- Home
- Kinesiology/Exercise and Sport Science
- Physiology of Sport and Exercise
- Advanced Exercise Physiology

Advanced Exercise Physiology
Essential Concepts and Applications
by Jonathan K Ehrman, Dennis J. Kerrigan and Steven J. Keteyian
384 Pages
Advanced Exercise Physiology: Essential Concepts and Applications builds upon foundational topics and looks further into key physiological components to help advanced students gain a deeper level of understanding. Authors Jonathan K. Ehrman, Dennis J. Kerrigan, and Steven J. Keteyian address a wide range of complex topics with evidence-based information and a focused, targeted style.
The first five chapters offer a detailed examination of the various body systems. The next two chapters focus on exercise testing and training principles, as well as training adaptations as they relate to aerobic power, anaerobic power, range of motion, and resistance training of healthy individuals and competitive athletes. The remaining chapters focus on a variety of topics, including athletic performance, body composition and weight management, and environmental influences of exercise physiology. The final two chapters bring a unique perspective to the book with a review of the relationship between exercise physiology and public health and a look at recent and emerging topics in the field, including genomics and pharmacology.
Enhancing the content are learning aids, more than 140 images and illustrations, and practical examples from among clinical patients, healthy individuals, and competitive athletes. Key terms and their definitions appear at the end of each chapter; these help students understand key concepts and serve as a useful reference for practitioners. The appendixes contain information related to topics such as efficiency and energy expenditure, metabolic equivalent (MET) values of common activities, and the professionalization of exercise physiology.
For instructors, Advanced Exercise Physiology also includes a test package and an image bank to assist wtih classroom lecture preparations. The ancillaries, in-text learning components, and comprehensive content combine to create an ideal text to be used in advanced courses in exercise physiology.
Chapter 1. Exercise Metabolism
Chapter 2. Dynamics of Skeletal-Neuromuscular and Gastrointestinal Physiology
Chapter 3. Cardiovascular System: Function and Control
Chapter 4. Pulmonary Exercise Physiology
Chapter 5. Immune and Endocrine System
Chapter 6. Principles for Testing and Training for Aerobic Power
Chapter 7. Principles for Testing and Training Anaerobic Strength, Power, and Range of Motion
Chapter 8. Body Composition and Weight Management
Chapter 9. Performance: Environmental Stressors, Genetics, Nutrition, and Ergogenic Aids
Chapter 10. Physical Activity and Exercise for Health and Fitness
Chapter 11. Emerging Concepts: Exercise Pharmacology and Exercise Genomics
Appendix A. Calculations for Oxygen Consumption and Carbon Dioxide Production
Appendix B. Efficiency and Energy Expenditure
Appendix C. Metabolic Equivalent of Task Values of Common Activities
Appendix D. Professionalization of the Exercise Professional
Appendix E. Common Scientific Abbreviations and Units
Jonathan K. Ehrman, PhD, FACSM, FAACVPR, is the associate program director of preventive cardiology and of the Exercise Physiology Core Laboratory and the director of the clinical weight management program at Henry Ford Hospital in Detroit, Michigan. He specializes in cardiac rehabilitation and preventive cardiology. He is also a clinical assistant professor in the exercise science program at Oakland University. He is a fellow of the American Association of Cardiovascular and Pulmonary Rehabilitation (AACVPR) and the American College of Sports Medicine (ACSM), and he is certified by the ACSM as a clinical exercise physiologist. In addition to the ACSM and AACVPR, he is also an active member of the Clinical Exercise Physiology Association (CEPA), the American Heart Association, and the American College of Cardiology. Dr. Ehrman earned his PhD in clinical exercise physiology from The Ohio State University.
Dr. Ehrman is a coeditor of Clinical Exercise Physiology, Fourth Edition, and served as section editor of the 10th edition of ACSM's Resource Manual for Guidelines for Exercise Testing and Prescription. In addition, he has published more than 100 research manuscripts, abstracts, and book chapters. He is also the current editor of the Journal of Clinical Exercise Physiology, which is the official journal of the CEPA.
Dennis J. Kerrigan, PhD, FACSM, is a senior exercise physiologist in preventive cardiology in the Division of Cardiovascular Medicine and the William Clay Ford Center for Athletic Medicine at Henry Ford Hospital in Detroit, Michigan. His current role is as the director of outpatient exercise programs in preventive cardiology, and he oversees exercise programs for individuals with chronic health conditions. In addition to his clinical duties, Dr. Kerrigan also conducts research in patients with heart disease, cancer, and obesity. He was the lead author in a randomized trial that showed improvements in fitness and quality of life in patients with left ventricular assist devices who participated in cardiac rehabilitation. In 2017, Dr. Kerrigan was elected president of the Clinical Exercise Physiology Association (CEPA). He earned his PhD in clinical exercise physiology from The Ohio State University.
Dr. Kerrigan coauthored a book chapter in Guidelines for Cardiac Rehabilitation and Secondary Prevention Programs, Fifth Edition, and has published scholarly articles in peer-reviewed journals, including the Journal of Cardiopulmonary Rehabilitation and Prevention, American Journal of Cardiology, Journal of Cardiac Failure, and Medicine in Sports and Exercise. In 2012, he received the Midwest ACSM Clinical Exercise Professional of the Year award.
Steven J. Keteyian, PhD, FACSM, is the director of preventive cardiology in the Division of Cardiovascular Medicine and director of the Exercise Physiology Core Laboratory, both at the Henry Ford Hospital in Detroit. He specializes in clinical exercise physiology and preventive cardiology. He also serves as a clinical professor in the exercise science program at Oakland University and as an adjunct professor in the physiology department at Wayne State University, where he earned his PhD. He is an active member of the American Heart Association and the American Association of Cardiovascular and Pulmonary Rehabilitation (AACVPR).
Dr. Keteyian has published more than 200 research manuscripts aand book chapters and has coauthored or coedited four textbooks, including Clinical Exercise Physiology, Third Edition. He has also served as an editor-in-chief, associate editor, or editorial board member for several academic journals. Dr. Keteyian received the President's Award from the AACVPR in 2013 and the Established Investigator Award from the AACVPR in 2009.
Exercise Genomics
The rapidly expanding field of exercise genomics advances our understanding of the preventive and therapeutic properties of exercise by increasing our knowledge about the physiology of exercise and human behavior.
Contribution by Mark A. Sarzynski, PhD, University of South Carolina
The rapidly expanding field of exercise genomics advances our understanding of the preventive and therapeutic properties of exercise by increasing our knowledge about the physiology of exercise and human behavior. Although understanding the effects of various factors (e.g., environmental) on exercise-related phenotypes has long been of interest, understanding of the role of genetic factors (i.e., exercise genomics) is still in its infancy. Most of the major developments have occurred over the past 50 years. This section of the chapter does not have the capacity to fully review the field of genetics; therefore, the following sections introduce the basic concepts of genetics, deoxyribonucleic acid (DNA), and molecular biology relative to exercise physiology. A more thorough review on the topic can be found in Genetics Primer for Exercise Science and Health by Stephen M. Roth (2007).
Basics of Human Genetics
Genetics is the study of genes, heredity, and genetic variation in living organisms. The human genome, which contains all of the genetic material in human cells, consists of about 3 billion DNA base pairs. DNA encodes the instructions for the development, function, and reproduction of the entire human being. DNA is located in both the nucleus of the cell and the mitochondria, the majority of which is located in the nucleus. The nuclear genome comprises 22 pairs of autosomes (non-sex-specific chromosomes) and one pair of sex chromosomes for a total of 46 chromosomes. Humans inherit half of their genome from their mother (22 autosomes and an X chromosome) and half from their father (22 autosomes and either an X or Y chromosome). Women carry two copies of the X chromosome, whereas men carry one X chromosome and one Y chromosome. The presence or absence of the Y chromosome (responsible for testis development) determines the sex of the offspring.
Each DNA molecule consists of two complementary strands that each comprise four nucleotide bases - adenine (A), cytosine (C), guanine (G), and thymine (T) - that form a double helix. The binding between the two DNA strands is complementary: A always binds to T and C with G, creating complementary base pairs. The order of these nucleotide bases determines the meaning of the biological information encoded in that part of the DNA molecule. Specific sequences or regions of DNA that provide instructions to build ribonucleic acid (RNA) and proteins are called genes. Genes are the basic physical and functional units of heredity. The human genome contains about 20,500 genes. DNA found in the mitochondria is a circular double helix and contains 37 genes. The typical structure of a gene consists of many regions, including the coding region (exons), noncoding region (introns), promoter region (5'-end; upstream region; beginning of gene), and 3'-untranslated and terminator regions (3'-end; downstream region; end of gene; figure 11.2). The promoter region contains elements that direct the transcription of a gene (i.e., turn the gene on or off), whereas the terminator region contains the DNA sequence responsible for stopping the transcription of a gene.

The basic structure of a gene, including the upstream promoter region, the coding exons separated by introns, and the downstream terminator region at the end of the gene.
A central tenet of molecular biology describes the flow of information from DNA to RNA to proteins (figure 11.3). During the process of transcription, or gene expression, the nuclear DNA sequence found in a gene is read and copied onto a complementary strand of RNA called premature messenger RNA (mRNA) by the enzyme RNA polymerase. RNA is single stranded and contains the nucleotides A, G, C, and uracil (U), which replaces T and similarly binds only to A. Before the premature mRNA can be used to build protein, the noncoding regions of introns are removed, resulting in mature mRNA that consists of the coding exonic regions only. The mature mRNA then travels out of the nucleus and into the cell's cytoplasm, where it undergoes the process of translation. During translation, the genetic code is read by special organelles in the cell called ribosomes, which pair the mRNA to transfer RNA and eventually attach a corresponding amino acid to the polypeptide chain. Repetition of this step assembles a protein one amino acid at a time (figure 11.4). With just the four nucleotides used in three-letter combinations, the 20 standard amino acids are assembled.

The central principle of molecular biology, whereby DNA codes for RNA, which codes for proteins.
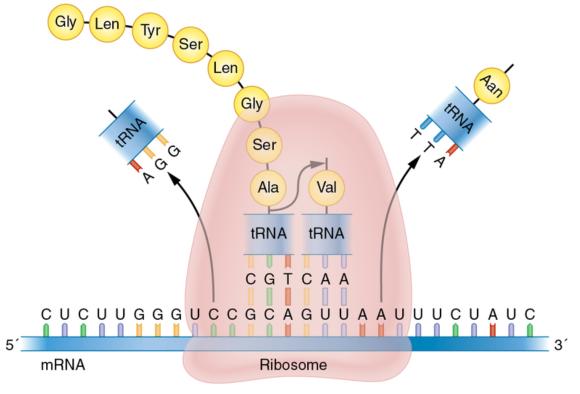
Overview of the translation of mRNA into protein. The ribosome binds to mRNA and moves one codon at a time downstream, where transfer RNA drops off an amino acid that links with the previous amino acid, thereby forming a polypeptide chain that continues until the ribosome reaches a stop codon.
Heritability and Genetic Variation
More than 99.9% of the DNA sequence in humans is similar. The 0.1% that differs is what makes each individual unique. Because family members share an even greater proportion of DNA sequence compared with unrelated individuals, analysis of familial aggregation (i.e., resemblance across family members) often is used to determine whether genetic variation contributes to a trait. For a given trait, familial aggregation is tested by comparing the variance between families with the variance within family members. For example, the HERITAGE Family Study examined the familial resemblance for maximal oxygen uptake (![]() O2max), the gold standard measure of cardiorespiratory fitness, in 426 sedentary subjects from 86 nuclear families. The authors found that achieved levels of
O2max), the gold standard measure of cardiorespiratory fitness, in 426 sedentary subjects from 86 nuclear families. The authors found that achieved levels of ![]() O2max clearly aggregate in families; there was 2.7 times more variance between different families than within families for adjusted
O2max clearly aggregate in families; there was 2.7 times more variance between different families than within families for adjusted ![]() O2max. Figure 11.5shows that some families tended to have below-average
O2max. Figure 11.5shows that some families tended to have below-average ![]() O2max values, whereas others had above-average values. Because families share genetic factors as well as similar environmental factors (e.g., diet, education, physical activity, and sedentary behaviors), further analyses are needed to determine whether the familial resemblance in
O2max values, whereas others had above-average values. Because families share genetic factors as well as similar environmental factors (e.g., diet, education, physical activity, and sedentary behaviors), further analyses are needed to determine whether the familial resemblance in ![]() O2max is due to genetic or environmental factors.
O2max is due to genetic or environmental factors.
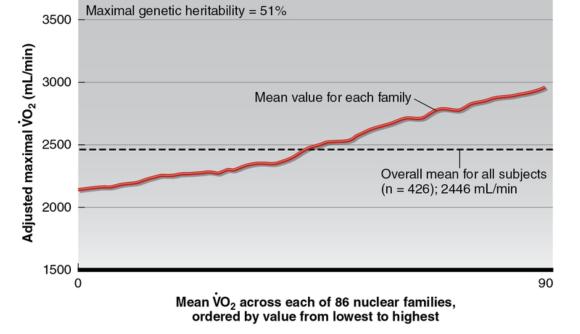
General depiction of familial aggregation for adjusted
Heritability is an estimate of how much of the variation in a trait is due to genetic factors alone. Heritability estimates are quantified by comparing trait similarities between pairs of relatives with different degrees of relatedness. Thus, twin, adoption, and family studies commonly are used to distinguish between the contribution of genetic and environmental factors on the familial aggregation of a trait. For example, a pattern of significant correlations among siblings and between parents and siblings but not between spouses would imply that the familial resemblance primarily is due to genetic factors, whereas significant correlations between spouses and lesser correlations between siblings or between parents and siblings would suggest a stronger influence of shared environmental factors such as diet and exercise habits. In the HERITAGE Family Study, the authors estimated that the genetic heritability of ![]() O2max was 51%. In addition to
O2max was 51%. In addition to ![]() O2max, numerous exercise-related traits have been shown to have a significant genetic component, as evidenced by their estimated heritability levels from twin and family studies (table 11.5).
O2max, numerous exercise-related traits have been shown to have a significant genetic component, as evidenced by their estimated heritability levels from twin and family studies (table 11.5).
After familial aggregation and heritability have been estimated for a trait, the next step is to determine which specific genetic factors contribute to the trait. Here, the term genetic factors refers to genetic variation or differences in the DNA sequence that may influence the information contained in a gene, thus resulting in trait variability between individuals. A variant nucleotide found at a mutation or polymorphism is known as an allele. Typically, two alleles are found at a polymorphism in the genome (e.g., A and G). Because genes come in pairs (one inherited from the mother and the other from the father), every individual has a pair of alleles for each mutation or polymorphism. The combination of alleles at any mutation or polymorphism is known as a genotype (i.e., that part of the genetic makeup that determines specific characteristics or phenotype). Thus, an individual may have either two copies of the same allele or one copy each of the variant allele. For example, if the nucleotides A and G are found at a particular polymorphism, an individual could have one of the following three genotypes: A/A, A/G, or G/G. An individual is a homozygote if they carry two copies of the same allele (e.g., A/A or G/G), whereas a heterozygote carries one of each allele (e.g., A/G). There are several forms of genetic variation, the most common of which is the single nucleotide polymorphism (SNP). An SNP is a single position in the DNA sequence where more than one nucleotide base is found in greater than 1% of the population. There are more than 10 million SNPs in the human genome. A mutation differs from a polymorphism in that the rare allele is found in less than 1% of the population.
Future Directions and Outlook
The field of exercise genomics has rapidly expanded over the past two decades with the advent of next-generation sequencing technologies, allowing for higher throughput and less expensive sequencing of common and rare variants. However, the field is mired by a general reliance on the candidate gene approach and observational studies with small sample sizes. Furthermore, lack of suitable replication studies or available DNA samples has made the replication of findings a difficult task, particularly for genome-wide studies. Thus, moving forward, exercise genomics needs to utilize a systems biology approach that integrates data from multiple technologies, including genomics, transcriptomics, metabolomics, proteomics, and epigenomics, among others. This will require large, well-designed, well-powered collaborative studies with replication from multiple sources along with the development of computational and bioinformatics tools and expertise within the field. Ultimately, identifying the genetic factors underlying the variability in health- and fitness-related traits due to regular exercise would significantly contribute to the study of the biology of adaptation to exercise and the development of an exercise component of personalized preventive and therapeutic medicine.
Save
Save
Save
Learn more about Advanced Exercise Physiology.
Anaerobic Testing
To accurately determine baseline status in order to guide exercise prescription development and determine whether adaptations occur in response to the exercise training stimulus, one needs to be able to precisely measure the variables of interest.
To accurately determine baseline status in order to guide exercise prescription development and determine whether adaptations occur in response to the exercise training stimulus, one needs to be able to precisely measure the variables of interest. Measures must be both repeatable and accurate (i.e., valid). To attain valid measures, the testing methods used must be performed according to specific guidelines with respect to
- the subject's preparation (e.g., meals, rest, prior exercise, time of day),
- equipment use (e.g., appropriateness of equipment for measuring variables of interest, maintenance, calibration),
- implementation according to testing guidelines applied by the individual conducting the test, and
- proper interpretation of the test results.
Typical variables of interest in anaerobic performance assessment are anaerobic power and anaerobic capacity. Anaerobic power is important for sprint, mid-distance, and distance athletes but for varying reasons. For most athletic events, there is interplay between the aerobic and anaerobic energy systems. Referring to figure 7.1, we see that sprinters (events lasting 4 min) predominantly utilize aerobic metabolic sources. Even aerobic athletes must rely on anaerobic sources at critical times of an event, such as during a hill climb in a bicycle race or the final sprint of a 10K running race.
No direct method of determining anaerobic energy power and capacity currently exists. Although blood lactate accumulation generally is considered to be the product of a high rate of anaerobic glycolysis, blood lactate concentration measurement does not provide specific information about the rate and capacity of the production of ATP. Additionally, the concentration of blood lactate is affected by the rate of its clearance, which differs in individuals due to factors such as - but not limited to - recovery activity status (i.e., active vs. passive); recovery exercise intensity; ratio of individual Type I to Type II skeletal muscle fiber composition; the rate of blood flow to the skeletal muscles, heart, and liver (Cori cycle); and the rate of release of muscle lactate into the blood.
The following is a comprehensive list of common anaerobic tests. The test to be utilized must be specific to the variable being measured. For instance, to measure maximal anaerobic muscle power, a test needs to be very short in duration to isolate the ATP-PCr energy system. Maximal muscle power is used in activities such as jumping and throwing. A vertical jump test is a good example of a short-duration muscle power test. Speed often is thought of as a useful measure, and the 40-yd (36.6 m) dash is used by the National Football League (NFL) to measure speed and provide a ranking of potential draftees. However, a 40-yd dash technically assesses acceleration, velocity, and average speed. The top speed is the fastest instantaneous rate of an object in motion while the average speed is the distance divided by the time to cover that distance. Velocity includes the component of direction of movement; thus, speed is the magnitude component of velocity. NSCA's Guide to Tests and Assessments (Human Kinetics, 2012) provides an excellent review of the performance of anaerobic tests.
Anaerobic Tests
- Vertical jump test
- Margaria-Kalamen power test
- Modified Margaria-Kalamen power test (also known as the football staircase test)
- Three Modified Box Long Jump (MBLJ) test
- Wingate Anaerobic Test (WAnT)
- Critical power test
Various studies have determined that each test in the list is a valid measure of anaerobic power. In particular, the vertical jump test, standing long jump test, Margaria-Kalamen power test, Modified Margaria-Kalamen power test, and three modified box long jump test are considered to be the most sport specific of these tests. The following sections briefly discuss and provide directions for performing several of these anaerobic tests.
Vertical Jump Test
The vertical jump test is commonly used by coaches to measure lower body power and to test an athlete's jumping ability. Previous investigations determined that the vertical jump has high predictive value for measuring power production for athletes participating in such sports as track and field, weightlifting, volleyball, basketball, and football. To test the vertical jump, schools, organizations, and sport teams commonly use a commercially designed device consisting of plastic swivel vanes placed in 0.5-in. (12.7 cm) increments. Because the athlete uses countermovement of the lower body and an outstretched arm swing to reach the highest vane, the vertical jump test is also known as the jump and reach test.
As an example of the sophistication that can be developed for simple tests such as the vertical jump, consider the following. Some researchers believe that the gold standard for measuring the vertical jump includes implementing video analysis and using biomechanical reflective markers on the hip to measure the displacement of the center of mass. Although valid and reliable, this method is cost prohibitive for many fitness and sport organizations. A commercial jump mat is another device used to measure the vertical jump. Embedded in the mat are microswitches that determine flight time - that is, the interval between the liftoff and landing of both feet during a countermovement from a flat-footed standing position. The flight time in the air is used to compute the subject's vertical jump. A study by García-López et al. using three countermovement jumps found that jump mats designed with photo cells showed higher correlations with force plate technologies compared with a contact jump mat. Similarly, Whitmer et al. determined that practitioners using a contact jump mat may underestimate the vertical jump for high performers. A promising new technology for measuring vertical jump is the Myotest (Myotest Inc., Switzerland). The Myotest device is approximately the size of a small smartphone, and the subject wears the device on the hip to determine the displacement of the center of mass. This test does not require the subject to reach and stretch with one arm to displace vanes like when using a vane jump test device. A study by Nuzzo et al. found that the Myotest demonstrated the best intrasession reliability for measuring a countermovement vertical jump when compared with the vane jump test device and jump mat system.

Vertical jump test.
Procedures for the Vertical Jump Test
- Before the test: To measure the highest standing reach, instruct the subject to stand flat footed and reach with one arm fully extended. This should be the same arm that will extend and displace the vanes. Then measure again during plantar flexion with the same arm extended and during plantar flexion. Measure the subject's reach at the middle finger. This measure will be subtracted from the highest recorded vertical jump value.
- During the test: Instruct the subject to take a vertical jump from a standing position using a countermovement. The subject should squat down and back while simultaneously using a bilateral backward arm swing. The subject should then explode upward by extending the hips, knees, ankles (also known as the triple extension), shoulders, elbows, and wrists and attempt to displace the highest vane with one arm (see figure 7.2). Alternatively, a wall-mounted jump-and-reach board may be used.
- Obtain the measurement and repeat two more times. Instruct the subject to rest for 30 s between trials.
- Calculate the maximum vertical jump by subtracting the highest standing reach from the highest vane displaced during the three vertical jumps.
Learn more about Advanced Exercise Physiology.
Using Body Composition Methods to Identify Cachexia in Cancer Patients
Cachexia is not simply weight loss. In some cancer populations, such as patients with early-stage breast cancer, weight gain is actually a more common occurrence that is associated with poor prognosis.
Cachexia is not simply weight loss. In some cancer populations, such as patients with early-stage breast cancer, weight gain is actually a more common occurrence that is associated with poor prognosis. Cachexia is a metabolic syndrome linked to an underlying condition (e.g., cancer, heart failure) that results in the loss of muscle with or without fat that impairs function. Although the mechanisms that lead to cachexia are not fully understood, one factor that differentiates itself from sarcopenia (see "Body Composition and Weight Management Across the Life Span") is an increase in metabolic rate. This increased metabolic rate may be attributable to the cancer tumor itself, especially when the cancer cells spread to metabolically active tissue. An example of this was seen inpatients with colorectal cancer, where an increase in liver mass due to metastatic cancer cells was associated with a concurrent decrease in total muscle mass. Regardless of what triggers the increased metabolic rate, the end result is increased muscle catabolism, which places the cancer patient at higher risk of early death.
One misconception about cachexia is that obese individuals are somehow protected because of increased energy reserves. Although the obesity paradox suggests a protective effect with increases in certain cancer populations (e.g., individuals undergoing chemotherapy), in general BMI does a poor job of classifying those patients with a high mortality risk. The obvious reason why is the inability of BMI to differentiate FFM from FM. Using a bioelectrical impedance analysis, Gonzalez et al. showed that FFM index (i.e., FFM divided by the square of height) was a better predictor of mortality regardless of how much FM was present. In other words, it did not matter if a patient's BMI was higher or lower; if the patient had a reduced amount of muscle mass, the risk of death was increased.
The clinical implications for measuring FM and FFM become evident if you compare two obese patients, one with cachexia and one without. Both patients lose 20 lb (9.1 kg) after a diagnosis of cancer. Using body composition methods, a clinician can identify the higher risk patient. Methods such as the CT measurement of lumbar skeletal muscle currently are being used, although unfortunately not widely. Regardless, the identification of cachexia is one potential area where knowledge of body composition methods can be invaluable.
Learn more about Advanced Exercise Physiology.
Exercise Genomics
The rapidly expanding field of exercise genomics advances our understanding of the preventive and therapeutic properties of exercise by increasing our knowledge about the physiology of exercise and human behavior.
Contribution by Mark A. Sarzynski, PhD, University of South Carolina
The rapidly expanding field of exercise genomics advances our understanding of the preventive and therapeutic properties of exercise by increasing our knowledge about the physiology of exercise and human behavior. Although understanding the effects of various factors (e.g., environmental) on exercise-related phenotypes has long been of interest, understanding of the role of genetic factors (i.e., exercise genomics) is still in its infancy. Most of the major developments have occurred over the past 50 years. This section of the chapter does not have the capacity to fully review the field of genetics; therefore, the following sections introduce the basic concepts of genetics, deoxyribonucleic acid (DNA), and molecular biology relative to exercise physiology. A more thorough review on the topic can be found in Genetics Primer for Exercise Science and Health by Stephen M. Roth (2007).
Basics of Human Genetics
Genetics is the study of genes, heredity, and genetic variation in living organisms. The human genome, which contains all of the genetic material in human cells, consists of about 3 billion DNA base pairs. DNA encodes the instructions for the development, function, and reproduction of the entire human being. DNA is located in both the nucleus of the cell and the mitochondria, the majority of which is located in the nucleus. The nuclear genome comprises 22 pairs of autosomes (non-sex-specific chromosomes) and one pair of sex chromosomes for a total of 46 chromosomes. Humans inherit half of their genome from their mother (22 autosomes and an X chromosome) and half from their father (22 autosomes and either an X or Y chromosome). Women carry two copies of the X chromosome, whereas men carry one X chromosome and one Y chromosome. The presence or absence of the Y chromosome (responsible for testis development) determines the sex of the offspring.
Each DNA molecule consists of two complementary strands that each comprise four nucleotide bases - adenine (A), cytosine (C), guanine (G), and thymine (T) - that form a double helix. The binding between the two DNA strands is complementary: A always binds to T and C with G, creating complementary base pairs. The order of these nucleotide bases determines the meaning of the biological information encoded in that part of the DNA molecule. Specific sequences or regions of DNA that provide instructions to build ribonucleic acid (RNA) and proteins are called genes. Genes are the basic physical and functional units of heredity. The human genome contains about 20,500 genes. DNA found in the mitochondria is a circular double helix and contains 37 genes. The typical structure of a gene consists of many regions, including the coding region (exons), noncoding region (introns), promoter region (5'-end; upstream region; beginning of gene), and 3'-untranslated and terminator regions (3'-end; downstream region; end of gene; figure 11.2). The promoter region contains elements that direct the transcription of a gene (i.e., turn the gene on or off), whereas the terminator region contains the DNA sequence responsible for stopping the transcription of a gene.
The basic structure of a gene, including the upstream promoter region, the coding exons separated by introns, and the downstream terminator region at the end of the gene.
A central tenet of molecular biology describes the flow of information from DNA to RNA to proteins (figure 11.3). During the process of transcription, or gene expression, the nuclear DNA sequence found in a gene is read and copied onto a complementary strand of RNA called premature messenger RNA (mRNA) by the enzyme RNA polymerase. RNA is single stranded and contains the nucleotides A, G, C, and uracil (U), which replaces T and similarly binds only to A. Before the premature mRNA can be used to build protein, the noncoding regions of introns are removed, resulting in mature mRNA that consists of the coding exonic regions only. The mature mRNA then travels out of the nucleus and into the cell's cytoplasm, where it undergoes the process of translation. During translation, the genetic code is read by special organelles in the cell called ribosomes, which pair the mRNA to transfer RNA and eventually attach a corresponding amino acid to the polypeptide chain. Repetition of this step assembles a protein one amino acid at a time (figure 11.4). With just the four nucleotides used in three-letter combinations, the 20 standard amino acids are assembled.
The central principle of molecular biology, whereby DNA codes for RNA, which codes for proteins.
Overview of the translation of mRNA into protein. The ribosome binds to mRNA and moves one codon at a time downstream, where transfer RNA drops off an amino acid that links with the previous amino acid, thereby forming a polypeptide chain that continues until the ribosome reaches a stop codon.
Heritability and Genetic Variation
More than 99.9% of the DNA sequence in humans is similar. The 0.1% that differs is what makes each individual unique. Because family members share an even greater proportion of DNA sequence compared with unrelated individuals, analysis of familial aggregation (i.e., resemblance across family members) often is used to determine whether genetic variation contributes to a trait. For a given trait, familial aggregation is tested by comparing the variance between families with the variance within family members. For example, the HERITAGE Family Study examined the familial resemblance for maximal oxygen uptake (![]() O2max), the gold standard measure of cardiorespiratory fitness, in 426 sedentary subjects from 86 nuclear families. The authors found that achieved levels of
O2max), the gold standard measure of cardiorespiratory fitness, in 426 sedentary subjects from 86 nuclear families. The authors found that achieved levels of ![]() O2max clearly aggregate in families; there was 2.7 times more variance between different families than within families for adjusted
O2max clearly aggregate in families; there was 2.7 times more variance between different families than within families for adjusted ![]() O2max. Figure 11.5shows that some families tended to have below-average
O2max. Figure 11.5shows that some families tended to have below-average ![]() O2max values, whereas others had above-average values. Because families share genetic factors as well as similar environmental factors (e.g., diet, education, physical activity, and sedentary behaviors), further analyses are needed to determine whether the familial resemblance in
O2max values, whereas others had above-average values. Because families share genetic factors as well as similar environmental factors (e.g., diet, education, physical activity, and sedentary behaviors), further analyses are needed to determine whether the familial resemblance in ![]() O2max is due to genetic or environmental factors.
O2max is due to genetic or environmental factors.
General depiction of familial aggregation for adjusted
Heritability is an estimate of how much of the variation in a trait is due to genetic factors alone. Heritability estimates are quantified by comparing trait similarities between pairs of relatives with different degrees of relatedness. Thus, twin, adoption, and family studies commonly are used to distinguish between the contribution of genetic and environmental factors on the familial aggregation of a trait. For example, a pattern of significant correlations among siblings and between parents and siblings but not between spouses would imply that the familial resemblance primarily is due to genetic factors, whereas significant correlations between spouses and lesser correlations between siblings or between parents and siblings would suggest a stronger influence of shared environmental factors such as diet and exercise habits. In the HERITAGE Family Study, the authors estimated that the genetic heritability of ![]() O2max was 51%. In addition to
O2max was 51%. In addition to ![]() O2max, numerous exercise-related traits have been shown to have a significant genetic component, as evidenced by their estimated heritability levels from twin and family studies (table 11.5).
O2max, numerous exercise-related traits have been shown to have a significant genetic component, as evidenced by their estimated heritability levels from twin and family studies (table 11.5).
After familial aggregation and heritability have been estimated for a trait, the next step is to determine which specific genetic factors contribute to the trait. Here, the term genetic factors refers to genetic variation or differences in the DNA sequence that may influence the information contained in a gene, thus resulting in trait variability between individuals. A variant nucleotide found at a mutation or polymorphism is known as an allele. Typically, two alleles are found at a polymorphism in the genome (e.g., A and G). Because genes come in pairs (one inherited from the mother and the other from the father), every individual has a pair of alleles for each mutation or polymorphism. The combination of alleles at any mutation or polymorphism is known as a genotype (i.e., that part of the genetic makeup that determines specific characteristics or phenotype). Thus, an individual may have either two copies of the same allele or one copy each of the variant allele. For example, if the nucleotides A and G are found at a particular polymorphism, an individual could have one of the following three genotypes: A/A, A/G, or G/G. An individual is a homozygote if they carry two copies of the same allele (e.g., A/A or G/G), whereas a heterozygote carries one of each allele (e.g., A/G). There are several forms of genetic variation, the most common of which is the single nucleotide polymorphism (SNP). An SNP is a single position in the DNA sequence where more than one nucleotide base is found in greater than 1% of the population. There are more than 10 million SNPs in the human genome. A mutation differs from a polymorphism in that the rare allele is found in less than 1% of the population.
Future Directions and Outlook
The field of exercise genomics has rapidly expanded over the past two decades with the advent of next-generation sequencing technologies, allowing for higher throughput and less expensive sequencing of common and rare variants. However, the field is mired by a general reliance on the candidate gene approach and observational studies with small sample sizes. Furthermore, lack of suitable replication studies or available DNA samples has made the replication of findings a difficult task, particularly for genome-wide studies. Thus, moving forward, exercise genomics needs to utilize a systems biology approach that integrates data from multiple technologies, including genomics, transcriptomics, metabolomics, proteomics, and epigenomics, among others. This will require large, well-designed, well-powered collaborative studies with replication from multiple sources along with the development of computational and bioinformatics tools and expertise within the field. Ultimately, identifying the genetic factors underlying the variability in health- and fitness-related traits due to regular exercise would significantly contribute to the study of the biology of adaptation to exercise and the development of an exercise component of personalized preventive and therapeutic medicine.
Save
Save
Save
Learn more about Advanced Exercise Physiology.
Anaerobic Testing
To accurately determine baseline status in order to guide exercise prescription development and determine whether adaptations occur in response to the exercise training stimulus, one needs to be able to precisely measure the variables of interest.
To accurately determine baseline status in order to guide exercise prescription development and determine whether adaptations occur in response to the exercise training stimulus, one needs to be able to precisely measure the variables of interest. Measures must be both repeatable and accurate (i.e., valid). To attain valid measures, the testing methods used must be performed according to specific guidelines with respect to
- the subject's preparation (e.g., meals, rest, prior exercise, time of day),
- equipment use (e.g., appropriateness of equipment for measuring variables of interest, maintenance, calibration),
- implementation according to testing guidelines applied by the individual conducting the test, and
- proper interpretation of the test results.
Typical variables of interest in anaerobic performance assessment are anaerobic power and anaerobic capacity. Anaerobic power is important for sprint, mid-distance, and distance athletes but for varying reasons. For most athletic events, there is interplay between the aerobic and anaerobic energy systems. Referring to figure 7.1, we see that sprinters (events lasting 4 min) predominantly utilize aerobic metabolic sources. Even aerobic athletes must rely on anaerobic sources at critical times of an event, such as during a hill climb in a bicycle race or the final sprint of a 10K running race.
No direct method of determining anaerobic energy power and capacity currently exists. Although blood lactate accumulation generally is considered to be the product of a high rate of anaerobic glycolysis, blood lactate concentration measurement does not provide specific information about the rate and capacity of the production of ATP. Additionally, the concentration of blood lactate is affected by the rate of its clearance, which differs in individuals due to factors such as - but not limited to - recovery activity status (i.e., active vs. passive); recovery exercise intensity; ratio of individual Type I to Type II skeletal muscle fiber composition; the rate of blood flow to the skeletal muscles, heart, and liver (Cori cycle); and the rate of release of muscle lactate into the blood.
The following is a comprehensive list of common anaerobic tests. The test to be utilized must be specific to the variable being measured. For instance, to measure maximal anaerobic muscle power, a test needs to be very short in duration to isolate the ATP-PCr energy system. Maximal muscle power is used in activities such as jumping and throwing. A vertical jump test is a good example of a short-duration muscle power test. Speed often is thought of as a useful measure, and the 40-yd (36.6 m) dash is used by the National Football League (NFL) to measure speed and provide a ranking of potential draftees. However, a 40-yd dash technically assesses acceleration, velocity, and average speed. The top speed is the fastest instantaneous rate of an object in motion while the average speed is the distance divided by the time to cover that distance. Velocity includes the component of direction of movement; thus, speed is the magnitude component of velocity. NSCA's Guide to Tests and Assessments (Human Kinetics, 2012) provides an excellent review of the performance of anaerobic tests.
Anaerobic Tests
- Vertical jump test
- Margaria-Kalamen power test
- Modified Margaria-Kalamen power test (also known as the football staircase test)
- Three Modified Box Long Jump (MBLJ) test
- Wingate Anaerobic Test (WAnT)
- Critical power test
Various studies have determined that each test in the list is a valid measure of anaerobic power. In particular, the vertical jump test, standing long jump test, Margaria-Kalamen power test, Modified Margaria-Kalamen power test, and three modified box long jump test are considered to be the most sport specific of these tests. The following sections briefly discuss and provide directions for performing several of these anaerobic tests.
Vertical Jump Test
The vertical jump test is commonly used by coaches to measure lower body power and to test an athlete's jumping ability. Previous investigations determined that the vertical jump has high predictive value for measuring power production for athletes participating in such sports as track and field, weightlifting, volleyball, basketball, and football. To test the vertical jump, schools, organizations, and sport teams commonly use a commercially designed device consisting of plastic swivel vanes placed in 0.5-in. (12.7 cm) increments. Because the athlete uses countermovement of the lower body and an outstretched arm swing to reach the highest vane, the vertical jump test is also known as the jump and reach test.
As an example of the sophistication that can be developed for simple tests such as the vertical jump, consider the following. Some researchers believe that the gold standard for measuring the vertical jump includes implementing video analysis and using biomechanical reflective markers on the hip to measure the displacement of the center of mass. Although valid and reliable, this method is cost prohibitive for many fitness and sport organizations. A commercial jump mat is another device used to measure the vertical jump. Embedded in the mat are microswitches that determine flight time - that is, the interval between the liftoff and landing of both feet during a countermovement from a flat-footed standing position. The flight time in the air is used to compute the subject's vertical jump. A study by García-López et al. using three countermovement jumps found that jump mats designed with photo cells showed higher correlations with force plate technologies compared with a contact jump mat. Similarly, Whitmer et al. determined that practitioners using a contact jump mat may underestimate the vertical jump for high performers. A promising new technology for measuring vertical jump is the Myotest (Myotest Inc., Switzerland). The Myotest device is approximately the size of a small smartphone, and the subject wears the device on the hip to determine the displacement of the center of mass. This test does not require the subject to reach and stretch with one arm to displace vanes like when using a vane jump test device. A study by Nuzzo et al. found that the Myotest demonstrated the best intrasession reliability for measuring a countermovement vertical jump when compared with the vane jump test device and jump mat system.
Vertical jump test.
Procedures for the Vertical Jump Test
- Before the test: To measure the highest standing reach, instruct the subject to stand flat footed and reach with one arm fully extended. This should be the same arm that will extend and displace the vanes. Then measure again during plantar flexion with the same arm extended and during plantar flexion. Measure the subject's reach at the middle finger. This measure will be subtracted from the highest recorded vertical jump value.
- During the test: Instruct the subject to take a vertical jump from a standing position using a countermovement. The subject should squat down and back while simultaneously using a bilateral backward arm swing. The subject should then explode upward by extending the hips, knees, ankles (also known as the triple extension), shoulders, elbows, and wrists and attempt to displace the highest vane with one arm (see figure 7.2). Alternatively, a wall-mounted jump-and-reach board may be used.
- Obtain the measurement and repeat two more times. Instruct the subject to rest for 30 s between trials.
- Calculate the maximum vertical jump by subtracting the highest standing reach from the highest vane displaced during the three vertical jumps.
Learn more about Advanced Exercise Physiology.
Using Body Composition Methods to Identify Cachexia in Cancer Patients
Cachexia is not simply weight loss. In some cancer populations, such as patients with early-stage breast cancer, weight gain is actually a more common occurrence that is associated with poor prognosis.
Cachexia is not simply weight loss. In some cancer populations, such as patients with early-stage breast cancer, weight gain is actually a more common occurrence that is associated with poor prognosis. Cachexia is a metabolic syndrome linked to an underlying condition (e.g., cancer, heart failure) that results in the loss of muscle with or without fat that impairs function. Although the mechanisms that lead to cachexia are not fully understood, one factor that differentiates itself from sarcopenia (see "Body Composition and Weight Management Across the Life Span") is an increase in metabolic rate. This increased metabolic rate may be attributable to the cancer tumor itself, especially when the cancer cells spread to metabolically active tissue. An example of this was seen inpatients with colorectal cancer, where an increase in liver mass due to metastatic cancer cells was associated with a concurrent decrease in total muscle mass. Regardless of what triggers the increased metabolic rate, the end result is increased muscle catabolism, which places the cancer patient at higher risk of early death.
One misconception about cachexia is that obese individuals are somehow protected because of increased energy reserves. Although the obesity paradox suggests a protective effect with increases in certain cancer populations (e.g., individuals undergoing chemotherapy), in general BMI does a poor job of classifying those patients with a high mortality risk. The obvious reason why is the inability of BMI to differentiate FFM from FM. Using a bioelectrical impedance analysis, Gonzalez et al. showed that FFM index (i.e., FFM divided by the square of height) was a better predictor of mortality regardless of how much FM was present. In other words, it did not matter if a patient's BMI was higher or lower; if the patient had a reduced amount of muscle mass, the risk of death was increased.
The clinical implications for measuring FM and FFM become evident if you compare two obese patients, one with cachexia and one without. Both patients lose 20 lb (9.1 kg) after a diagnosis of cancer. Using body composition methods, a clinician can identify the higher risk patient. Methods such as the CT measurement of lumbar skeletal muscle currently are being used, although unfortunately not widely. Regardless, the identification of cachexia is one potential area where knowledge of body composition methods can be invaluable.
Learn more about Advanced Exercise Physiology.
Exercise Genomics
The rapidly expanding field of exercise genomics advances our understanding of the preventive and therapeutic properties of exercise by increasing our knowledge about the physiology of exercise and human behavior.
Contribution by Mark A. Sarzynski, PhD, University of South Carolina
The rapidly expanding field of exercise genomics advances our understanding of the preventive and therapeutic properties of exercise by increasing our knowledge about the physiology of exercise and human behavior. Although understanding the effects of various factors (e.g., environmental) on exercise-related phenotypes has long been of interest, understanding of the role of genetic factors (i.e., exercise genomics) is still in its infancy. Most of the major developments have occurred over the past 50 years. This section of the chapter does not have the capacity to fully review the field of genetics; therefore, the following sections introduce the basic concepts of genetics, deoxyribonucleic acid (DNA), and molecular biology relative to exercise physiology. A more thorough review on the topic can be found in Genetics Primer for Exercise Science and Health by Stephen M. Roth (2007).
Basics of Human Genetics
Genetics is the study of genes, heredity, and genetic variation in living organisms. The human genome, which contains all of the genetic material in human cells, consists of about 3 billion DNA base pairs. DNA encodes the instructions for the development, function, and reproduction of the entire human being. DNA is located in both the nucleus of the cell and the mitochondria, the majority of which is located in the nucleus. The nuclear genome comprises 22 pairs of autosomes (non-sex-specific chromosomes) and one pair of sex chromosomes for a total of 46 chromosomes. Humans inherit half of their genome from their mother (22 autosomes and an X chromosome) and half from their father (22 autosomes and either an X or Y chromosome). Women carry two copies of the X chromosome, whereas men carry one X chromosome and one Y chromosome. The presence or absence of the Y chromosome (responsible for testis development) determines the sex of the offspring.
Each DNA molecule consists of two complementary strands that each comprise four nucleotide bases - adenine (A), cytosine (C), guanine (G), and thymine (T) - that form a double helix. The binding between the two DNA strands is complementary: A always binds to T and C with G, creating complementary base pairs. The order of these nucleotide bases determines the meaning of the biological information encoded in that part of the DNA molecule. Specific sequences or regions of DNA that provide instructions to build ribonucleic acid (RNA) and proteins are called genes. Genes are the basic physical and functional units of heredity. The human genome contains about 20,500 genes. DNA found in the mitochondria is a circular double helix and contains 37 genes. The typical structure of a gene consists of many regions, including the coding region (exons), noncoding region (introns), promoter region (5'-end; upstream region; beginning of gene), and 3'-untranslated and terminator regions (3'-end; downstream region; end of gene; figure 11.2). The promoter region contains elements that direct the transcription of a gene (i.e., turn the gene on or off), whereas the terminator region contains the DNA sequence responsible for stopping the transcription of a gene.
The basic structure of a gene, including the upstream promoter region, the coding exons separated by introns, and the downstream terminator region at the end of the gene.
A central tenet of molecular biology describes the flow of information from DNA to RNA to proteins (figure 11.3). During the process of transcription, or gene expression, the nuclear DNA sequence found in a gene is read and copied onto a complementary strand of RNA called premature messenger RNA (mRNA) by the enzyme RNA polymerase. RNA is single stranded and contains the nucleotides A, G, C, and uracil (U), which replaces T and similarly binds only to A. Before the premature mRNA can be used to build protein, the noncoding regions of introns are removed, resulting in mature mRNA that consists of the coding exonic regions only. The mature mRNA then travels out of the nucleus and into the cell's cytoplasm, where it undergoes the process of translation. During translation, the genetic code is read by special organelles in the cell called ribosomes, which pair the mRNA to transfer RNA and eventually attach a corresponding amino acid to the polypeptide chain. Repetition of this step assembles a protein one amino acid at a time (figure 11.4). With just the four nucleotides used in three-letter combinations, the 20 standard amino acids are assembled.
The central principle of molecular biology, whereby DNA codes for RNA, which codes for proteins.
Overview of the translation of mRNA into protein. The ribosome binds to mRNA and moves one codon at a time downstream, where transfer RNA drops off an amino acid that links with the previous amino acid, thereby forming a polypeptide chain that continues until the ribosome reaches a stop codon.
Heritability and Genetic Variation
More than 99.9% of the DNA sequence in humans is similar. The 0.1% that differs is what makes each individual unique. Because family members share an even greater proportion of DNA sequence compared with unrelated individuals, analysis of familial aggregation (i.e., resemblance across family members) often is used to determine whether genetic variation contributes to a trait. For a given trait, familial aggregation is tested by comparing the variance between families with the variance within family members. For example, the HERITAGE Family Study examined the familial resemblance for maximal oxygen uptake (![]() O2max), the gold standard measure of cardiorespiratory fitness, in 426 sedentary subjects from 86 nuclear families. The authors found that achieved levels of
O2max), the gold standard measure of cardiorespiratory fitness, in 426 sedentary subjects from 86 nuclear families. The authors found that achieved levels of ![]() O2max clearly aggregate in families; there was 2.7 times more variance between different families than within families for adjusted
O2max clearly aggregate in families; there was 2.7 times more variance between different families than within families for adjusted ![]() O2max. Figure 11.5shows that some families tended to have below-average
O2max. Figure 11.5shows that some families tended to have below-average ![]() O2max values, whereas others had above-average values. Because families share genetic factors as well as similar environmental factors (e.g., diet, education, physical activity, and sedentary behaviors), further analyses are needed to determine whether the familial resemblance in
O2max values, whereas others had above-average values. Because families share genetic factors as well as similar environmental factors (e.g., diet, education, physical activity, and sedentary behaviors), further analyses are needed to determine whether the familial resemblance in ![]() O2max is due to genetic or environmental factors.
O2max is due to genetic or environmental factors.
General depiction of familial aggregation for adjusted
Heritability is an estimate of how much of the variation in a trait is due to genetic factors alone. Heritability estimates are quantified by comparing trait similarities between pairs of relatives with different degrees of relatedness. Thus, twin, adoption, and family studies commonly are used to distinguish between the contribution of genetic and environmental factors on the familial aggregation of a trait. For example, a pattern of significant correlations among siblings and between parents and siblings but not between spouses would imply that the familial resemblance primarily is due to genetic factors, whereas significant correlations between spouses and lesser correlations between siblings or between parents and siblings would suggest a stronger influence of shared environmental factors such as diet and exercise habits. In the HERITAGE Family Study, the authors estimated that the genetic heritability of ![]() O2max was 51%. In addition to
O2max was 51%. In addition to ![]() O2max, numerous exercise-related traits have been shown to have a significant genetic component, as evidenced by their estimated heritability levels from twin and family studies (table 11.5).
O2max, numerous exercise-related traits have been shown to have a significant genetic component, as evidenced by their estimated heritability levels from twin and family studies (table 11.5).
After familial aggregation and heritability have been estimated for a trait, the next step is to determine which specific genetic factors contribute to the trait. Here, the term genetic factors refers to genetic variation or differences in the DNA sequence that may influence the information contained in a gene, thus resulting in trait variability between individuals. A variant nucleotide found at a mutation or polymorphism is known as an allele. Typically, two alleles are found at a polymorphism in the genome (e.g., A and G). Because genes come in pairs (one inherited from the mother and the other from the father), every individual has a pair of alleles for each mutation or polymorphism. The combination of alleles at any mutation or polymorphism is known as a genotype (i.e., that part of the genetic makeup that determines specific characteristics or phenotype). Thus, an individual may have either two copies of the same allele or one copy each of the variant allele. For example, if the nucleotides A and G are found at a particular polymorphism, an individual could have one of the following three genotypes: A/A, A/G, or G/G. An individual is a homozygote if they carry two copies of the same allele (e.g., A/A or G/G), whereas a heterozygote carries one of each allele (e.g., A/G). There are several forms of genetic variation, the most common of which is the single nucleotide polymorphism (SNP). An SNP is a single position in the DNA sequence where more than one nucleotide base is found in greater than 1% of the population. There are more than 10 million SNPs in the human genome. A mutation differs from a polymorphism in that the rare allele is found in less than 1% of the population.
Future Directions and Outlook
The field of exercise genomics has rapidly expanded over the past two decades with the advent of next-generation sequencing technologies, allowing for higher throughput and less expensive sequencing of common and rare variants. However, the field is mired by a general reliance on the candidate gene approach and observational studies with small sample sizes. Furthermore, lack of suitable replication studies or available DNA samples has made the replication of findings a difficult task, particularly for genome-wide studies. Thus, moving forward, exercise genomics needs to utilize a systems biology approach that integrates data from multiple technologies, including genomics, transcriptomics, metabolomics, proteomics, and epigenomics, among others. This will require large, well-designed, well-powered collaborative studies with replication from multiple sources along with the development of computational and bioinformatics tools and expertise within the field. Ultimately, identifying the genetic factors underlying the variability in health- and fitness-related traits due to regular exercise would significantly contribute to the study of the biology of adaptation to exercise and the development of an exercise component of personalized preventive and therapeutic medicine.
Save
Save
Save
Learn more about Advanced Exercise Physiology.
Anaerobic Testing
To accurately determine baseline status in order to guide exercise prescription development and determine whether adaptations occur in response to the exercise training stimulus, one needs to be able to precisely measure the variables of interest.
To accurately determine baseline status in order to guide exercise prescription development and determine whether adaptations occur in response to the exercise training stimulus, one needs to be able to precisely measure the variables of interest. Measures must be both repeatable and accurate (i.e., valid). To attain valid measures, the testing methods used must be performed according to specific guidelines with respect to
- the subject's preparation (e.g., meals, rest, prior exercise, time of day),
- equipment use (e.g., appropriateness of equipment for measuring variables of interest, maintenance, calibration),
- implementation according to testing guidelines applied by the individual conducting the test, and
- proper interpretation of the test results.
Typical variables of interest in anaerobic performance assessment are anaerobic power and anaerobic capacity. Anaerobic power is important for sprint, mid-distance, and distance athletes but for varying reasons. For most athletic events, there is interplay between the aerobic and anaerobic energy systems. Referring to figure 7.1, we see that sprinters (events lasting 4 min) predominantly utilize aerobic metabolic sources. Even aerobic athletes must rely on anaerobic sources at critical times of an event, such as during a hill climb in a bicycle race or the final sprint of a 10K running race.
No direct method of determining anaerobic energy power and capacity currently exists. Although blood lactate accumulation generally is considered to be the product of a high rate of anaerobic glycolysis, blood lactate concentration measurement does not provide specific information about the rate and capacity of the production of ATP. Additionally, the concentration of blood lactate is affected by the rate of its clearance, which differs in individuals due to factors such as - but not limited to - recovery activity status (i.e., active vs. passive); recovery exercise intensity; ratio of individual Type I to Type II skeletal muscle fiber composition; the rate of blood flow to the skeletal muscles, heart, and liver (Cori cycle); and the rate of release of muscle lactate into the blood.
The following is a comprehensive list of common anaerobic tests. The test to be utilized must be specific to the variable being measured. For instance, to measure maximal anaerobic muscle power, a test needs to be very short in duration to isolate the ATP-PCr energy system. Maximal muscle power is used in activities such as jumping and throwing. A vertical jump test is a good example of a short-duration muscle power test. Speed often is thought of as a useful measure, and the 40-yd (36.6 m) dash is used by the National Football League (NFL) to measure speed and provide a ranking of potential draftees. However, a 40-yd dash technically assesses acceleration, velocity, and average speed. The top speed is the fastest instantaneous rate of an object in motion while the average speed is the distance divided by the time to cover that distance. Velocity includes the component of direction of movement; thus, speed is the magnitude component of velocity. NSCA's Guide to Tests and Assessments (Human Kinetics, 2012) provides an excellent review of the performance of anaerobic tests.
Anaerobic Tests
- Vertical jump test
- Margaria-Kalamen power test
- Modified Margaria-Kalamen power test (also known as the football staircase test)
- Three Modified Box Long Jump (MBLJ) test
- Wingate Anaerobic Test (WAnT)
- Critical power test
Various studies have determined that each test in the list is a valid measure of anaerobic power. In particular, the vertical jump test, standing long jump test, Margaria-Kalamen power test, Modified Margaria-Kalamen power test, and three modified box long jump test are considered to be the most sport specific of these tests. The following sections briefly discuss and provide directions for performing several of these anaerobic tests.
Vertical Jump Test
The vertical jump test is commonly used by coaches to measure lower body power and to test an athlete's jumping ability. Previous investigations determined that the vertical jump has high predictive value for measuring power production for athletes participating in such sports as track and field, weightlifting, volleyball, basketball, and football. To test the vertical jump, schools, organizations, and sport teams commonly use a commercially designed device consisting of plastic swivel vanes placed in 0.5-in. (12.7 cm) increments. Because the athlete uses countermovement of the lower body and an outstretched arm swing to reach the highest vane, the vertical jump test is also known as the jump and reach test.
As an example of the sophistication that can be developed for simple tests such as the vertical jump, consider the following. Some researchers believe that the gold standard for measuring the vertical jump includes implementing video analysis and using biomechanical reflective markers on the hip to measure the displacement of the center of mass. Although valid and reliable, this method is cost prohibitive for many fitness and sport organizations. A commercial jump mat is another device used to measure the vertical jump. Embedded in the mat are microswitches that determine flight time - that is, the interval between the liftoff and landing of both feet during a countermovement from a flat-footed standing position. The flight time in the air is used to compute the subject's vertical jump. A study by García-López et al. using three countermovement jumps found that jump mats designed with photo cells showed higher correlations with force plate technologies compared with a contact jump mat. Similarly, Whitmer et al. determined that practitioners using a contact jump mat may underestimate the vertical jump for high performers. A promising new technology for measuring vertical jump is the Myotest (Myotest Inc., Switzerland). The Myotest device is approximately the size of a small smartphone, and the subject wears the device on the hip to determine the displacement of the center of mass. This test does not require the subject to reach and stretch with one arm to displace vanes like when using a vane jump test device. A study by Nuzzo et al. found that the Myotest demonstrated the best intrasession reliability for measuring a countermovement vertical jump when compared with the vane jump test device and jump mat system.
Vertical jump test.
Procedures for the Vertical Jump Test
- Before the test: To measure the highest standing reach, instruct the subject to stand flat footed and reach with one arm fully extended. This should be the same arm that will extend and displace the vanes. Then measure again during plantar flexion with the same arm extended and during plantar flexion. Measure the subject's reach at the middle finger. This measure will be subtracted from the highest recorded vertical jump value.
- During the test: Instruct the subject to take a vertical jump from a standing position using a countermovement. The subject should squat down and back while simultaneously using a bilateral backward arm swing. The subject should then explode upward by extending the hips, knees, ankles (also known as the triple extension), shoulders, elbows, and wrists and attempt to displace the highest vane with one arm (see figure 7.2). Alternatively, a wall-mounted jump-and-reach board may be used.
- Obtain the measurement and repeat two more times. Instruct the subject to rest for 30 s between trials.
- Calculate the maximum vertical jump by subtracting the highest standing reach from the highest vane displaced during the three vertical jumps.
Learn more about Advanced Exercise Physiology.
Using Body Composition Methods to Identify Cachexia in Cancer Patients
Cachexia is not simply weight loss. In some cancer populations, such as patients with early-stage breast cancer, weight gain is actually a more common occurrence that is associated with poor prognosis.
Cachexia is not simply weight loss. In some cancer populations, such as patients with early-stage breast cancer, weight gain is actually a more common occurrence that is associated with poor prognosis. Cachexia is a metabolic syndrome linked to an underlying condition (e.g., cancer, heart failure) that results in the loss of muscle with or without fat that impairs function. Although the mechanisms that lead to cachexia are not fully understood, one factor that differentiates itself from sarcopenia (see "Body Composition and Weight Management Across the Life Span") is an increase in metabolic rate. This increased metabolic rate may be attributable to the cancer tumor itself, especially when the cancer cells spread to metabolically active tissue. An example of this was seen inpatients with colorectal cancer, where an increase in liver mass due to metastatic cancer cells was associated with a concurrent decrease in total muscle mass. Regardless of what triggers the increased metabolic rate, the end result is increased muscle catabolism, which places the cancer patient at higher risk of early death.
One misconception about cachexia is that obese individuals are somehow protected because of increased energy reserves. Although the obesity paradox suggests a protective effect with increases in certain cancer populations (e.g., individuals undergoing chemotherapy), in general BMI does a poor job of classifying those patients with a high mortality risk. The obvious reason why is the inability of BMI to differentiate FFM from FM. Using a bioelectrical impedance analysis, Gonzalez et al. showed that FFM index (i.e., FFM divided by the square of height) was a better predictor of mortality regardless of how much FM was present. In other words, it did not matter if a patient's BMI was higher or lower; if the patient had a reduced amount of muscle mass, the risk of death was increased.
The clinical implications for measuring FM and FFM become evident if you compare two obese patients, one with cachexia and one without. Both patients lose 20 lb (9.1 kg) after a diagnosis of cancer. Using body composition methods, a clinician can identify the higher risk patient. Methods such as the CT measurement of lumbar skeletal muscle currently are being used, although unfortunately not widely. Regardless, the identification of cachexia is one potential area where knowledge of body composition methods can be invaluable.
Learn more about Advanced Exercise Physiology.
Exercise Genomics
The rapidly expanding field of exercise genomics advances our understanding of the preventive and therapeutic properties of exercise by increasing our knowledge about the physiology of exercise and human behavior.
Contribution by Mark A. Sarzynski, PhD, University of South Carolina
The rapidly expanding field of exercise genomics advances our understanding of the preventive and therapeutic properties of exercise by increasing our knowledge about the physiology of exercise and human behavior. Although understanding the effects of various factors (e.g., environmental) on exercise-related phenotypes has long been of interest, understanding of the role of genetic factors (i.e., exercise genomics) is still in its infancy. Most of the major developments have occurred over the past 50 years. This section of the chapter does not have the capacity to fully review the field of genetics; therefore, the following sections introduce the basic concepts of genetics, deoxyribonucleic acid (DNA), and molecular biology relative to exercise physiology. A more thorough review on the topic can be found in Genetics Primer for Exercise Science and Health by Stephen M. Roth (2007).
Basics of Human Genetics
Genetics is the study of genes, heredity, and genetic variation in living organisms. The human genome, which contains all of the genetic material in human cells, consists of about 3 billion DNA base pairs. DNA encodes the instructions for the development, function, and reproduction of the entire human being. DNA is located in both the nucleus of the cell and the mitochondria, the majority of which is located in the nucleus. The nuclear genome comprises 22 pairs of autosomes (non-sex-specific chromosomes) and one pair of sex chromosomes for a total of 46 chromosomes. Humans inherit half of their genome from their mother (22 autosomes and an X chromosome) and half from their father (22 autosomes and either an X or Y chromosome). Women carry two copies of the X chromosome, whereas men carry one X chromosome and one Y chromosome. The presence or absence of the Y chromosome (responsible for testis development) determines the sex of the offspring.
Each DNA molecule consists of two complementary strands that each comprise four nucleotide bases - adenine (A), cytosine (C), guanine (G), and thymine (T) - that form a double helix. The binding between the two DNA strands is complementary: A always binds to T and C with G, creating complementary base pairs. The order of these nucleotide bases determines the meaning of the biological information encoded in that part of the DNA molecule. Specific sequences or regions of DNA that provide instructions to build ribonucleic acid (RNA) and proteins are called genes. Genes are the basic physical and functional units of heredity. The human genome contains about 20,500 genes. DNA found in the mitochondria is a circular double helix and contains 37 genes. The typical structure of a gene consists of many regions, including the coding region (exons), noncoding region (introns), promoter region (5'-end; upstream region; beginning of gene), and 3'-untranslated and terminator regions (3'-end; downstream region; end of gene; figure 11.2). The promoter region contains elements that direct the transcription of a gene (i.e., turn the gene on or off), whereas the terminator region contains the DNA sequence responsible for stopping the transcription of a gene.
The basic structure of a gene, including the upstream promoter region, the coding exons separated by introns, and the downstream terminator region at the end of the gene.
A central tenet of molecular biology describes the flow of information from DNA to RNA to proteins (figure 11.3). During the process of transcription, or gene expression, the nuclear DNA sequence found in a gene is read and copied onto a complementary strand of RNA called premature messenger RNA (mRNA) by the enzyme RNA polymerase. RNA is single stranded and contains the nucleotides A, G, C, and uracil (U), which replaces T and similarly binds only to A. Before the premature mRNA can be used to build protein, the noncoding regions of introns are removed, resulting in mature mRNA that consists of the coding exonic regions only. The mature mRNA then travels out of the nucleus and into the cell's cytoplasm, where it undergoes the process of translation. During translation, the genetic code is read by special organelles in the cell called ribosomes, which pair the mRNA to transfer RNA and eventually attach a corresponding amino acid to the polypeptide chain. Repetition of this step assembles a protein one amino acid at a time (figure 11.4). With just the four nucleotides used in three-letter combinations, the 20 standard amino acids are assembled.
The central principle of molecular biology, whereby DNA codes for RNA, which codes for proteins.
Overview of the translation of mRNA into protein. The ribosome binds to mRNA and moves one codon at a time downstream, where transfer RNA drops off an amino acid that links with the previous amino acid, thereby forming a polypeptide chain that continues until the ribosome reaches a stop codon.
Heritability and Genetic Variation
More than 99.9% of the DNA sequence in humans is similar. The 0.1% that differs is what makes each individual unique. Because family members share an even greater proportion of DNA sequence compared with unrelated individuals, analysis of familial aggregation (i.e., resemblance across family members) often is used to determine whether genetic variation contributes to a trait. For a given trait, familial aggregation is tested by comparing the variance between families with the variance within family members. For example, the HERITAGE Family Study examined the familial resemblance for maximal oxygen uptake (![]() O2max), the gold standard measure of cardiorespiratory fitness, in 426 sedentary subjects from 86 nuclear families. The authors found that achieved levels of
O2max), the gold standard measure of cardiorespiratory fitness, in 426 sedentary subjects from 86 nuclear families. The authors found that achieved levels of ![]() O2max clearly aggregate in families; there was 2.7 times more variance between different families than within families for adjusted
O2max clearly aggregate in families; there was 2.7 times more variance between different families than within families for adjusted ![]() O2max. Figure 11.5shows that some families tended to have below-average
O2max. Figure 11.5shows that some families tended to have below-average ![]() O2max values, whereas others had above-average values. Because families share genetic factors as well as similar environmental factors (e.g., diet, education, physical activity, and sedentary behaviors), further analyses are needed to determine whether the familial resemblance in
O2max values, whereas others had above-average values. Because families share genetic factors as well as similar environmental factors (e.g., diet, education, physical activity, and sedentary behaviors), further analyses are needed to determine whether the familial resemblance in ![]() O2max is due to genetic or environmental factors.
O2max is due to genetic or environmental factors.
General depiction of familial aggregation for adjusted
Heritability is an estimate of how much of the variation in a trait is due to genetic factors alone. Heritability estimates are quantified by comparing trait similarities between pairs of relatives with different degrees of relatedness. Thus, twin, adoption, and family studies commonly are used to distinguish between the contribution of genetic and environmental factors on the familial aggregation of a trait. For example, a pattern of significant correlations among siblings and between parents and siblings but not between spouses would imply that the familial resemblance primarily is due to genetic factors, whereas significant correlations between spouses and lesser correlations between siblings or between parents and siblings would suggest a stronger influence of shared environmental factors such as diet and exercise habits. In the HERITAGE Family Study, the authors estimated that the genetic heritability of ![]() O2max was 51%. In addition to
O2max was 51%. In addition to ![]() O2max, numerous exercise-related traits have been shown to have a significant genetic component, as evidenced by their estimated heritability levels from twin and family studies (table 11.5).
O2max, numerous exercise-related traits have been shown to have a significant genetic component, as evidenced by their estimated heritability levels from twin and family studies (table 11.5).
After familial aggregation and heritability have been estimated for a trait, the next step is to determine which specific genetic factors contribute to the trait. Here, the term genetic factors refers to genetic variation or differences in the DNA sequence that may influence the information contained in a gene, thus resulting in trait variability between individuals. A variant nucleotide found at a mutation or polymorphism is known as an allele. Typically, two alleles are found at a polymorphism in the genome (e.g., A and G). Because genes come in pairs (one inherited from the mother and the other from the father), every individual has a pair of alleles for each mutation or polymorphism. The combination of alleles at any mutation or polymorphism is known as a genotype (i.e., that part of the genetic makeup that determines specific characteristics or phenotype). Thus, an individual may have either two copies of the same allele or one copy each of the variant allele. For example, if the nucleotides A and G are found at a particular polymorphism, an individual could have one of the following three genotypes: A/A, A/G, or G/G. An individual is a homozygote if they carry two copies of the same allele (e.g., A/A or G/G), whereas a heterozygote carries one of each allele (e.g., A/G). There are several forms of genetic variation, the most common of which is the single nucleotide polymorphism (SNP). An SNP is a single position in the DNA sequence where more than one nucleotide base is found in greater than 1% of the population. There are more than 10 million SNPs in the human genome. A mutation differs from a polymorphism in that the rare allele is found in less than 1% of the population.
Future Directions and Outlook
The field of exercise genomics has rapidly expanded over the past two decades with the advent of next-generation sequencing technologies, allowing for higher throughput and less expensive sequencing of common and rare variants. However, the field is mired by a general reliance on the candidate gene approach and observational studies with small sample sizes. Furthermore, lack of suitable replication studies or available DNA samples has made the replication of findings a difficult task, particularly for genome-wide studies. Thus, moving forward, exercise genomics needs to utilize a systems biology approach that integrates data from multiple technologies, including genomics, transcriptomics, metabolomics, proteomics, and epigenomics, among others. This will require large, well-designed, well-powered collaborative studies with replication from multiple sources along with the development of computational and bioinformatics tools and expertise within the field. Ultimately, identifying the genetic factors underlying the variability in health- and fitness-related traits due to regular exercise would significantly contribute to the study of the biology of adaptation to exercise and the development of an exercise component of personalized preventive and therapeutic medicine.
Save
Save
Save
Learn more about Advanced Exercise Physiology.
Anaerobic Testing
To accurately determine baseline status in order to guide exercise prescription development and determine whether adaptations occur in response to the exercise training stimulus, one needs to be able to precisely measure the variables of interest.
To accurately determine baseline status in order to guide exercise prescription development and determine whether adaptations occur in response to the exercise training stimulus, one needs to be able to precisely measure the variables of interest. Measures must be both repeatable and accurate (i.e., valid). To attain valid measures, the testing methods used must be performed according to specific guidelines with respect to
- the subject's preparation (e.g., meals, rest, prior exercise, time of day),
- equipment use (e.g., appropriateness of equipment for measuring variables of interest, maintenance, calibration),
- implementation according to testing guidelines applied by the individual conducting the test, and
- proper interpretation of the test results.
Typical variables of interest in anaerobic performance assessment are anaerobic power and anaerobic capacity. Anaerobic power is important for sprint, mid-distance, and distance athletes but for varying reasons. For most athletic events, there is interplay between the aerobic and anaerobic energy systems. Referring to figure 7.1, we see that sprinters (events lasting 4 min) predominantly utilize aerobic metabolic sources. Even aerobic athletes must rely on anaerobic sources at critical times of an event, such as during a hill climb in a bicycle race or the final sprint of a 10K running race.
No direct method of determining anaerobic energy power and capacity currently exists. Although blood lactate accumulation generally is considered to be the product of a high rate of anaerobic glycolysis, blood lactate concentration measurement does not provide specific information about the rate and capacity of the production of ATP. Additionally, the concentration of blood lactate is affected by the rate of its clearance, which differs in individuals due to factors such as - but not limited to - recovery activity status (i.e., active vs. passive); recovery exercise intensity; ratio of individual Type I to Type II skeletal muscle fiber composition; the rate of blood flow to the skeletal muscles, heart, and liver (Cori cycle); and the rate of release of muscle lactate into the blood.
The following is a comprehensive list of common anaerobic tests. The test to be utilized must be specific to the variable being measured. For instance, to measure maximal anaerobic muscle power, a test needs to be very short in duration to isolate the ATP-PCr energy system. Maximal muscle power is used in activities such as jumping and throwing. A vertical jump test is a good example of a short-duration muscle power test. Speed often is thought of as a useful measure, and the 40-yd (36.6 m) dash is used by the National Football League (NFL) to measure speed and provide a ranking of potential draftees. However, a 40-yd dash technically assesses acceleration, velocity, and average speed. The top speed is the fastest instantaneous rate of an object in motion while the average speed is the distance divided by the time to cover that distance. Velocity includes the component of direction of movement; thus, speed is the magnitude component of velocity. NSCA's Guide to Tests and Assessments (Human Kinetics, 2012) provides an excellent review of the performance of anaerobic tests.
Anaerobic Tests
- Vertical jump test
- Margaria-Kalamen power test
- Modified Margaria-Kalamen power test (also known as the football staircase test)
- Three Modified Box Long Jump (MBLJ) test
- Wingate Anaerobic Test (WAnT)
- Critical power test
Various studies have determined that each test in the list is a valid measure of anaerobic power. In particular, the vertical jump test, standing long jump test, Margaria-Kalamen power test, Modified Margaria-Kalamen power test, and three modified box long jump test are considered to be the most sport specific of these tests. The following sections briefly discuss and provide directions for performing several of these anaerobic tests.
Vertical Jump Test
The vertical jump test is commonly used by coaches to measure lower body power and to test an athlete's jumping ability. Previous investigations determined that the vertical jump has high predictive value for measuring power production for athletes participating in such sports as track and field, weightlifting, volleyball, basketball, and football. To test the vertical jump, schools, organizations, and sport teams commonly use a commercially designed device consisting of plastic swivel vanes placed in 0.5-in. (12.7 cm) increments. Because the athlete uses countermovement of the lower body and an outstretched arm swing to reach the highest vane, the vertical jump test is also known as the jump and reach test.
As an example of the sophistication that can be developed for simple tests such as the vertical jump, consider the following. Some researchers believe that the gold standard for measuring the vertical jump includes implementing video analysis and using biomechanical reflective markers on the hip to measure the displacement of the center of mass. Although valid and reliable, this method is cost prohibitive for many fitness and sport organizations. A commercial jump mat is another device used to measure the vertical jump. Embedded in the mat are microswitches that determine flight time - that is, the interval between the liftoff and landing of both feet during a countermovement from a flat-footed standing position. The flight time in the air is used to compute the subject's vertical jump. A study by García-López et al. using three countermovement jumps found that jump mats designed with photo cells showed higher correlations with force plate technologies compared with a contact jump mat. Similarly, Whitmer et al. determined that practitioners using a contact jump mat may underestimate the vertical jump for high performers. A promising new technology for measuring vertical jump is the Myotest (Myotest Inc., Switzerland). The Myotest device is approximately the size of a small smartphone, and the subject wears the device on the hip to determine the displacement of the center of mass. This test does not require the subject to reach and stretch with one arm to displace vanes like when using a vane jump test device. A study by Nuzzo et al. found that the Myotest demonstrated the best intrasession reliability for measuring a countermovement vertical jump when compared with the vane jump test device and jump mat system.
Vertical jump test.
Procedures for the Vertical Jump Test
- Before the test: To measure the highest standing reach, instruct the subject to stand flat footed and reach with one arm fully extended. This should be the same arm that will extend and displace the vanes. Then measure again during plantar flexion with the same arm extended and during plantar flexion. Measure the subject's reach at the middle finger. This measure will be subtracted from the highest recorded vertical jump value.
- During the test: Instruct the subject to take a vertical jump from a standing position using a countermovement. The subject should squat down and back while simultaneously using a bilateral backward arm swing. The subject should then explode upward by extending the hips, knees, ankles (also known as the triple extension), shoulders, elbows, and wrists and attempt to displace the highest vane with one arm (see figure 7.2). Alternatively, a wall-mounted jump-and-reach board may be used.
- Obtain the measurement and repeat two more times. Instruct the subject to rest for 30 s between trials.
- Calculate the maximum vertical jump by subtracting the highest standing reach from the highest vane displaced during the three vertical jumps.
Learn more about Advanced Exercise Physiology.
Using Body Composition Methods to Identify Cachexia in Cancer Patients
Cachexia is not simply weight loss. In some cancer populations, such as patients with early-stage breast cancer, weight gain is actually a more common occurrence that is associated with poor prognosis.
Cachexia is not simply weight loss. In some cancer populations, such as patients with early-stage breast cancer, weight gain is actually a more common occurrence that is associated with poor prognosis. Cachexia is a metabolic syndrome linked to an underlying condition (e.g., cancer, heart failure) that results in the loss of muscle with or without fat that impairs function. Although the mechanisms that lead to cachexia are not fully understood, one factor that differentiates itself from sarcopenia (see "Body Composition and Weight Management Across the Life Span") is an increase in metabolic rate. This increased metabolic rate may be attributable to the cancer tumor itself, especially when the cancer cells spread to metabolically active tissue. An example of this was seen inpatients with colorectal cancer, where an increase in liver mass due to metastatic cancer cells was associated with a concurrent decrease in total muscle mass. Regardless of what triggers the increased metabolic rate, the end result is increased muscle catabolism, which places the cancer patient at higher risk of early death.
One misconception about cachexia is that obese individuals are somehow protected because of increased energy reserves. Although the obesity paradox suggests a protective effect with increases in certain cancer populations (e.g., individuals undergoing chemotherapy), in general BMI does a poor job of classifying those patients with a high mortality risk. The obvious reason why is the inability of BMI to differentiate FFM from FM. Using a bioelectrical impedance analysis, Gonzalez et al. showed that FFM index (i.e., FFM divided by the square of height) was a better predictor of mortality regardless of how much FM was present. In other words, it did not matter if a patient's BMI was higher or lower; if the patient had a reduced amount of muscle mass, the risk of death was increased.
The clinical implications for measuring FM and FFM become evident if you compare two obese patients, one with cachexia and one without. Both patients lose 20 lb (9.1 kg) after a diagnosis of cancer. Using body composition methods, a clinician can identify the higher risk patient. Methods such as the CT measurement of lumbar skeletal muscle currently are being used, although unfortunately not widely. Regardless, the identification of cachexia is one potential area where knowledge of body composition methods can be invaluable.
Learn more about Advanced Exercise Physiology.
Exercise Genomics
The rapidly expanding field of exercise genomics advances our understanding of the preventive and therapeutic properties of exercise by increasing our knowledge about the physiology of exercise and human behavior.
Contribution by Mark A. Sarzynski, PhD, University of South Carolina
The rapidly expanding field of exercise genomics advances our understanding of the preventive and therapeutic properties of exercise by increasing our knowledge about the physiology of exercise and human behavior. Although understanding the effects of various factors (e.g., environmental) on exercise-related phenotypes has long been of interest, understanding of the role of genetic factors (i.e., exercise genomics) is still in its infancy. Most of the major developments have occurred over the past 50 years. This section of the chapter does not have the capacity to fully review the field of genetics; therefore, the following sections introduce the basic concepts of genetics, deoxyribonucleic acid (DNA), and molecular biology relative to exercise physiology. A more thorough review on the topic can be found in Genetics Primer for Exercise Science and Health by Stephen M. Roth (2007).
Basics of Human Genetics
Genetics is the study of genes, heredity, and genetic variation in living organisms. The human genome, which contains all of the genetic material in human cells, consists of about 3 billion DNA base pairs. DNA encodes the instructions for the development, function, and reproduction of the entire human being. DNA is located in both the nucleus of the cell and the mitochondria, the majority of which is located in the nucleus. The nuclear genome comprises 22 pairs of autosomes (non-sex-specific chromosomes) and one pair of sex chromosomes for a total of 46 chromosomes. Humans inherit half of their genome from their mother (22 autosomes and an X chromosome) and half from their father (22 autosomes and either an X or Y chromosome). Women carry two copies of the X chromosome, whereas men carry one X chromosome and one Y chromosome. The presence or absence of the Y chromosome (responsible for testis development) determines the sex of the offspring.
Each DNA molecule consists of two complementary strands that each comprise four nucleotide bases - adenine (A), cytosine (C), guanine (G), and thymine (T) - that form a double helix. The binding between the two DNA strands is complementary: A always binds to T and C with G, creating complementary base pairs. The order of these nucleotide bases determines the meaning of the biological information encoded in that part of the DNA molecule. Specific sequences or regions of DNA that provide instructions to build ribonucleic acid (RNA) and proteins are called genes. Genes are the basic physical and functional units of heredity. The human genome contains about 20,500 genes. DNA found in the mitochondria is a circular double helix and contains 37 genes. The typical structure of a gene consists of many regions, including the coding region (exons), noncoding region (introns), promoter region (5'-end; upstream region; beginning of gene), and 3'-untranslated and terminator regions (3'-end; downstream region; end of gene; figure 11.2). The promoter region contains elements that direct the transcription of a gene (i.e., turn the gene on or off), whereas the terminator region contains the DNA sequence responsible for stopping the transcription of a gene.
The basic structure of a gene, including the upstream promoter region, the coding exons separated by introns, and the downstream terminator region at the end of the gene.
A central tenet of molecular biology describes the flow of information from DNA to RNA to proteins (figure 11.3). During the process of transcription, or gene expression, the nuclear DNA sequence found in a gene is read and copied onto a complementary strand of RNA called premature messenger RNA (mRNA) by the enzyme RNA polymerase. RNA is single stranded and contains the nucleotides A, G, C, and uracil (U), which replaces T and similarly binds only to A. Before the premature mRNA can be used to build protein, the noncoding regions of introns are removed, resulting in mature mRNA that consists of the coding exonic regions only. The mature mRNA then travels out of the nucleus and into the cell's cytoplasm, where it undergoes the process of translation. During translation, the genetic code is read by special organelles in the cell called ribosomes, which pair the mRNA to transfer RNA and eventually attach a corresponding amino acid to the polypeptide chain. Repetition of this step assembles a protein one amino acid at a time (figure 11.4). With just the four nucleotides used in three-letter combinations, the 20 standard amino acids are assembled.
The central principle of molecular biology, whereby DNA codes for RNA, which codes for proteins.
Overview of the translation of mRNA into protein. The ribosome binds to mRNA and moves one codon at a time downstream, where transfer RNA drops off an amino acid that links with the previous amino acid, thereby forming a polypeptide chain that continues until the ribosome reaches a stop codon.
Heritability and Genetic Variation
More than 99.9% of the DNA sequence in humans is similar. The 0.1% that differs is what makes each individual unique. Because family members share an even greater proportion of DNA sequence compared with unrelated individuals, analysis of familial aggregation (i.e., resemblance across family members) often is used to determine whether genetic variation contributes to a trait. For a given trait, familial aggregation is tested by comparing the variance between families with the variance within family members. For example, the HERITAGE Family Study examined the familial resemblance for maximal oxygen uptake (![]() O2max), the gold standard measure of cardiorespiratory fitness, in 426 sedentary subjects from 86 nuclear families. The authors found that achieved levels of
O2max), the gold standard measure of cardiorespiratory fitness, in 426 sedentary subjects from 86 nuclear families. The authors found that achieved levels of ![]() O2max clearly aggregate in families; there was 2.7 times more variance between different families than within families for adjusted
O2max clearly aggregate in families; there was 2.7 times more variance between different families than within families for adjusted ![]() O2max. Figure 11.5shows that some families tended to have below-average
O2max. Figure 11.5shows that some families tended to have below-average ![]() O2max values, whereas others had above-average values. Because families share genetic factors as well as similar environmental factors (e.g., diet, education, physical activity, and sedentary behaviors), further analyses are needed to determine whether the familial resemblance in
O2max values, whereas others had above-average values. Because families share genetic factors as well as similar environmental factors (e.g., diet, education, physical activity, and sedentary behaviors), further analyses are needed to determine whether the familial resemblance in ![]() O2max is due to genetic or environmental factors.
O2max is due to genetic or environmental factors.
General depiction of familial aggregation for adjusted
Heritability is an estimate of how much of the variation in a trait is due to genetic factors alone. Heritability estimates are quantified by comparing trait similarities between pairs of relatives with different degrees of relatedness. Thus, twin, adoption, and family studies commonly are used to distinguish between the contribution of genetic and environmental factors on the familial aggregation of a trait. For example, a pattern of significant correlations among siblings and between parents and siblings but not between spouses would imply that the familial resemblance primarily is due to genetic factors, whereas significant correlations between spouses and lesser correlations between siblings or between parents and siblings would suggest a stronger influence of shared environmental factors such as diet and exercise habits. In the HERITAGE Family Study, the authors estimated that the genetic heritability of ![]() O2max was 51%. In addition to
O2max was 51%. In addition to ![]() O2max, numerous exercise-related traits have been shown to have a significant genetic component, as evidenced by their estimated heritability levels from twin and family studies (table 11.5).
O2max, numerous exercise-related traits have been shown to have a significant genetic component, as evidenced by their estimated heritability levels from twin and family studies (table 11.5).
After familial aggregation and heritability have been estimated for a trait, the next step is to determine which specific genetic factors contribute to the trait. Here, the term genetic factors refers to genetic variation or differences in the DNA sequence that may influence the information contained in a gene, thus resulting in trait variability between individuals. A variant nucleotide found at a mutation or polymorphism is known as an allele. Typically, two alleles are found at a polymorphism in the genome (e.g., A and G). Because genes come in pairs (one inherited from the mother and the other from the father), every individual has a pair of alleles for each mutation or polymorphism. The combination of alleles at any mutation or polymorphism is known as a genotype (i.e., that part of the genetic makeup that determines specific characteristics or phenotype). Thus, an individual may have either two copies of the same allele or one copy each of the variant allele. For example, if the nucleotides A and G are found at a particular polymorphism, an individual could have one of the following three genotypes: A/A, A/G, or G/G. An individual is a homozygote if they carry two copies of the same allele (e.g., A/A or G/G), whereas a heterozygote carries one of each allele (e.g., A/G). There are several forms of genetic variation, the most common of which is the single nucleotide polymorphism (SNP). An SNP is a single position in the DNA sequence where more than one nucleotide base is found in greater than 1% of the population. There are more than 10 million SNPs in the human genome. A mutation differs from a polymorphism in that the rare allele is found in less than 1% of the population.
Future Directions and Outlook
The field of exercise genomics has rapidly expanded over the past two decades with the advent of next-generation sequencing technologies, allowing for higher throughput and less expensive sequencing of common and rare variants. However, the field is mired by a general reliance on the candidate gene approach and observational studies with small sample sizes. Furthermore, lack of suitable replication studies or available DNA samples has made the replication of findings a difficult task, particularly for genome-wide studies. Thus, moving forward, exercise genomics needs to utilize a systems biology approach that integrates data from multiple technologies, including genomics, transcriptomics, metabolomics, proteomics, and epigenomics, among others. This will require large, well-designed, well-powered collaborative studies with replication from multiple sources along with the development of computational and bioinformatics tools and expertise within the field. Ultimately, identifying the genetic factors underlying the variability in health- and fitness-related traits due to regular exercise would significantly contribute to the study of the biology of adaptation to exercise and the development of an exercise component of personalized preventive and therapeutic medicine.
Save
Save
Save
Learn more about Advanced Exercise Physiology.
Anaerobic Testing
To accurately determine baseline status in order to guide exercise prescription development and determine whether adaptations occur in response to the exercise training stimulus, one needs to be able to precisely measure the variables of interest.
To accurately determine baseline status in order to guide exercise prescription development and determine whether adaptations occur in response to the exercise training stimulus, one needs to be able to precisely measure the variables of interest. Measures must be both repeatable and accurate (i.e., valid). To attain valid measures, the testing methods used must be performed according to specific guidelines with respect to
- the subject's preparation (e.g., meals, rest, prior exercise, time of day),
- equipment use (e.g., appropriateness of equipment for measuring variables of interest, maintenance, calibration),
- implementation according to testing guidelines applied by the individual conducting the test, and
- proper interpretation of the test results.
Typical variables of interest in anaerobic performance assessment are anaerobic power and anaerobic capacity. Anaerobic power is important for sprint, mid-distance, and distance athletes but for varying reasons. For most athletic events, there is interplay between the aerobic and anaerobic energy systems. Referring to figure 7.1, we see that sprinters (events lasting 4 min) predominantly utilize aerobic metabolic sources. Even aerobic athletes must rely on anaerobic sources at critical times of an event, such as during a hill climb in a bicycle race or the final sprint of a 10K running race.
No direct method of determining anaerobic energy power and capacity currently exists. Although blood lactate accumulation generally is considered to be the product of a high rate of anaerobic glycolysis, blood lactate concentration measurement does not provide specific information about the rate and capacity of the production of ATP. Additionally, the concentration of blood lactate is affected by the rate of its clearance, which differs in individuals due to factors such as - but not limited to - recovery activity status (i.e., active vs. passive); recovery exercise intensity; ratio of individual Type I to Type II skeletal muscle fiber composition; the rate of blood flow to the skeletal muscles, heart, and liver (Cori cycle); and the rate of release of muscle lactate into the blood.
The following is a comprehensive list of common anaerobic tests. The test to be utilized must be specific to the variable being measured. For instance, to measure maximal anaerobic muscle power, a test needs to be very short in duration to isolate the ATP-PCr energy system. Maximal muscle power is used in activities such as jumping and throwing. A vertical jump test is a good example of a short-duration muscle power test. Speed often is thought of as a useful measure, and the 40-yd (36.6 m) dash is used by the National Football League (NFL) to measure speed and provide a ranking of potential draftees. However, a 40-yd dash technically assesses acceleration, velocity, and average speed. The top speed is the fastest instantaneous rate of an object in motion while the average speed is the distance divided by the time to cover that distance. Velocity includes the component of direction of movement; thus, speed is the magnitude component of velocity. NSCA's Guide to Tests and Assessments (Human Kinetics, 2012) provides an excellent review of the performance of anaerobic tests.
Anaerobic Tests
- Vertical jump test
- Margaria-Kalamen power test
- Modified Margaria-Kalamen power test (also known as the football staircase test)
- Three Modified Box Long Jump (MBLJ) test
- Wingate Anaerobic Test (WAnT)
- Critical power test
Various studies have determined that each test in the list is a valid measure of anaerobic power. In particular, the vertical jump test, standing long jump test, Margaria-Kalamen power test, Modified Margaria-Kalamen power test, and three modified box long jump test are considered to be the most sport specific of these tests. The following sections briefly discuss and provide directions for performing several of these anaerobic tests.
Vertical Jump Test
The vertical jump test is commonly used by coaches to measure lower body power and to test an athlete's jumping ability. Previous investigations determined that the vertical jump has high predictive value for measuring power production for athletes participating in such sports as track and field, weightlifting, volleyball, basketball, and football. To test the vertical jump, schools, organizations, and sport teams commonly use a commercially designed device consisting of plastic swivel vanes placed in 0.5-in. (12.7 cm) increments. Because the athlete uses countermovement of the lower body and an outstretched arm swing to reach the highest vane, the vertical jump test is also known as the jump and reach test.
As an example of the sophistication that can be developed for simple tests such as the vertical jump, consider the following. Some researchers believe that the gold standard for measuring the vertical jump includes implementing video analysis and using biomechanical reflective markers on the hip to measure the displacement of the center of mass. Although valid and reliable, this method is cost prohibitive for many fitness and sport organizations. A commercial jump mat is another device used to measure the vertical jump. Embedded in the mat are microswitches that determine flight time - that is, the interval between the liftoff and landing of both feet during a countermovement from a flat-footed standing position. The flight time in the air is used to compute the subject's vertical jump. A study by García-López et al. using three countermovement jumps found that jump mats designed with photo cells showed higher correlations with force plate technologies compared with a contact jump mat. Similarly, Whitmer et al. determined that practitioners using a contact jump mat may underestimate the vertical jump for high performers. A promising new technology for measuring vertical jump is the Myotest (Myotest Inc., Switzerland). The Myotest device is approximately the size of a small smartphone, and the subject wears the device on the hip to determine the displacement of the center of mass. This test does not require the subject to reach and stretch with one arm to displace vanes like when using a vane jump test device. A study by Nuzzo et al. found that the Myotest demonstrated the best intrasession reliability for measuring a countermovement vertical jump when compared with the vane jump test device and jump mat system.
Vertical jump test.
Procedures for the Vertical Jump Test
- Before the test: To measure the highest standing reach, instruct the subject to stand flat footed and reach with one arm fully extended. This should be the same arm that will extend and displace the vanes. Then measure again during plantar flexion with the same arm extended and during plantar flexion. Measure the subject's reach at the middle finger. This measure will be subtracted from the highest recorded vertical jump value.
- During the test: Instruct the subject to take a vertical jump from a standing position using a countermovement. The subject should squat down and back while simultaneously using a bilateral backward arm swing. The subject should then explode upward by extending the hips, knees, ankles (also known as the triple extension), shoulders, elbows, and wrists and attempt to displace the highest vane with one arm (see figure 7.2). Alternatively, a wall-mounted jump-and-reach board may be used.
- Obtain the measurement and repeat two more times. Instruct the subject to rest for 30 s between trials.
- Calculate the maximum vertical jump by subtracting the highest standing reach from the highest vane displaced during the three vertical jumps.
Learn more about Advanced Exercise Physiology.
Using Body Composition Methods to Identify Cachexia in Cancer Patients
Cachexia is not simply weight loss. In some cancer populations, such as patients with early-stage breast cancer, weight gain is actually a more common occurrence that is associated with poor prognosis.
Cachexia is not simply weight loss. In some cancer populations, such as patients with early-stage breast cancer, weight gain is actually a more common occurrence that is associated with poor prognosis. Cachexia is a metabolic syndrome linked to an underlying condition (e.g., cancer, heart failure) that results in the loss of muscle with or without fat that impairs function. Although the mechanisms that lead to cachexia are not fully understood, one factor that differentiates itself from sarcopenia (see "Body Composition and Weight Management Across the Life Span") is an increase in metabolic rate. This increased metabolic rate may be attributable to the cancer tumor itself, especially when the cancer cells spread to metabolically active tissue. An example of this was seen inpatients with colorectal cancer, where an increase in liver mass due to metastatic cancer cells was associated with a concurrent decrease in total muscle mass. Regardless of what triggers the increased metabolic rate, the end result is increased muscle catabolism, which places the cancer patient at higher risk of early death.
One misconception about cachexia is that obese individuals are somehow protected because of increased energy reserves. Although the obesity paradox suggests a protective effect with increases in certain cancer populations (e.g., individuals undergoing chemotherapy), in general BMI does a poor job of classifying those patients with a high mortality risk. The obvious reason why is the inability of BMI to differentiate FFM from FM. Using a bioelectrical impedance analysis, Gonzalez et al. showed that FFM index (i.e., FFM divided by the square of height) was a better predictor of mortality regardless of how much FM was present. In other words, it did not matter if a patient's BMI was higher or lower; if the patient had a reduced amount of muscle mass, the risk of death was increased.
The clinical implications for measuring FM and FFM become evident if you compare two obese patients, one with cachexia and one without. Both patients lose 20 lb (9.1 kg) after a diagnosis of cancer. Using body composition methods, a clinician can identify the higher risk patient. Methods such as the CT measurement of lumbar skeletal muscle currently are being used, although unfortunately not widely. Regardless, the identification of cachexia is one potential area where knowledge of body composition methods can be invaluable.
Learn more about Advanced Exercise Physiology.
Exercise Genomics
The rapidly expanding field of exercise genomics advances our understanding of the preventive and therapeutic properties of exercise by increasing our knowledge about the physiology of exercise and human behavior.
Contribution by Mark A. Sarzynski, PhD, University of South Carolina
The rapidly expanding field of exercise genomics advances our understanding of the preventive and therapeutic properties of exercise by increasing our knowledge about the physiology of exercise and human behavior. Although understanding the effects of various factors (e.g., environmental) on exercise-related phenotypes has long been of interest, understanding of the role of genetic factors (i.e., exercise genomics) is still in its infancy. Most of the major developments have occurred over the past 50 years. This section of the chapter does not have the capacity to fully review the field of genetics; therefore, the following sections introduce the basic concepts of genetics, deoxyribonucleic acid (DNA), and molecular biology relative to exercise physiology. A more thorough review on the topic can be found in Genetics Primer for Exercise Science and Health by Stephen M. Roth (2007).
Basics of Human Genetics
Genetics is the study of genes, heredity, and genetic variation in living organisms. The human genome, which contains all of the genetic material in human cells, consists of about 3 billion DNA base pairs. DNA encodes the instructions for the development, function, and reproduction of the entire human being. DNA is located in both the nucleus of the cell and the mitochondria, the majority of which is located in the nucleus. The nuclear genome comprises 22 pairs of autosomes (non-sex-specific chromosomes) and one pair of sex chromosomes for a total of 46 chromosomes. Humans inherit half of their genome from their mother (22 autosomes and an X chromosome) and half from their father (22 autosomes and either an X or Y chromosome). Women carry two copies of the X chromosome, whereas men carry one X chromosome and one Y chromosome. The presence or absence of the Y chromosome (responsible for testis development) determines the sex of the offspring.
Each DNA molecule consists of two complementary strands that each comprise four nucleotide bases - adenine (A), cytosine (C), guanine (G), and thymine (T) - that form a double helix. The binding between the two DNA strands is complementary: A always binds to T and C with G, creating complementary base pairs. The order of these nucleotide bases determines the meaning of the biological information encoded in that part of the DNA molecule. Specific sequences or regions of DNA that provide instructions to build ribonucleic acid (RNA) and proteins are called genes. Genes are the basic physical and functional units of heredity. The human genome contains about 20,500 genes. DNA found in the mitochondria is a circular double helix and contains 37 genes. The typical structure of a gene consists of many regions, including the coding region (exons), noncoding region (introns), promoter region (5'-end; upstream region; beginning of gene), and 3'-untranslated and terminator regions (3'-end; downstream region; end of gene; figure 11.2). The promoter region contains elements that direct the transcription of a gene (i.e., turn the gene on or off), whereas the terminator region contains the DNA sequence responsible for stopping the transcription of a gene.
The basic structure of a gene, including the upstream promoter region, the coding exons separated by introns, and the downstream terminator region at the end of the gene.
A central tenet of molecular biology describes the flow of information from DNA to RNA to proteins (figure 11.3). During the process of transcription, or gene expression, the nuclear DNA sequence found in a gene is read and copied onto a complementary strand of RNA called premature messenger RNA (mRNA) by the enzyme RNA polymerase. RNA is single stranded and contains the nucleotides A, G, C, and uracil (U), which replaces T and similarly binds only to A. Before the premature mRNA can be used to build protein, the noncoding regions of introns are removed, resulting in mature mRNA that consists of the coding exonic regions only. The mature mRNA then travels out of the nucleus and into the cell's cytoplasm, where it undergoes the process of translation. During translation, the genetic code is read by special organelles in the cell called ribosomes, which pair the mRNA to transfer RNA and eventually attach a corresponding amino acid to the polypeptide chain. Repetition of this step assembles a protein one amino acid at a time (figure 11.4). With just the four nucleotides used in three-letter combinations, the 20 standard amino acids are assembled.
The central principle of molecular biology, whereby DNA codes for RNA, which codes for proteins.
Overview of the translation of mRNA into protein. The ribosome binds to mRNA and moves one codon at a time downstream, where transfer RNA drops off an amino acid that links with the previous amino acid, thereby forming a polypeptide chain that continues until the ribosome reaches a stop codon.
Heritability and Genetic Variation
More than 99.9% of the DNA sequence in humans is similar. The 0.1% that differs is what makes each individual unique. Because family members share an even greater proportion of DNA sequence compared with unrelated individuals, analysis of familial aggregation (i.e., resemblance across family members) often is used to determine whether genetic variation contributes to a trait. For a given trait, familial aggregation is tested by comparing the variance between families with the variance within family members. For example, the HERITAGE Family Study examined the familial resemblance for maximal oxygen uptake (![]() O2max), the gold standard measure of cardiorespiratory fitness, in 426 sedentary subjects from 86 nuclear families. The authors found that achieved levels of
O2max), the gold standard measure of cardiorespiratory fitness, in 426 sedentary subjects from 86 nuclear families. The authors found that achieved levels of ![]() O2max clearly aggregate in families; there was 2.7 times more variance between different families than within families for adjusted
O2max clearly aggregate in families; there was 2.7 times more variance between different families than within families for adjusted ![]() O2max. Figure 11.5shows that some families tended to have below-average
O2max. Figure 11.5shows that some families tended to have below-average ![]() O2max values, whereas others had above-average values. Because families share genetic factors as well as similar environmental factors (e.g., diet, education, physical activity, and sedentary behaviors), further analyses are needed to determine whether the familial resemblance in
O2max values, whereas others had above-average values. Because families share genetic factors as well as similar environmental factors (e.g., diet, education, physical activity, and sedentary behaviors), further analyses are needed to determine whether the familial resemblance in ![]() O2max is due to genetic or environmental factors.
O2max is due to genetic or environmental factors.
General depiction of familial aggregation for adjusted
Heritability is an estimate of how much of the variation in a trait is due to genetic factors alone. Heritability estimates are quantified by comparing trait similarities between pairs of relatives with different degrees of relatedness. Thus, twin, adoption, and family studies commonly are used to distinguish between the contribution of genetic and environmental factors on the familial aggregation of a trait. For example, a pattern of significant correlations among siblings and between parents and siblings but not between spouses would imply that the familial resemblance primarily is due to genetic factors, whereas significant correlations between spouses and lesser correlations between siblings or between parents and siblings would suggest a stronger influence of shared environmental factors such as diet and exercise habits. In the HERITAGE Family Study, the authors estimated that the genetic heritability of ![]() O2max was 51%. In addition to
O2max was 51%. In addition to ![]() O2max, numerous exercise-related traits have been shown to have a significant genetic component, as evidenced by their estimated heritability levels from twin and family studies (table 11.5).
O2max, numerous exercise-related traits have been shown to have a significant genetic component, as evidenced by their estimated heritability levels from twin and family studies (table 11.5).
After familial aggregation and heritability have been estimated for a trait, the next step is to determine which specific genetic factors contribute to the trait. Here, the term genetic factors refers to genetic variation or differences in the DNA sequence that may influence the information contained in a gene, thus resulting in trait variability between individuals. A variant nucleotide found at a mutation or polymorphism is known as an allele. Typically, two alleles are found at a polymorphism in the genome (e.g., A and G). Because genes come in pairs (one inherited from the mother and the other from the father), every individual has a pair of alleles for each mutation or polymorphism. The combination of alleles at any mutation or polymorphism is known as a genotype (i.e., that part of the genetic makeup that determines specific characteristics or phenotype). Thus, an individual may have either two copies of the same allele or one copy each of the variant allele. For example, if the nucleotides A and G are found at a particular polymorphism, an individual could have one of the following three genotypes: A/A, A/G, or G/G. An individual is a homozygote if they carry two copies of the same allele (e.g., A/A or G/G), whereas a heterozygote carries one of each allele (e.g., A/G). There are several forms of genetic variation, the most common of which is the single nucleotide polymorphism (SNP). An SNP is a single position in the DNA sequence where more than one nucleotide base is found in greater than 1% of the population. There are more than 10 million SNPs in the human genome. A mutation differs from a polymorphism in that the rare allele is found in less than 1% of the population.
Future Directions and Outlook
The field of exercise genomics has rapidly expanded over the past two decades with the advent of next-generation sequencing technologies, allowing for higher throughput and less expensive sequencing of common and rare variants. However, the field is mired by a general reliance on the candidate gene approach and observational studies with small sample sizes. Furthermore, lack of suitable replication studies or available DNA samples has made the replication of findings a difficult task, particularly for genome-wide studies. Thus, moving forward, exercise genomics needs to utilize a systems biology approach that integrates data from multiple technologies, including genomics, transcriptomics, metabolomics, proteomics, and epigenomics, among others. This will require large, well-designed, well-powered collaborative studies with replication from multiple sources along with the development of computational and bioinformatics tools and expertise within the field. Ultimately, identifying the genetic factors underlying the variability in health- and fitness-related traits due to regular exercise would significantly contribute to the study of the biology of adaptation to exercise and the development of an exercise component of personalized preventive and therapeutic medicine.
Save
Save
Save
Learn more about Advanced Exercise Physiology.
Anaerobic Testing
To accurately determine baseline status in order to guide exercise prescription development and determine whether adaptations occur in response to the exercise training stimulus, one needs to be able to precisely measure the variables of interest.
To accurately determine baseline status in order to guide exercise prescription development and determine whether adaptations occur in response to the exercise training stimulus, one needs to be able to precisely measure the variables of interest. Measures must be both repeatable and accurate (i.e., valid). To attain valid measures, the testing methods used must be performed according to specific guidelines with respect to
- the subject's preparation (e.g., meals, rest, prior exercise, time of day),
- equipment use (e.g., appropriateness of equipment for measuring variables of interest, maintenance, calibration),
- implementation according to testing guidelines applied by the individual conducting the test, and
- proper interpretation of the test results.
Typical variables of interest in anaerobic performance assessment are anaerobic power and anaerobic capacity. Anaerobic power is important for sprint, mid-distance, and distance athletes but for varying reasons. For most athletic events, there is interplay between the aerobic and anaerobic energy systems. Referring to figure 7.1, we see that sprinters (events lasting 4 min) predominantly utilize aerobic metabolic sources. Even aerobic athletes must rely on anaerobic sources at critical times of an event, such as during a hill climb in a bicycle race or the final sprint of a 10K running race.
No direct method of determining anaerobic energy power and capacity currently exists. Although blood lactate accumulation generally is considered to be the product of a high rate of anaerobic glycolysis, blood lactate concentration measurement does not provide specific information about the rate and capacity of the production of ATP. Additionally, the concentration of blood lactate is affected by the rate of its clearance, which differs in individuals due to factors such as - but not limited to - recovery activity status (i.e., active vs. passive); recovery exercise intensity; ratio of individual Type I to Type II skeletal muscle fiber composition; the rate of blood flow to the skeletal muscles, heart, and liver (Cori cycle); and the rate of release of muscle lactate into the blood.
The following is a comprehensive list of common anaerobic tests. The test to be utilized must be specific to the variable being measured. For instance, to measure maximal anaerobic muscle power, a test needs to be very short in duration to isolate the ATP-PCr energy system. Maximal muscle power is used in activities such as jumping and throwing. A vertical jump test is a good example of a short-duration muscle power test. Speed often is thought of as a useful measure, and the 40-yd (36.6 m) dash is used by the National Football League (NFL) to measure speed and provide a ranking of potential draftees. However, a 40-yd dash technically assesses acceleration, velocity, and average speed. The top speed is the fastest instantaneous rate of an object in motion while the average speed is the distance divided by the time to cover that distance. Velocity includes the component of direction of movement; thus, speed is the magnitude component of velocity. NSCA's Guide to Tests and Assessments (Human Kinetics, 2012) provides an excellent review of the performance of anaerobic tests.
Anaerobic Tests
- Vertical jump test
- Margaria-Kalamen power test
- Modified Margaria-Kalamen power test (also known as the football staircase test)
- Three Modified Box Long Jump (MBLJ) test
- Wingate Anaerobic Test (WAnT)
- Critical power test
Various studies have determined that each test in the list is a valid measure of anaerobic power. In particular, the vertical jump test, standing long jump test, Margaria-Kalamen power test, Modified Margaria-Kalamen power test, and three modified box long jump test are considered to be the most sport specific of these tests. The following sections briefly discuss and provide directions for performing several of these anaerobic tests.
Vertical Jump Test
The vertical jump test is commonly used by coaches to measure lower body power and to test an athlete's jumping ability. Previous investigations determined that the vertical jump has high predictive value for measuring power production for athletes participating in such sports as track and field, weightlifting, volleyball, basketball, and football. To test the vertical jump, schools, organizations, and sport teams commonly use a commercially designed device consisting of plastic swivel vanes placed in 0.5-in. (12.7 cm) increments. Because the athlete uses countermovement of the lower body and an outstretched arm swing to reach the highest vane, the vertical jump test is also known as the jump and reach test.
As an example of the sophistication that can be developed for simple tests such as the vertical jump, consider the following. Some researchers believe that the gold standard for measuring the vertical jump includes implementing video analysis and using biomechanical reflective markers on the hip to measure the displacement of the center of mass. Although valid and reliable, this method is cost prohibitive for many fitness and sport organizations. A commercial jump mat is another device used to measure the vertical jump. Embedded in the mat are microswitches that determine flight time - that is, the interval between the liftoff and landing of both feet during a countermovement from a flat-footed standing position. The flight time in the air is used to compute the subject's vertical jump. A study by García-López et al. using three countermovement jumps found that jump mats designed with photo cells showed higher correlations with force plate technologies compared with a contact jump mat. Similarly, Whitmer et al. determined that practitioners using a contact jump mat may underestimate the vertical jump for high performers. A promising new technology for measuring vertical jump is the Myotest (Myotest Inc., Switzerland). The Myotest device is approximately the size of a small smartphone, and the subject wears the device on the hip to determine the displacement of the center of mass. This test does not require the subject to reach and stretch with one arm to displace vanes like when using a vane jump test device. A study by Nuzzo et al. found that the Myotest demonstrated the best intrasession reliability for measuring a countermovement vertical jump when compared with the vane jump test device and jump mat system.
Vertical jump test.
Procedures for the Vertical Jump Test
- Before the test: To measure the highest standing reach, instruct the subject to stand flat footed and reach with one arm fully extended. This should be the same arm that will extend and displace the vanes. Then measure again during plantar flexion with the same arm extended and during plantar flexion. Measure the subject's reach at the middle finger. This measure will be subtracted from the highest recorded vertical jump value.
- During the test: Instruct the subject to take a vertical jump from a standing position using a countermovement. The subject should squat down and back while simultaneously using a bilateral backward arm swing. The subject should then explode upward by extending the hips, knees, ankles (also known as the triple extension), shoulders, elbows, and wrists and attempt to displace the highest vane with one arm (see figure 7.2). Alternatively, a wall-mounted jump-and-reach board may be used.
- Obtain the measurement and repeat two more times. Instruct the subject to rest for 30 s between trials.
- Calculate the maximum vertical jump by subtracting the highest standing reach from the highest vane displaced during the three vertical jumps.
Learn more about Advanced Exercise Physiology.
Using Body Composition Methods to Identify Cachexia in Cancer Patients
Cachexia is not simply weight loss. In some cancer populations, such as patients with early-stage breast cancer, weight gain is actually a more common occurrence that is associated with poor prognosis.
Cachexia is not simply weight loss. In some cancer populations, such as patients with early-stage breast cancer, weight gain is actually a more common occurrence that is associated with poor prognosis. Cachexia is a metabolic syndrome linked to an underlying condition (e.g., cancer, heart failure) that results in the loss of muscle with or without fat that impairs function. Although the mechanisms that lead to cachexia are not fully understood, one factor that differentiates itself from sarcopenia (see "Body Composition and Weight Management Across the Life Span") is an increase in metabolic rate. This increased metabolic rate may be attributable to the cancer tumor itself, especially when the cancer cells spread to metabolically active tissue. An example of this was seen inpatients with colorectal cancer, where an increase in liver mass due to metastatic cancer cells was associated with a concurrent decrease in total muscle mass. Regardless of what triggers the increased metabolic rate, the end result is increased muscle catabolism, which places the cancer patient at higher risk of early death.
One misconception about cachexia is that obese individuals are somehow protected because of increased energy reserves. Although the obesity paradox suggests a protective effect with increases in certain cancer populations (e.g., individuals undergoing chemotherapy), in general BMI does a poor job of classifying those patients with a high mortality risk. The obvious reason why is the inability of BMI to differentiate FFM from FM. Using a bioelectrical impedance analysis, Gonzalez et al. showed that FFM index (i.e., FFM divided by the square of height) was a better predictor of mortality regardless of how much FM was present. In other words, it did not matter if a patient's BMI was higher or lower; if the patient had a reduced amount of muscle mass, the risk of death was increased.
The clinical implications for measuring FM and FFM become evident if you compare two obese patients, one with cachexia and one without. Both patients lose 20 lb (9.1 kg) after a diagnosis of cancer. Using body composition methods, a clinician can identify the higher risk patient. Methods such as the CT measurement of lumbar skeletal muscle currently are being used, although unfortunately not widely. Regardless, the identification of cachexia is one potential area where knowledge of body composition methods can be invaluable.
Learn more about Advanced Exercise Physiology.
Exercise Genomics
The rapidly expanding field of exercise genomics advances our understanding of the preventive and therapeutic properties of exercise by increasing our knowledge about the physiology of exercise and human behavior.
Contribution by Mark A. Sarzynski, PhD, University of South Carolina
The rapidly expanding field of exercise genomics advances our understanding of the preventive and therapeutic properties of exercise by increasing our knowledge about the physiology of exercise and human behavior. Although understanding the effects of various factors (e.g., environmental) on exercise-related phenotypes has long been of interest, understanding of the role of genetic factors (i.e., exercise genomics) is still in its infancy. Most of the major developments have occurred over the past 50 years. This section of the chapter does not have the capacity to fully review the field of genetics; therefore, the following sections introduce the basic concepts of genetics, deoxyribonucleic acid (DNA), and molecular biology relative to exercise physiology. A more thorough review on the topic can be found in Genetics Primer for Exercise Science and Health by Stephen M. Roth (2007).
Basics of Human Genetics
Genetics is the study of genes, heredity, and genetic variation in living organisms. The human genome, which contains all of the genetic material in human cells, consists of about 3 billion DNA base pairs. DNA encodes the instructions for the development, function, and reproduction of the entire human being. DNA is located in both the nucleus of the cell and the mitochondria, the majority of which is located in the nucleus. The nuclear genome comprises 22 pairs of autosomes (non-sex-specific chromosomes) and one pair of sex chromosomes for a total of 46 chromosomes. Humans inherit half of their genome from their mother (22 autosomes and an X chromosome) and half from their father (22 autosomes and either an X or Y chromosome). Women carry two copies of the X chromosome, whereas men carry one X chromosome and one Y chromosome. The presence or absence of the Y chromosome (responsible for testis development) determines the sex of the offspring.
Each DNA molecule consists of two complementary strands that each comprise four nucleotide bases - adenine (A), cytosine (C), guanine (G), and thymine (T) - that form a double helix. The binding between the two DNA strands is complementary: A always binds to T and C with G, creating complementary base pairs. The order of these nucleotide bases determines the meaning of the biological information encoded in that part of the DNA molecule. Specific sequences or regions of DNA that provide instructions to build ribonucleic acid (RNA) and proteins are called genes. Genes are the basic physical and functional units of heredity. The human genome contains about 20,500 genes. DNA found in the mitochondria is a circular double helix and contains 37 genes. The typical structure of a gene consists of many regions, including the coding region (exons), noncoding region (introns), promoter region (5'-end; upstream region; beginning of gene), and 3'-untranslated and terminator regions (3'-end; downstream region; end of gene; figure 11.2). The promoter region contains elements that direct the transcription of a gene (i.e., turn the gene on or off), whereas the terminator region contains the DNA sequence responsible for stopping the transcription of a gene.
The basic structure of a gene, including the upstream promoter region, the coding exons separated by introns, and the downstream terminator region at the end of the gene.
A central tenet of molecular biology describes the flow of information from DNA to RNA to proteins (figure 11.3). During the process of transcription, or gene expression, the nuclear DNA sequence found in a gene is read and copied onto a complementary strand of RNA called premature messenger RNA (mRNA) by the enzyme RNA polymerase. RNA is single stranded and contains the nucleotides A, G, C, and uracil (U), which replaces T and similarly binds only to A. Before the premature mRNA can be used to build protein, the noncoding regions of introns are removed, resulting in mature mRNA that consists of the coding exonic regions only. The mature mRNA then travels out of the nucleus and into the cell's cytoplasm, where it undergoes the process of translation. During translation, the genetic code is read by special organelles in the cell called ribosomes, which pair the mRNA to transfer RNA and eventually attach a corresponding amino acid to the polypeptide chain. Repetition of this step assembles a protein one amino acid at a time (figure 11.4). With just the four nucleotides used in three-letter combinations, the 20 standard amino acids are assembled.
The central principle of molecular biology, whereby DNA codes for RNA, which codes for proteins.
Overview of the translation of mRNA into protein. The ribosome binds to mRNA and moves one codon at a time downstream, where transfer RNA drops off an amino acid that links with the previous amino acid, thereby forming a polypeptide chain that continues until the ribosome reaches a stop codon.
Heritability and Genetic Variation
More than 99.9% of the DNA sequence in humans is similar. The 0.1% that differs is what makes each individual unique. Because family members share an even greater proportion of DNA sequence compared with unrelated individuals, analysis of familial aggregation (i.e., resemblance across family members) often is used to determine whether genetic variation contributes to a trait. For a given trait, familial aggregation is tested by comparing the variance between families with the variance within family members. For example, the HERITAGE Family Study examined the familial resemblance for maximal oxygen uptake (![]() O2max), the gold standard measure of cardiorespiratory fitness, in 426 sedentary subjects from 86 nuclear families. The authors found that achieved levels of
O2max), the gold standard measure of cardiorespiratory fitness, in 426 sedentary subjects from 86 nuclear families. The authors found that achieved levels of ![]() O2max clearly aggregate in families; there was 2.7 times more variance between different families than within families for adjusted
O2max clearly aggregate in families; there was 2.7 times more variance between different families than within families for adjusted ![]() O2max. Figure 11.5shows that some families tended to have below-average
O2max. Figure 11.5shows that some families tended to have below-average ![]() O2max values, whereas others had above-average values. Because families share genetic factors as well as similar environmental factors (e.g., diet, education, physical activity, and sedentary behaviors), further analyses are needed to determine whether the familial resemblance in
O2max values, whereas others had above-average values. Because families share genetic factors as well as similar environmental factors (e.g., diet, education, physical activity, and sedentary behaviors), further analyses are needed to determine whether the familial resemblance in ![]() O2max is due to genetic or environmental factors.
O2max is due to genetic or environmental factors.
General depiction of familial aggregation for adjusted
Heritability is an estimate of how much of the variation in a trait is due to genetic factors alone. Heritability estimates are quantified by comparing trait similarities between pairs of relatives with different degrees of relatedness. Thus, twin, adoption, and family studies commonly are used to distinguish between the contribution of genetic and environmental factors on the familial aggregation of a trait. For example, a pattern of significant correlations among siblings and between parents and siblings but not between spouses would imply that the familial resemblance primarily is due to genetic factors, whereas significant correlations between spouses and lesser correlations between siblings or between parents and siblings would suggest a stronger influence of shared environmental factors such as diet and exercise habits. In the HERITAGE Family Study, the authors estimated that the genetic heritability of ![]() O2max was 51%. In addition to
O2max was 51%. In addition to ![]() O2max, numerous exercise-related traits have been shown to have a significant genetic component, as evidenced by their estimated heritability levels from twin and family studies (table 11.5).
O2max, numerous exercise-related traits have been shown to have a significant genetic component, as evidenced by their estimated heritability levels from twin and family studies (table 11.5).
After familial aggregation and heritability have been estimated for a trait, the next step is to determine which specific genetic factors contribute to the trait. Here, the term genetic factors refers to genetic variation or differences in the DNA sequence that may influence the information contained in a gene, thus resulting in trait variability between individuals. A variant nucleotide found at a mutation or polymorphism is known as an allele. Typically, two alleles are found at a polymorphism in the genome (e.g., A and G). Because genes come in pairs (one inherited from the mother and the other from the father), every individual has a pair of alleles for each mutation or polymorphism. The combination of alleles at any mutation or polymorphism is known as a genotype (i.e., that part of the genetic makeup that determines specific characteristics or phenotype). Thus, an individual may have either two copies of the same allele or one copy each of the variant allele. For example, if the nucleotides A and G are found at a particular polymorphism, an individual could have one of the following three genotypes: A/A, A/G, or G/G. An individual is a homozygote if they carry two copies of the same allele (e.g., A/A or G/G), whereas a heterozygote carries one of each allele (e.g., A/G). There are several forms of genetic variation, the most common of which is the single nucleotide polymorphism (SNP). An SNP is a single position in the DNA sequence where more than one nucleotide base is found in greater than 1% of the population. There are more than 10 million SNPs in the human genome. A mutation differs from a polymorphism in that the rare allele is found in less than 1% of the population.
Future Directions and Outlook
The field of exercise genomics has rapidly expanded over the past two decades with the advent of next-generation sequencing technologies, allowing for higher throughput and less expensive sequencing of common and rare variants. However, the field is mired by a general reliance on the candidate gene approach and observational studies with small sample sizes. Furthermore, lack of suitable replication studies or available DNA samples has made the replication of findings a difficult task, particularly for genome-wide studies. Thus, moving forward, exercise genomics needs to utilize a systems biology approach that integrates data from multiple technologies, including genomics, transcriptomics, metabolomics, proteomics, and epigenomics, among others. This will require large, well-designed, well-powered collaborative studies with replication from multiple sources along with the development of computational and bioinformatics tools and expertise within the field. Ultimately, identifying the genetic factors underlying the variability in health- and fitness-related traits due to regular exercise would significantly contribute to the study of the biology of adaptation to exercise and the development of an exercise component of personalized preventive and therapeutic medicine.
Save
Save
Save
Learn more about Advanced Exercise Physiology.
Anaerobic Testing
To accurately determine baseline status in order to guide exercise prescription development and determine whether adaptations occur in response to the exercise training stimulus, one needs to be able to precisely measure the variables of interest.
To accurately determine baseline status in order to guide exercise prescription development and determine whether adaptations occur in response to the exercise training stimulus, one needs to be able to precisely measure the variables of interest. Measures must be both repeatable and accurate (i.e., valid). To attain valid measures, the testing methods used must be performed according to specific guidelines with respect to
- the subject's preparation (e.g., meals, rest, prior exercise, time of day),
- equipment use (e.g., appropriateness of equipment for measuring variables of interest, maintenance, calibration),
- implementation according to testing guidelines applied by the individual conducting the test, and
- proper interpretation of the test results.
Typical variables of interest in anaerobic performance assessment are anaerobic power and anaerobic capacity. Anaerobic power is important for sprint, mid-distance, and distance athletes but for varying reasons. For most athletic events, there is interplay between the aerobic and anaerobic energy systems. Referring to figure 7.1, we see that sprinters (events lasting 4 min) predominantly utilize aerobic metabolic sources. Even aerobic athletes must rely on anaerobic sources at critical times of an event, such as during a hill climb in a bicycle race or the final sprint of a 10K running race.
No direct method of determining anaerobic energy power and capacity currently exists. Although blood lactate accumulation generally is considered to be the product of a high rate of anaerobic glycolysis, blood lactate concentration measurement does not provide specific information about the rate and capacity of the production of ATP. Additionally, the concentration of blood lactate is affected by the rate of its clearance, which differs in individuals due to factors such as - but not limited to - recovery activity status (i.e., active vs. passive); recovery exercise intensity; ratio of individual Type I to Type II skeletal muscle fiber composition; the rate of blood flow to the skeletal muscles, heart, and liver (Cori cycle); and the rate of release of muscle lactate into the blood.
The following is a comprehensive list of common anaerobic tests. The test to be utilized must be specific to the variable being measured. For instance, to measure maximal anaerobic muscle power, a test needs to be very short in duration to isolate the ATP-PCr energy system. Maximal muscle power is used in activities such as jumping and throwing. A vertical jump test is a good example of a short-duration muscle power test. Speed often is thought of as a useful measure, and the 40-yd (36.6 m) dash is used by the National Football League (NFL) to measure speed and provide a ranking of potential draftees. However, a 40-yd dash technically assesses acceleration, velocity, and average speed. The top speed is the fastest instantaneous rate of an object in motion while the average speed is the distance divided by the time to cover that distance. Velocity includes the component of direction of movement; thus, speed is the magnitude component of velocity. NSCA's Guide to Tests and Assessments (Human Kinetics, 2012) provides an excellent review of the performance of anaerobic tests.
Anaerobic Tests
- Vertical jump test
- Margaria-Kalamen power test
- Modified Margaria-Kalamen power test (also known as the football staircase test)
- Three Modified Box Long Jump (MBLJ) test
- Wingate Anaerobic Test (WAnT)
- Critical power test
Various studies have determined that each test in the list is a valid measure of anaerobic power. In particular, the vertical jump test, standing long jump test, Margaria-Kalamen power test, Modified Margaria-Kalamen power test, and three modified box long jump test are considered to be the most sport specific of these tests. The following sections briefly discuss and provide directions for performing several of these anaerobic tests.
Vertical Jump Test
The vertical jump test is commonly used by coaches to measure lower body power and to test an athlete's jumping ability. Previous investigations determined that the vertical jump has high predictive value for measuring power production for athletes participating in such sports as track and field, weightlifting, volleyball, basketball, and football. To test the vertical jump, schools, organizations, and sport teams commonly use a commercially designed device consisting of plastic swivel vanes placed in 0.5-in. (12.7 cm) increments. Because the athlete uses countermovement of the lower body and an outstretched arm swing to reach the highest vane, the vertical jump test is also known as the jump and reach test.
As an example of the sophistication that can be developed for simple tests such as the vertical jump, consider the following. Some researchers believe that the gold standard for measuring the vertical jump includes implementing video analysis and using biomechanical reflective markers on the hip to measure the displacement of the center of mass. Although valid and reliable, this method is cost prohibitive for many fitness and sport organizations. A commercial jump mat is another device used to measure the vertical jump. Embedded in the mat are microswitches that determine flight time - that is, the interval between the liftoff and landing of both feet during a countermovement from a flat-footed standing position. The flight time in the air is used to compute the subject's vertical jump. A study by García-López et al. using three countermovement jumps found that jump mats designed with photo cells showed higher correlations with force plate technologies compared with a contact jump mat. Similarly, Whitmer et al. determined that practitioners using a contact jump mat may underestimate the vertical jump for high performers. A promising new technology for measuring vertical jump is the Myotest (Myotest Inc., Switzerland). The Myotest device is approximately the size of a small smartphone, and the subject wears the device on the hip to determine the displacement of the center of mass. This test does not require the subject to reach and stretch with one arm to displace vanes like when using a vane jump test device. A study by Nuzzo et al. found that the Myotest demonstrated the best intrasession reliability for measuring a countermovement vertical jump when compared with the vane jump test device and jump mat system.
Vertical jump test.
Procedures for the Vertical Jump Test
- Before the test: To measure the highest standing reach, instruct the subject to stand flat footed and reach with one arm fully extended. This should be the same arm that will extend and displace the vanes. Then measure again during plantar flexion with the same arm extended and during plantar flexion. Measure the subject's reach at the middle finger. This measure will be subtracted from the highest recorded vertical jump value.
- During the test: Instruct the subject to take a vertical jump from a standing position using a countermovement. The subject should squat down and back while simultaneously using a bilateral backward arm swing. The subject should then explode upward by extending the hips, knees, ankles (also known as the triple extension), shoulders, elbows, and wrists and attempt to displace the highest vane with one arm (see figure 7.2). Alternatively, a wall-mounted jump-and-reach board may be used.
- Obtain the measurement and repeat two more times. Instruct the subject to rest for 30 s between trials.
- Calculate the maximum vertical jump by subtracting the highest standing reach from the highest vane displaced during the three vertical jumps.
Learn more about Advanced Exercise Physiology.
Using Body Composition Methods to Identify Cachexia in Cancer Patients
Cachexia is not simply weight loss. In some cancer populations, such as patients with early-stage breast cancer, weight gain is actually a more common occurrence that is associated with poor prognosis.
Cachexia is not simply weight loss. In some cancer populations, such as patients with early-stage breast cancer, weight gain is actually a more common occurrence that is associated with poor prognosis. Cachexia is a metabolic syndrome linked to an underlying condition (e.g., cancer, heart failure) that results in the loss of muscle with or without fat that impairs function. Although the mechanisms that lead to cachexia are not fully understood, one factor that differentiates itself from sarcopenia (see "Body Composition and Weight Management Across the Life Span") is an increase in metabolic rate. This increased metabolic rate may be attributable to the cancer tumor itself, especially when the cancer cells spread to metabolically active tissue. An example of this was seen inpatients with colorectal cancer, where an increase in liver mass due to metastatic cancer cells was associated with a concurrent decrease in total muscle mass. Regardless of what triggers the increased metabolic rate, the end result is increased muscle catabolism, which places the cancer patient at higher risk of early death.
One misconception about cachexia is that obese individuals are somehow protected because of increased energy reserves. Although the obesity paradox suggests a protective effect with increases in certain cancer populations (e.g., individuals undergoing chemotherapy), in general BMI does a poor job of classifying those patients with a high mortality risk. The obvious reason why is the inability of BMI to differentiate FFM from FM. Using a bioelectrical impedance analysis, Gonzalez et al. showed that FFM index (i.e., FFM divided by the square of height) was a better predictor of mortality regardless of how much FM was present. In other words, it did not matter if a patient's BMI was higher or lower; if the patient had a reduced amount of muscle mass, the risk of death was increased.
The clinical implications for measuring FM and FFM become evident if you compare two obese patients, one with cachexia and one without. Both patients lose 20 lb (9.1 kg) after a diagnosis of cancer. Using body composition methods, a clinician can identify the higher risk patient. Methods such as the CT measurement of lumbar skeletal muscle currently are being used, although unfortunately not widely. Regardless, the identification of cachexia is one potential area where knowledge of body composition methods can be invaluable.
Learn more about Advanced Exercise Physiology.
Exercise Genomics
The rapidly expanding field of exercise genomics advances our understanding of the preventive and therapeutic properties of exercise by increasing our knowledge about the physiology of exercise and human behavior.
Contribution by Mark A. Sarzynski, PhD, University of South Carolina
The rapidly expanding field of exercise genomics advances our understanding of the preventive and therapeutic properties of exercise by increasing our knowledge about the physiology of exercise and human behavior. Although understanding the effects of various factors (e.g., environmental) on exercise-related phenotypes has long been of interest, understanding of the role of genetic factors (i.e., exercise genomics) is still in its infancy. Most of the major developments have occurred over the past 50 years. This section of the chapter does not have the capacity to fully review the field of genetics; therefore, the following sections introduce the basic concepts of genetics, deoxyribonucleic acid (DNA), and molecular biology relative to exercise physiology. A more thorough review on the topic can be found in Genetics Primer for Exercise Science and Health by Stephen M. Roth (2007).
Basics of Human Genetics
Genetics is the study of genes, heredity, and genetic variation in living organisms. The human genome, which contains all of the genetic material in human cells, consists of about 3 billion DNA base pairs. DNA encodes the instructions for the development, function, and reproduction of the entire human being. DNA is located in both the nucleus of the cell and the mitochondria, the majority of which is located in the nucleus. The nuclear genome comprises 22 pairs of autosomes (non-sex-specific chromosomes) and one pair of sex chromosomes for a total of 46 chromosomes. Humans inherit half of their genome from their mother (22 autosomes and an X chromosome) and half from their father (22 autosomes and either an X or Y chromosome). Women carry two copies of the X chromosome, whereas men carry one X chromosome and one Y chromosome. The presence or absence of the Y chromosome (responsible for testis development) determines the sex of the offspring.
Each DNA molecule consists of two complementary strands that each comprise four nucleotide bases - adenine (A), cytosine (C), guanine (G), and thymine (T) - that form a double helix. The binding between the two DNA strands is complementary: A always binds to T and C with G, creating complementary base pairs. The order of these nucleotide bases determines the meaning of the biological information encoded in that part of the DNA molecule. Specific sequences or regions of DNA that provide instructions to build ribonucleic acid (RNA) and proteins are called genes. Genes are the basic physical and functional units of heredity. The human genome contains about 20,500 genes. DNA found in the mitochondria is a circular double helix and contains 37 genes. The typical structure of a gene consists of many regions, including the coding region (exons), noncoding region (introns), promoter region (5'-end; upstream region; beginning of gene), and 3'-untranslated and terminator regions (3'-end; downstream region; end of gene; figure 11.2). The promoter region contains elements that direct the transcription of a gene (i.e., turn the gene on or off), whereas the terminator region contains the DNA sequence responsible for stopping the transcription of a gene.
The basic structure of a gene, including the upstream promoter region, the coding exons separated by introns, and the downstream terminator region at the end of the gene.
A central tenet of molecular biology describes the flow of information from DNA to RNA to proteins (figure 11.3). During the process of transcription, or gene expression, the nuclear DNA sequence found in a gene is read and copied onto a complementary strand of RNA called premature messenger RNA (mRNA) by the enzyme RNA polymerase. RNA is single stranded and contains the nucleotides A, G, C, and uracil (U), which replaces T and similarly binds only to A. Before the premature mRNA can be used to build protein, the noncoding regions of introns are removed, resulting in mature mRNA that consists of the coding exonic regions only. The mature mRNA then travels out of the nucleus and into the cell's cytoplasm, where it undergoes the process of translation. During translation, the genetic code is read by special organelles in the cell called ribosomes, which pair the mRNA to transfer RNA and eventually attach a corresponding amino acid to the polypeptide chain. Repetition of this step assembles a protein one amino acid at a time (figure 11.4). With just the four nucleotides used in three-letter combinations, the 20 standard amino acids are assembled.
The central principle of molecular biology, whereby DNA codes for RNA, which codes for proteins.
Overview of the translation of mRNA into protein. The ribosome binds to mRNA and moves one codon at a time downstream, where transfer RNA drops off an amino acid that links with the previous amino acid, thereby forming a polypeptide chain that continues until the ribosome reaches a stop codon.
Heritability and Genetic Variation
More than 99.9% of the DNA sequence in humans is similar. The 0.1% that differs is what makes each individual unique. Because family members share an even greater proportion of DNA sequence compared with unrelated individuals, analysis of familial aggregation (i.e., resemblance across family members) often is used to determine whether genetic variation contributes to a trait. For a given trait, familial aggregation is tested by comparing the variance between families with the variance within family members. For example, the HERITAGE Family Study examined the familial resemblance for maximal oxygen uptake (![]() O2max), the gold standard measure of cardiorespiratory fitness, in 426 sedentary subjects from 86 nuclear families. The authors found that achieved levels of
O2max), the gold standard measure of cardiorespiratory fitness, in 426 sedentary subjects from 86 nuclear families. The authors found that achieved levels of ![]() O2max clearly aggregate in families; there was 2.7 times more variance between different families than within families for adjusted
O2max clearly aggregate in families; there was 2.7 times more variance between different families than within families for adjusted ![]() O2max. Figure 11.5shows that some families tended to have below-average
O2max. Figure 11.5shows that some families tended to have below-average ![]() O2max values, whereas others had above-average values. Because families share genetic factors as well as similar environmental factors (e.g., diet, education, physical activity, and sedentary behaviors), further analyses are needed to determine whether the familial resemblance in
O2max values, whereas others had above-average values. Because families share genetic factors as well as similar environmental factors (e.g., diet, education, physical activity, and sedentary behaviors), further analyses are needed to determine whether the familial resemblance in ![]() O2max is due to genetic or environmental factors.
O2max is due to genetic or environmental factors.
General depiction of familial aggregation for adjusted
Heritability is an estimate of how much of the variation in a trait is due to genetic factors alone. Heritability estimates are quantified by comparing trait similarities between pairs of relatives with different degrees of relatedness. Thus, twin, adoption, and family studies commonly are used to distinguish between the contribution of genetic and environmental factors on the familial aggregation of a trait. For example, a pattern of significant correlations among siblings and between parents and siblings but not between spouses would imply that the familial resemblance primarily is due to genetic factors, whereas significant correlations between spouses and lesser correlations between siblings or between parents and siblings would suggest a stronger influence of shared environmental factors such as diet and exercise habits. In the HERITAGE Family Study, the authors estimated that the genetic heritability of ![]() O2max was 51%. In addition to
O2max was 51%. In addition to ![]() O2max, numerous exercise-related traits have been shown to have a significant genetic component, as evidenced by their estimated heritability levels from twin and family studies (table 11.5).
O2max, numerous exercise-related traits have been shown to have a significant genetic component, as evidenced by their estimated heritability levels from twin and family studies (table 11.5).
After familial aggregation and heritability have been estimated for a trait, the next step is to determine which specific genetic factors contribute to the trait. Here, the term genetic factors refers to genetic variation or differences in the DNA sequence that may influence the information contained in a gene, thus resulting in trait variability between individuals. A variant nucleotide found at a mutation or polymorphism is known as an allele. Typically, two alleles are found at a polymorphism in the genome (e.g., A and G). Because genes come in pairs (one inherited from the mother and the other from the father), every individual has a pair of alleles for each mutation or polymorphism. The combination of alleles at any mutation or polymorphism is known as a genotype (i.e., that part of the genetic makeup that determines specific characteristics or phenotype). Thus, an individual may have either two copies of the same allele or one copy each of the variant allele. For example, if the nucleotides A and G are found at a particular polymorphism, an individual could have one of the following three genotypes: A/A, A/G, or G/G. An individual is a homozygote if they carry two copies of the same allele (e.g., A/A or G/G), whereas a heterozygote carries one of each allele (e.g., A/G). There are several forms of genetic variation, the most common of which is the single nucleotide polymorphism (SNP). An SNP is a single position in the DNA sequence where more than one nucleotide base is found in greater than 1% of the population. There are more than 10 million SNPs in the human genome. A mutation differs from a polymorphism in that the rare allele is found in less than 1% of the population.
Future Directions and Outlook
The field of exercise genomics has rapidly expanded over the past two decades with the advent of next-generation sequencing technologies, allowing for higher throughput and less expensive sequencing of common and rare variants. However, the field is mired by a general reliance on the candidate gene approach and observational studies with small sample sizes. Furthermore, lack of suitable replication studies or available DNA samples has made the replication of findings a difficult task, particularly for genome-wide studies. Thus, moving forward, exercise genomics needs to utilize a systems biology approach that integrates data from multiple technologies, including genomics, transcriptomics, metabolomics, proteomics, and epigenomics, among others. This will require large, well-designed, well-powered collaborative studies with replication from multiple sources along with the development of computational and bioinformatics tools and expertise within the field. Ultimately, identifying the genetic factors underlying the variability in health- and fitness-related traits due to regular exercise would significantly contribute to the study of the biology of adaptation to exercise and the development of an exercise component of personalized preventive and therapeutic medicine.
Save
Save
Save
Learn more about Advanced Exercise Physiology.
Anaerobic Testing
To accurately determine baseline status in order to guide exercise prescription development and determine whether adaptations occur in response to the exercise training stimulus, one needs to be able to precisely measure the variables of interest.
To accurately determine baseline status in order to guide exercise prescription development and determine whether adaptations occur in response to the exercise training stimulus, one needs to be able to precisely measure the variables of interest. Measures must be both repeatable and accurate (i.e., valid). To attain valid measures, the testing methods used must be performed according to specific guidelines with respect to
- the subject's preparation (e.g., meals, rest, prior exercise, time of day),
- equipment use (e.g., appropriateness of equipment for measuring variables of interest, maintenance, calibration),
- implementation according to testing guidelines applied by the individual conducting the test, and
- proper interpretation of the test results.
Typical variables of interest in anaerobic performance assessment are anaerobic power and anaerobic capacity. Anaerobic power is important for sprint, mid-distance, and distance athletes but for varying reasons. For most athletic events, there is interplay between the aerobic and anaerobic energy systems. Referring to figure 7.1, we see that sprinters (events lasting 4 min) predominantly utilize aerobic metabolic sources. Even aerobic athletes must rely on anaerobic sources at critical times of an event, such as during a hill climb in a bicycle race or the final sprint of a 10K running race.
No direct method of determining anaerobic energy power and capacity currently exists. Although blood lactate accumulation generally is considered to be the product of a high rate of anaerobic glycolysis, blood lactate concentration measurement does not provide specific information about the rate and capacity of the production of ATP. Additionally, the concentration of blood lactate is affected by the rate of its clearance, which differs in individuals due to factors such as - but not limited to - recovery activity status (i.e., active vs. passive); recovery exercise intensity; ratio of individual Type I to Type II skeletal muscle fiber composition; the rate of blood flow to the skeletal muscles, heart, and liver (Cori cycle); and the rate of release of muscle lactate into the blood.
The following is a comprehensive list of common anaerobic tests. The test to be utilized must be specific to the variable being measured. For instance, to measure maximal anaerobic muscle power, a test needs to be very short in duration to isolate the ATP-PCr energy system. Maximal muscle power is used in activities such as jumping and throwing. A vertical jump test is a good example of a short-duration muscle power test. Speed often is thought of as a useful measure, and the 40-yd (36.6 m) dash is used by the National Football League (NFL) to measure speed and provide a ranking of potential draftees. However, a 40-yd dash technically assesses acceleration, velocity, and average speed. The top speed is the fastest instantaneous rate of an object in motion while the average speed is the distance divided by the time to cover that distance. Velocity includes the component of direction of movement; thus, speed is the magnitude component of velocity. NSCA's Guide to Tests and Assessments (Human Kinetics, 2012) provides an excellent review of the performance of anaerobic tests.
Anaerobic Tests
- Vertical jump test
- Margaria-Kalamen power test
- Modified Margaria-Kalamen power test (also known as the football staircase test)
- Three Modified Box Long Jump (MBLJ) test
- Wingate Anaerobic Test (WAnT)
- Critical power test
Various studies have determined that each test in the list is a valid measure of anaerobic power. In particular, the vertical jump test, standing long jump test, Margaria-Kalamen power test, Modified Margaria-Kalamen power test, and three modified box long jump test are considered to be the most sport specific of these tests. The following sections briefly discuss and provide directions for performing several of these anaerobic tests.
Vertical Jump Test
The vertical jump test is commonly used by coaches to measure lower body power and to test an athlete's jumping ability. Previous investigations determined that the vertical jump has high predictive value for measuring power production for athletes participating in such sports as track and field, weightlifting, volleyball, basketball, and football. To test the vertical jump, schools, organizations, and sport teams commonly use a commercially designed device consisting of plastic swivel vanes placed in 0.5-in. (12.7 cm) increments. Because the athlete uses countermovement of the lower body and an outstretched arm swing to reach the highest vane, the vertical jump test is also known as the jump and reach test.
As an example of the sophistication that can be developed for simple tests such as the vertical jump, consider the following. Some researchers believe that the gold standard for measuring the vertical jump includes implementing video analysis and using biomechanical reflective markers on the hip to measure the displacement of the center of mass. Although valid and reliable, this method is cost prohibitive for many fitness and sport organizations. A commercial jump mat is another device used to measure the vertical jump. Embedded in the mat are microswitches that determine flight time - that is, the interval between the liftoff and landing of both feet during a countermovement from a flat-footed standing position. The flight time in the air is used to compute the subject's vertical jump. A study by García-López et al. using three countermovement jumps found that jump mats designed with photo cells showed higher correlations with force plate technologies compared with a contact jump mat. Similarly, Whitmer et al. determined that practitioners using a contact jump mat may underestimate the vertical jump for high performers. A promising new technology for measuring vertical jump is the Myotest (Myotest Inc., Switzerland). The Myotest device is approximately the size of a small smartphone, and the subject wears the device on the hip to determine the displacement of the center of mass. This test does not require the subject to reach and stretch with one arm to displace vanes like when using a vane jump test device. A study by Nuzzo et al. found that the Myotest demonstrated the best intrasession reliability for measuring a countermovement vertical jump when compared with the vane jump test device and jump mat system.
Vertical jump test.
Procedures for the Vertical Jump Test
- Before the test: To measure the highest standing reach, instruct the subject to stand flat footed and reach with one arm fully extended. This should be the same arm that will extend and displace the vanes. Then measure again during plantar flexion with the same arm extended and during plantar flexion. Measure the subject's reach at the middle finger. This measure will be subtracted from the highest recorded vertical jump value.
- During the test: Instruct the subject to take a vertical jump from a standing position using a countermovement. The subject should squat down and back while simultaneously using a bilateral backward arm swing. The subject should then explode upward by extending the hips, knees, ankles (also known as the triple extension), shoulders, elbows, and wrists and attempt to displace the highest vane with one arm (see figure 7.2). Alternatively, a wall-mounted jump-and-reach board may be used.
- Obtain the measurement and repeat two more times. Instruct the subject to rest for 30 s between trials.
- Calculate the maximum vertical jump by subtracting the highest standing reach from the highest vane displaced during the three vertical jumps.
Learn more about Advanced Exercise Physiology.
Using Body Composition Methods to Identify Cachexia in Cancer Patients
Cachexia is not simply weight loss. In some cancer populations, such as patients with early-stage breast cancer, weight gain is actually a more common occurrence that is associated with poor prognosis.
Cachexia is not simply weight loss. In some cancer populations, such as patients with early-stage breast cancer, weight gain is actually a more common occurrence that is associated with poor prognosis. Cachexia is a metabolic syndrome linked to an underlying condition (e.g., cancer, heart failure) that results in the loss of muscle with or without fat that impairs function. Although the mechanisms that lead to cachexia are not fully understood, one factor that differentiates itself from sarcopenia (see "Body Composition and Weight Management Across the Life Span") is an increase in metabolic rate. This increased metabolic rate may be attributable to the cancer tumor itself, especially when the cancer cells spread to metabolically active tissue. An example of this was seen inpatients with colorectal cancer, where an increase in liver mass due to metastatic cancer cells was associated with a concurrent decrease in total muscle mass. Regardless of what triggers the increased metabolic rate, the end result is increased muscle catabolism, which places the cancer patient at higher risk of early death.
One misconception about cachexia is that obese individuals are somehow protected because of increased energy reserves. Although the obesity paradox suggests a protective effect with increases in certain cancer populations (e.g., individuals undergoing chemotherapy), in general BMI does a poor job of classifying those patients with a high mortality risk. The obvious reason why is the inability of BMI to differentiate FFM from FM. Using a bioelectrical impedance analysis, Gonzalez et al. showed that FFM index (i.e., FFM divided by the square of height) was a better predictor of mortality regardless of how much FM was present. In other words, it did not matter if a patient's BMI was higher or lower; if the patient had a reduced amount of muscle mass, the risk of death was increased.
The clinical implications for measuring FM and FFM become evident if you compare two obese patients, one with cachexia and one without. Both patients lose 20 lb (9.1 kg) after a diagnosis of cancer. Using body composition methods, a clinician can identify the higher risk patient. Methods such as the CT measurement of lumbar skeletal muscle currently are being used, although unfortunately not widely. Regardless, the identification of cachexia is one potential area where knowledge of body composition methods can be invaluable.
Learn more about Advanced Exercise Physiology.
Exercise Genomics
The rapidly expanding field of exercise genomics advances our understanding of the preventive and therapeutic properties of exercise by increasing our knowledge about the physiology of exercise and human behavior.
Contribution by Mark A. Sarzynski, PhD, University of South Carolina
The rapidly expanding field of exercise genomics advances our understanding of the preventive and therapeutic properties of exercise by increasing our knowledge about the physiology of exercise and human behavior. Although understanding the effects of various factors (e.g., environmental) on exercise-related phenotypes has long been of interest, understanding of the role of genetic factors (i.e., exercise genomics) is still in its infancy. Most of the major developments have occurred over the past 50 years. This section of the chapter does not have the capacity to fully review the field of genetics; therefore, the following sections introduce the basic concepts of genetics, deoxyribonucleic acid (DNA), and molecular biology relative to exercise physiology. A more thorough review on the topic can be found in Genetics Primer for Exercise Science and Health by Stephen M. Roth (2007).
Basics of Human Genetics
Genetics is the study of genes, heredity, and genetic variation in living organisms. The human genome, which contains all of the genetic material in human cells, consists of about 3 billion DNA base pairs. DNA encodes the instructions for the development, function, and reproduction of the entire human being. DNA is located in both the nucleus of the cell and the mitochondria, the majority of which is located in the nucleus. The nuclear genome comprises 22 pairs of autosomes (non-sex-specific chromosomes) and one pair of sex chromosomes for a total of 46 chromosomes. Humans inherit half of their genome from their mother (22 autosomes and an X chromosome) and half from their father (22 autosomes and either an X or Y chromosome). Women carry two copies of the X chromosome, whereas men carry one X chromosome and one Y chromosome. The presence or absence of the Y chromosome (responsible for testis development) determines the sex of the offspring.
Each DNA molecule consists of two complementary strands that each comprise four nucleotide bases - adenine (A), cytosine (C), guanine (G), and thymine (T) - that form a double helix. The binding between the two DNA strands is complementary: A always binds to T and C with G, creating complementary base pairs. The order of these nucleotide bases determines the meaning of the biological information encoded in that part of the DNA molecule. Specific sequences or regions of DNA that provide instructions to build ribonucleic acid (RNA) and proteins are called genes. Genes are the basic physical and functional units of heredity. The human genome contains about 20,500 genes. DNA found in the mitochondria is a circular double helix and contains 37 genes. The typical structure of a gene consists of many regions, including the coding region (exons), noncoding region (introns), promoter region (5'-end; upstream region; beginning of gene), and 3'-untranslated and terminator regions (3'-end; downstream region; end of gene; figure 11.2). The promoter region contains elements that direct the transcription of a gene (i.e., turn the gene on or off), whereas the terminator region contains the DNA sequence responsible for stopping the transcription of a gene.
The basic structure of a gene, including the upstream promoter region, the coding exons separated by introns, and the downstream terminator region at the end of the gene.
A central tenet of molecular biology describes the flow of information from DNA to RNA to proteins (figure 11.3). During the process of transcription, or gene expression, the nuclear DNA sequence found in a gene is read and copied onto a complementary strand of RNA called premature messenger RNA (mRNA) by the enzyme RNA polymerase. RNA is single stranded and contains the nucleotides A, G, C, and uracil (U), which replaces T and similarly binds only to A. Before the premature mRNA can be used to build protein, the noncoding regions of introns are removed, resulting in mature mRNA that consists of the coding exonic regions only. The mature mRNA then travels out of the nucleus and into the cell's cytoplasm, where it undergoes the process of translation. During translation, the genetic code is read by special organelles in the cell called ribosomes, which pair the mRNA to transfer RNA and eventually attach a corresponding amino acid to the polypeptide chain. Repetition of this step assembles a protein one amino acid at a time (figure 11.4). With just the four nucleotides used in three-letter combinations, the 20 standard amino acids are assembled.
The central principle of molecular biology, whereby DNA codes for RNA, which codes for proteins.
Overview of the translation of mRNA into protein. The ribosome binds to mRNA and moves one codon at a time downstream, where transfer RNA drops off an amino acid that links with the previous amino acid, thereby forming a polypeptide chain that continues until the ribosome reaches a stop codon.
Heritability and Genetic Variation
More than 99.9% of the DNA sequence in humans is similar. The 0.1% that differs is what makes each individual unique. Because family members share an even greater proportion of DNA sequence compared with unrelated individuals, analysis of familial aggregation (i.e., resemblance across family members) often is used to determine whether genetic variation contributes to a trait. For a given trait, familial aggregation is tested by comparing the variance between families with the variance within family members. For example, the HERITAGE Family Study examined the familial resemblance for maximal oxygen uptake (![]() O2max), the gold standard measure of cardiorespiratory fitness, in 426 sedentary subjects from 86 nuclear families. The authors found that achieved levels of
O2max), the gold standard measure of cardiorespiratory fitness, in 426 sedentary subjects from 86 nuclear families. The authors found that achieved levels of ![]() O2max clearly aggregate in families; there was 2.7 times more variance between different families than within families for adjusted
O2max clearly aggregate in families; there was 2.7 times more variance between different families than within families for adjusted ![]() O2max. Figure 11.5shows that some families tended to have below-average
O2max. Figure 11.5shows that some families tended to have below-average ![]() O2max values, whereas others had above-average values. Because families share genetic factors as well as similar environmental factors (e.g., diet, education, physical activity, and sedentary behaviors), further analyses are needed to determine whether the familial resemblance in
O2max values, whereas others had above-average values. Because families share genetic factors as well as similar environmental factors (e.g., diet, education, physical activity, and sedentary behaviors), further analyses are needed to determine whether the familial resemblance in ![]() O2max is due to genetic or environmental factors.
O2max is due to genetic or environmental factors.
General depiction of familial aggregation for adjusted
Heritability is an estimate of how much of the variation in a trait is due to genetic factors alone. Heritability estimates are quantified by comparing trait similarities between pairs of relatives with different degrees of relatedness. Thus, twin, adoption, and family studies commonly are used to distinguish between the contribution of genetic and environmental factors on the familial aggregation of a trait. For example, a pattern of significant correlations among siblings and between parents and siblings but not between spouses would imply that the familial resemblance primarily is due to genetic factors, whereas significant correlations between spouses and lesser correlations between siblings or between parents and siblings would suggest a stronger influence of shared environmental factors such as diet and exercise habits. In the HERITAGE Family Study, the authors estimated that the genetic heritability of ![]() O2max was 51%. In addition to
O2max was 51%. In addition to ![]() O2max, numerous exercise-related traits have been shown to have a significant genetic component, as evidenced by their estimated heritability levels from twin and family studies (table 11.5).
O2max, numerous exercise-related traits have been shown to have a significant genetic component, as evidenced by their estimated heritability levels from twin and family studies (table 11.5).
After familial aggregation and heritability have been estimated for a trait, the next step is to determine which specific genetic factors contribute to the trait. Here, the term genetic factors refers to genetic variation or differences in the DNA sequence that may influence the information contained in a gene, thus resulting in trait variability between individuals. A variant nucleotide found at a mutation or polymorphism is known as an allele. Typically, two alleles are found at a polymorphism in the genome (e.g., A and G). Because genes come in pairs (one inherited from the mother and the other from the father), every individual has a pair of alleles for each mutation or polymorphism. The combination of alleles at any mutation or polymorphism is known as a genotype (i.e., that part of the genetic makeup that determines specific characteristics or phenotype). Thus, an individual may have either two copies of the same allele or one copy each of the variant allele. For example, if the nucleotides A and G are found at a particular polymorphism, an individual could have one of the following three genotypes: A/A, A/G, or G/G. An individual is a homozygote if they carry two copies of the same allele (e.g., A/A or G/G), whereas a heterozygote carries one of each allele (e.g., A/G). There are several forms of genetic variation, the most common of which is the single nucleotide polymorphism (SNP). An SNP is a single position in the DNA sequence where more than one nucleotide base is found in greater than 1% of the population. There are more than 10 million SNPs in the human genome. A mutation differs from a polymorphism in that the rare allele is found in less than 1% of the population.
Future Directions and Outlook
The field of exercise genomics has rapidly expanded over the past two decades with the advent of next-generation sequencing technologies, allowing for higher throughput and less expensive sequencing of common and rare variants. However, the field is mired by a general reliance on the candidate gene approach and observational studies with small sample sizes. Furthermore, lack of suitable replication studies or available DNA samples has made the replication of findings a difficult task, particularly for genome-wide studies. Thus, moving forward, exercise genomics needs to utilize a systems biology approach that integrates data from multiple technologies, including genomics, transcriptomics, metabolomics, proteomics, and epigenomics, among others. This will require large, well-designed, well-powered collaborative studies with replication from multiple sources along with the development of computational and bioinformatics tools and expertise within the field. Ultimately, identifying the genetic factors underlying the variability in health- and fitness-related traits due to regular exercise would significantly contribute to the study of the biology of adaptation to exercise and the development of an exercise component of personalized preventive and therapeutic medicine.
Save
Save
Save
Learn more about Advanced Exercise Physiology.
Anaerobic Testing
To accurately determine baseline status in order to guide exercise prescription development and determine whether adaptations occur in response to the exercise training stimulus, one needs to be able to precisely measure the variables of interest.
To accurately determine baseline status in order to guide exercise prescription development and determine whether adaptations occur in response to the exercise training stimulus, one needs to be able to precisely measure the variables of interest. Measures must be both repeatable and accurate (i.e., valid). To attain valid measures, the testing methods used must be performed according to specific guidelines with respect to
- the subject's preparation (e.g., meals, rest, prior exercise, time of day),
- equipment use (e.g., appropriateness of equipment for measuring variables of interest, maintenance, calibration),
- implementation according to testing guidelines applied by the individual conducting the test, and
- proper interpretation of the test results.
Typical variables of interest in anaerobic performance assessment are anaerobic power and anaerobic capacity. Anaerobic power is important for sprint, mid-distance, and distance athletes but for varying reasons. For most athletic events, there is interplay between the aerobic and anaerobic energy systems. Referring to figure 7.1, we see that sprinters (events lasting 4 min) predominantly utilize aerobic metabolic sources. Even aerobic athletes must rely on anaerobic sources at critical times of an event, such as during a hill climb in a bicycle race or the final sprint of a 10K running race.
No direct method of determining anaerobic energy power and capacity currently exists. Although blood lactate accumulation generally is considered to be the product of a high rate of anaerobic glycolysis, blood lactate concentration measurement does not provide specific information about the rate and capacity of the production of ATP. Additionally, the concentration of blood lactate is affected by the rate of its clearance, which differs in individuals due to factors such as - but not limited to - recovery activity status (i.e., active vs. passive); recovery exercise intensity; ratio of individual Type I to Type II skeletal muscle fiber composition; the rate of blood flow to the skeletal muscles, heart, and liver (Cori cycle); and the rate of release of muscle lactate into the blood.
The following is a comprehensive list of common anaerobic tests. The test to be utilized must be specific to the variable being measured. For instance, to measure maximal anaerobic muscle power, a test needs to be very short in duration to isolate the ATP-PCr energy system. Maximal muscle power is used in activities such as jumping and throwing. A vertical jump test is a good example of a short-duration muscle power test. Speed often is thought of as a useful measure, and the 40-yd (36.6 m) dash is used by the National Football League (NFL) to measure speed and provide a ranking of potential draftees. However, a 40-yd dash technically assesses acceleration, velocity, and average speed. The top speed is the fastest instantaneous rate of an object in motion while the average speed is the distance divided by the time to cover that distance. Velocity includes the component of direction of movement; thus, speed is the magnitude component of velocity. NSCA's Guide to Tests and Assessments (Human Kinetics, 2012) provides an excellent review of the performance of anaerobic tests.
Anaerobic Tests
- Vertical jump test
- Margaria-Kalamen power test
- Modified Margaria-Kalamen power test (also known as the football staircase test)
- Three Modified Box Long Jump (MBLJ) test
- Wingate Anaerobic Test (WAnT)
- Critical power test
Various studies have determined that each test in the list is a valid measure of anaerobic power. In particular, the vertical jump test, standing long jump test, Margaria-Kalamen power test, Modified Margaria-Kalamen power test, and three modified box long jump test are considered to be the most sport specific of these tests. The following sections briefly discuss and provide directions for performing several of these anaerobic tests.
Vertical Jump Test
The vertical jump test is commonly used by coaches to measure lower body power and to test an athlete's jumping ability. Previous investigations determined that the vertical jump has high predictive value for measuring power production for athletes participating in such sports as track and field, weightlifting, volleyball, basketball, and football. To test the vertical jump, schools, organizations, and sport teams commonly use a commercially designed device consisting of plastic swivel vanes placed in 0.5-in. (12.7 cm) increments. Because the athlete uses countermovement of the lower body and an outstretched arm swing to reach the highest vane, the vertical jump test is also known as the jump and reach test.
As an example of the sophistication that can be developed for simple tests such as the vertical jump, consider the following. Some researchers believe that the gold standard for measuring the vertical jump includes implementing video analysis and using biomechanical reflective markers on the hip to measure the displacement of the center of mass. Although valid and reliable, this method is cost prohibitive for many fitness and sport organizations. A commercial jump mat is another device used to measure the vertical jump. Embedded in the mat are microswitches that determine flight time - that is, the interval between the liftoff and landing of both feet during a countermovement from a flat-footed standing position. The flight time in the air is used to compute the subject's vertical jump. A study by García-López et al. using three countermovement jumps found that jump mats designed with photo cells showed higher correlations with force plate technologies compared with a contact jump mat. Similarly, Whitmer et al. determined that practitioners using a contact jump mat may underestimate the vertical jump for high performers. A promising new technology for measuring vertical jump is the Myotest (Myotest Inc., Switzerland). The Myotest device is approximately the size of a small smartphone, and the subject wears the device on the hip to determine the displacement of the center of mass. This test does not require the subject to reach and stretch with one arm to displace vanes like when using a vane jump test device. A study by Nuzzo et al. found that the Myotest demonstrated the best intrasession reliability for measuring a countermovement vertical jump when compared with the vane jump test device and jump mat system.
Vertical jump test.
Procedures for the Vertical Jump Test
- Before the test: To measure the highest standing reach, instruct the subject to stand flat footed and reach with one arm fully extended. This should be the same arm that will extend and displace the vanes. Then measure again during plantar flexion with the same arm extended and during plantar flexion. Measure the subject's reach at the middle finger. This measure will be subtracted from the highest recorded vertical jump value.
- During the test: Instruct the subject to take a vertical jump from a standing position using a countermovement. The subject should squat down and back while simultaneously using a bilateral backward arm swing. The subject should then explode upward by extending the hips, knees, ankles (also known as the triple extension), shoulders, elbows, and wrists and attempt to displace the highest vane with one arm (see figure 7.2). Alternatively, a wall-mounted jump-and-reach board may be used.
- Obtain the measurement and repeat two more times. Instruct the subject to rest for 30 s between trials.
- Calculate the maximum vertical jump by subtracting the highest standing reach from the highest vane displaced during the three vertical jumps.
Learn more about Advanced Exercise Physiology.
Using Body Composition Methods to Identify Cachexia in Cancer Patients
Cachexia is not simply weight loss. In some cancer populations, such as patients with early-stage breast cancer, weight gain is actually a more common occurrence that is associated with poor prognosis.
Cachexia is not simply weight loss. In some cancer populations, such as patients with early-stage breast cancer, weight gain is actually a more common occurrence that is associated with poor prognosis. Cachexia is a metabolic syndrome linked to an underlying condition (e.g., cancer, heart failure) that results in the loss of muscle with or without fat that impairs function. Although the mechanisms that lead to cachexia are not fully understood, one factor that differentiates itself from sarcopenia (see "Body Composition and Weight Management Across the Life Span") is an increase in metabolic rate. This increased metabolic rate may be attributable to the cancer tumor itself, especially when the cancer cells spread to metabolically active tissue. An example of this was seen inpatients with colorectal cancer, where an increase in liver mass due to metastatic cancer cells was associated with a concurrent decrease in total muscle mass. Regardless of what triggers the increased metabolic rate, the end result is increased muscle catabolism, which places the cancer patient at higher risk of early death.
One misconception about cachexia is that obese individuals are somehow protected because of increased energy reserves. Although the obesity paradox suggests a protective effect with increases in certain cancer populations (e.g., individuals undergoing chemotherapy), in general BMI does a poor job of classifying those patients with a high mortality risk. The obvious reason why is the inability of BMI to differentiate FFM from FM. Using a bioelectrical impedance analysis, Gonzalez et al. showed that FFM index (i.e., FFM divided by the square of height) was a better predictor of mortality regardless of how much FM was present. In other words, it did not matter if a patient's BMI was higher or lower; if the patient had a reduced amount of muscle mass, the risk of death was increased.
The clinical implications for measuring FM and FFM become evident if you compare two obese patients, one with cachexia and one without. Both patients lose 20 lb (9.1 kg) after a diagnosis of cancer. Using body composition methods, a clinician can identify the higher risk patient. Methods such as the CT measurement of lumbar skeletal muscle currently are being used, although unfortunately not widely. Regardless, the identification of cachexia is one potential area where knowledge of body composition methods can be invaluable.
Learn more about Advanced Exercise Physiology.
Exercise Genomics
The rapidly expanding field of exercise genomics advances our understanding of the preventive and therapeutic properties of exercise by increasing our knowledge about the physiology of exercise and human behavior.
Contribution by Mark A. Sarzynski, PhD, University of South Carolina
The rapidly expanding field of exercise genomics advances our understanding of the preventive and therapeutic properties of exercise by increasing our knowledge about the physiology of exercise and human behavior. Although understanding the effects of various factors (e.g., environmental) on exercise-related phenotypes has long been of interest, understanding of the role of genetic factors (i.e., exercise genomics) is still in its infancy. Most of the major developments have occurred over the past 50 years. This section of the chapter does not have the capacity to fully review the field of genetics; therefore, the following sections introduce the basic concepts of genetics, deoxyribonucleic acid (DNA), and molecular biology relative to exercise physiology. A more thorough review on the topic can be found in Genetics Primer for Exercise Science and Health by Stephen M. Roth (2007).
Basics of Human Genetics
Genetics is the study of genes, heredity, and genetic variation in living organisms. The human genome, which contains all of the genetic material in human cells, consists of about 3 billion DNA base pairs. DNA encodes the instructions for the development, function, and reproduction of the entire human being. DNA is located in both the nucleus of the cell and the mitochondria, the majority of which is located in the nucleus. The nuclear genome comprises 22 pairs of autosomes (non-sex-specific chromosomes) and one pair of sex chromosomes for a total of 46 chromosomes. Humans inherit half of their genome from their mother (22 autosomes and an X chromosome) and half from their father (22 autosomes and either an X or Y chromosome). Women carry two copies of the X chromosome, whereas men carry one X chromosome and one Y chromosome. The presence or absence of the Y chromosome (responsible for testis development) determines the sex of the offspring.
Each DNA molecule consists of two complementary strands that each comprise four nucleotide bases - adenine (A), cytosine (C), guanine (G), and thymine (T) - that form a double helix. The binding between the two DNA strands is complementary: A always binds to T and C with G, creating complementary base pairs. The order of these nucleotide bases determines the meaning of the biological information encoded in that part of the DNA molecule. Specific sequences or regions of DNA that provide instructions to build ribonucleic acid (RNA) and proteins are called genes. Genes are the basic physical and functional units of heredity. The human genome contains about 20,500 genes. DNA found in the mitochondria is a circular double helix and contains 37 genes. The typical structure of a gene consists of many regions, including the coding region (exons), noncoding region (introns), promoter region (5'-end; upstream region; beginning of gene), and 3'-untranslated and terminator regions (3'-end; downstream region; end of gene; figure 11.2). The promoter region contains elements that direct the transcription of a gene (i.e., turn the gene on or off), whereas the terminator region contains the DNA sequence responsible for stopping the transcription of a gene.
The basic structure of a gene, including the upstream promoter region, the coding exons separated by introns, and the downstream terminator region at the end of the gene.
A central tenet of molecular biology describes the flow of information from DNA to RNA to proteins (figure 11.3). During the process of transcription, or gene expression, the nuclear DNA sequence found in a gene is read and copied onto a complementary strand of RNA called premature messenger RNA (mRNA) by the enzyme RNA polymerase. RNA is single stranded and contains the nucleotides A, G, C, and uracil (U), which replaces T and similarly binds only to A. Before the premature mRNA can be used to build protein, the noncoding regions of introns are removed, resulting in mature mRNA that consists of the coding exonic regions only. The mature mRNA then travels out of the nucleus and into the cell's cytoplasm, where it undergoes the process of translation. During translation, the genetic code is read by special organelles in the cell called ribosomes, which pair the mRNA to transfer RNA and eventually attach a corresponding amino acid to the polypeptide chain. Repetition of this step assembles a protein one amino acid at a time (figure 11.4). With just the four nucleotides used in three-letter combinations, the 20 standard amino acids are assembled.
The central principle of molecular biology, whereby DNA codes for RNA, which codes for proteins.
Overview of the translation of mRNA into protein. The ribosome binds to mRNA and moves one codon at a time downstream, where transfer RNA drops off an amino acid that links with the previous amino acid, thereby forming a polypeptide chain that continues until the ribosome reaches a stop codon.
Heritability and Genetic Variation
More than 99.9% of the DNA sequence in humans is similar. The 0.1% that differs is what makes each individual unique. Because family members share an even greater proportion of DNA sequence compared with unrelated individuals, analysis of familial aggregation (i.e., resemblance across family members) often is used to determine whether genetic variation contributes to a trait. For a given trait, familial aggregation is tested by comparing the variance between families with the variance within family members. For example, the HERITAGE Family Study examined the familial resemblance for maximal oxygen uptake (![]() O2max), the gold standard measure of cardiorespiratory fitness, in 426 sedentary subjects from 86 nuclear families. The authors found that achieved levels of
O2max), the gold standard measure of cardiorespiratory fitness, in 426 sedentary subjects from 86 nuclear families. The authors found that achieved levels of ![]() O2max clearly aggregate in families; there was 2.7 times more variance between different families than within families for adjusted
O2max clearly aggregate in families; there was 2.7 times more variance between different families than within families for adjusted ![]() O2max. Figure 11.5shows that some families tended to have below-average
O2max. Figure 11.5shows that some families tended to have below-average ![]() O2max values, whereas others had above-average values. Because families share genetic factors as well as similar environmental factors (e.g., diet, education, physical activity, and sedentary behaviors), further analyses are needed to determine whether the familial resemblance in
O2max values, whereas others had above-average values. Because families share genetic factors as well as similar environmental factors (e.g., diet, education, physical activity, and sedentary behaviors), further analyses are needed to determine whether the familial resemblance in ![]() O2max is due to genetic or environmental factors.
O2max is due to genetic or environmental factors.
General depiction of familial aggregation for adjusted
Heritability is an estimate of how much of the variation in a trait is due to genetic factors alone. Heritability estimates are quantified by comparing trait similarities between pairs of relatives with different degrees of relatedness. Thus, twin, adoption, and family studies commonly are used to distinguish between the contribution of genetic and environmental factors on the familial aggregation of a trait. For example, a pattern of significant correlations among siblings and between parents and siblings but not between spouses would imply that the familial resemblance primarily is due to genetic factors, whereas significant correlations between spouses and lesser correlations between siblings or between parents and siblings would suggest a stronger influence of shared environmental factors such as diet and exercise habits. In the HERITAGE Family Study, the authors estimated that the genetic heritability of ![]() O2max was 51%. In addition to
O2max was 51%. In addition to ![]() O2max, numerous exercise-related traits have been shown to have a significant genetic component, as evidenced by their estimated heritability levels from twin and family studies (table 11.5).
O2max, numerous exercise-related traits have been shown to have a significant genetic component, as evidenced by their estimated heritability levels from twin and family studies (table 11.5).
After familial aggregation and heritability have been estimated for a trait, the next step is to determine which specific genetic factors contribute to the trait. Here, the term genetic factors refers to genetic variation or differences in the DNA sequence that may influence the information contained in a gene, thus resulting in trait variability between individuals. A variant nucleotide found at a mutation or polymorphism is known as an allele. Typically, two alleles are found at a polymorphism in the genome (e.g., A and G). Because genes come in pairs (one inherited from the mother and the other from the father), every individual has a pair of alleles for each mutation or polymorphism. The combination of alleles at any mutation or polymorphism is known as a genotype (i.e., that part of the genetic makeup that determines specific characteristics or phenotype). Thus, an individual may have either two copies of the same allele or one copy each of the variant allele. For example, if the nucleotides A and G are found at a particular polymorphism, an individual could have one of the following three genotypes: A/A, A/G, or G/G. An individual is a homozygote if they carry two copies of the same allele (e.g., A/A or G/G), whereas a heterozygote carries one of each allele (e.g., A/G). There are several forms of genetic variation, the most common of which is the single nucleotide polymorphism (SNP). An SNP is a single position in the DNA sequence where more than one nucleotide base is found in greater than 1% of the population. There are more than 10 million SNPs in the human genome. A mutation differs from a polymorphism in that the rare allele is found in less than 1% of the population.
Future Directions and Outlook
The field of exercise genomics has rapidly expanded over the past two decades with the advent of next-generation sequencing technologies, allowing for higher throughput and less expensive sequencing of common and rare variants. However, the field is mired by a general reliance on the candidate gene approach and observational studies with small sample sizes. Furthermore, lack of suitable replication studies or available DNA samples has made the replication of findings a difficult task, particularly for genome-wide studies. Thus, moving forward, exercise genomics needs to utilize a systems biology approach that integrates data from multiple technologies, including genomics, transcriptomics, metabolomics, proteomics, and epigenomics, among others. This will require large, well-designed, well-powered collaborative studies with replication from multiple sources along with the development of computational and bioinformatics tools and expertise within the field. Ultimately, identifying the genetic factors underlying the variability in health- and fitness-related traits due to regular exercise would significantly contribute to the study of the biology of adaptation to exercise and the development of an exercise component of personalized preventive and therapeutic medicine.
Save
Save
Save
Learn more about Advanced Exercise Physiology.
Anaerobic Testing
To accurately determine baseline status in order to guide exercise prescription development and determine whether adaptations occur in response to the exercise training stimulus, one needs to be able to precisely measure the variables of interest.
To accurately determine baseline status in order to guide exercise prescription development and determine whether adaptations occur in response to the exercise training stimulus, one needs to be able to precisely measure the variables of interest. Measures must be both repeatable and accurate (i.e., valid). To attain valid measures, the testing methods used must be performed according to specific guidelines with respect to
- the subject's preparation (e.g., meals, rest, prior exercise, time of day),
- equipment use (e.g., appropriateness of equipment for measuring variables of interest, maintenance, calibration),
- implementation according to testing guidelines applied by the individual conducting the test, and
- proper interpretation of the test results.
Typical variables of interest in anaerobic performance assessment are anaerobic power and anaerobic capacity. Anaerobic power is important for sprint, mid-distance, and distance athletes but for varying reasons. For most athletic events, there is interplay between the aerobic and anaerobic energy systems. Referring to figure 7.1, we see that sprinters (events lasting 4 min) predominantly utilize aerobic metabolic sources. Even aerobic athletes must rely on anaerobic sources at critical times of an event, such as during a hill climb in a bicycle race or the final sprint of a 10K running race.
No direct method of determining anaerobic energy power and capacity currently exists. Although blood lactate accumulation generally is considered to be the product of a high rate of anaerobic glycolysis, blood lactate concentration measurement does not provide specific information about the rate and capacity of the production of ATP. Additionally, the concentration of blood lactate is affected by the rate of its clearance, which differs in individuals due to factors such as - but not limited to - recovery activity status (i.e., active vs. passive); recovery exercise intensity; ratio of individual Type I to Type II skeletal muscle fiber composition; the rate of blood flow to the skeletal muscles, heart, and liver (Cori cycle); and the rate of release of muscle lactate into the blood.
The following is a comprehensive list of common anaerobic tests. The test to be utilized must be specific to the variable being measured. For instance, to measure maximal anaerobic muscle power, a test needs to be very short in duration to isolate the ATP-PCr energy system. Maximal muscle power is used in activities such as jumping and throwing. A vertical jump test is a good example of a short-duration muscle power test. Speed often is thought of as a useful measure, and the 40-yd (36.6 m) dash is used by the National Football League (NFL) to measure speed and provide a ranking of potential draftees. However, a 40-yd dash technically assesses acceleration, velocity, and average speed. The top speed is the fastest instantaneous rate of an object in motion while the average speed is the distance divided by the time to cover that distance. Velocity includes the component of direction of movement; thus, speed is the magnitude component of velocity. NSCA's Guide to Tests and Assessments (Human Kinetics, 2012) provides an excellent review of the performance of anaerobic tests.
Anaerobic Tests
- Vertical jump test
- Margaria-Kalamen power test
- Modified Margaria-Kalamen power test (also known as the football staircase test)
- Three Modified Box Long Jump (MBLJ) test
- Wingate Anaerobic Test (WAnT)
- Critical power test
Various studies have determined that each test in the list is a valid measure of anaerobic power. In particular, the vertical jump test, standing long jump test, Margaria-Kalamen power test, Modified Margaria-Kalamen power test, and three modified box long jump test are considered to be the most sport specific of these tests. The following sections briefly discuss and provide directions for performing several of these anaerobic tests.
Vertical Jump Test
The vertical jump test is commonly used by coaches to measure lower body power and to test an athlete's jumping ability. Previous investigations determined that the vertical jump has high predictive value for measuring power production for athletes participating in such sports as track and field, weightlifting, volleyball, basketball, and football. To test the vertical jump, schools, organizations, and sport teams commonly use a commercially designed device consisting of plastic swivel vanes placed in 0.5-in. (12.7 cm) increments. Because the athlete uses countermovement of the lower body and an outstretched arm swing to reach the highest vane, the vertical jump test is also known as the jump and reach test.
As an example of the sophistication that can be developed for simple tests such as the vertical jump, consider the following. Some researchers believe that the gold standard for measuring the vertical jump includes implementing video analysis and using biomechanical reflective markers on the hip to measure the displacement of the center of mass. Although valid and reliable, this method is cost prohibitive for many fitness and sport organizations. A commercial jump mat is another device used to measure the vertical jump. Embedded in the mat are microswitches that determine flight time - that is, the interval between the liftoff and landing of both feet during a countermovement from a flat-footed standing position. The flight time in the air is used to compute the subject's vertical jump. A study by García-López et al. using three countermovement jumps found that jump mats designed with photo cells showed higher correlations with force plate technologies compared with a contact jump mat. Similarly, Whitmer et al. determined that practitioners using a contact jump mat may underestimate the vertical jump for high performers. A promising new technology for measuring vertical jump is the Myotest (Myotest Inc., Switzerland). The Myotest device is approximately the size of a small smartphone, and the subject wears the device on the hip to determine the displacement of the center of mass. This test does not require the subject to reach and stretch with one arm to displace vanes like when using a vane jump test device. A study by Nuzzo et al. found that the Myotest demonstrated the best intrasession reliability for measuring a countermovement vertical jump when compared with the vane jump test device and jump mat system.
Vertical jump test.
Procedures for the Vertical Jump Test
- Before the test: To measure the highest standing reach, instruct the subject to stand flat footed and reach with one arm fully extended. This should be the same arm that will extend and displace the vanes. Then measure again during plantar flexion with the same arm extended and during plantar flexion. Measure the subject's reach at the middle finger. This measure will be subtracted from the highest recorded vertical jump value.
- During the test: Instruct the subject to take a vertical jump from a standing position using a countermovement. The subject should squat down and back while simultaneously using a bilateral backward arm swing. The subject should then explode upward by extending the hips, knees, ankles (also known as the triple extension), shoulders, elbows, and wrists and attempt to displace the highest vane with one arm (see figure 7.2). Alternatively, a wall-mounted jump-and-reach board may be used.
- Obtain the measurement and repeat two more times. Instruct the subject to rest for 30 s between trials.
- Calculate the maximum vertical jump by subtracting the highest standing reach from the highest vane displaced during the three vertical jumps.
Learn more about Advanced Exercise Physiology.
Using Body Composition Methods to Identify Cachexia in Cancer Patients
Cachexia is not simply weight loss. In some cancer populations, such as patients with early-stage breast cancer, weight gain is actually a more common occurrence that is associated with poor prognosis.
Cachexia is not simply weight loss. In some cancer populations, such as patients with early-stage breast cancer, weight gain is actually a more common occurrence that is associated with poor prognosis. Cachexia is a metabolic syndrome linked to an underlying condition (e.g., cancer, heart failure) that results in the loss of muscle with or without fat that impairs function. Although the mechanisms that lead to cachexia are not fully understood, one factor that differentiates itself from sarcopenia (see "Body Composition and Weight Management Across the Life Span") is an increase in metabolic rate. This increased metabolic rate may be attributable to the cancer tumor itself, especially when the cancer cells spread to metabolically active tissue. An example of this was seen inpatients with colorectal cancer, where an increase in liver mass due to metastatic cancer cells was associated with a concurrent decrease in total muscle mass. Regardless of what triggers the increased metabolic rate, the end result is increased muscle catabolism, which places the cancer patient at higher risk of early death.
One misconception about cachexia is that obese individuals are somehow protected because of increased energy reserves. Although the obesity paradox suggests a protective effect with increases in certain cancer populations (e.g., individuals undergoing chemotherapy), in general BMI does a poor job of classifying those patients with a high mortality risk. The obvious reason why is the inability of BMI to differentiate FFM from FM. Using a bioelectrical impedance analysis, Gonzalez et al. showed that FFM index (i.e., FFM divided by the square of height) was a better predictor of mortality regardless of how much FM was present. In other words, it did not matter if a patient's BMI was higher or lower; if the patient had a reduced amount of muscle mass, the risk of death was increased.
The clinical implications for measuring FM and FFM become evident if you compare two obese patients, one with cachexia and one without. Both patients lose 20 lb (9.1 kg) after a diagnosis of cancer. Using body composition methods, a clinician can identify the higher risk patient. Methods such as the CT measurement of lumbar skeletal muscle currently are being used, although unfortunately not widely. Regardless, the identification of cachexia is one potential area where knowledge of body composition methods can be invaluable.
Learn more about Advanced Exercise Physiology.
Exercise Genomics
The rapidly expanding field of exercise genomics advances our understanding of the preventive and therapeutic properties of exercise by increasing our knowledge about the physiology of exercise and human behavior.
Contribution by Mark A. Sarzynski, PhD, University of South Carolina
The rapidly expanding field of exercise genomics advances our understanding of the preventive and therapeutic properties of exercise by increasing our knowledge about the physiology of exercise and human behavior. Although understanding the effects of various factors (e.g., environmental) on exercise-related phenotypes has long been of interest, understanding of the role of genetic factors (i.e., exercise genomics) is still in its infancy. Most of the major developments have occurred over the past 50 years. This section of the chapter does not have the capacity to fully review the field of genetics; therefore, the following sections introduce the basic concepts of genetics, deoxyribonucleic acid (DNA), and molecular biology relative to exercise physiology. A more thorough review on the topic can be found in Genetics Primer for Exercise Science and Health by Stephen M. Roth (2007).
Basics of Human Genetics
Genetics is the study of genes, heredity, and genetic variation in living organisms. The human genome, which contains all of the genetic material in human cells, consists of about 3 billion DNA base pairs. DNA encodes the instructions for the development, function, and reproduction of the entire human being. DNA is located in both the nucleus of the cell and the mitochondria, the majority of which is located in the nucleus. The nuclear genome comprises 22 pairs of autosomes (non-sex-specific chromosomes) and one pair of sex chromosomes for a total of 46 chromosomes. Humans inherit half of their genome from their mother (22 autosomes and an X chromosome) and half from their father (22 autosomes and either an X or Y chromosome). Women carry two copies of the X chromosome, whereas men carry one X chromosome and one Y chromosome. The presence or absence of the Y chromosome (responsible for testis development) determines the sex of the offspring.
Each DNA molecule consists of two complementary strands that each comprise four nucleotide bases - adenine (A), cytosine (C), guanine (G), and thymine (T) - that form a double helix. The binding between the two DNA strands is complementary: A always binds to T and C with G, creating complementary base pairs. The order of these nucleotide bases determines the meaning of the biological information encoded in that part of the DNA molecule. Specific sequences or regions of DNA that provide instructions to build ribonucleic acid (RNA) and proteins are called genes. Genes are the basic physical and functional units of heredity. The human genome contains about 20,500 genes. DNA found in the mitochondria is a circular double helix and contains 37 genes. The typical structure of a gene consists of many regions, including the coding region (exons), noncoding region (introns), promoter region (5'-end; upstream region; beginning of gene), and 3'-untranslated and terminator regions (3'-end; downstream region; end of gene; figure 11.2). The promoter region contains elements that direct the transcription of a gene (i.e., turn the gene on or off), whereas the terminator region contains the DNA sequence responsible for stopping the transcription of a gene.
The basic structure of a gene, including the upstream promoter region, the coding exons separated by introns, and the downstream terminator region at the end of the gene.
A central tenet of molecular biology describes the flow of information from DNA to RNA to proteins (figure 11.3). During the process of transcription, or gene expression, the nuclear DNA sequence found in a gene is read and copied onto a complementary strand of RNA called premature messenger RNA (mRNA) by the enzyme RNA polymerase. RNA is single stranded and contains the nucleotides A, G, C, and uracil (U), which replaces T and similarly binds only to A. Before the premature mRNA can be used to build protein, the noncoding regions of introns are removed, resulting in mature mRNA that consists of the coding exonic regions only. The mature mRNA then travels out of the nucleus and into the cell's cytoplasm, where it undergoes the process of translation. During translation, the genetic code is read by special organelles in the cell called ribosomes, which pair the mRNA to transfer RNA and eventually attach a corresponding amino acid to the polypeptide chain. Repetition of this step assembles a protein one amino acid at a time (figure 11.4). With just the four nucleotides used in three-letter combinations, the 20 standard amino acids are assembled.
The central principle of molecular biology, whereby DNA codes for RNA, which codes for proteins.
Overview of the translation of mRNA into protein. The ribosome binds to mRNA and moves one codon at a time downstream, where transfer RNA drops off an amino acid that links with the previous amino acid, thereby forming a polypeptide chain that continues until the ribosome reaches a stop codon.
Heritability and Genetic Variation
More than 99.9% of the DNA sequence in humans is similar. The 0.1% that differs is what makes each individual unique. Because family members share an even greater proportion of DNA sequence compared with unrelated individuals, analysis of familial aggregation (i.e., resemblance across family members) often is used to determine whether genetic variation contributes to a trait. For a given trait, familial aggregation is tested by comparing the variance between families with the variance within family members. For example, the HERITAGE Family Study examined the familial resemblance for maximal oxygen uptake (![]() O2max), the gold standard measure of cardiorespiratory fitness, in 426 sedentary subjects from 86 nuclear families. The authors found that achieved levels of
O2max), the gold standard measure of cardiorespiratory fitness, in 426 sedentary subjects from 86 nuclear families. The authors found that achieved levels of ![]() O2max clearly aggregate in families; there was 2.7 times more variance between different families than within families for adjusted
O2max clearly aggregate in families; there was 2.7 times more variance between different families than within families for adjusted ![]() O2max. Figure 11.5shows that some families tended to have below-average
O2max. Figure 11.5shows that some families tended to have below-average ![]() O2max values, whereas others had above-average values. Because families share genetic factors as well as similar environmental factors (e.g., diet, education, physical activity, and sedentary behaviors), further analyses are needed to determine whether the familial resemblance in
O2max values, whereas others had above-average values. Because families share genetic factors as well as similar environmental factors (e.g., diet, education, physical activity, and sedentary behaviors), further analyses are needed to determine whether the familial resemblance in ![]() O2max is due to genetic or environmental factors.
O2max is due to genetic or environmental factors.
General depiction of familial aggregation for adjusted
Heritability is an estimate of how much of the variation in a trait is due to genetic factors alone. Heritability estimates are quantified by comparing trait similarities between pairs of relatives with different degrees of relatedness. Thus, twin, adoption, and family studies commonly are used to distinguish between the contribution of genetic and environmental factors on the familial aggregation of a trait. For example, a pattern of significant correlations among siblings and between parents and siblings but not between spouses would imply that the familial resemblance primarily is due to genetic factors, whereas significant correlations between spouses and lesser correlations between siblings or between parents and siblings would suggest a stronger influence of shared environmental factors such as diet and exercise habits. In the HERITAGE Family Study, the authors estimated that the genetic heritability of ![]() O2max was 51%. In addition to
O2max was 51%. In addition to ![]() O2max, numerous exercise-related traits have been shown to have a significant genetic component, as evidenced by their estimated heritability levels from twin and family studies (table 11.5).
O2max, numerous exercise-related traits have been shown to have a significant genetic component, as evidenced by their estimated heritability levels from twin and family studies (table 11.5).
After familial aggregation and heritability have been estimated for a trait, the next step is to determine which specific genetic factors contribute to the trait. Here, the term genetic factors refers to genetic variation or differences in the DNA sequence that may influence the information contained in a gene, thus resulting in trait variability between individuals. A variant nucleotide found at a mutation or polymorphism is known as an allele. Typically, two alleles are found at a polymorphism in the genome (e.g., A and G). Because genes come in pairs (one inherited from the mother and the other from the father), every individual has a pair of alleles for each mutation or polymorphism. The combination of alleles at any mutation or polymorphism is known as a genotype (i.e., that part of the genetic makeup that determines specific characteristics or phenotype). Thus, an individual may have either two copies of the same allele or one copy each of the variant allele. For example, if the nucleotides A and G are found at a particular polymorphism, an individual could have one of the following three genotypes: A/A, A/G, or G/G. An individual is a homozygote if they carry two copies of the same allele (e.g., A/A or G/G), whereas a heterozygote carries one of each allele (e.g., A/G). There are several forms of genetic variation, the most common of which is the single nucleotide polymorphism (SNP). An SNP is a single position in the DNA sequence where more than one nucleotide base is found in greater than 1% of the population. There are more than 10 million SNPs in the human genome. A mutation differs from a polymorphism in that the rare allele is found in less than 1% of the population.
Future Directions and Outlook
The field of exercise genomics has rapidly expanded over the past two decades with the advent of next-generation sequencing technologies, allowing for higher throughput and less expensive sequencing of common and rare variants. However, the field is mired by a general reliance on the candidate gene approach and observational studies with small sample sizes. Furthermore, lack of suitable replication studies or available DNA samples has made the replication of findings a difficult task, particularly for genome-wide studies. Thus, moving forward, exercise genomics needs to utilize a systems biology approach that integrates data from multiple technologies, including genomics, transcriptomics, metabolomics, proteomics, and epigenomics, among others. This will require large, well-designed, well-powered collaborative studies with replication from multiple sources along with the development of computational and bioinformatics tools and expertise within the field. Ultimately, identifying the genetic factors underlying the variability in health- and fitness-related traits due to regular exercise would significantly contribute to the study of the biology of adaptation to exercise and the development of an exercise component of personalized preventive and therapeutic medicine.
Save
Save
Save
Learn more about Advanced Exercise Physiology.
Anaerobic Testing
To accurately determine baseline status in order to guide exercise prescription development and determine whether adaptations occur in response to the exercise training stimulus, one needs to be able to precisely measure the variables of interest.
To accurately determine baseline status in order to guide exercise prescription development and determine whether adaptations occur in response to the exercise training stimulus, one needs to be able to precisely measure the variables of interest. Measures must be both repeatable and accurate (i.e., valid). To attain valid measures, the testing methods used must be performed according to specific guidelines with respect to
- the subject's preparation (e.g., meals, rest, prior exercise, time of day),
- equipment use (e.g., appropriateness of equipment for measuring variables of interest, maintenance, calibration),
- implementation according to testing guidelines applied by the individual conducting the test, and
- proper interpretation of the test results.
Typical variables of interest in anaerobic performance assessment are anaerobic power and anaerobic capacity. Anaerobic power is important for sprint, mid-distance, and distance athletes but for varying reasons. For most athletic events, there is interplay between the aerobic and anaerobic energy systems. Referring to figure 7.1, we see that sprinters (events lasting 4 min) predominantly utilize aerobic metabolic sources. Even aerobic athletes must rely on anaerobic sources at critical times of an event, such as during a hill climb in a bicycle race or the final sprint of a 10K running race.
No direct method of determining anaerobic energy power and capacity currently exists. Although blood lactate accumulation generally is considered to be the product of a high rate of anaerobic glycolysis, blood lactate concentration measurement does not provide specific information about the rate and capacity of the production of ATP. Additionally, the concentration of blood lactate is affected by the rate of its clearance, which differs in individuals due to factors such as - but not limited to - recovery activity status (i.e., active vs. passive); recovery exercise intensity; ratio of individual Type I to Type II skeletal muscle fiber composition; the rate of blood flow to the skeletal muscles, heart, and liver (Cori cycle); and the rate of release of muscle lactate into the blood.
The following is a comprehensive list of common anaerobic tests. The test to be utilized must be specific to the variable being measured. For instance, to measure maximal anaerobic muscle power, a test needs to be very short in duration to isolate the ATP-PCr energy system. Maximal muscle power is used in activities such as jumping and throwing. A vertical jump test is a good example of a short-duration muscle power test. Speed often is thought of as a useful measure, and the 40-yd (36.6 m) dash is used by the National Football League (NFL) to measure speed and provide a ranking of potential draftees. However, a 40-yd dash technically assesses acceleration, velocity, and average speed. The top speed is the fastest instantaneous rate of an object in motion while the average speed is the distance divided by the time to cover that distance. Velocity includes the component of direction of movement; thus, speed is the magnitude component of velocity. NSCA's Guide to Tests and Assessments (Human Kinetics, 2012) provides an excellent review of the performance of anaerobic tests.
Anaerobic Tests
- Vertical jump test
- Margaria-Kalamen power test
- Modified Margaria-Kalamen power test (also known as the football staircase test)
- Three Modified Box Long Jump (MBLJ) test
- Wingate Anaerobic Test (WAnT)
- Critical power test
Various studies have determined that each test in the list is a valid measure of anaerobic power. In particular, the vertical jump test, standing long jump test, Margaria-Kalamen power test, Modified Margaria-Kalamen power test, and three modified box long jump test are considered to be the most sport specific of these tests. The following sections briefly discuss and provide directions for performing several of these anaerobic tests.
Vertical Jump Test
The vertical jump test is commonly used by coaches to measure lower body power and to test an athlete's jumping ability. Previous investigations determined that the vertical jump has high predictive value for measuring power production for athletes participating in such sports as track and field, weightlifting, volleyball, basketball, and football. To test the vertical jump, schools, organizations, and sport teams commonly use a commercially designed device consisting of plastic swivel vanes placed in 0.5-in. (12.7 cm) increments. Because the athlete uses countermovement of the lower body and an outstretched arm swing to reach the highest vane, the vertical jump test is also known as the jump and reach test.
As an example of the sophistication that can be developed for simple tests such as the vertical jump, consider the following. Some researchers believe that the gold standard for measuring the vertical jump includes implementing video analysis and using biomechanical reflective markers on the hip to measure the displacement of the center of mass. Although valid and reliable, this method is cost prohibitive for many fitness and sport organizations. A commercial jump mat is another device used to measure the vertical jump. Embedded in the mat are microswitches that determine flight time - that is, the interval between the liftoff and landing of both feet during a countermovement from a flat-footed standing position. The flight time in the air is used to compute the subject's vertical jump. A study by García-López et al. using three countermovement jumps found that jump mats designed with photo cells showed higher correlations with force plate technologies compared with a contact jump mat. Similarly, Whitmer et al. determined that practitioners using a contact jump mat may underestimate the vertical jump for high performers. A promising new technology for measuring vertical jump is the Myotest (Myotest Inc., Switzerland). The Myotest device is approximately the size of a small smartphone, and the subject wears the device on the hip to determine the displacement of the center of mass. This test does not require the subject to reach and stretch with one arm to displace vanes like when using a vane jump test device. A study by Nuzzo et al. found that the Myotest demonstrated the best intrasession reliability for measuring a countermovement vertical jump when compared with the vane jump test device and jump mat system.
Vertical jump test.
Procedures for the Vertical Jump Test
- Before the test: To measure the highest standing reach, instruct the subject to stand flat footed and reach with one arm fully extended. This should be the same arm that will extend and displace the vanes. Then measure again during plantar flexion with the same arm extended and during plantar flexion. Measure the subject's reach at the middle finger. This measure will be subtracted from the highest recorded vertical jump value.
- During the test: Instruct the subject to take a vertical jump from a standing position using a countermovement. The subject should squat down and back while simultaneously using a bilateral backward arm swing. The subject should then explode upward by extending the hips, knees, ankles (also known as the triple extension), shoulders, elbows, and wrists and attempt to displace the highest vane with one arm (see figure 7.2). Alternatively, a wall-mounted jump-and-reach board may be used.
- Obtain the measurement and repeat two more times. Instruct the subject to rest for 30 s between trials.
- Calculate the maximum vertical jump by subtracting the highest standing reach from the highest vane displaced during the three vertical jumps.
Learn more about Advanced Exercise Physiology.
Using Body Composition Methods to Identify Cachexia in Cancer Patients
Cachexia is not simply weight loss. In some cancer populations, such as patients with early-stage breast cancer, weight gain is actually a more common occurrence that is associated with poor prognosis.
Cachexia is not simply weight loss. In some cancer populations, such as patients with early-stage breast cancer, weight gain is actually a more common occurrence that is associated with poor prognosis. Cachexia is a metabolic syndrome linked to an underlying condition (e.g., cancer, heart failure) that results in the loss of muscle with or without fat that impairs function. Although the mechanisms that lead to cachexia are not fully understood, one factor that differentiates itself from sarcopenia (see "Body Composition and Weight Management Across the Life Span") is an increase in metabolic rate. This increased metabolic rate may be attributable to the cancer tumor itself, especially when the cancer cells spread to metabolically active tissue. An example of this was seen inpatients with colorectal cancer, where an increase in liver mass due to metastatic cancer cells was associated with a concurrent decrease in total muscle mass. Regardless of what triggers the increased metabolic rate, the end result is increased muscle catabolism, which places the cancer patient at higher risk of early death.
One misconception about cachexia is that obese individuals are somehow protected because of increased energy reserves. Although the obesity paradox suggests a protective effect with increases in certain cancer populations (e.g., individuals undergoing chemotherapy), in general BMI does a poor job of classifying those patients with a high mortality risk. The obvious reason why is the inability of BMI to differentiate FFM from FM. Using a bioelectrical impedance analysis, Gonzalez et al. showed that FFM index (i.e., FFM divided by the square of height) was a better predictor of mortality regardless of how much FM was present. In other words, it did not matter if a patient's BMI was higher or lower; if the patient had a reduced amount of muscle mass, the risk of death was increased.
The clinical implications for measuring FM and FFM become evident if you compare two obese patients, one with cachexia and one without. Both patients lose 20 lb (9.1 kg) after a diagnosis of cancer. Using body composition methods, a clinician can identify the higher risk patient. Methods such as the CT measurement of lumbar skeletal muscle currently are being used, although unfortunately not widely. Regardless, the identification of cachexia is one potential area where knowledge of body composition methods can be invaluable.
Learn more about Advanced Exercise Physiology.
Related Books