
- Home
- Nutrition and Healthy Eating
- Fitness and Health
- Sport Nutrition

Sport Nutrition, Third Edition, presents the principles and rationale for current nutrition guidelines for athletes. Using a physiological basis, this text provides an in-depth look at the science behind sport nutrition. Students will come away with an understanding of nutrition as it relates to sport and the influence of nutrition on performance, training, and recovery.
This text is organized with the student in mind, with content sequenced in a logical order that puts building blocks in place to facilitate greater comprehension as more advanced topics are introduced. The book moves from general principles of nutrition and nutrient requirements to estimating and fulfilling energy needs with the appropriate combinations of macronutrients and micronutrients. Supplements are addressed from a scientific standpoint, followed by the influence of nutrition on training adaptations, immune function, body composition, weight management, and eating disorders. The new chapter on personalized nutrition covers periodized nutrition, gender differences, and special populations (young athletes, older athletes, and diabetic athletes) and offers practical examples from specific sports.
This third edition contains revised and expanded information to keep students current on the latest findings in sport nutrition:
• Updated nutrition guidelines
• A new chapter on personalized nutrition that helps readers move from theory into practice as they better understand how to customize nutrition based on an individual’s unique background and needs
• Addition of practical carbohydrate intake guidelines for athletes in a wide variety of sports
• Updated information on protein metabolism and recommendations on the type, amount, and timing of protein intake to maximize training adaptation
• Developments from the field of molecular biology that explain how adaptations to exercise training are influenced by nutrition
• Expanded coverage of the rapidly developing field of immunonutrition
Sport Nutrition, Third Edition, includes a number of tools to facilitate student learning. More than 300 figures, tables, and photos offer visual illustration of important concepts, methods, and research findings. Updated and new sidebars provide in-depth coverage of selected topics, making it easier to grasp the scientific concepts presented. Each chapter also includes learning objectives and key points to help students retain the information.
In addition to being mindful of students, the authors remained conscious of the needs of instructors. With years of experience in teaching sport nutrition, the authors constructed chapters in a natural progression, making class lectures easier to prepare and deliver. Instructors will also find an ancillary package consisting of an instructor guide, test package, and presentation package plus image bank to further support their efforts.
More than a simple prescription of recommendations, Sport Nutrition, Third Edition, offers a systematic presentation of the science supporting nutrition guidelines. It is an ideal book to provide a comprehensive understanding of nutrition as it relates to sport, exercise performance, training, and recovery.
Chapter 1. Nutrients and Recommended Intakes
Function of Nutrients
Carbohydrate
Fat
Protein
Water
Alcohol
Vitamins, Minerals, and Trace Elements
Phytonutrients
Recommended Intakes of Nutrients
Development of Recommended Intakes
Current Recommended Intakes
Analyzing Dietary Intake
Chapter 2. Healthy Eating
Health Effects of Consuming Excess Amounts of Nutrients
Practical Guidelines for a Balanced, Healthy Diet
Recommendations for a Healthy Diet and Lifestyle
Nutrition Facts Labels
Nutrient Content and Health Claims on Food Packaging
Processed Food and Additives
Fat Substitutes
Chapter 3. Fuel Sources for Muscle and Exercise Metabolism
Subcellular Skeletal Muscle Structure
Force Generation in Skeletal Muscle
Fiber Types
Energy for Muscle Force Generation
Fuel Stores in Skeletal Muscle
Regulation of Energy Metabolism
Metabolic Responses to Exercise
Metabolic Adaptations to Exercise Training
Chapter 4. Energy
Energetic Efficiency
Measuring the Energy Content of Food
Measuring Energy Expenditure
Components of Energy Expenditure
Energy Balance
Chapter 5. Gastric Emptying, Digestion, and Absorption
Anatomy of the Gastrointestinal Tract
Regulation of the Gastrointestinal Tract
Digestion
Absorption
Gut Microbiota
Regulation of Gastric Emptying
Gastrointestinal Problems During and After Exercise
Chapter 6. Carbohydrate
History
Role of Carbohydrate
Recommendations for Carbohydrate Intake
Carbohydrate Intake in the Days Before Competition
Carbohydrate Intake in the Hours Before Exercise
Carbohydrate Intake 30 to 60 Minutes Before Exercise
Carbohydrate Intake During Exercise
Carbohydrate Intake After Exercise
Chapter 7. Fat
Fat Metabolism During Exercise
Limits to Fat Oxidation
Fat as a Fuel During Exercise
Regulation of Carbohydrate and Fat Metabolism
Fat Supplementation and Exercise
Effects of Diet on Fat Metabolism and Performance
Chapter 8. Protein and Amino Acids
Amino Acids
Techniques to Study Protein and Amino Acid Metabolism
Protein Requirements for Exercise
Training and Protein Metabolism
Effect of Protein Intake on Protein Synthesis
Amino Acids as Ergogenic Aids
Protein Intake and Health Risks
Chapter 9. Water Requirements and Fluid Balance
Thermoregulation and Exercise in the Heat
Effects of Dehydration on Exercise Performance
Mechanisms of Heat Illness
Effects of Fluid Intake on Exercise Performance
Daily Water Balance
Fluid Requirements for Athletes
Chapter 10. Vitamins and Minerals
Water-Soluble and Fat-Soluble Vitamins
Recommended Intakes of Vitamins
Recommended Intakes of Vitamins for Athletes
Macrominerals and Microminerals
Recommended Intakes of Minerals
Critical Micronutrient Functions
Assessing Micronutrient Status
Exercise and Micronutrient Requirements
Ergogenic Effect of Micronutrient Supplementation
Summary of Recommendations for Micronutrient Intake in Athletes
Chapter 11. Nutrition Supplements
Relative Importance of Supplements to a Normal Diet
Nonregulation of Nutrition Supplements
Critical Evaluation of Nutrition Supplements Studies
Androstenedione
Bee Pollen
Beetroot Juice
Beta Alanine and Carnosine
Beta-Hydroxy Beta-Methylbutyrate
Boron
Caffeine
Carnitine
Cherry Juice
Choline
Chromium
Coenzyme Q10
Creatine
Dehydroepiandrosterone
Fish Oil and Omega-3 Fatty Acids
Ginseng
Glandulars
Glycerol
Green Tea
Inosine
Ketone Salts
Lactate Salts and Polylactate
Lecithin
Medium-Chain Triacylglycerol
Pangamic Acid
Phosphatidylserine
Phosphorus and Phosphate Salts
Polyphenols
Pyruvate and Dihydroxyacetone
Sodium Bicarbonate
Sodium Citrate
Sodium Nitrate
Vanadium
Wheat Germ Oil
Additive Effects of Combining Different Supplements
Contamination of Nutrition Supplements
Chapter 12. Nutrition and Training Adaptations
Training Adaptations
Signal Transduction Pathways
Starting a Signaling Cascade
Secondary Signals
Nutrition and Effects on Training Adaptations
Overreaching and the Overtraining Syndrome
Nutrition and Effects on Sleep
Nutrition and Effects on Rehabilitation
Chapter 13. Nutrition and Immune Function in Athletes
Functions of the Immune System and Its Cellular Components
General Mechanism of the Immune Response
Causes of Illness in Athletes
Effects of Exercise on the Immune System
Nutritional Manipulations to Decrease Immunodepression in Athletes
Conclusions and Recommendations
Chapter 14. Body Composition
Optimal Body Weight and Composition
Body Composition Models
Normal Ranges of Body Weight and Body Fat
Body Composition Measurement Techniques
Chapter 15. Weight Management
Genetics
Energy and Macronutrient Intake
Regulation of Appetite
Effect of Exercise on Appetite
Physical Activity and Energy Expenditure
Dietary Weight-Loss Methods
Exercise for Weight Loss
Decreased Resting Metabolic Rate With Weight Loss
Weight Cycling
Gender Differences in Weight Loss
Practicalities of Weight Loss for Athletes
Weight Gain
Chapter 16. Eating Disorders in Athletes
Types of Eating Disorders
Prevalence of Eating Disorders in Athletes
Effects of Eating Disorders on Sports Performance
Effects of Eating Disorders on Health
Treatment and Prevention of Eating Disorders
Chapter 17. Personalized Nutrition
Genetic Influences
Turning Science Into Practice
Specific Populations
Nutrition Application in Different Sport Situations and Populations
Appendix A. Key Concepts in Biological Chemistry Relevant to Sport Nutrition
Appendix B. Unit Conversion Tables
Appendix C. Recommended Daily Allowances for North America
Appendix D. Reference Nutrient Intakes for the United Kingdom
Appendix E. Recommended Dietary Intakes for Australia and New Zealand
Asker Jeukendrup, PhD, is a professor at Loughborough University in the United Kingdom, the director of the Mysportscience performance consulting firm, and cofounder and co-CEO of CORE Nutrition Planning. After obtaining his degrees at Maastricht University in the Netherlands, he spent a year at the University of Texas at Austin before accepting a position at the University of Birmingham in the United Kingdom. At the University of Birmingham, he served for 12 years as the director of the Human Performance Laboratory, heading up the exercise metabolism research group. His research focused on the metabolic responses to exercise, the regulation of carbohydrate and fat metabolism during exercise, adaptations to training, and the influence of nutrition on metabolism and exercise nutrition. He is considered a leading expert in the general areas of sports nutrition, training and overtraining, and recovery.
Jeukendrup received several awards for his achievements, including the Danone Chair at the University of Brussels in 2005. In 2011 he accepted a position as global senior director of exercise physiology at the Gatorade Sports Science Institute, defining strategies for research, education, and sport science services for the largest sports nutrition company in the world. He is a registered sport and exercise nutritionist, having worked with many elite athletes and clubs, including the Rabobank, Lotto-Soudal, and Lotto-Jumbo professional cycling teams; Chelsea Football Club; FC Barcelona; Red Bull Salzburg; UK Athletics; the British Olympic Association; African runners; and several Olympic and world champions. He is currently nutrition performance manager for the Dutch Olympic Committee and head of performance nutrition for the Lotto-Jumbo professional cycling team.
Jeukendrup has published extensively in sport nutrition. He is a fellow of the American College of Sports Medicine and the European College of Sport Science. In his leisure time, he enjoys running, cycling, and competing in triathlons. To date, he has completed 21 Ironman-distance races, including the Ironman Hawaii six times.
Michael Gleeson, PhD, is a professor of exercise biochemistry in the School of Sport, Exercise, and Health Sciences at Loughborough University in Leicestershire, United Kingdom. Gleeson is considered a world authority on exercise biochemistry, immunology, and nutrition, and he has worked with numerous world-class athletes and professional football clubs. He has taught sport nutrition at the university level and has published several books and over 250 scientific articles in scientific and medical journals. He has a particular interest and expertise in the effects of exercise, training, and nutrition on immune function.
Gleeson has been both president and vice president of the International Society of Exercise and Immunology. He is a fellow of the European College of Sport Science and a member of the American College of Sports Medicine, the Physiological Society, and the British Association of Sport and Exercise Sciences.
Gleeson enjoys playing tennis, hill walking, and watching football and films.
Quality of protein
The quality of a protein relates to the degree to which that protein contributes to daily requirements. Various methods have been proposed to measure the protein quality of a food.
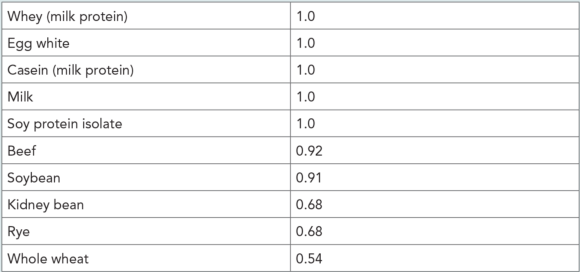
The quality of a protein relates to the degree to which that protein contributes to daily requirements. Various methods have been proposed to measure the protein quality of a food. The most recent method is the protein digestibility corrected amino acid score (PDCAAS). PDCAAS is a method of evaluating protein quality based on the amino acid requirements of humans. Using the PDCAAS, protein-quality rankings are determined by comparing the amino acid profile of a specific food protein against a standard amino acid profile. The maximum score of 1.0 means that after digestion of the protein, it provides, per unit of protein, 100% or more of the indispensable amino acids required. Although this classification was adopted by the U.S. Food and Drug Administration (FDA), the Food and Agricultural Organization of the United Nations, and the World Health Organization in 1993 as “the preferred best” method to determine protein quality, it has received much criticism. People rarely eat a single source of protein; therefore, having the information for individual sources of protein does not give information about the protein quality of the overall diet unless all protein-containing food sources are considered to calculate an average score. In addition, the fact that common protein sources, which have different amino acid profiles, receive identical scores of 1.0 limits its usefulness as a comparative tool. But in the absence of a better method, the PDCAAS is frequently used.
A PDCAAS value of 1.0 is the highest and 0.0 is the lowest. The following are the ratings of some common foods:
Sugar intake and health effects
Over the past century, the yearly intake of simple sugars has increased dramatically to approximately 50 kg (110 lb) per person, which is 25 times more than 100 years ago.
Over the past century, the yearly intake of simple sugars has increased dramatically to approximately 50 kg (110 lb) per person, which is 25 times more than 100 years ago. This change is largely due to increased consumption of soft drinks, but consumption of candy and baked goods also contributes (figure 2.1).
Accumulating evidence indicates that the intake of large amounts of simple sugars is linked to increased risk of obesity and cardiovascular disease, but considerable debate exists about this topic (Gibson 1996; Rippe and Angelopoulos 2016; Slyper 2013). Although sugar consumption is often plotted against obesity rates and a linear correlation is shown, in the last 10 years, sugar consumption has decreased but the development of obesity has not slowed down. Also, the results of studies are not conclusive. Often, epidemiological studies are quoted to support the role of carbohydrate, specifically sugar, in increasing the prevalence of obesity and related diseases. However, a higher sugar intake is often accompanied by higher saturated fat intake and higher energy intake. Therefore, sugar could simply be an indicator of a higher energy intake. A recent analysis of food availability data in the United States confirmed that this is the case. A report by the U.S. Department of Agriculture presented data about the amount of food available for consumption between 1970 and 2014 and estimated what American food consumption was by subtracting food waste. It was found that between 1970 and 2014, food intakes from all major food groups increased (Bentley et al. 2017). In fact, the average total energy intake increased by 474 calories per person; however, most of this increase in energy intake (about 94%) was attributed to an increased consumption of flour, cereal products, and added fats rather than added sugars.
Given that Americans have been eating more and many have sedentary lifestyles (e.g., driving rather than walking or cycling, watching TV, playing video games), it is easy to understand how the obesity epidemic has developed. Carbohydrate and sugar intakes might not be solely to blame, but they are contributing factors.
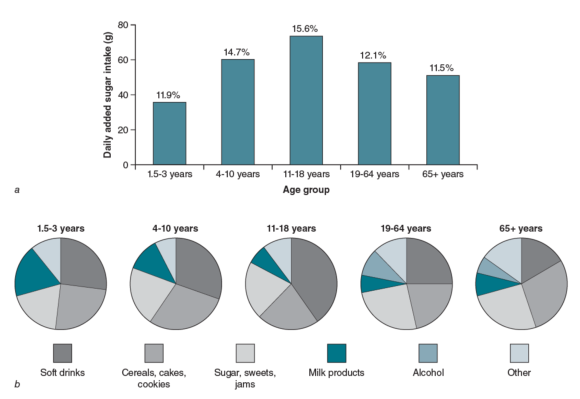
Figure 2.1 Sources of sugar intake in the Western diet: (a) daily added sugar intake by age group and (b) where different age groups get their added sugar.
Data from UK National Diet and Nutrition Survey Rolling Programme (2008/2009 - 2011/12), published 2014. Available: www.gov.uk/government/collections/national-diet-and-nutrition-survey
The carbohydrate mouth rinse phenomenon
One hour of sustained or intermittent high-intensity exercise is not limited by the availability of muscle glycogen stores given adequate nutritional preparation.
One hour of sustained or intermittent high-intensity exercise is not limited by the availability of muscle glycogen stores given adequate nutritional preparation. Therefore, evidence of enhanced performance when carbohydrate is consumed during a variety of such exercise protocols has been perplexing. Findings of a lack of improvement in the performance of a 1-hour cycling time trial protocol with glucose infusion but benefits from carbohydrate ingestion (Carter, Jeukendrup, and Jones 2004) created an intriguing hypothesis that the central nervous system might sense the presence of carbohydrate via receptors in the mouth and oral space, thereby promoting an enhanced sense of well-being and improved pacing. This theory was subsequently confirmed by observations that simply rinsing the mouth with a carbohydrate solution can also enhance performance of the cycling bout (Carter, Jeukendrup, and Jones 2004). A number of studies have now investigated this phenomenon, including several in which brain imaging technology (fMRI) tracked changes in various areas of the brain related to carbohydrate mouth sensing (Chambers, Bridges, and Jones 2009). In these studies, both sweet and nonsweet carbohydrates were shown to activate regions in the brain associated with reward and motor control. There is robust evidence that in situations when a high power output is required over durations of about 45 to 75 minutes, mouth rinsing or ingesting very small amounts of carbohydrate play a nonmetabolic role in enhancing performance by about 2% to 3% (figure 6.6). Not all studies have reported this effect though, possibly because a carbohydrate-rich preevent meal is associated with a dampening of the effect (Jeukendrup and Chambers 2013a).
Mouth rinse studies were initiated to study the mechanisms, not to develop a new strategy whereby athletes rinse their mouths with a carbohydrate solution and then spit it out. Ingesting the carbohydrate solution works just as well. There may be a few situations in which a mouth rinse can be practical, such as when an athlete cannot ingest any carbohydrate because of stomach problems or when energy intake needs to be restricted. Whether the central nervous system effects of glucose feeding are mediated by sensory detection of glucose or perception of sweetness is not known, but studies with placebo solutions containing artificial sweeteners with identical taste to glucose solutions suggest that sweetness is not the key factor (Jeukendrup 2013a, 2014). Brain imaging studies also show that increased brain activity is specific to carbohydrates.
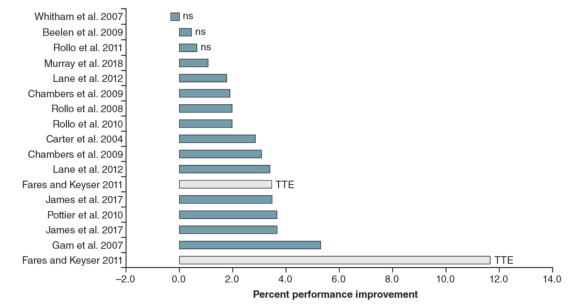
Fig 6.6 Overview of carbohydrate mouth rinse studies. The gray bars indicate time to exhaustion tests as opposed to time trials. The magnitude of performance change is influenced by the type of performance test (i.e., time to exhaustion gives exaggerated changes; time trials provide more realistic estimates of the effects as they are typically more representative of real sporting events). ns = nonsignificant; TTE = time to exhaustion.
© Asker Jeukendrup. www.mysportscience.com
Quality of protein
The quality of a protein relates to the degree to which that protein contributes to daily requirements. Various methods have been proposed to measure the protein quality of a food.
The quality of a protein relates to the degree to which that protein contributes to daily requirements. Various methods have been proposed to measure the protein quality of a food. The most recent method is the protein digestibility corrected amino acid score (PDCAAS). PDCAAS is a method of evaluating protein quality based on the amino acid requirements of humans. Using the PDCAAS, protein-quality rankings are determined by comparing the amino acid profile of a specific food protein against a standard amino acid profile. The maximum score of 1.0 means that after digestion of the protein, it provides, per unit of protein, 100% or more of the indispensable amino acids required. Although this classification was adopted by the U.S. Food and Drug Administration (FDA), the Food and Agricultural Organization of the United Nations, and the World Health Organization in 1993 as “the preferred best” method to determine protein quality, it has received much criticism. People rarely eat a single source of protein; therefore, having the information for individual sources of protein does not give information about the protein quality of the overall diet unless all protein-containing food sources are considered to calculate an average score. In addition, the fact that common protein sources, which have different amino acid profiles, receive identical scores of 1.0 limits its usefulness as a comparative tool. But in the absence of a better method, the PDCAAS is frequently used.
A PDCAAS value of 1.0 is the highest and 0.0 is the lowest. The following are the ratings of some common foods:
Sugar intake and health effects
Over the past century, the yearly intake of simple sugars has increased dramatically to approximately 50 kg (110 lb) per person, which is 25 times more than 100 years ago.
Over the past century, the yearly intake of simple sugars has increased dramatically to approximately 50 kg (110 lb) per person, which is 25 times more than 100 years ago. This change is largely due to increased consumption of soft drinks, but consumption of candy and baked goods also contributes (figure 2.1).
Accumulating evidence indicates that the intake of large amounts of simple sugars is linked to increased risk of obesity and cardiovascular disease, but considerable debate exists about this topic (Gibson 1996; Rippe and Angelopoulos 2016; Slyper 2013). Although sugar consumption is often plotted against obesity rates and a linear correlation is shown, in the last 10 years, sugar consumption has decreased but the development of obesity has not slowed down. Also, the results of studies are not conclusive. Often, epidemiological studies are quoted to support the role of carbohydrate, specifically sugar, in increasing the prevalence of obesity and related diseases. However, a higher sugar intake is often accompanied by higher saturated fat intake and higher energy intake. Therefore, sugar could simply be an indicator of a higher energy intake. A recent analysis of food availability data in the United States confirmed that this is the case. A report by the U.S. Department of Agriculture presented data about the amount of food available for consumption between 1970 and 2014 and estimated what American food consumption was by subtracting food waste. It was found that between 1970 and 2014, food intakes from all major food groups increased (Bentley et al. 2017). In fact, the average total energy intake increased by 474 calories per person; however, most of this increase in energy intake (about 94%) was attributed to an increased consumption of flour, cereal products, and added fats rather than added sugars.
Given that Americans have been eating more and many have sedentary lifestyles (e.g., driving rather than walking or cycling, watching TV, playing video games), it is easy to understand how the obesity epidemic has developed. Carbohydrate and sugar intakes might not be solely to blame, but they are contributing factors.
Figure 2.1 Sources of sugar intake in the Western diet: (a) daily added sugar intake by age group and (b) where different age groups get their added sugar.
Data from UK National Diet and Nutrition Survey Rolling Programme (2008/2009 - 2011/12), published 2014. Available: www.gov.uk/government/collections/national-diet-and-nutrition-survey
The carbohydrate mouth rinse phenomenon
One hour of sustained or intermittent high-intensity exercise is not limited by the availability of muscle glycogen stores given adequate nutritional preparation.
One hour of sustained or intermittent high-intensity exercise is not limited by the availability of muscle glycogen stores given adequate nutritional preparation. Therefore, evidence of enhanced performance when carbohydrate is consumed during a variety of such exercise protocols has been perplexing. Findings of a lack of improvement in the performance of a 1-hour cycling time trial protocol with glucose infusion but benefits from carbohydrate ingestion (Carter, Jeukendrup, and Jones 2004) created an intriguing hypothesis that the central nervous system might sense the presence of carbohydrate via receptors in the mouth and oral space, thereby promoting an enhanced sense of well-being and improved pacing. This theory was subsequently confirmed by observations that simply rinsing the mouth with a carbohydrate solution can also enhance performance of the cycling bout (Carter, Jeukendrup, and Jones 2004). A number of studies have now investigated this phenomenon, including several in which brain imaging technology (fMRI) tracked changes in various areas of the brain related to carbohydrate mouth sensing (Chambers, Bridges, and Jones 2009). In these studies, both sweet and nonsweet carbohydrates were shown to activate regions in the brain associated with reward and motor control. There is robust evidence that in situations when a high power output is required over durations of about 45 to 75 minutes, mouth rinsing or ingesting very small amounts of carbohydrate play a nonmetabolic role in enhancing performance by about 2% to 3% (figure 6.6). Not all studies have reported this effect though, possibly because a carbohydrate-rich preevent meal is associated with a dampening of the effect (Jeukendrup and Chambers 2013a).
Mouth rinse studies were initiated to study the mechanisms, not to develop a new strategy whereby athletes rinse their mouths with a carbohydrate solution and then spit it out. Ingesting the carbohydrate solution works just as well. There may be a few situations in which a mouth rinse can be practical, such as when an athlete cannot ingest any carbohydrate because of stomach problems or when energy intake needs to be restricted. Whether the central nervous system effects of glucose feeding are mediated by sensory detection of glucose or perception of sweetness is not known, but studies with placebo solutions containing artificial sweeteners with identical taste to glucose solutions suggest that sweetness is not the key factor (Jeukendrup 2013a, 2014). Brain imaging studies also show that increased brain activity is specific to carbohydrates.
Fig 6.6 Overview of carbohydrate mouth rinse studies. The gray bars indicate time to exhaustion tests as opposed to time trials. The magnitude of performance change is influenced by the type of performance test (i.e., time to exhaustion gives exaggerated changes; time trials provide more realistic estimates of the effects as they are typically more representative of real sporting events). ns = nonsignificant; TTE = time to exhaustion.
© Asker Jeukendrup. www.mysportscience.com
Quality of protein
The quality of a protein relates to the degree to which that protein contributes to daily requirements. Various methods have been proposed to measure the protein quality of a food.
The quality of a protein relates to the degree to which that protein contributes to daily requirements. Various methods have been proposed to measure the protein quality of a food. The most recent method is the protein digestibility corrected amino acid score (PDCAAS). PDCAAS is a method of evaluating protein quality based on the amino acid requirements of humans. Using the PDCAAS, protein-quality rankings are determined by comparing the amino acid profile of a specific food protein against a standard amino acid profile. The maximum score of 1.0 means that after digestion of the protein, it provides, per unit of protein, 100% or more of the indispensable amino acids required. Although this classification was adopted by the U.S. Food and Drug Administration (FDA), the Food and Agricultural Organization of the United Nations, and the World Health Organization in 1993 as “the preferred best” method to determine protein quality, it has received much criticism. People rarely eat a single source of protein; therefore, having the information for individual sources of protein does not give information about the protein quality of the overall diet unless all protein-containing food sources are considered to calculate an average score. In addition, the fact that common protein sources, which have different amino acid profiles, receive identical scores of 1.0 limits its usefulness as a comparative tool. But in the absence of a better method, the PDCAAS is frequently used.
A PDCAAS value of 1.0 is the highest and 0.0 is the lowest. The following are the ratings of some common foods:
Sugar intake and health effects
Over the past century, the yearly intake of simple sugars has increased dramatically to approximately 50 kg (110 lb) per person, which is 25 times more than 100 years ago.
Over the past century, the yearly intake of simple sugars has increased dramatically to approximately 50 kg (110 lb) per person, which is 25 times more than 100 years ago. This change is largely due to increased consumption of soft drinks, but consumption of candy and baked goods also contributes (figure 2.1).
Accumulating evidence indicates that the intake of large amounts of simple sugars is linked to increased risk of obesity and cardiovascular disease, but considerable debate exists about this topic (Gibson 1996; Rippe and Angelopoulos 2016; Slyper 2013). Although sugar consumption is often plotted against obesity rates and a linear correlation is shown, in the last 10 years, sugar consumption has decreased but the development of obesity has not slowed down. Also, the results of studies are not conclusive. Often, epidemiological studies are quoted to support the role of carbohydrate, specifically sugar, in increasing the prevalence of obesity and related diseases. However, a higher sugar intake is often accompanied by higher saturated fat intake and higher energy intake. Therefore, sugar could simply be an indicator of a higher energy intake. A recent analysis of food availability data in the United States confirmed that this is the case. A report by the U.S. Department of Agriculture presented data about the amount of food available for consumption between 1970 and 2014 and estimated what American food consumption was by subtracting food waste. It was found that between 1970 and 2014, food intakes from all major food groups increased (Bentley et al. 2017). In fact, the average total energy intake increased by 474 calories per person; however, most of this increase in energy intake (about 94%) was attributed to an increased consumption of flour, cereal products, and added fats rather than added sugars.
Given that Americans have been eating more and many have sedentary lifestyles (e.g., driving rather than walking or cycling, watching TV, playing video games), it is easy to understand how the obesity epidemic has developed. Carbohydrate and sugar intakes might not be solely to blame, but they are contributing factors.
Figure 2.1 Sources of sugar intake in the Western diet: (a) daily added sugar intake by age group and (b) where different age groups get their added sugar.
Data from UK National Diet and Nutrition Survey Rolling Programme (2008/2009 - 2011/12), published 2014. Available: www.gov.uk/government/collections/national-diet-and-nutrition-survey
The carbohydrate mouth rinse phenomenon
One hour of sustained or intermittent high-intensity exercise is not limited by the availability of muscle glycogen stores given adequate nutritional preparation.
One hour of sustained or intermittent high-intensity exercise is not limited by the availability of muscle glycogen stores given adequate nutritional preparation. Therefore, evidence of enhanced performance when carbohydrate is consumed during a variety of such exercise protocols has been perplexing. Findings of a lack of improvement in the performance of a 1-hour cycling time trial protocol with glucose infusion but benefits from carbohydrate ingestion (Carter, Jeukendrup, and Jones 2004) created an intriguing hypothesis that the central nervous system might sense the presence of carbohydrate via receptors in the mouth and oral space, thereby promoting an enhanced sense of well-being and improved pacing. This theory was subsequently confirmed by observations that simply rinsing the mouth with a carbohydrate solution can also enhance performance of the cycling bout (Carter, Jeukendrup, and Jones 2004). A number of studies have now investigated this phenomenon, including several in which brain imaging technology (fMRI) tracked changes in various areas of the brain related to carbohydrate mouth sensing (Chambers, Bridges, and Jones 2009). In these studies, both sweet and nonsweet carbohydrates were shown to activate regions in the brain associated with reward and motor control. There is robust evidence that in situations when a high power output is required over durations of about 45 to 75 minutes, mouth rinsing or ingesting very small amounts of carbohydrate play a nonmetabolic role in enhancing performance by about 2% to 3% (figure 6.6). Not all studies have reported this effect though, possibly because a carbohydrate-rich preevent meal is associated with a dampening of the effect (Jeukendrup and Chambers 2013a).
Mouth rinse studies were initiated to study the mechanisms, not to develop a new strategy whereby athletes rinse their mouths with a carbohydrate solution and then spit it out. Ingesting the carbohydrate solution works just as well. There may be a few situations in which a mouth rinse can be practical, such as when an athlete cannot ingest any carbohydrate because of stomach problems or when energy intake needs to be restricted. Whether the central nervous system effects of glucose feeding are mediated by sensory detection of glucose or perception of sweetness is not known, but studies with placebo solutions containing artificial sweeteners with identical taste to glucose solutions suggest that sweetness is not the key factor (Jeukendrup 2013a, 2014). Brain imaging studies also show that increased brain activity is specific to carbohydrates.
Fig 6.6 Overview of carbohydrate mouth rinse studies. The gray bars indicate time to exhaustion tests as opposed to time trials. The magnitude of performance change is influenced by the type of performance test (i.e., time to exhaustion gives exaggerated changes; time trials provide more realistic estimates of the effects as they are typically more representative of real sporting events). ns = nonsignificant; TTE = time to exhaustion.
© Asker Jeukendrup. www.mysportscience.com
Quality of protein
The quality of a protein relates to the degree to which that protein contributes to daily requirements. Various methods have been proposed to measure the protein quality of a food.
The quality of a protein relates to the degree to which that protein contributes to daily requirements. Various methods have been proposed to measure the protein quality of a food. The most recent method is the protein digestibility corrected amino acid score (PDCAAS). PDCAAS is a method of evaluating protein quality based on the amino acid requirements of humans. Using the PDCAAS, protein-quality rankings are determined by comparing the amino acid profile of a specific food protein against a standard amino acid profile. The maximum score of 1.0 means that after digestion of the protein, it provides, per unit of protein, 100% or more of the indispensable amino acids required. Although this classification was adopted by the U.S. Food and Drug Administration (FDA), the Food and Agricultural Organization of the United Nations, and the World Health Organization in 1993 as “the preferred best” method to determine protein quality, it has received much criticism. People rarely eat a single source of protein; therefore, having the information for individual sources of protein does not give information about the protein quality of the overall diet unless all protein-containing food sources are considered to calculate an average score. In addition, the fact that common protein sources, which have different amino acid profiles, receive identical scores of 1.0 limits its usefulness as a comparative tool. But in the absence of a better method, the PDCAAS is frequently used.
A PDCAAS value of 1.0 is the highest and 0.0 is the lowest. The following are the ratings of some common foods:
Sugar intake and health effects
Over the past century, the yearly intake of simple sugars has increased dramatically to approximately 50 kg (110 lb) per person, which is 25 times more than 100 years ago.
Over the past century, the yearly intake of simple sugars has increased dramatically to approximately 50 kg (110 lb) per person, which is 25 times more than 100 years ago. This change is largely due to increased consumption of soft drinks, but consumption of candy and baked goods also contributes (figure 2.1).
Accumulating evidence indicates that the intake of large amounts of simple sugars is linked to increased risk of obesity and cardiovascular disease, but considerable debate exists about this topic (Gibson 1996; Rippe and Angelopoulos 2016; Slyper 2013). Although sugar consumption is often plotted against obesity rates and a linear correlation is shown, in the last 10 years, sugar consumption has decreased but the development of obesity has not slowed down. Also, the results of studies are not conclusive. Often, epidemiological studies are quoted to support the role of carbohydrate, specifically sugar, in increasing the prevalence of obesity and related diseases. However, a higher sugar intake is often accompanied by higher saturated fat intake and higher energy intake. Therefore, sugar could simply be an indicator of a higher energy intake. A recent analysis of food availability data in the United States confirmed that this is the case. A report by the U.S. Department of Agriculture presented data about the amount of food available for consumption between 1970 and 2014 and estimated what American food consumption was by subtracting food waste. It was found that between 1970 and 2014, food intakes from all major food groups increased (Bentley et al. 2017). In fact, the average total energy intake increased by 474 calories per person; however, most of this increase in energy intake (about 94%) was attributed to an increased consumption of flour, cereal products, and added fats rather than added sugars.
Given that Americans have been eating more and many have sedentary lifestyles (e.g., driving rather than walking or cycling, watching TV, playing video games), it is easy to understand how the obesity epidemic has developed. Carbohydrate and sugar intakes might not be solely to blame, but they are contributing factors.
Figure 2.1 Sources of sugar intake in the Western diet: (a) daily added sugar intake by age group and (b) where different age groups get their added sugar.
Data from UK National Diet and Nutrition Survey Rolling Programme (2008/2009 - 2011/12), published 2014. Available: www.gov.uk/government/collections/national-diet-and-nutrition-survey
The carbohydrate mouth rinse phenomenon
One hour of sustained or intermittent high-intensity exercise is not limited by the availability of muscle glycogen stores given adequate nutritional preparation.
One hour of sustained or intermittent high-intensity exercise is not limited by the availability of muscle glycogen stores given adequate nutritional preparation. Therefore, evidence of enhanced performance when carbohydrate is consumed during a variety of such exercise protocols has been perplexing. Findings of a lack of improvement in the performance of a 1-hour cycling time trial protocol with glucose infusion but benefits from carbohydrate ingestion (Carter, Jeukendrup, and Jones 2004) created an intriguing hypothesis that the central nervous system might sense the presence of carbohydrate via receptors in the mouth and oral space, thereby promoting an enhanced sense of well-being and improved pacing. This theory was subsequently confirmed by observations that simply rinsing the mouth with a carbohydrate solution can also enhance performance of the cycling bout (Carter, Jeukendrup, and Jones 2004). A number of studies have now investigated this phenomenon, including several in which brain imaging technology (fMRI) tracked changes in various areas of the brain related to carbohydrate mouth sensing (Chambers, Bridges, and Jones 2009). In these studies, both sweet and nonsweet carbohydrates were shown to activate regions in the brain associated with reward and motor control. There is robust evidence that in situations when a high power output is required over durations of about 45 to 75 minutes, mouth rinsing or ingesting very small amounts of carbohydrate play a nonmetabolic role in enhancing performance by about 2% to 3% (figure 6.6). Not all studies have reported this effect though, possibly because a carbohydrate-rich preevent meal is associated with a dampening of the effect (Jeukendrup and Chambers 2013a).
Mouth rinse studies were initiated to study the mechanisms, not to develop a new strategy whereby athletes rinse their mouths with a carbohydrate solution and then spit it out. Ingesting the carbohydrate solution works just as well. There may be a few situations in which a mouth rinse can be practical, such as when an athlete cannot ingest any carbohydrate because of stomach problems or when energy intake needs to be restricted. Whether the central nervous system effects of glucose feeding are mediated by sensory detection of glucose or perception of sweetness is not known, but studies with placebo solutions containing artificial sweeteners with identical taste to glucose solutions suggest that sweetness is not the key factor (Jeukendrup 2013a, 2014). Brain imaging studies also show that increased brain activity is specific to carbohydrates.
Fig 6.6 Overview of carbohydrate mouth rinse studies. The gray bars indicate time to exhaustion tests as opposed to time trials. The magnitude of performance change is influenced by the type of performance test (i.e., time to exhaustion gives exaggerated changes; time trials provide more realistic estimates of the effects as they are typically more representative of real sporting events). ns = nonsignificant; TTE = time to exhaustion.
© Asker Jeukendrup. www.mysportscience.com
Quality of protein
The quality of a protein relates to the degree to which that protein contributes to daily requirements. Various methods have been proposed to measure the protein quality of a food.
The quality of a protein relates to the degree to which that protein contributes to daily requirements. Various methods have been proposed to measure the protein quality of a food. The most recent method is the protein digestibility corrected amino acid score (PDCAAS). PDCAAS is a method of evaluating protein quality based on the amino acid requirements of humans. Using the PDCAAS, protein-quality rankings are determined by comparing the amino acid profile of a specific food protein against a standard amino acid profile. The maximum score of 1.0 means that after digestion of the protein, it provides, per unit of protein, 100% or more of the indispensable amino acids required. Although this classification was adopted by the U.S. Food and Drug Administration (FDA), the Food and Agricultural Organization of the United Nations, and the World Health Organization in 1993 as “the preferred best” method to determine protein quality, it has received much criticism. People rarely eat a single source of protein; therefore, having the information for individual sources of protein does not give information about the protein quality of the overall diet unless all protein-containing food sources are considered to calculate an average score. In addition, the fact that common protein sources, which have different amino acid profiles, receive identical scores of 1.0 limits its usefulness as a comparative tool. But in the absence of a better method, the PDCAAS is frequently used.
A PDCAAS value of 1.0 is the highest and 0.0 is the lowest. The following are the ratings of some common foods:
Sugar intake and health effects
Over the past century, the yearly intake of simple sugars has increased dramatically to approximately 50 kg (110 lb) per person, which is 25 times more than 100 years ago.
Over the past century, the yearly intake of simple sugars has increased dramatically to approximately 50 kg (110 lb) per person, which is 25 times more than 100 years ago. This change is largely due to increased consumption of soft drinks, but consumption of candy and baked goods also contributes (figure 2.1).
Accumulating evidence indicates that the intake of large amounts of simple sugars is linked to increased risk of obesity and cardiovascular disease, but considerable debate exists about this topic (Gibson 1996; Rippe and Angelopoulos 2016; Slyper 2013). Although sugar consumption is often plotted against obesity rates and a linear correlation is shown, in the last 10 years, sugar consumption has decreased but the development of obesity has not slowed down. Also, the results of studies are not conclusive. Often, epidemiological studies are quoted to support the role of carbohydrate, specifically sugar, in increasing the prevalence of obesity and related diseases. However, a higher sugar intake is often accompanied by higher saturated fat intake and higher energy intake. Therefore, sugar could simply be an indicator of a higher energy intake. A recent analysis of food availability data in the United States confirmed that this is the case. A report by the U.S. Department of Agriculture presented data about the amount of food available for consumption between 1970 and 2014 and estimated what American food consumption was by subtracting food waste. It was found that between 1970 and 2014, food intakes from all major food groups increased (Bentley et al. 2017). In fact, the average total energy intake increased by 474 calories per person; however, most of this increase in energy intake (about 94%) was attributed to an increased consumption of flour, cereal products, and added fats rather than added sugars.
Given that Americans have been eating more and many have sedentary lifestyles (e.g., driving rather than walking or cycling, watching TV, playing video games), it is easy to understand how the obesity epidemic has developed. Carbohydrate and sugar intakes might not be solely to blame, but they are contributing factors.
Figure 2.1 Sources of sugar intake in the Western diet: (a) daily added sugar intake by age group and (b) where different age groups get their added sugar.
Data from UK National Diet and Nutrition Survey Rolling Programme (2008/2009 - 2011/12), published 2014. Available: www.gov.uk/government/collections/national-diet-and-nutrition-survey
The carbohydrate mouth rinse phenomenon
One hour of sustained or intermittent high-intensity exercise is not limited by the availability of muscle glycogen stores given adequate nutritional preparation.
One hour of sustained or intermittent high-intensity exercise is not limited by the availability of muscle glycogen stores given adequate nutritional preparation. Therefore, evidence of enhanced performance when carbohydrate is consumed during a variety of such exercise protocols has been perplexing. Findings of a lack of improvement in the performance of a 1-hour cycling time trial protocol with glucose infusion but benefits from carbohydrate ingestion (Carter, Jeukendrup, and Jones 2004) created an intriguing hypothesis that the central nervous system might sense the presence of carbohydrate via receptors in the mouth and oral space, thereby promoting an enhanced sense of well-being and improved pacing. This theory was subsequently confirmed by observations that simply rinsing the mouth with a carbohydrate solution can also enhance performance of the cycling bout (Carter, Jeukendrup, and Jones 2004). A number of studies have now investigated this phenomenon, including several in which brain imaging technology (fMRI) tracked changes in various areas of the brain related to carbohydrate mouth sensing (Chambers, Bridges, and Jones 2009). In these studies, both sweet and nonsweet carbohydrates were shown to activate regions in the brain associated with reward and motor control. There is robust evidence that in situations when a high power output is required over durations of about 45 to 75 minutes, mouth rinsing or ingesting very small amounts of carbohydrate play a nonmetabolic role in enhancing performance by about 2% to 3% (figure 6.6). Not all studies have reported this effect though, possibly because a carbohydrate-rich preevent meal is associated with a dampening of the effect (Jeukendrup and Chambers 2013a).
Mouth rinse studies were initiated to study the mechanisms, not to develop a new strategy whereby athletes rinse their mouths with a carbohydrate solution and then spit it out. Ingesting the carbohydrate solution works just as well. There may be a few situations in which a mouth rinse can be practical, such as when an athlete cannot ingest any carbohydrate because of stomach problems or when energy intake needs to be restricted. Whether the central nervous system effects of glucose feeding are mediated by sensory detection of glucose or perception of sweetness is not known, but studies with placebo solutions containing artificial sweeteners with identical taste to glucose solutions suggest that sweetness is not the key factor (Jeukendrup 2013a, 2014). Brain imaging studies also show that increased brain activity is specific to carbohydrates.
Fig 6.6 Overview of carbohydrate mouth rinse studies. The gray bars indicate time to exhaustion tests as opposed to time trials. The magnitude of performance change is influenced by the type of performance test (i.e., time to exhaustion gives exaggerated changes; time trials provide more realistic estimates of the effects as they are typically more representative of real sporting events). ns = nonsignificant; TTE = time to exhaustion.
© Asker Jeukendrup. www.mysportscience.com
Quality of protein
The quality of a protein relates to the degree to which that protein contributes to daily requirements. Various methods have been proposed to measure the protein quality of a food.
The quality of a protein relates to the degree to which that protein contributes to daily requirements. Various methods have been proposed to measure the protein quality of a food. The most recent method is the protein digestibility corrected amino acid score (PDCAAS). PDCAAS is a method of evaluating protein quality based on the amino acid requirements of humans. Using the PDCAAS, protein-quality rankings are determined by comparing the amino acid profile of a specific food protein against a standard amino acid profile. The maximum score of 1.0 means that after digestion of the protein, it provides, per unit of protein, 100% or more of the indispensable amino acids required. Although this classification was adopted by the U.S. Food and Drug Administration (FDA), the Food and Agricultural Organization of the United Nations, and the World Health Organization in 1993 as “the preferred best” method to determine protein quality, it has received much criticism. People rarely eat a single source of protein; therefore, having the information for individual sources of protein does not give information about the protein quality of the overall diet unless all protein-containing food sources are considered to calculate an average score. In addition, the fact that common protein sources, which have different amino acid profiles, receive identical scores of 1.0 limits its usefulness as a comparative tool. But in the absence of a better method, the PDCAAS is frequently used.
A PDCAAS value of 1.0 is the highest and 0.0 is the lowest. The following are the ratings of some common foods:
Sugar intake and health effects
Over the past century, the yearly intake of simple sugars has increased dramatically to approximately 50 kg (110 lb) per person, which is 25 times more than 100 years ago.
Over the past century, the yearly intake of simple sugars has increased dramatically to approximately 50 kg (110 lb) per person, which is 25 times more than 100 years ago. This change is largely due to increased consumption of soft drinks, but consumption of candy and baked goods also contributes (figure 2.1).
Accumulating evidence indicates that the intake of large amounts of simple sugars is linked to increased risk of obesity and cardiovascular disease, but considerable debate exists about this topic (Gibson 1996; Rippe and Angelopoulos 2016; Slyper 2013). Although sugar consumption is often plotted against obesity rates and a linear correlation is shown, in the last 10 years, sugar consumption has decreased but the development of obesity has not slowed down. Also, the results of studies are not conclusive. Often, epidemiological studies are quoted to support the role of carbohydrate, specifically sugar, in increasing the prevalence of obesity and related diseases. However, a higher sugar intake is often accompanied by higher saturated fat intake and higher energy intake. Therefore, sugar could simply be an indicator of a higher energy intake. A recent analysis of food availability data in the United States confirmed that this is the case. A report by the U.S. Department of Agriculture presented data about the amount of food available for consumption between 1970 and 2014 and estimated what American food consumption was by subtracting food waste. It was found that between 1970 and 2014, food intakes from all major food groups increased (Bentley et al. 2017). In fact, the average total energy intake increased by 474 calories per person; however, most of this increase in energy intake (about 94%) was attributed to an increased consumption of flour, cereal products, and added fats rather than added sugars.
Given that Americans have been eating more and many have sedentary lifestyles (e.g., driving rather than walking or cycling, watching TV, playing video games), it is easy to understand how the obesity epidemic has developed. Carbohydrate and sugar intakes might not be solely to blame, but they are contributing factors.
Figure 2.1 Sources of sugar intake in the Western diet: (a) daily added sugar intake by age group and (b) where different age groups get their added sugar.
Data from UK National Diet and Nutrition Survey Rolling Programme (2008/2009 - 2011/12), published 2014. Available: www.gov.uk/government/collections/national-diet-and-nutrition-survey
The carbohydrate mouth rinse phenomenon
One hour of sustained or intermittent high-intensity exercise is not limited by the availability of muscle glycogen stores given adequate nutritional preparation.
One hour of sustained or intermittent high-intensity exercise is not limited by the availability of muscle glycogen stores given adequate nutritional preparation. Therefore, evidence of enhanced performance when carbohydrate is consumed during a variety of such exercise protocols has been perplexing. Findings of a lack of improvement in the performance of a 1-hour cycling time trial protocol with glucose infusion but benefits from carbohydrate ingestion (Carter, Jeukendrup, and Jones 2004) created an intriguing hypothesis that the central nervous system might sense the presence of carbohydrate via receptors in the mouth and oral space, thereby promoting an enhanced sense of well-being and improved pacing. This theory was subsequently confirmed by observations that simply rinsing the mouth with a carbohydrate solution can also enhance performance of the cycling bout (Carter, Jeukendrup, and Jones 2004). A number of studies have now investigated this phenomenon, including several in which brain imaging technology (fMRI) tracked changes in various areas of the brain related to carbohydrate mouth sensing (Chambers, Bridges, and Jones 2009). In these studies, both sweet and nonsweet carbohydrates were shown to activate regions in the brain associated with reward and motor control. There is robust evidence that in situations when a high power output is required over durations of about 45 to 75 minutes, mouth rinsing or ingesting very small amounts of carbohydrate play a nonmetabolic role in enhancing performance by about 2% to 3% (figure 6.6). Not all studies have reported this effect though, possibly because a carbohydrate-rich preevent meal is associated with a dampening of the effect (Jeukendrup and Chambers 2013a).
Mouth rinse studies were initiated to study the mechanisms, not to develop a new strategy whereby athletes rinse their mouths with a carbohydrate solution and then spit it out. Ingesting the carbohydrate solution works just as well. There may be a few situations in which a mouth rinse can be practical, such as when an athlete cannot ingest any carbohydrate because of stomach problems or when energy intake needs to be restricted. Whether the central nervous system effects of glucose feeding are mediated by sensory detection of glucose or perception of sweetness is not known, but studies with placebo solutions containing artificial sweeteners with identical taste to glucose solutions suggest that sweetness is not the key factor (Jeukendrup 2013a, 2014). Brain imaging studies also show that increased brain activity is specific to carbohydrates.
Fig 6.6 Overview of carbohydrate mouth rinse studies. The gray bars indicate time to exhaustion tests as opposed to time trials. The magnitude of performance change is influenced by the type of performance test (i.e., time to exhaustion gives exaggerated changes; time trials provide more realistic estimates of the effects as they are typically more representative of real sporting events). ns = nonsignificant; TTE = time to exhaustion.
© Asker Jeukendrup. www.mysportscience.com
Quality of protein
The quality of a protein relates to the degree to which that protein contributes to daily requirements. Various methods have been proposed to measure the protein quality of a food.
The quality of a protein relates to the degree to which that protein contributes to daily requirements. Various methods have been proposed to measure the protein quality of a food. The most recent method is the protein digestibility corrected amino acid score (PDCAAS). PDCAAS is a method of evaluating protein quality based on the amino acid requirements of humans. Using the PDCAAS, protein-quality rankings are determined by comparing the amino acid profile of a specific food protein against a standard amino acid profile. The maximum score of 1.0 means that after digestion of the protein, it provides, per unit of protein, 100% or more of the indispensable amino acids required. Although this classification was adopted by the U.S. Food and Drug Administration (FDA), the Food and Agricultural Organization of the United Nations, and the World Health Organization in 1993 as “the preferred best” method to determine protein quality, it has received much criticism. People rarely eat a single source of protein; therefore, having the information for individual sources of protein does not give information about the protein quality of the overall diet unless all protein-containing food sources are considered to calculate an average score. In addition, the fact that common protein sources, which have different amino acid profiles, receive identical scores of 1.0 limits its usefulness as a comparative tool. But in the absence of a better method, the PDCAAS is frequently used.
A PDCAAS value of 1.0 is the highest and 0.0 is the lowest. The following are the ratings of some common foods:
Sugar intake and health effects
Over the past century, the yearly intake of simple sugars has increased dramatically to approximately 50 kg (110 lb) per person, which is 25 times more than 100 years ago.
Over the past century, the yearly intake of simple sugars has increased dramatically to approximately 50 kg (110 lb) per person, which is 25 times more than 100 years ago. This change is largely due to increased consumption of soft drinks, but consumption of candy and baked goods also contributes (figure 2.1).
Accumulating evidence indicates that the intake of large amounts of simple sugars is linked to increased risk of obesity and cardiovascular disease, but considerable debate exists about this topic (Gibson 1996; Rippe and Angelopoulos 2016; Slyper 2013). Although sugar consumption is often plotted against obesity rates and a linear correlation is shown, in the last 10 years, sugar consumption has decreased but the development of obesity has not slowed down. Also, the results of studies are not conclusive. Often, epidemiological studies are quoted to support the role of carbohydrate, specifically sugar, in increasing the prevalence of obesity and related diseases. However, a higher sugar intake is often accompanied by higher saturated fat intake and higher energy intake. Therefore, sugar could simply be an indicator of a higher energy intake. A recent analysis of food availability data in the United States confirmed that this is the case. A report by the U.S. Department of Agriculture presented data about the amount of food available for consumption between 1970 and 2014 and estimated what American food consumption was by subtracting food waste. It was found that between 1970 and 2014, food intakes from all major food groups increased (Bentley et al. 2017). In fact, the average total energy intake increased by 474 calories per person; however, most of this increase in energy intake (about 94%) was attributed to an increased consumption of flour, cereal products, and added fats rather than added sugars.
Given that Americans have been eating more and many have sedentary lifestyles (e.g., driving rather than walking or cycling, watching TV, playing video games), it is easy to understand how the obesity epidemic has developed. Carbohydrate and sugar intakes might not be solely to blame, but they are contributing factors.
Figure 2.1 Sources of sugar intake in the Western diet: (a) daily added sugar intake by age group and (b) where different age groups get their added sugar.
Data from UK National Diet and Nutrition Survey Rolling Programme (2008/2009 - 2011/12), published 2014. Available: www.gov.uk/government/collections/national-diet-and-nutrition-survey
The carbohydrate mouth rinse phenomenon
One hour of sustained or intermittent high-intensity exercise is not limited by the availability of muscle glycogen stores given adequate nutritional preparation.
One hour of sustained or intermittent high-intensity exercise is not limited by the availability of muscle glycogen stores given adequate nutritional preparation. Therefore, evidence of enhanced performance when carbohydrate is consumed during a variety of such exercise protocols has been perplexing. Findings of a lack of improvement in the performance of a 1-hour cycling time trial protocol with glucose infusion but benefits from carbohydrate ingestion (Carter, Jeukendrup, and Jones 2004) created an intriguing hypothesis that the central nervous system might sense the presence of carbohydrate via receptors in the mouth and oral space, thereby promoting an enhanced sense of well-being and improved pacing. This theory was subsequently confirmed by observations that simply rinsing the mouth with a carbohydrate solution can also enhance performance of the cycling bout (Carter, Jeukendrup, and Jones 2004). A number of studies have now investigated this phenomenon, including several in which brain imaging technology (fMRI) tracked changes in various areas of the brain related to carbohydrate mouth sensing (Chambers, Bridges, and Jones 2009). In these studies, both sweet and nonsweet carbohydrates were shown to activate regions in the brain associated with reward and motor control. There is robust evidence that in situations when a high power output is required over durations of about 45 to 75 minutes, mouth rinsing or ingesting very small amounts of carbohydrate play a nonmetabolic role in enhancing performance by about 2% to 3% (figure 6.6). Not all studies have reported this effect though, possibly because a carbohydrate-rich preevent meal is associated with a dampening of the effect (Jeukendrup and Chambers 2013a).
Mouth rinse studies were initiated to study the mechanisms, not to develop a new strategy whereby athletes rinse their mouths with a carbohydrate solution and then spit it out. Ingesting the carbohydrate solution works just as well. There may be a few situations in which a mouth rinse can be practical, such as when an athlete cannot ingest any carbohydrate because of stomach problems or when energy intake needs to be restricted. Whether the central nervous system effects of glucose feeding are mediated by sensory detection of glucose or perception of sweetness is not known, but studies with placebo solutions containing artificial sweeteners with identical taste to glucose solutions suggest that sweetness is not the key factor (Jeukendrup 2013a, 2014). Brain imaging studies also show that increased brain activity is specific to carbohydrates.
Fig 6.6 Overview of carbohydrate mouth rinse studies. The gray bars indicate time to exhaustion tests as opposed to time trials. The magnitude of performance change is influenced by the type of performance test (i.e., time to exhaustion gives exaggerated changes; time trials provide more realistic estimates of the effects as they are typically more representative of real sporting events). ns = nonsignificant; TTE = time to exhaustion.
© Asker Jeukendrup. www.mysportscience.com
Quality of protein
The quality of a protein relates to the degree to which that protein contributes to daily requirements. Various methods have been proposed to measure the protein quality of a food.
The quality of a protein relates to the degree to which that protein contributes to daily requirements. Various methods have been proposed to measure the protein quality of a food. The most recent method is the protein digestibility corrected amino acid score (PDCAAS). PDCAAS is a method of evaluating protein quality based on the amino acid requirements of humans. Using the PDCAAS, protein-quality rankings are determined by comparing the amino acid profile of a specific food protein against a standard amino acid profile. The maximum score of 1.0 means that after digestion of the protein, it provides, per unit of protein, 100% or more of the indispensable amino acids required. Although this classification was adopted by the U.S. Food and Drug Administration (FDA), the Food and Agricultural Organization of the United Nations, and the World Health Organization in 1993 as “the preferred best” method to determine protein quality, it has received much criticism. People rarely eat a single source of protein; therefore, having the information for individual sources of protein does not give information about the protein quality of the overall diet unless all protein-containing food sources are considered to calculate an average score. In addition, the fact that common protein sources, which have different amino acid profiles, receive identical scores of 1.0 limits its usefulness as a comparative tool. But in the absence of a better method, the PDCAAS is frequently used.
A PDCAAS value of 1.0 is the highest and 0.0 is the lowest. The following are the ratings of some common foods:
Sugar intake and health effects
Over the past century, the yearly intake of simple sugars has increased dramatically to approximately 50 kg (110 lb) per person, which is 25 times more than 100 years ago.
Over the past century, the yearly intake of simple sugars has increased dramatically to approximately 50 kg (110 lb) per person, which is 25 times more than 100 years ago. This change is largely due to increased consumption of soft drinks, but consumption of candy and baked goods also contributes (figure 2.1).
Accumulating evidence indicates that the intake of large amounts of simple sugars is linked to increased risk of obesity and cardiovascular disease, but considerable debate exists about this topic (Gibson 1996; Rippe and Angelopoulos 2016; Slyper 2013). Although sugar consumption is often plotted against obesity rates and a linear correlation is shown, in the last 10 years, sugar consumption has decreased but the development of obesity has not slowed down. Also, the results of studies are not conclusive. Often, epidemiological studies are quoted to support the role of carbohydrate, specifically sugar, in increasing the prevalence of obesity and related diseases. However, a higher sugar intake is often accompanied by higher saturated fat intake and higher energy intake. Therefore, sugar could simply be an indicator of a higher energy intake. A recent analysis of food availability data in the United States confirmed that this is the case. A report by the U.S. Department of Agriculture presented data about the amount of food available for consumption between 1970 and 2014 and estimated what American food consumption was by subtracting food waste. It was found that between 1970 and 2014, food intakes from all major food groups increased (Bentley et al. 2017). In fact, the average total energy intake increased by 474 calories per person; however, most of this increase in energy intake (about 94%) was attributed to an increased consumption of flour, cereal products, and added fats rather than added sugars.
Given that Americans have been eating more and many have sedentary lifestyles (e.g., driving rather than walking or cycling, watching TV, playing video games), it is easy to understand how the obesity epidemic has developed. Carbohydrate and sugar intakes might not be solely to blame, but they are contributing factors.
Figure 2.1 Sources of sugar intake in the Western diet: (a) daily added sugar intake by age group and (b) where different age groups get their added sugar.
Data from UK National Diet and Nutrition Survey Rolling Programme (2008/2009 - 2011/12), published 2014. Available: www.gov.uk/government/collections/national-diet-and-nutrition-survey
The carbohydrate mouth rinse phenomenon
One hour of sustained or intermittent high-intensity exercise is not limited by the availability of muscle glycogen stores given adequate nutritional preparation.
One hour of sustained or intermittent high-intensity exercise is not limited by the availability of muscle glycogen stores given adequate nutritional preparation. Therefore, evidence of enhanced performance when carbohydrate is consumed during a variety of such exercise protocols has been perplexing. Findings of a lack of improvement in the performance of a 1-hour cycling time trial protocol with glucose infusion but benefits from carbohydrate ingestion (Carter, Jeukendrup, and Jones 2004) created an intriguing hypothesis that the central nervous system might sense the presence of carbohydrate via receptors in the mouth and oral space, thereby promoting an enhanced sense of well-being and improved pacing. This theory was subsequently confirmed by observations that simply rinsing the mouth with a carbohydrate solution can also enhance performance of the cycling bout (Carter, Jeukendrup, and Jones 2004). A number of studies have now investigated this phenomenon, including several in which brain imaging technology (fMRI) tracked changes in various areas of the brain related to carbohydrate mouth sensing (Chambers, Bridges, and Jones 2009). In these studies, both sweet and nonsweet carbohydrates were shown to activate regions in the brain associated with reward and motor control. There is robust evidence that in situations when a high power output is required over durations of about 45 to 75 minutes, mouth rinsing or ingesting very small amounts of carbohydrate play a nonmetabolic role in enhancing performance by about 2% to 3% (figure 6.6). Not all studies have reported this effect though, possibly because a carbohydrate-rich preevent meal is associated with a dampening of the effect (Jeukendrup and Chambers 2013a).
Mouth rinse studies were initiated to study the mechanisms, not to develop a new strategy whereby athletes rinse their mouths with a carbohydrate solution and then spit it out. Ingesting the carbohydrate solution works just as well. There may be a few situations in which a mouth rinse can be practical, such as when an athlete cannot ingest any carbohydrate because of stomach problems or when energy intake needs to be restricted. Whether the central nervous system effects of glucose feeding are mediated by sensory detection of glucose or perception of sweetness is not known, but studies with placebo solutions containing artificial sweeteners with identical taste to glucose solutions suggest that sweetness is not the key factor (Jeukendrup 2013a, 2014). Brain imaging studies also show that increased brain activity is specific to carbohydrates.
Fig 6.6 Overview of carbohydrate mouth rinse studies. The gray bars indicate time to exhaustion tests as opposed to time trials. The magnitude of performance change is influenced by the type of performance test (i.e., time to exhaustion gives exaggerated changes; time trials provide more realistic estimates of the effects as they are typically more representative of real sporting events). ns = nonsignificant; TTE = time to exhaustion.
© Asker Jeukendrup. www.mysportscience.com
Quality of protein
The quality of a protein relates to the degree to which that protein contributes to daily requirements. Various methods have been proposed to measure the protein quality of a food.
The quality of a protein relates to the degree to which that protein contributes to daily requirements. Various methods have been proposed to measure the protein quality of a food. The most recent method is the protein digestibility corrected amino acid score (PDCAAS). PDCAAS is a method of evaluating protein quality based on the amino acid requirements of humans. Using the PDCAAS, protein-quality rankings are determined by comparing the amino acid profile of a specific food protein against a standard amino acid profile. The maximum score of 1.0 means that after digestion of the protein, it provides, per unit of protein, 100% or more of the indispensable amino acids required. Although this classification was adopted by the U.S. Food and Drug Administration (FDA), the Food and Agricultural Organization of the United Nations, and the World Health Organization in 1993 as “the preferred best” method to determine protein quality, it has received much criticism. People rarely eat a single source of protein; therefore, having the information for individual sources of protein does not give information about the protein quality of the overall diet unless all protein-containing food sources are considered to calculate an average score. In addition, the fact that common protein sources, which have different amino acid profiles, receive identical scores of 1.0 limits its usefulness as a comparative tool. But in the absence of a better method, the PDCAAS is frequently used.
A PDCAAS value of 1.0 is the highest and 0.0 is the lowest. The following are the ratings of some common foods:
Sugar intake and health effects
Over the past century, the yearly intake of simple sugars has increased dramatically to approximately 50 kg (110 lb) per person, which is 25 times more than 100 years ago.
Over the past century, the yearly intake of simple sugars has increased dramatically to approximately 50 kg (110 lb) per person, which is 25 times more than 100 years ago. This change is largely due to increased consumption of soft drinks, but consumption of candy and baked goods also contributes (figure 2.1).
Accumulating evidence indicates that the intake of large amounts of simple sugars is linked to increased risk of obesity and cardiovascular disease, but considerable debate exists about this topic (Gibson 1996; Rippe and Angelopoulos 2016; Slyper 2013). Although sugar consumption is often plotted against obesity rates and a linear correlation is shown, in the last 10 years, sugar consumption has decreased but the development of obesity has not slowed down. Also, the results of studies are not conclusive. Often, epidemiological studies are quoted to support the role of carbohydrate, specifically sugar, in increasing the prevalence of obesity and related diseases. However, a higher sugar intake is often accompanied by higher saturated fat intake and higher energy intake. Therefore, sugar could simply be an indicator of a higher energy intake. A recent analysis of food availability data in the United States confirmed that this is the case. A report by the U.S. Department of Agriculture presented data about the amount of food available for consumption between 1970 and 2014 and estimated what American food consumption was by subtracting food waste. It was found that between 1970 and 2014, food intakes from all major food groups increased (Bentley et al. 2017). In fact, the average total energy intake increased by 474 calories per person; however, most of this increase in energy intake (about 94%) was attributed to an increased consumption of flour, cereal products, and added fats rather than added sugars.
Given that Americans have been eating more and many have sedentary lifestyles (e.g., driving rather than walking or cycling, watching TV, playing video games), it is easy to understand how the obesity epidemic has developed. Carbohydrate and sugar intakes might not be solely to blame, but they are contributing factors.
Figure 2.1 Sources of sugar intake in the Western diet: (a) daily added sugar intake by age group and (b) where different age groups get their added sugar.
Data from UK National Diet and Nutrition Survey Rolling Programme (2008/2009 - 2011/12), published 2014. Available: www.gov.uk/government/collections/national-diet-and-nutrition-survey
The carbohydrate mouth rinse phenomenon
One hour of sustained or intermittent high-intensity exercise is not limited by the availability of muscle glycogen stores given adequate nutritional preparation.
One hour of sustained or intermittent high-intensity exercise is not limited by the availability of muscle glycogen stores given adequate nutritional preparation. Therefore, evidence of enhanced performance when carbohydrate is consumed during a variety of such exercise protocols has been perplexing. Findings of a lack of improvement in the performance of a 1-hour cycling time trial protocol with glucose infusion but benefits from carbohydrate ingestion (Carter, Jeukendrup, and Jones 2004) created an intriguing hypothesis that the central nervous system might sense the presence of carbohydrate via receptors in the mouth and oral space, thereby promoting an enhanced sense of well-being and improved pacing. This theory was subsequently confirmed by observations that simply rinsing the mouth with a carbohydrate solution can also enhance performance of the cycling bout (Carter, Jeukendrup, and Jones 2004). A number of studies have now investigated this phenomenon, including several in which brain imaging technology (fMRI) tracked changes in various areas of the brain related to carbohydrate mouth sensing (Chambers, Bridges, and Jones 2009). In these studies, both sweet and nonsweet carbohydrates were shown to activate regions in the brain associated with reward and motor control. There is robust evidence that in situations when a high power output is required over durations of about 45 to 75 minutes, mouth rinsing or ingesting very small amounts of carbohydrate play a nonmetabolic role in enhancing performance by about 2% to 3% (figure 6.6). Not all studies have reported this effect though, possibly because a carbohydrate-rich preevent meal is associated with a dampening of the effect (Jeukendrup and Chambers 2013a).
Mouth rinse studies were initiated to study the mechanisms, not to develop a new strategy whereby athletes rinse their mouths with a carbohydrate solution and then spit it out. Ingesting the carbohydrate solution works just as well. There may be a few situations in which a mouth rinse can be practical, such as when an athlete cannot ingest any carbohydrate because of stomach problems or when energy intake needs to be restricted. Whether the central nervous system effects of glucose feeding are mediated by sensory detection of glucose or perception of sweetness is not known, but studies with placebo solutions containing artificial sweeteners with identical taste to glucose solutions suggest that sweetness is not the key factor (Jeukendrup 2013a, 2014). Brain imaging studies also show that increased brain activity is specific to carbohydrates.
Fig 6.6 Overview of carbohydrate mouth rinse studies. The gray bars indicate time to exhaustion tests as opposed to time trials. The magnitude of performance change is influenced by the type of performance test (i.e., time to exhaustion gives exaggerated changes; time trials provide more realistic estimates of the effects as they are typically more representative of real sporting events). ns = nonsignificant; TTE = time to exhaustion.
© Asker Jeukendrup. www.mysportscience.com
Quality of protein
The quality of a protein relates to the degree to which that protein contributes to daily requirements. Various methods have been proposed to measure the protein quality of a food.
The quality of a protein relates to the degree to which that protein contributes to daily requirements. Various methods have been proposed to measure the protein quality of a food. The most recent method is the protein digestibility corrected amino acid score (PDCAAS). PDCAAS is a method of evaluating protein quality based on the amino acid requirements of humans. Using the PDCAAS, protein-quality rankings are determined by comparing the amino acid profile of a specific food protein against a standard amino acid profile. The maximum score of 1.0 means that after digestion of the protein, it provides, per unit of protein, 100% or more of the indispensable amino acids required. Although this classification was adopted by the U.S. Food and Drug Administration (FDA), the Food and Agricultural Organization of the United Nations, and the World Health Organization in 1993 as “the preferred best” method to determine protein quality, it has received much criticism. People rarely eat a single source of protein; therefore, having the information for individual sources of protein does not give information about the protein quality of the overall diet unless all protein-containing food sources are considered to calculate an average score. In addition, the fact that common protein sources, which have different amino acid profiles, receive identical scores of 1.0 limits its usefulness as a comparative tool. But in the absence of a better method, the PDCAAS is frequently used.
A PDCAAS value of 1.0 is the highest and 0.0 is the lowest. The following are the ratings of some common foods:
Sugar intake and health effects
Over the past century, the yearly intake of simple sugars has increased dramatically to approximately 50 kg (110 lb) per person, which is 25 times more than 100 years ago.
Over the past century, the yearly intake of simple sugars has increased dramatically to approximately 50 kg (110 lb) per person, which is 25 times more than 100 years ago. This change is largely due to increased consumption of soft drinks, but consumption of candy and baked goods also contributes (figure 2.1).
Accumulating evidence indicates that the intake of large amounts of simple sugars is linked to increased risk of obesity and cardiovascular disease, but considerable debate exists about this topic (Gibson 1996; Rippe and Angelopoulos 2016; Slyper 2013). Although sugar consumption is often plotted against obesity rates and a linear correlation is shown, in the last 10 years, sugar consumption has decreased but the development of obesity has not slowed down. Also, the results of studies are not conclusive. Often, epidemiological studies are quoted to support the role of carbohydrate, specifically sugar, in increasing the prevalence of obesity and related diseases. However, a higher sugar intake is often accompanied by higher saturated fat intake and higher energy intake. Therefore, sugar could simply be an indicator of a higher energy intake. A recent analysis of food availability data in the United States confirmed that this is the case. A report by the U.S. Department of Agriculture presented data about the amount of food available for consumption between 1970 and 2014 and estimated what American food consumption was by subtracting food waste. It was found that between 1970 and 2014, food intakes from all major food groups increased (Bentley et al. 2017). In fact, the average total energy intake increased by 474 calories per person; however, most of this increase in energy intake (about 94%) was attributed to an increased consumption of flour, cereal products, and added fats rather than added sugars.
Given that Americans have been eating more and many have sedentary lifestyles (e.g., driving rather than walking or cycling, watching TV, playing video games), it is easy to understand how the obesity epidemic has developed. Carbohydrate and sugar intakes might not be solely to blame, but they are contributing factors.
Figure 2.1 Sources of sugar intake in the Western diet: (a) daily added sugar intake by age group and (b) where different age groups get their added sugar.
Data from UK National Diet and Nutrition Survey Rolling Programme (2008/2009 - 2011/12), published 2014. Available: www.gov.uk/government/collections/national-diet-and-nutrition-survey
The carbohydrate mouth rinse phenomenon
One hour of sustained or intermittent high-intensity exercise is not limited by the availability of muscle glycogen stores given adequate nutritional preparation.
One hour of sustained or intermittent high-intensity exercise is not limited by the availability of muscle glycogen stores given adequate nutritional preparation. Therefore, evidence of enhanced performance when carbohydrate is consumed during a variety of such exercise protocols has been perplexing. Findings of a lack of improvement in the performance of a 1-hour cycling time trial protocol with glucose infusion but benefits from carbohydrate ingestion (Carter, Jeukendrup, and Jones 2004) created an intriguing hypothesis that the central nervous system might sense the presence of carbohydrate via receptors in the mouth and oral space, thereby promoting an enhanced sense of well-being and improved pacing. This theory was subsequently confirmed by observations that simply rinsing the mouth with a carbohydrate solution can also enhance performance of the cycling bout (Carter, Jeukendrup, and Jones 2004). A number of studies have now investigated this phenomenon, including several in which brain imaging technology (fMRI) tracked changes in various areas of the brain related to carbohydrate mouth sensing (Chambers, Bridges, and Jones 2009). In these studies, both sweet and nonsweet carbohydrates were shown to activate regions in the brain associated with reward and motor control. There is robust evidence that in situations when a high power output is required over durations of about 45 to 75 minutes, mouth rinsing or ingesting very small amounts of carbohydrate play a nonmetabolic role in enhancing performance by about 2% to 3% (figure 6.6). Not all studies have reported this effect though, possibly because a carbohydrate-rich preevent meal is associated with a dampening of the effect (Jeukendrup and Chambers 2013a).
Mouth rinse studies were initiated to study the mechanisms, not to develop a new strategy whereby athletes rinse their mouths with a carbohydrate solution and then spit it out. Ingesting the carbohydrate solution works just as well. There may be a few situations in which a mouth rinse can be practical, such as when an athlete cannot ingest any carbohydrate because of stomach problems or when energy intake needs to be restricted. Whether the central nervous system effects of glucose feeding are mediated by sensory detection of glucose or perception of sweetness is not known, but studies with placebo solutions containing artificial sweeteners with identical taste to glucose solutions suggest that sweetness is not the key factor (Jeukendrup 2013a, 2014). Brain imaging studies also show that increased brain activity is specific to carbohydrates.
Fig 6.6 Overview of carbohydrate mouth rinse studies. The gray bars indicate time to exhaustion tests as opposed to time trials. The magnitude of performance change is influenced by the type of performance test (i.e., time to exhaustion gives exaggerated changes; time trials provide more realistic estimates of the effects as they are typically more representative of real sporting events). ns = nonsignificant; TTE = time to exhaustion.
© Asker Jeukendrup. www.mysportscience.com
Related Books









