in metabolically unhealthy people. An interaction between extrinsic factors (i.e., physical activity) and genetic background (Caucasians versus Asians) may also influence the dose - response relationship between physical activity and metabolic health.
Save
Learn more about Sedentary Behavior and Health.
Screen Time and Cardiometabolic Risk Factors
In addition to the relationships with overweight and obesity, there is mounting evidence that screen time is associated with other cardiometabolic risk factors such as hypertension, high cholesterol levels, insulin resistance and type 2 diabetes mellitus, and metabolic syndrome (Council on Communications and Media 2011).
In addition to the relationships with overweight and obesity, there is mounting evidence that screen time is associated with other cardiometabolic risk factors such as hypertension, high cholesterol levels, insulin resistance and type 2 diabetes mellitus, and metabolic syndrome (Council on Communications and Media 2011). A study of 6- to 19-year-olds in the 2003-2004 and 2005-2006 NHANES found that the odds of having a higher cardiometabolic risk score (calculated from waist circumference, resting systolic blood pressure, non-high-density lipoprotein cholesterol, and C-reactive protein) were significantly higher for children who viewed 4 or more hours per day of television than for children who viewed less than 1 hour per day, adjusting for demographic characteristics, smoking, total calories from fat, total calories from saturated fat, dietary cholesterol intake, sodium intake, and physical activity (Carson and Janssen 2011). Similar results were found in a population-based sample of Portuguese 2- to 12-year-olds in the 2009 and 2010 Portuguese Prevalence Study of Obesity in Childhood, which found that higher television viewing time was significantly associated with an unfavorable cardiometabolic risk score (calculated from resting heart rate, resting diastolic blood pressure, resting systolic blood pressure, BMI, and skinfold thickness), adjusting for age, gender, parental education, parental BMI, perceptions of crime in the area, sleep duration, birth weight, duration of breastfeeding, a "bad diet" score, number of fruit portions eaten per week, and physical activity. This study also found significant positive associations between television viewing and resting systolic blood pressure and resting diastolic blood pressure (Stamatakis et al. 2013). In addition, a cross-sectional study of overweight and obese 14- to 18-year-olds found a significant positive association between television viewing and fasting insulin and HOMA-IR (indicators of insulin resistance), adjusting for demographic characteristics, waist-to-hip ratio, total caloric intake, percent of caloric intake from carbohydrate, and physical activity (Goldfield et al. 2013).
Although more limited than the television viewing research literature, studies provide some evidence for associations between computer use and video game playing with cardiometabolic risk factors. A cross-sectional study of overweight and obese 12- to 18-year-olds found a significant positive association between computer use and total cholesterol and low-density-lipoprotein cholesterol, adjusting for age, gender, pubertal stage, race/ethnicity, and physical activity (Altenburg et al. 2012). Another cross-sectional study of overweight and obese 14- to 18-year-olds found a significant positive association between video game playing and systolic blood pressure and ratio of total cholesterol to high-density lipoprotein, adjusting for demographic characteristics, BMI, sexual maturity, total caloric intake, percent of caloric intake from dietary fat, and physical activity (Goldfield et al. 2011).
Mechanisms Linking Screen Time and Obesity and Other Cardiometabolic Risks
Five mechanisms have been hypothesized to explain screen media viewing's contribution to obesity and other cardiometabolic risk factors (Council on Communications and Media 2011; Robinson 2001):
- Screen media viewing decreases metabolic rate.
- Screen media viewing displaces sleep or disturbs sleep patterns.
- Screen media viewing displaces physical activity, resulting in reduced energy expenditure.
- Dietary energy intake increases and dietary quality decreases during screen media viewing.
- Dietary energy intake increases and dietary practices worsen in response to advertising.
Although all of these mechanisms may be playing at least some role in the development of obesity and other cardiometabolic risk factors, limited evidence exists for the first three mechanisms. To date, the bulk of epidemiological and experimental studies are providing the greatest support for the fourth and fifth mechanisms.
Learn more about Sedentary Behavior and Health.
Sedentary Behavior and Depression
Teychenne, Ball, and Salmon (2008) conducted a systematic review on depression and sedentary behavior in adults. Seven observational (5 cross-sectional and 2 longitudinal) and four intervention studies were included.
Teychenne, Ball, and Salmon (2008) conducted a systematic review on depression and sedentary behavior in adults. Seven observational (5 cross-sectional and 2 longitudinal) and four intervention studies were included. Of the observational studies, 6 of 7 showed a positive association between sedentary behavior and depression; that is, higher sedentary behavior was associated with greater depression. The other study also showed this for time spent surfing the Internet, but reported negative associations for depression with hours spent e-mailing and using chat rooms. This suggests that the type of sedentary behavior may be an important moderator of any association between sedentary behavior and depression. More is said on this subject later in the chapter.
The four intervention studies reviewed by Teychenne et al. (2008) showed mixed results: one study showed no effect and one showed an increase in depression after the introduction of free computer and Internet use, while two showed that the risk of depression was reduced during the intervention. One provided extra computer and Internet use while the other used extra chat sessions. The latter may have boosted well-being through social interaction. It is important to note that the authors of the review concluded that at the time, no interventions had attempted to reduce sedentary behavior in an effort to assess changes in depression.
Since the review by Teychenne et al. (2008), there have been several large-scale epidemiological studies published on this topic. Vallance and colleagues (2011) analyzed data from 2,862 adults from the National Health and Nutrition Examination Survey (NHANES) for 2005-2006. This is a national survey of U.S. adults that, for this time period, assessed physical activity and sedentary behavior objectively using accelerometers. Depression was assessed using the Patient Health Questionnaire-9.
Results showed that in comparison to the least sedentary quartile (the reference group), there was a trend for a greater risk of depression for those with higher levels of sedentary behavior. This was most clearly shown in the most sedentary quartile. This is shown in figure 12.1 for data from model 1 (odds ratios adjusted for gender, ethnicity, and age) and for model 2 with additional adjustment for other sociodemographic factors, health status, and moderate- to vigorous-intensity physical activity (MVPA). Although model 2 shows some attenuation of the odds for depression, the same trend is evident, and the most sedentary group has a twofold elevated risk of depression over those in the lowest sedentary quartile.
Odds ratios (OR) for depression across quartiles of objectively assessed sedentary time from the NHANES study. Model 1 is the least adjusted model and model 2 is the most adjusted.
Data from Vallance et al. 2011.
Save
Learn more about Sedentary Behavior and Health.
Metabolic Effects of Reduced Sitting and the Postprandial State
Several studies have investigated the effects on cardiometabolic biomarkers of short episodes (2- to 9-hr, single-day experiment) of prolonged uninterrupted sitting versus various manipulations of reduced sitting during the postprandial period.
Several studies have investigated the effects on cardiometabolic biomarkers of short episodes (2- to 9-hr, single-day experiment) of prolonged uninterrupted sitting versus various manipulations of reduced sitting during the postprandial period. Although the findings from the experimental studies that have specifically addressed the cardiometabolic consequences of prolonged sitting and reduced sitting are promising, there is still a clear need for the development of further high-quality research evidence. In addition to examining the effect of longer-term exposures (i.e., weeks or months), the various perturbations in the frequency (high versus low), length (short versus long), and type (ambulation versus standing) of activity interruptions to prolonged sitting and interactions with moderate- to vigorous-intensity physical activity, dietary intake, and meal patterns need to be examined.
Furthermore, there are likely to be effects of reducing and breaking up sitting time on multiple body tissues, organs, and systems (e.g., vascular and hemodynamic mechanisms, cognitive function, musculoskeletal adaptations). Establishing the dose - response relationships among interrupting sitting, risk markers, and physiological adaptations also has the potential to inform further work in specific disease groups - for example, among patients with hypertension, peripheral artery disease, osteoarthritis, overweight and obesity, metabolic syndrome and diabetes, and cognitive impairment, and among those with elevated thrombotic risk.
Prolonged Slow Walking Post Meal
Within the work-office setting, a randomized crossover trial by Nygaard and colleagues (2009) investigated the capillary (finger-prick) blood glucose response to a carbohydrate-rich meal over a 2-hour period (see table 3.1). The study compared, in healthy women aged >50 years, uninterrupted sitting to reduced sitting achieved through initial 15- and 40-minute bouts of slow, very light walking followed by sitting. The 40-minute walking condition, but not the 15-minute walking condition, induced a significant decrease in the 2-hour incremental glucose area under the curve (AUC), leading the authors to suggest that a dose response between the duration of slow walking (and the resultant increase in energy expenditure) and reductions in postprandial glycemia may exist. However, a subsequent study by Lunde and others (2012) using a similar study design and methodologies in female Pakistani immigrants (most of whom had abnormal glucose tolerance) demonstrated reductions in the 2-hour incremental area under the curve for both the 20-minute (by 30.6%) and 40-minute (by 39.0%) walking conditions relative to the control day. A significant reduction in systolic blood pressure was also observed after the 40-minute walking condition. The discrepancies between the results in these two studies suggest that a greater workload in terms of duration of the bout of activity or in terms of energy expenditure is required in metabolically unhealthy people. An interaction between extrinsic factors (i.e., physical activity) and genetic background (Caucasians versus Asians) may also influence the dose - response relationship between physical activity and metabolic health.
Save
Learn more about Sedentary Behavior and Health.
Screen Time and Cardiometabolic Risk Factors
In addition to the relationships with overweight and obesity, there is mounting evidence that screen time is associated with other cardiometabolic risk factors such as hypertension, high cholesterol levels, insulin resistance and type 2 diabetes mellitus, and metabolic syndrome (Council on Communications and Media 2011).
In addition to the relationships with overweight and obesity, there is mounting evidence that screen time is associated with other cardiometabolic risk factors such as hypertension, high cholesterol levels, insulin resistance and type 2 diabetes mellitus, and metabolic syndrome (Council on Communications and Media 2011). A study of 6- to 19-year-olds in the 2003-2004 and 2005-2006 NHANES found that the odds of having a higher cardiometabolic risk score (calculated from waist circumference, resting systolic blood pressure, non-high-density lipoprotein cholesterol, and C-reactive protein) were significantly higher for children who viewed 4 or more hours per day of television than for children who viewed less than 1 hour per day, adjusting for demographic characteristics, smoking, total calories from fat, total calories from saturated fat, dietary cholesterol intake, sodium intake, and physical activity (Carson and Janssen 2011). Similar results were found in a population-based sample of Portuguese 2- to 12-year-olds in the 2009 and 2010 Portuguese Prevalence Study of Obesity in Childhood, which found that higher television viewing time was significantly associated with an unfavorable cardiometabolic risk score (calculated from resting heart rate, resting diastolic blood pressure, resting systolic blood pressure, BMI, and skinfold thickness), adjusting for age, gender, parental education, parental BMI, perceptions of crime in the area, sleep duration, birth weight, duration of breastfeeding, a "bad diet" score, number of fruit portions eaten per week, and physical activity. This study also found significant positive associations between television viewing and resting systolic blood pressure and resting diastolic blood pressure (Stamatakis et al. 2013). In addition, a cross-sectional study of overweight and obese 14- to 18-year-olds found a significant positive association between television viewing and fasting insulin and HOMA-IR (indicators of insulin resistance), adjusting for demographic characteristics, waist-to-hip ratio, total caloric intake, percent of caloric intake from carbohydrate, and physical activity (Goldfield et al. 2013).
Although more limited than the television viewing research literature, studies provide some evidence for associations between computer use and video game playing with cardiometabolic risk factors. A cross-sectional study of overweight and obese 12- to 18-year-olds found a significant positive association between computer use and total cholesterol and low-density-lipoprotein cholesterol, adjusting for age, gender, pubertal stage, race/ethnicity, and physical activity (Altenburg et al. 2012). Another cross-sectional study of overweight and obese 14- to 18-year-olds found a significant positive association between video game playing and systolic blood pressure and ratio of total cholesterol to high-density lipoprotein, adjusting for demographic characteristics, BMI, sexual maturity, total caloric intake, percent of caloric intake from dietary fat, and physical activity (Goldfield et al. 2011).
Mechanisms Linking Screen Time and Obesity and Other Cardiometabolic Risks
Five mechanisms have been hypothesized to explain screen media viewing's contribution to obesity and other cardiometabolic risk factors (Council on Communications and Media 2011; Robinson 2001):
- Screen media viewing decreases metabolic rate.
- Screen media viewing displaces sleep or disturbs sleep patterns.
- Screen media viewing displaces physical activity, resulting in reduced energy expenditure.
- Dietary energy intake increases and dietary quality decreases during screen media viewing.
- Dietary energy intake increases and dietary practices worsen in response to advertising.
Although all of these mechanisms may be playing at least some role in the development of obesity and other cardiometabolic risk factors, limited evidence exists for the first three mechanisms. To date, the bulk of epidemiological and experimental studies are providing the greatest support for the fourth and fifth mechanisms.
Learn more about Sedentary Behavior and Health.
Sedentary Behavior and Depression
Teychenne, Ball, and Salmon (2008) conducted a systematic review on depression and sedentary behavior in adults. Seven observational (5 cross-sectional and 2 longitudinal) and four intervention studies were included.
Teychenne, Ball, and Salmon (2008) conducted a systematic review on depression and sedentary behavior in adults. Seven observational (5 cross-sectional and 2 longitudinal) and four intervention studies were included. Of the observational studies, 6 of 7 showed a positive association between sedentary behavior and depression; that is, higher sedentary behavior was associated with greater depression. The other study also showed this for time spent surfing the Internet, but reported negative associations for depression with hours spent e-mailing and using chat rooms. This suggests that the type of sedentary behavior may be an important moderator of any association between sedentary behavior and depression. More is said on this subject later in the chapter.
The four intervention studies reviewed by Teychenne et al. (2008) showed mixed results: one study showed no effect and one showed an increase in depression after the introduction of free computer and Internet use, while two showed that the risk of depression was reduced during the intervention. One provided extra computer and Internet use while the other used extra chat sessions. The latter may have boosted well-being through social interaction. It is important to note that the authors of the review concluded that at the time, no interventions had attempted to reduce sedentary behavior in an effort to assess changes in depression.
Since the review by Teychenne et al. (2008), there have been several large-scale epidemiological studies published on this topic. Vallance and colleagues (2011) analyzed data from 2,862 adults from the National Health and Nutrition Examination Survey (NHANES) for 2005-2006. This is a national survey of U.S. adults that, for this time period, assessed physical activity and sedentary behavior objectively using accelerometers. Depression was assessed using the Patient Health Questionnaire-9.
Results showed that in comparison to the least sedentary quartile (the reference group), there was a trend for a greater risk of depression for those with higher levels of sedentary behavior. This was most clearly shown in the most sedentary quartile. This is shown in figure 12.1 for data from model 1 (odds ratios adjusted for gender, ethnicity, and age) and for model 2 with additional adjustment for other sociodemographic factors, health status, and moderate- to vigorous-intensity physical activity (MVPA). Although model 2 shows some attenuation of the odds for depression, the same trend is evident, and the most sedentary group has a twofold elevated risk of depression over those in the lowest sedentary quartile.
Odds ratios (OR) for depression across quartiles of objectively assessed sedentary time from the NHANES study. Model 1 is the least adjusted model and model 2 is the most adjusted.
Data from Vallance et al. 2011.
Save
Learn more about Sedentary Behavior and Health.
Metabolic Effects of Reduced Sitting and the Postprandial State
Several studies have investigated the effects on cardiometabolic biomarkers of short episodes (2- to 9-hr, single-day experiment) of prolonged uninterrupted sitting versus various manipulations of reduced sitting during the postprandial period.
Several studies have investigated the effects on cardiometabolic biomarkers of short episodes (2- to 9-hr, single-day experiment) of prolonged uninterrupted sitting versus various manipulations of reduced sitting during the postprandial period. Although the findings from the experimental studies that have specifically addressed the cardiometabolic consequences of prolonged sitting and reduced sitting are promising, there is still a clear need for the development of further high-quality research evidence. In addition to examining the effect of longer-term exposures (i.e., weeks or months), the various perturbations in the frequency (high versus low), length (short versus long), and type (ambulation versus standing) of activity interruptions to prolonged sitting and interactions with moderate- to vigorous-intensity physical activity, dietary intake, and meal patterns need to be examined.
Furthermore, there are likely to be effects of reducing and breaking up sitting time on multiple body tissues, organs, and systems (e.g., vascular and hemodynamic mechanisms, cognitive function, musculoskeletal adaptations). Establishing the dose - response relationships among interrupting sitting, risk markers, and physiological adaptations also has the potential to inform further work in specific disease groups - for example, among patients with hypertension, peripheral artery disease, osteoarthritis, overweight and obesity, metabolic syndrome and diabetes, and cognitive impairment, and among those with elevated thrombotic risk.
Prolonged Slow Walking Post Meal
Within the work-office setting, a randomized crossover trial by Nygaard and colleagues (2009) investigated the capillary (finger-prick) blood glucose response to a carbohydrate-rich meal over a 2-hour period (see table 3.1). The study compared, in healthy women aged >50 years, uninterrupted sitting to reduced sitting achieved through initial 15- and 40-minute bouts of slow, very light walking followed by sitting. The 40-minute walking condition, but not the 15-minute walking condition, induced a significant decrease in the 2-hour incremental glucose area under the curve (AUC), leading the authors to suggest that a dose response between the duration of slow walking (and the resultant increase in energy expenditure) and reductions in postprandial glycemia may exist. However, a subsequent study by Lunde and others (2012) using a similar study design and methodologies in female Pakistani immigrants (most of whom had abnormal glucose tolerance) demonstrated reductions in the 2-hour incremental area under the curve for both the 20-minute (by 30.6%) and 40-minute (by 39.0%) walking conditions relative to the control day. A significant reduction in systolic blood pressure was also observed after the 40-minute walking condition. The discrepancies between the results in these two studies suggest that a greater workload in terms of duration of the bout of activity or in terms of energy expenditure is required in metabolically unhealthy people. An interaction between extrinsic factors (i.e., physical activity) and genetic background (Caucasians versus Asians) may also influence the dose - response relationship between physical activity and metabolic health.
Save
Learn more about Sedentary Behavior and Health.
Screen Time and Cardiometabolic Risk Factors
In addition to the relationships with overweight and obesity, there is mounting evidence that screen time is associated with other cardiometabolic risk factors such as hypertension, high cholesterol levels, insulin resistance and type 2 diabetes mellitus, and metabolic syndrome (Council on Communications and Media 2011).
In addition to the relationships with overweight and obesity, there is mounting evidence that screen time is associated with other cardiometabolic risk factors such as hypertension, high cholesterol levels, insulin resistance and type 2 diabetes mellitus, and metabolic syndrome (Council on Communications and Media 2011). A study of 6- to 19-year-olds in the 2003-2004 and 2005-2006 NHANES found that the odds of having a higher cardiometabolic risk score (calculated from waist circumference, resting systolic blood pressure, non-high-density lipoprotein cholesterol, and C-reactive protein) were significantly higher for children who viewed 4 or more hours per day of television than for children who viewed less than 1 hour per day, adjusting for demographic characteristics, smoking, total calories from fat, total calories from saturated fat, dietary cholesterol intake, sodium intake, and physical activity (Carson and Janssen 2011). Similar results were found in a population-based sample of Portuguese 2- to 12-year-olds in the 2009 and 2010 Portuguese Prevalence Study of Obesity in Childhood, which found that higher television viewing time was significantly associated with an unfavorable cardiometabolic risk score (calculated from resting heart rate, resting diastolic blood pressure, resting systolic blood pressure, BMI, and skinfold thickness), adjusting for age, gender, parental education, parental BMI, perceptions of crime in the area, sleep duration, birth weight, duration of breastfeeding, a "bad diet" score, number of fruit portions eaten per week, and physical activity. This study also found significant positive associations between television viewing and resting systolic blood pressure and resting diastolic blood pressure (Stamatakis et al. 2013). In addition, a cross-sectional study of overweight and obese 14- to 18-year-olds found a significant positive association between television viewing and fasting insulin and HOMA-IR (indicators of insulin resistance), adjusting for demographic characteristics, waist-to-hip ratio, total caloric intake, percent of caloric intake from carbohydrate, and physical activity (Goldfield et al. 2013).
Although more limited than the television viewing research literature, studies provide some evidence for associations between computer use and video game playing with cardiometabolic risk factors. A cross-sectional study of overweight and obese 12- to 18-year-olds found a significant positive association between computer use and total cholesterol and low-density-lipoprotein cholesterol, adjusting for age, gender, pubertal stage, race/ethnicity, and physical activity (Altenburg et al. 2012). Another cross-sectional study of overweight and obese 14- to 18-year-olds found a significant positive association between video game playing and systolic blood pressure and ratio of total cholesterol to high-density lipoprotein, adjusting for demographic characteristics, BMI, sexual maturity, total caloric intake, percent of caloric intake from dietary fat, and physical activity (Goldfield et al. 2011).
Mechanisms Linking Screen Time and Obesity and Other Cardiometabolic Risks
Five mechanisms have been hypothesized to explain screen media viewing's contribution to obesity and other cardiometabolic risk factors (Council on Communications and Media 2011; Robinson 2001):
- Screen media viewing decreases metabolic rate.
- Screen media viewing displaces sleep or disturbs sleep patterns.
- Screen media viewing displaces physical activity, resulting in reduced energy expenditure.
- Dietary energy intake increases and dietary quality decreases during screen media viewing.
- Dietary energy intake increases and dietary practices worsen in response to advertising.
Although all of these mechanisms may be playing at least some role in the development of obesity and other cardiometabolic risk factors, limited evidence exists for the first three mechanisms. To date, the bulk of epidemiological and experimental studies are providing the greatest support for the fourth and fifth mechanisms.
Learn more about Sedentary Behavior and Health.
Sedentary Behavior and Depression
Teychenne, Ball, and Salmon (2008) conducted a systematic review on depression and sedentary behavior in adults. Seven observational (5 cross-sectional and 2 longitudinal) and four intervention studies were included.
Teychenne, Ball, and Salmon (2008) conducted a systematic review on depression and sedentary behavior in adults. Seven observational (5 cross-sectional and 2 longitudinal) and four intervention studies were included. Of the observational studies, 6 of 7 showed a positive association between sedentary behavior and depression; that is, higher sedentary behavior was associated with greater depression. The other study also showed this for time spent surfing the Internet, but reported negative associations for depression with hours spent e-mailing and using chat rooms. This suggests that the type of sedentary behavior may be an important moderator of any association between sedentary behavior and depression. More is said on this subject later in the chapter.
The four intervention studies reviewed by Teychenne et al. (2008) showed mixed results: one study showed no effect and one showed an increase in depression after the introduction of free computer and Internet use, while two showed that the risk of depression was reduced during the intervention. One provided extra computer and Internet use while the other used extra chat sessions. The latter may have boosted well-being through social interaction. It is important to note that the authors of the review concluded that at the time, no interventions had attempted to reduce sedentary behavior in an effort to assess changes in depression.
Since the review by Teychenne et al. (2008), there have been several large-scale epidemiological studies published on this topic. Vallance and colleagues (2011) analyzed data from 2,862 adults from the National Health and Nutrition Examination Survey (NHANES) for 2005-2006. This is a national survey of U.S. adults that, for this time period, assessed physical activity and sedentary behavior objectively using accelerometers. Depression was assessed using the Patient Health Questionnaire-9.
Results showed that in comparison to the least sedentary quartile (the reference group), there was a trend for a greater risk of depression for those with higher levels of sedentary behavior. This was most clearly shown in the most sedentary quartile. This is shown in figure 12.1 for data from model 1 (odds ratios adjusted for gender, ethnicity, and age) and for model 2 with additional adjustment for other sociodemographic factors, health status, and moderate- to vigorous-intensity physical activity (MVPA). Although model 2 shows some attenuation of the odds for depression, the same trend is evident, and the most sedentary group has a twofold elevated risk of depression over those in the lowest sedentary quartile.
Odds ratios (OR) for depression across quartiles of objectively assessed sedentary time from the NHANES study. Model 1 is the least adjusted model and model 2 is the most adjusted.
Data from Vallance et al. 2011.
Save
Learn more about Sedentary Behavior and Health.
Metabolic Effects of Reduced Sitting and the Postprandial State
Several studies have investigated the effects on cardiometabolic biomarkers of short episodes (2- to 9-hr, single-day experiment) of prolonged uninterrupted sitting versus various manipulations of reduced sitting during the postprandial period.
Several studies have investigated the effects on cardiometabolic biomarkers of short episodes (2- to 9-hr, single-day experiment) of prolonged uninterrupted sitting versus various manipulations of reduced sitting during the postprandial period. Although the findings from the experimental studies that have specifically addressed the cardiometabolic consequences of prolonged sitting and reduced sitting are promising, there is still a clear need for the development of further high-quality research evidence. In addition to examining the effect of longer-term exposures (i.e., weeks or months), the various perturbations in the frequency (high versus low), length (short versus long), and type (ambulation versus standing) of activity interruptions to prolonged sitting and interactions with moderate- to vigorous-intensity physical activity, dietary intake, and meal patterns need to be examined.
Furthermore, there are likely to be effects of reducing and breaking up sitting time on multiple body tissues, organs, and systems (e.g., vascular and hemodynamic mechanisms, cognitive function, musculoskeletal adaptations). Establishing the dose - response relationships among interrupting sitting, risk markers, and physiological adaptations also has the potential to inform further work in specific disease groups - for example, among patients with hypertension, peripheral artery disease, osteoarthritis, overweight and obesity, metabolic syndrome and diabetes, and cognitive impairment, and among those with elevated thrombotic risk.
Prolonged Slow Walking Post Meal
Within the work-office setting, a randomized crossover trial by Nygaard and colleagues (2009) investigated the capillary (finger-prick) blood glucose response to a carbohydrate-rich meal over a 2-hour period (see table 3.1). The study compared, in healthy women aged >50 years, uninterrupted sitting to reduced sitting achieved through initial 15- and 40-minute bouts of slow, very light walking followed by sitting. The 40-minute walking condition, but not the 15-minute walking condition, induced a significant decrease in the 2-hour incremental glucose area under the curve (AUC), leading the authors to suggest that a dose response between the duration of slow walking (and the resultant increase in energy expenditure) and reductions in postprandial glycemia may exist. However, a subsequent study by Lunde and others (2012) using a similar study design and methodologies in female Pakistani immigrants (most of whom had abnormal glucose tolerance) demonstrated reductions in the 2-hour incremental area under the curve for both the 20-minute (by 30.6%) and 40-minute (by 39.0%) walking conditions relative to the control day. A significant reduction in systolic blood pressure was also observed after the 40-minute walking condition. The discrepancies between the results in these two studies suggest that a greater workload in terms of duration of the bout of activity or in terms of energy expenditure is required in metabolically unhealthy people. An interaction between extrinsic factors (i.e., physical activity) and genetic background (Caucasians versus Asians) may also influence the dose - response relationship between physical activity and metabolic health.
Save
Learn more about Sedentary Behavior and Health.
Screen Time and Cardiometabolic Risk Factors
In addition to the relationships with overweight and obesity, there is mounting evidence that screen time is associated with other cardiometabolic risk factors such as hypertension, high cholesterol levels, insulin resistance and type 2 diabetes mellitus, and metabolic syndrome (Council on Communications and Media 2011).
In addition to the relationships with overweight and obesity, there is mounting evidence that screen time is associated with other cardiometabolic risk factors such as hypertension, high cholesterol levels, insulin resistance and type 2 diabetes mellitus, and metabolic syndrome (Council on Communications and Media 2011). A study of 6- to 19-year-olds in the 2003-2004 and 2005-2006 NHANES found that the odds of having a higher cardiometabolic risk score (calculated from waist circumference, resting systolic blood pressure, non-high-density lipoprotein cholesterol, and C-reactive protein) were significantly higher for children who viewed 4 or more hours per day of television than for children who viewed less than 1 hour per day, adjusting for demographic characteristics, smoking, total calories from fat, total calories from saturated fat, dietary cholesterol intake, sodium intake, and physical activity (Carson and Janssen 2011). Similar results were found in a population-based sample of Portuguese 2- to 12-year-olds in the 2009 and 2010 Portuguese Prevalence Study of Obesity in Childhood, which found that higher television viewing time was significantly associated with an unfavorable cardiometabolic risk score (calculated from resting heart rate, resting diastolic blood pressure, resting systolic blood pressure, BMI, and skinfold thickness), adjusting for age, gender, parental education, parental BMI, perceptions of crime in the area, sleep duration, birth weight, duration of breastfeeding, a "bad diet" score, number of fruit portions eaten per week, and physical activity. This study also found significant positive associations between television viewing and resting systolic blood pressure and resting diastolic blood pressure (Stamatakis et al. 2013). In addition, a cross-sectional study of overweight and obese 14- to 18-year-olds found a significant positive association between television viewing and fasting insulin and HOMA-IR (indicators of insulin resistance), adjusting for demographic characteristics, waist-to-hip ratio, total caloric intake, percent of caloric intake from carbohydrate, and physical activity (Goldfield et al. 2013).
Although more limited than the television viewing research literature, studies provide some evidence for associations between computer use and video game playing with cardiometabolic risk factors. A cross-sectional study of overweight and obese 12- to 18-year-olds found a significant positive association between computer use and total cholesterol and low-density-lipoprotein cholesterol, adjusting for age, gender, pubertal stage, race/ethnicity, and physical activity (Altenburg et al. 2012). Another cross-sectional study of overweight and obese 14- to 18-year-olds found a significant positive association between video game playing and systolic blood pressure and ratio of total cholesterol to high-density lipoprotein, adjusting for demographic characteristics, BMI, sexual maturity, total caloric intake, percent of caloric intake from dietary fat, and physical activity (Goldfield et al. 2011).
Mechanisms Linking Screen Time and Obesity and Other Cardiometabolic Risks
Five mechanisms have been hypothesized to explain screen media viewing's contribution to obesity and other cardiometabolic risk factors (Council on Communications and Media 2011; Robinson 2001):
- Screen media viewing decreases metabolic rate.
- Screen media viewing displaces sleep or disturbs sleep patterns.
- Screen media viewing displaces physical activity, resulting in reduced energy expenditure.
- Dietary energy intake increases and dietary quality decreases during screen media viewing.
- Dietary energy intake increases and dietary practices worsen in response to advertising.
Although all of these mechanisms may be playing at least some role in the development of obesity and other cardiometabolic risk factors, limited evidence exists for the first three mechanisms. To date, the bulk of epidemiological and experimental studies are providing the greatest support for the fourth and fifth mechanisms.
Learn more about Sedentary Behavior and Health.
Related Books









