
- Home
- Motor Behaviour
- Kinesiology/Exercise and Sport Science
- Biomechanics
- Anatomy
- Dynamic Human Anatomy

Dynamic Human Anatomy
336 Pages
Dynamic Human Anatomy, Second Edition With Web Study Guide, is back—with a new title, significant new material and learning aids, and the same goals: to cover concepts not found in traditional anatomy texts and to help students apply those concepts.
Formerly titled Dynatomy, the new edition of this introductory to upper-level biomechanics and anatomy text sets itself apart from other texts in this field by connecting biomechanical principles with applications in sports and dance, strength training, work settings, and clinical settings. Dynamic Human Anatomy offers applied dance- and sport-specific information on how the body performs dynamic movement, providing students an understanding of the body’s structure and function as it explores the elegance and complexity of the body’s functional movement anatomy.
New Tools and Learning Aids
Dynamic Human Anatomy comes with many tools and learning aids, including a web study guide and new instructor resources, each featuring new material and tools.
The web study guide offers the following:
• Tables that indicate articulations for the spine and upper and lower extremities
• Tables that list the origin, insertion, action, and innervation for all major muscle groups
• Practice problems that allow students to apply the muscle control formula discussed in chapter 6
• Critical thinking questions
The instructor resources include:
• A presentation package with slides that present the key concepts from the text and can be used for class discussion and demonstration
• An image bank that includes the figures and tables from the book to develop a custom presentation
• An instructor guide that includes a sample syllabus, chapter summaries, lecture outlines, ideas for additional assignments, and answers to the critical thinking questions presented in the web study guide
• A test package that includes 330 questions
Dynamic Human Anatomy also offers a full-color design and learning aids that include an updated glossary, chapter objectives, summaries, and suggested readings. Each chapter has Applying the Concept sidebars, which provide practical examples of concepts, and Research in Mechanics sidebars, which highlight recent research in biomechanics and human movement.
Organized Into Four Parts
Dynamic Human Anatomy is organized into four parts. Part I provides a concise review of relevant anatomical information and neuromechanical concepts. It covers the dynamics of human movement, the essentials of anatomical structure and the organization of the skeletal system. Part II details the essentials of a dynamic approach to movement, including a review of mechanical concepts essential to understanding human movement, the muscle control formula, and topics relevant to movement assessment.
In part III, the focus is on fundamental movements as the chapters examine posture and balance, gait, and basic movement patterns. Part IV explores movement-related aspects for strength and conditioning applications, sport and dance applications, clinical applications, and ergonomic applications.
Brings Anatomy to Life
Dynamic Human Anatomy, Second Edition, explores the potential of the human body to express itself through movement, making it a highly valuable text for students who have taken, or are taking, introductory anatomy and who need a more detailed exposure to concepts in human movement anatomy.
Part I. Anatomical Foundations
Chapter 1. Introduction to Human Anatomy and Movement
Introduction to Human Anatomy
Introduction to Human Movement
Movement Across the Life Span
Anatomical Concepts
Levels of Structural Organization
Anatomical References and Terminology
Study of Human Movement
Concluding Comments
Suggested Readings
Chapter 2. Osteology and the Skeletal System
Functions of the Skeletal System
Bone Histology and Composition
Bone Modeling, Growth, and Development
Skeletal System Organization
Bone Adaptation
Bone Health
Concluding Comments
Suggested Readings
Chapter 3. Joint Anatomy and Function
Joint Structure and Classification
Joint Motion and Movement Description
Types of Joint Movement
Joint Structure and Movement
Concluding Comments
Suggested Readings
Chapter 4. Skeletal Muscle
Functions of Skeletal Muscle
Structure and Function of Skeletal Muscle
Muscle Names
Functional Actions of Muscles
Muscles of Major Joints
Muscle Injury, Pain, and Soreness
Concluding Comments
Suggested Readings
Part II. Biomechanics and Movement Control
Chapter 5. Biomechanics
Biomechanical Concepts
Movement Mechanics
Fluid Mechanics
Joint Mechanics
Material Mechanics
Concluding Comments
Suggested Readings
Chapter 6. Muscular Control of Movement and Movement Assessment
Muscle Function
Muscle Action
Coordination of Movement
Movement Efficiency
Muscle Redundancy and Abundancy
Movement Assessment
Concluding Comments
Suggested Readings
Part III. Fundamentals of Movements
Chapter 7. Posture and Balance
Fundamentals of Posture and Balance
Concluding Comments
Suggested Readings
Chapter 8. Gait
Walking
Running
Concluding Comments
Suggested Readings
Chapter 9. Basic Movement Patterns
Jumping
Kicking
Lifting
Throwing
Striking
Concluding Comments
Suggested Readings
Part IV. Movement Applications
Chapter 10. Strength and Conditioning Applications
General Principles
Types of Strength and Conditioning Programs
Resistance Training
Concluding Comments
Suggested Readings
Chapter 11. Sport and Dance Applications
American Football
Baseball and Softball
Basketball
Cycling
Golf
Soccer
Swimming
Tennis
Volleyball
Dance Applications
Concluding Comments
Suggested Readings
Chapter 12. Clinical Applications
Concepts of Musculoskeletal Injury
Injury Prevention
Rehabilitation
Common Injuries
Prosthetics and Orthotics
Concluding Comments
Suggested Readings
Chapter 13. Ergonomics Applications
Ergonomic Concepts
Lifting
Overuse Conditions
Concluding Comments
Suggested Readings
William C. Whiting, PhD, is a professor and codirector of the biomechanics laboratory in the department of kinesiology at California State University at Northridge, where he has won both the Distinguished Teaching Award and Scholarly Publication Award. Whiting earned his PhD in kinesiology at UCLA. He has taught courses in biomechanics and human anatomy for more than 35 years and has published more than 40 articles and 30 research abstracts. He is coauthor of Biomechanics of Musculoskeletal Injury.
Whiting currently serves on the editorial board of NSCA’s Journal of Strength and Conditioning Research and serves as a reviewer for a number of scholarly journals. Whiting is a fellow of the American College of Sports Medicine (ACSM) and has served as president of the Southwest Regional Chapter of ACSM. He is also a member of the American Society of Biomechanics; the International Society of Biomechanics; and the National Strength and Conditioning Association.
In his leisure time, Whiting enjoys playing basketball and volleyball, reading, camping, and hiking. He lives in Glendale, California, with his wife, Marji; sons, Trevor and Tad; and daughter, Emmi.
Components of muscle function
The control of even the simplest joint movement typically requires the cooperative action of several muscles working together as a single unit. This cooperative action is called muscle synergy.
The control of even the simplest joint movement typically requires the cooperative action of several muscles working together as a single unit. This cooperative action is called muscle synergy. Synergistic muscles work together, but other muscles with opposite functions may work against a particular movement. The overall, or net, effect of all muscles acting at a joint determines the ultimate mechanical effect, or movement.
Several concepts of muscle function are important for understanding how muscles cooperate and compete to control movement: agonists, neutralization, stabilization, antagonists, and coactivation.
- Agonists. Muscles that actively produce or control a single joint movement or maintain a single joint position are called agonists. In most movements, several muscles act together as agonists, with some playing a greater role than others.
- Neutralization. Muscles often perform more than one movement function at a given joint. At the ankle complex, for example, a muscle might act as both a plantar flexor and invertor (e.g., tibialis posterior). To produce pure plantar flexion, another muscle whose action produces plantar flexion and eversion (e.g., peroneus longus) would also need to be involved. The eversion action of the second muscle would cancel out, or neutralize, the inversion action of the first muscle. This process of canceling out an unwanted secondary movement is called neutralization.
- Stabilization. During concentric action, a muscle attempts to shorten by pulling its two bony attachment sites together. In most cases, the bone with the least resistance to movement (inertia) will move. When the inertia of both bones is similar in magnitude, both ends tend to move. If movement of only one end is desired, the other end must be prevented from moving, or stabilized. This stabilization is provided by other muscles or an external force. As an example, consider hip flexion created by the anterior thigh musculature. In attempting to move the femur in flexion, the hip flexors also tilt the pelvis anteriorly. If pelvic tilt is unwanted, then the abdominal musculature must act isometrically to stabilize the pelvis and prevent its movement.
- Antagonists. Muscles acting against a movement or position are called antagonists. To perform a movement most effectively, when the agonists actively shorten in concentric action, the corresponding antagonists passively lengthen. When agonists actively lengthen in eccentric action, the associated antagonists passively shorten. In many movements, then, the agonists and stabilizers are active while the antagonists are passive.
- Coactivation . Simultaneous action of both agonists and antagonists is called coactivation (also co-contraction). Coactivation might occur, for example, when an unskilled performer is unsure of the necessary muscle recruitment strategy. Skilled performers, however, do not exhibit an absence of coactivation. At least four possible explanations exist for coactivation in skilled performers: (1) less overall effort may be required in agonist - antagonist pairings for movements that involve changes of direction when the muscles maintain some level of activity, as opposed to working in an on - off manner; (2) coactivation increases joint stiffness and consequently joint stability, which may be desired for movements involving heavy loads; (3) coactivation of a single-joint muscle (e.g., gluteus maximus) and a two-joint muscle (e.g., rectus femoris) can increase the torque at a joint (e.g., knee) acted on by the two-joint muscle; and (4) given the neural complexities of the forearm and hand, fine movements of the fingers require complex coactivation strategies (Enoka, 2002).
Note that the term coactivation is limited to the concurrent action of agonists and antagonists and should not be used to describe the simultaneous action of multiple agonists. For instance, concurrent activity of the biceps brachii and triceps brachii during an elbow curl exercise would be considered coactivation. On the other hand, if the triceps was passive (i.e., inactive), simultaneous action of the three elbow flexors (biceps brachii, brachialis, brachioradialis) would not be considered coactivation.
With these concepts in mind, we now consider a simple yet fundamental question: How do we determine which muscles are active in producing or controlling a given movement?
Learn more about Dynamic Human Anatomy, Second Edition.
Determine the involved muscles and their action for any joint movement
One of the most fundamental and important goals of movement analysis is identifying which specific muscles are active in producing and controlling movement at a particular joint.
One of the most fundamental and important goals of movement analysis is identifying which specific muscles are active in producing and controlling movement at a particular joint. In chapter 4, we presented specific muscles and their concentric actions. However, we know that muscles can act in three modes: isometric, concentric, and eccentric. The task at hand, therefore, is to determine for a given joint movement (1) the specific muscles involved in controlling the movement and (2) the type of muscle action.
The following muscle control formula provides a step-by-step procedure for determining the involved muscles and their action for any joint movement. This formula may appear a bit cumbersome and complex at first glance. However, with practice, you should be able to get through it quickly. Eventually (with enough practice), the process will become automatic and instinctive, and you will be able to analyze movements without consciously going through each step in the formula. It helps, though, to use the formula until you develop these movement analysis instincts.
Muscle Control Formula
We begin the muscle control formula with a statement of the problem: Given a specific joint movement (or position), identify the name of the movement (or position), the plane of movement, the effect of the external force acting on the system, the type of muscle action (i.e., shortening or concentric, lengthening or eccentric, or isometric), and the muscles involved (i.e., which muscle or muscles are actively involved in producing or controlling the movement or in maintaining a position).
Now, we move on to the formula itself, which involves six steps:
- Step 1: Identify the joint movement (e.g., flexion, abduction) or position.
- Step 2: Identify the effect of the external force (e.g., gravity) on the joint movement or position by asking the following question: What movement would the external force produce in the absence of muscle action (i.e., if there were no active muscles)?
- Step 3: Identify the type of muscle action (concentric, eccentric, isometric) based on the answers to step 1 (#1) and step 2 (#2) as follows:
- If #1 and #2 are in opposite directions, then the muscles are actively shortening in a concentric action. Speed of movement is not a factor.
- If #1 and #2 are in the same direction, then ask yourself, "What is the speed of movement?"
- If the movement is faster than what the external force would produce by itself, then the muscles are actively shortening in a concentric action.
- If the movement is slower than what the external force would produce by itself, then the muscles are actively lengthening in an eccentric action.
- If no movement is occurring, yet the external force would produce movement if acting by itself, then the muscles are performing an isometric action.
- Movements across gravity (i.e., parallel to the ground) are produced by a concentric action. When gravity cannot influence the joint movement in question, shortening (concentric) action is needed to pull the bone against its own inertia. The speed of movement is not a factor.
By this point, we have identified the type of muscle action. The next steps identify which muscles control the movement.
- Step 4: Identify the plane of movement (frontal, sagittal, transverse) and the axis of rotation (i.e., line about which the joint is rotating). The purpose of this step is to identify which side of the joint the muscles controlling the movement cross (e.g., flexors cross one side of a joint, while extensors cross the opposite side).
- Step 5:Ask yourself, "On which side of the joint axis are muscles lengthening and on which side are they shortening during the movement?"
- Step 6: Combine the information from steps 3 and 5 to determine which muscles must be producing or controlling the movement (or position). For example, if a concentric (shortening) action is required (from step 3) and the muscles on the anterior side of the joint are shortening (from step 5), then the anterior muscles must be actively producing the movement. The information in chapter 4 allows us to name the specific muscles.
Learn more about Dynamic Human Anatomy, Second Edition.
Ergonomic concepts
As an interdiscipline, ergonomics spans a variety of disciplines, including human anatomy, biomechanics, physiology, psychology, sociology, medicine, and engineering.
As an interdiscipline, ergonomics spans a variety of disciplines, including human anatomy, biomechanics, physiology, psychology, sociology, medicine, and engineering. Ergonomics is composed of three primary domains: organizational, cognitive, and physical. The organizational domain deals with organizational design, policies, and processes as they relate to workplace communication, work design and systems, networking, and teamwork. The cognitive domain involves mental processes, including perception, memory, reasoning, and motor response.
The physical domain is most relevant to our study of dynamic human anatomy. This domain integrates anthropometric, biomechanical, and physiological concepts as they relate to human movement, primarily in occupational settings. The principles of physical ergonomics have been used extensively in the design of consumer and industrial products, assessment of manual materials handling tasks, development of workplace safety guidelines, workplace design, and diagnosis of work-related medical conditions.
Goals
The primary goals of ergonomics are to improve productivity, improve efficiency, enhance safety, reduce injury risk, and reduce cost. Ergonomic interventions can improve both the quantity and quality of worker output and increase efficiency by facilitating production in a time-effective manner.
Safety enhancement and injury risk reduction are at the core of most ergonomic programs. One of the most common worker risks is a class of conditions collectively known as musculoskeletal disorders(MSDs). MSDs are the risk factor most closely associated with human movement tasks.
Research consistently has shown that ergonomic analysis and intervention can result in significant cost savings by reducing health care costs, lost work time, workers' compensation claims, and human error. Many ergonomic interventions are relatively inexpensive and are therefore cost effective for businesses, agencies, and workers alike.
Many governmental agencies and professional organizations have issued safety guidelines addressing specific ergonomic issues and recommendations. These guidelines cover a multitude of industrial and service areas, including agriculture, apparel and footwear, baggage handling, computer workstations, construction, health care, product manufacturing, metalwork foundries, meatpacking, mining, poultry processing, printing, sewing, shipyards, and telecommunications (U.S. Department of Labor, n.d.).
Methods of Analysis
Ergonomic analyses can be reactive or proactive. A reactive analysis addresses an existing problem or situation. A proactive analysis seeks to anticipate potential problems and make changes that prevent these problems.
An ergonomic analysis typically involves several steps, the first of which is identification of risk factors. General risk factors associated with movement-related ergonomic problems include awkward postures, repetitive motions, forceful exertions, pressure points, and sustained static postures(NIOSH, 2007).
In conducting an ergonomic assessment, the first step is to identify risk factors specific to the situation being assessed. Risk factors may be systematic (i.e., evident in the overall work environment) or specific to an individual. In assessing the work environment of a computer data-entry operator, for example, potential risk factors might include keyboard height and inclination, monitor height (relative to the operator's line of sight), distance, brightness, lack of arm and wrist support, chair design and support, and operator posture.
Once the ergonomic risk factors have been identified, the ergonomist must identify possible changes (e.g., new or adjusted keyboard, monitor, chair) to improve comfort and safety. After the changes have been implemented, the worker should be re-evaluated to ensure that the modifications have achieved the ergonomic goals.
Risk factors that are common to a group of workers can be addressed through either engineering or administrative controls. Engineering controls involve improving worker conditions by modifying tasks, adjusting movement patterns, redesigning workstations or tools, and providing protective equipment, as needed. Administrative controls include development and implementation of procedures and processes that can reduce risk such as job rotation (i.e., varying work tasks) and appropriate work breaks (e.g., rest or stretching breaks).
Numerous analysis approaches have been used to identify ergonomic problems and find solutions. Among those approaches are surveys and questionnaires, iterative prototyping, meta-analysis, work sampling, and a wide range of computer-based models applicable to specific tasks or systems.
Human - Machine Interface
Many occupations involve human interaction with a machine or device, in what is termed a human - machine interface. Examples include computer or keyboard operators (figure 13.1), assembly-line and construction workers, medical technicians and clinicians, and automobile mechanics.
Computer workstation anthropometrics for seated (left) and standing (right) operators.
Learn more about Dynamic Human Anatomy, Second Edition.
Components of muscle function
The control of even the simplest joint movement typically requires the cooperative action of several muscles working together as a single unit. This cooperative action is called muscle synergy.
The control of even the simplest joint movement typically requires the cooperative action of several muscles working together as a single unit. This cooperative action is called muscle synergy. Synergistic muscles work together, but other muscles with opposite functions may work against a particular movement. The overall, or net, effect of all muscles acting at a joint determines the ultimate mechanical effect, or movement.
Several concepts of muscle function are important for understanding how muscles cooperate and compete to control movement: agonists, neutralization, stabilization, antagonists, and coactivation.
- Agonists. Muscles that actively produce or control a single joint movement or maintain a single joint position are called agonists. In most movements, several muscles act together as agonists, with some playing a greater role than others.
- Neutralization. Muscles often perform more than one movement function at a given joint. At the ankle complex, for example, a muscle might act as both a plantar flexor and invertor (e.g., tibialis posterior). To produce pure plantar flexion, another muscle whose action produces plantar flexion and eversion (e.g., peroneus longus) would also need to be involved. The eversion action of the second muscle would cancel out, or neutralize, the inversion action of the first muscle. This process of canceling out an unwanted secondary movement is called neutralization.
- Stabilization. During concentric action, a muscle attempts to shorten by pulling its two bony attachment sites together. In most cases, the bone with the least resistance to movement (inertia) will move. When the inertia of both bones is similar in magnitude, both ends tend to move. If movement of only one end is desired, the other end must be prevented from moving, or stabilized. This stabilization is provided by other muscles or an external force. As an example, consider hip flexion created by the anterior thigh musculature. In attempting to move the femur in flexion, the hip flexors also tilt the pelvis anteriorly. If pelvic tilt is unwanted, then the abdominal musculature must act isometrically to stabilize the pelvis and prevent its movement.
- Antagonists. Muscles acting against a movement or position are called antagonists. To perform a movement most effectively, when the agonists actively shorten in concentric action, the corresponding antagonists passively lengthen. When agonists actively lengthen in eccentric action, the associated antagonists passively shorten. In many movements, then, the agonists and stabilizers are active while the antagonists are passive.
- Coactivation . Simultaneous action of both agonists and antagonists is called coactivation (also co-contraction). Coactivation might occur, for example, when an unskilled performer is unsure of the necessary muscle recruitment strategy. Skilled performers, however, do not exhibit an absence of coactivation. At least four possible explanations exist for coactivation in skilled performers: (1) less overall effort may be required in agonist - antagonist pairings for movements that involve changes of direction when the muscles maintain some level of activity, as opposed to working in an on - off manner; (2) coactivation increases joint stiffness and consequently joint stability, which may be desired for movements involving heavy loads; (3) coactivation of a single-joint muscle (e.g., gluteus maximus) and a two-joint muscle (e.g., rectus femoris) can increase the torque at a joint (e.g., knee) acted on by the two-joint muscle; and (4) given the neural complexities of the forearm and hand, fine movements of the fingers require complex coactivation strategies (Enoka, 2002).
Note that the term coactivation is limited to the concurrent action of agonists and antagonists and should not be used to describe the simultaneous action of multiple agonists. For instance, concurrent activity of the biceps brachii and triceps brachii during an elbow curl exercise would be considered coactivation. On the other hand, if the triceps was passive (i.e., inactive), simultaneous action of the three elbow flexors (biceps brachii, brachialis, brachioradialis) would not be considered coactivation.
With these concepts in mind, we now consider a simple yet fundamental question: How do we determine which muscles are active in producing or controlling a given movement?
Learn more about Dynamic Human Anatomy, Second Edition.
Determine the involved muscles and their action for any joint movement
One of the most fundamental and important goals of movement analysis is identifying which specific muscles are active in producing and controlling movement at a particular joint.
One of the most fundamental and important goals of movement analysis is identifying which specific muscles are active in producing and controlling movement at a particular joint. In chapter 4, we presented specific muscles and their concentric actions. However, we know that muscles can act in three modes: isometric, concentric, and eccentric. The task at hand, therefore, is to determine for a given joint movement (1) the specific muscles involved in controlling the movement and (2) the type of muscle action.
The following muscle control formula provides a step-by-step procedure for determining the involved muscles and their action for any joint movement. This formula may appear a bit cumbersome and complex at first glance. However, with practice, you should be able to get through it quickly. Eventually (with enough practice), the process will become automatic and instinctive, and you will be able to analyze movements without consciously going through each step in the formula. It helps, though, to use the formula until you develop these movement analysis instincts.
Muscle Control Formula
We begin the muscle control formula with a statement of the problem: Given a specific joint movement (or position), identify the name of the movement (or position), the plane of movement, the effect of the external force acting on the system, the type of muscle action (i.e., shortening or concentric, lengthening or eccentric, or isometric), and the muscles involved (i.e., which muscle or muscles are actively involved in producing or controlling the movement or in maintaining a position).
Now, we move on to the formula itself, which involves six steps:
- Step 1: Identify the joint movement (e.g., flexion, abduction) or position.
- Step 2: Identify the effect of the external force (e.g., gravity) on the joint movement or position by asking the following question: What movement would the external force produce in the absence of muscle action (i.e., if there were no active muscles)?
- Step 3: Identify the type of muscle action (concentric, eccentric, isometric) based on the answers to step 1 (#1) and step 2 (#2) as follows:
- If #1 and #2 are in opposite directions, then the muscles are actively shortening in a concentric action. Speed of movement is not a factor.
- If #1 and #2 are in the same direction, then ask yourself, "What is the speed of movement?"
- If the movement is faster than what the external force would produce by itself, then the muscles are actively shortening in a concentric action.
- If the movement is slower than what the external force would produce by itself, then the muscles are actively lengthening in an eccentric action.
- If no movement is occurring, yet the external force would produce movement if acting by itself, then the muscles are performing an isometric action.
- Movements across gravity (i.e., parallel to the ground) are produced by a concentric action. When gravity cannot influence the joint movement in question, shortening (concentric) action is needed to pull the bone against its own inertia. The speed of movement is not a factor.
By this point, we have identified the type of muscle action. The next steps identify which muscles control the movement.
- Step 4: Identify the plane of movement (frontal, sagittal, transverse) and the axis of rotation (i.e., line about which the joint is rotating). The purpose of this step is to identify which side of the joint the muscles controlling the movement cross (e.g., flexors cross one side of a joint, while extensors cross the opposite side).
- Step 5:Ask yourself, "On which side of the joint axis are muscles lengthening and on which side are they shortening during the movement?"
- Step 6: Combine the information from steps 3 and 5 to determine which muscles must be producing or controlling the movement (or position). For example, if a concentric (shortening) action is required (from step 3) and the muscles on the anterior side of the joint are shortening (from step 5), then the anterior muscles must be actively producing the movement. The information in chapter 4 allows us to name the specific muscles.
Learn more about Dynamic Human Anatomy, Second Edition.
Ergonomic concepts
As an interdiscipline, ergonomics spans a variety of disciplines, including human anatomy, biomechanics, physiology, psychology, sociology, medicine, and engineering.
As an interdiscipline, ergonomics spans a variety of disciplines, including human anatomy, biomechanics, physiology, psychology, sociology, medicine, and engineering. Ergonomics is composed of three primary domains: organizational, cognitive, and physical. The organizational domain deals with organizational design, policies, and processes as they relate to workplace communication, work design and systems, networking, and teamwork. The cognitive domain involves mental processes, including perception, memory, reasoning, and motor response.
The physical domain is most relevant to our study of dynamic human anatomy. This domain integrates anthropometric, biomechanical, and physiological concepts as they relate to human movement, primarily in occupational settings. The principles of physical ergonomics have been used extensively in the design of consumer and industrial products, assessment of manual materials handling tasks, development of workplace safety guidelines, workplace design, and diagnosis of work-related medical conditions.
Goals
The primary goals of ergonomics are to improve productivity, improve efficiency, enhance safety, reduce injury risk, and reduce cost. Ergonomic interventions can improve both the quantity and quality of worker output and increase efficiency by facilitating production in a time-effective manner.
Safety enhancement and injury risk reduction are at the core of most ergonomic programs. One of the most common worker risks is a class of conditions collectively known as musculoskeletal disorders(MSDs). MSDs are the risk factor most closely associated with human movement tasks.
Research consistently has shown that ergonomic analysis and intervention can result in significant cost savings by reducing health care costs, lost work time, workers' compensation claims, and human error. Many ergonomic interventions are relatively inexpensive and are therefore cost effective for businesses, agencies, and workers alike.
Many governmental agencies and professional organizations have issued safety guidelines addressing specific ergonomic issues and recommendations. These guidelines cover a multitude of industrial and service areas, including agriculture, apparel and footwear, baggage handling, computer workstations, construction, health care, product manufacturing, metalwork foundries, meatpacking, mining, poultry processing, printing, sewing, shipyards, and telecommunications (U.S. Department of Labor, n.d.).
Methods of Analysis
Ergonomic analyses can be reactive or proactive. A reactive analysis addresses an existing problem or situation. A proactive analysis seeks to anticipate potential problems and make changes that prevent these problems.
An ergonomic analysis typically involves several steps, the first of which is identification of risk factors. General risk factors associated with movement-related ergonomic problems include awkward postures, repetitive motions, forceful exertions, pressure points, and sustained static postures(NIOSH, 2007).
In conducting an ergonomic assessment, the first step is to identify risk factors specific to the situation being assessed. Risk factors may be systematic (i.e., evident in the overall work environment) or specific to an individual. In assessing the work environment of a computer data-entry operator, for example, potential risk factors might include keyboard height and inclination, monitor height (relative to the operator's line of sight), distance, brightness, lack of arm and wrist support, chair design and support, and operator posture.
Once the ergonomic risk factors have been identified, the ergonomist must identify possible changes (e.g., new or adjusted keyboard, monitor, chair) to improve comfort and safety. After the changes have been implemented, the worker should be re-evaluated to ensure that the modifications have achieved the ergonomic goals.
Risk factors that are common to a group of workers can be addressed through either engineering or administrative controls. Engineering controls involve improving worker conditions by modifying tasks, adjusting movement patterns, redesigning workstations or tools, and providing protective equipment, as needed. Administrative controls include development and implementation of procedures and processes that can reduce risk such as job rotation (i.e., varying work tasks) and appropriate work breaks (e.g., rest or stretching breaks).
Numerous analysis approaches have been used to identify ergonomic problems and find solutions. Among those approaches are surveys and questionnaires, iterative prototyping, meta-analysis, work sampling, and a wide range of computer-based models applicable to specific tasks or systems.
Human - Machine Interface
Many occupations involve human interaction with a machine or device, in what is termed a human - machine interface. Examples include computer or keyboard operators (figure 13.1), assembly-line and construction workers, medical technicians and clinicians, and automobile mechanics.
Computer workstation anthropometrics for seated (left) and standing (right) operators.
Learn more about Dynamic Human Anatomy, Second Edition.
Components of muscle function
The control of even the simplest joint movement typically requires the cooperative action of several muscles working together as a single unit. This cooperative action is called muscle synergy.
The control of even the simplest joint movement typically requires the cooperative action of several muscles working together as a single unit. This cooperative action is called muscle synergy. Synergistic muscles work together, but other muscles with opposite functions may work against a particular movement. The overall, or net, effect of all muscles acting at a joint determines the ultimate mechanical effect, or movement.
Several concepts of muscle function are important for understanding how muscles cooperate and compete to control movement: agonists, neutralization, stabilization, antagonists, and coactivation.
- Agonists. Muscles that actively produce or control a single joint movement or maintain a single joint position are called agonists. In most movements, several muscles act together as agonists, with some playing a greater role than others.
- Neutralization. Muscles often perform more than one movement function at a given joint. At the ankle complex, for example, a muscle might act as both a plantar flexor and invertor (e.g., tibialis posterior). To produce pure plantar flexion, another muscle whose action produces plantar flexion and eversion (e.g., peroneus longus) would also need to be involved. The eversion action of the second muscle would cancel out, or neutralize, the inversion action of the first muscle. This process of canceling out an unwanted secondary movement is called neutralization.
- Stabilization. During concentric action, a muscle attempts to shorten by pulling its two bony attachment sites together. In most cases, the bone with the least resistance to movement (inertia) will move. When the inertia of both bones is similar in magnitude, both ends tend to move. If movement of only one end is desired, the other end must be prevented from moving, or stabilized. This stabilization is provided by other muscles or an external force. As an example, consider hip flexion created by the anterior thigh musculature. In attempting to move the femur in flexion, the hip flexors also tilt the pelvis anteriorly. If pelvic tilt is unwanted, then the abdominal musculature must act isometrically to stabilize the pelvis and prevent its movement.
- Antagonists. Muscles acting against a movement or position are called antagonists. To perform a movement most effectively, when the agonists actively shorten in concentric action, the corresponding antagonists passively lengthen. When agonists actively lengthen in eccentric action, the associated antagonists passively shorten. In many movements, then, the agonists and stabilizers are active while the antagonists are passive.
- Coactivation . Simultaneous action of both agonists and antagonists is called coactivation (also co-contraction). Coactivation might occur, for example, when an unskilled performer is unsure of the necessary muscle recruitment strategy. Skilled performers, however, do not exhibit an absence of coactivation. At least four possible explanations exist for coactivation in skilled performers: (1) less overall effort may be required in agonist - antagonist pairings for movements that involve changes of direction when the muscles maintain some level of activity, as opposed to working in an on - off manner; (2) coactivation increases joint stiffness and consequently joint stability, which may be desired for movements involving heavy loads; (3) coactivation of a single-joint muscle (e.g., gluteus maximus) and a two-joint muscle (e.g., rectus femoris) can increase the torque at a joint (e.g., knee) acted on by the two-joint muscle; and (4) given the neural complexities of the forearm and hand, fine movements of the fingers require complex coactivation strategies (Enoka, 2002).
Note that the term coactivation is limited to the concurrent action of agonists and antagonists and should not be used to describe the simultaneous action of multiple agonists. For instance, concurrent activity of the biceps brachii and triceps brachii during an elbow curl exercise would be considered coactivation. On the other hand, if the triceps was passive (i.e., inactive), simultaneous action of the three elbow flexors (biceps brachii, brachialis, brachioradialis) would not be considered coactivation.
With these concepts in mind, we now consider a simple yet fundamental question: How do we determine which muscles are active in producing or controlling a given movement?
Learn more about Dynamic Human Anatomy, Second Edition.
Determine the involved muscles and their action for any joint movement
One of the most fundamental and important goals of movement analysis is identifying which specific muscles are active in producing and controlling movement at a particular joint.
One of the most fundamental and important goals of movement analysis is identifying which specific muscles are active in producing and controlling movement at a particular joint. In chapter 4, we presented specific muscles and their concentric actions. However, we know that muscles can act in three modes: isometric, concentric, and eccentric. The task at hand, therefore, is to determine for a given joint movement (1) the specific muscles involved in controlling the movement and (2) the type of muscle action.
The following muscle control formula provides a step-by-step procedure for determining the involved muscles and their action for any joint movement. This formula may appear a bit cumbersome and complex at first glance. However, with practice, you should be able to get through it quickly. Eventually (with enough practice), the process will become automatic and instinctive, and you will be able to analyze movements without consciously going through each step in the formula. It helps, though, to use the formula until you develop these movement analysis instincts.
Muscle Control Formula
We begin the muscle control formula with a statement of the problem: Given a specific joint movement (or position), identify the name of the movement (or position), the plane of movement, the effect of the external force acting on the system, the type of muscle action (i.e., shortening or concentric, lengthening or eccentric, or isometric), and the muscles involved (i.e., which muscle or muscles are actively involved in producing or controlling the movement or in maintaining a position).
Now, we move on to the formula itself, which involves six steps:
- Step 1: Identify the joint movement (e.g., flexion, abduction) or position.
- Step 2: Identify the effect of the external force (e.g., gravity) on the joint movement or position by asking the following question: What movement would the external force produce in the absence of muscle action (i.e., if there were no active muscles)?
- Step 3: Identify the type of muscle action (concentric, eccentric, isometric) based on the answers to step 1 (#1) and step 2 (#2) as follows:
- If #1 and #2 are in opposite directions, then the muscles are actively shortening in a concentric action. Speed of movement is not a factor.
- If #1 and #2 are in the same direction, then ask yourself, "What is the speed of movement?"
- If the movement is faster than what the external force would produce by itself, then the muscles are actively shortening in a concentric action.
- If the movement is slower than what the external force would produce by itself, then the muscles are actively lengthening in an eccentric action.
- If no movement is occurring, yet the external force would produce movement if acting by itself, then the muscles are performing an isometric action.
- Movements across gravity (i.e., parallel to the ground) are produced by a concentric action. When gravity cannot influence the joint movement in question, shortening (concentric) action is needed to pull the bone against its own inertia. The speed of movement is not a factor.
By this point, we have identified the type of muscle action. The next steps identify which muscles control the movement.
- Step 4: Identify the plane of movement (frontal, sagittal, transverse) and the axis of rotation (i.e., line about which the joint is rotating). The purpose of this step is to identify which side of the joint the muscles controlling the movement cross (e.g., flexors cross one side of a joint, while extensors cross the opposite side).
- Step 5:Ask yourself, "On which side of the joint axis are muscles lengthening and on which side are they shortening during the movement?"
- Step 6: Combine the information from steps 3 and 5 to determine which muscles must be producing or controlling the movement (or position). For example, if a concentric (shortening) action is required (from step 3) and the muscles on the anterior side of the joint are shortening (from step 5), then the anterior muscles must be actively producing the movement. The information in chapter 4 allows us to name the specific muscles.
Learn more about Dynamic Human Anatomy, Second Edition.
Ergonomic concepts
As an interdiscipline, ergonomics spans a variety of disciplines, including human anatomy, biomechanics, physiology, psychology, sociology, medicine, and engineering.
As an interdiscipline, ergonomics spans a variety of disciplines, including human anatomy, biomechanics, physiology, psychology, sociology, medicine, and engineering. Ergonomics is composed of three primary domains: organizational, cognitive, and physical. The organizational domain deals with organizational design, policies, and processes as they relate to workplace communication, work design and systems, networking, and teamwork. The cognitive domain involves mental processes, including perception, memory, reasoning, and motor response.
The physical domain is most relevant to our study of dynamic human anatomy. This domain integrates anthropometric, biomechanical, and physiological concepts as they relate to human movement, primarily in occupational settings. The principles of physical ergonomics have been used extensively in the design of consumer and industrial products, assessment of manual materials handling tasks, development of workplace safety guidelines, workplace design, and diagnosis of work-related medical conditions.
Goals
The primary goals of ergonomics are to improve productivity, improve efficiency, enhance safety, reduce injury risk, and reduce cost. Ergonomic interventions can improve both the quantity and quality of worker output and increase efficiency by facilitating production in a time-effective manner.
Safety enhancement and injury risk reduction are at the core of most ergonomic programs. One of the most common worker risks is a class of conditions collectively known as musculoskeletal disorders(MSDs). MSDs are the risk factor most closely associated with human movement tasks.
Research consistently has shown that ergonomic analysis and intervention can result in significant cost savings by reducing health care costs, lost work time, workers' compensation claims, and human error. Many ergonomic interventions are relatively inexpensive and are therefore cost effective for businesses, agencies, and workers alike.
Many governmental agencies and professional organizations have issued safety guidelines addressing specific ergonomic issues and recommendations. These guidelines cover a multitude of industrial and service areas, including agriculture, apparel and footwear, baggage handling, computer workstations, construction, health care, product manufacturing, metalwork foundries, meatpacking, mining, poultry processing, printing, sewing, shipyards, and telecommunications (U.S. Department of Labor, n.d.).
Methods of Analysis
Ergonomic analyses can be reactive or proactive. A reactive analysis addresses an existing problem or situation. A proactive analysis seeks to anticipate potential problems and make changes that prevent these problems.
An ergonomic analysis typically involves several steps, the first of which is identification of risk factors. General risk factors associated with movement-related ergonomic problems include awkward postures, repetitive motions, forceful exertions, pressure points, and sustained static postures(NIOSH, 2007).
In conducting an ergonomic assessment, the first step is to identify risk factors specific to the situation being assessed. Risk factors may be systematic (i.e., evident in the overall work environment) or specific to an individual. In assessing the work environment of a computer data-entry operator, for example, potential risk factors might include keyboard height and inclination, monitor height (relative to the operator's line of sight), distance, brightness, lack of arm and wrist support, chair design and support, and operator posture.
Once the ergonomic risk factors have been identified, the ergonomist must identify possible changes (e.g., new or adjusted keyboard, monitor, chair) to improve comfort and safety. After the changes have been implemented, the worker should be re-evaluated to ensure that the modifications have achieved the ergonomic goals.
Risk factors that are common to a group of workers can be addressed through either engineering or administrative controls. Engineering controls involve improving worker conditions by modifying tasks, adjusting movement patterns, redesigning workstations or tools, and providing protective equipment, as needed. Administrative controls include development and implementation of procedures and processes that can reduce risk such as job rotation (i.e., varying work tasks) and appropriate work breaks (e.g., rest or stretching breaks).
Numerous analysis approaches have been used to identify ergonomic problems and find solutions. Among those approaches are surveys and questionnaires, iterative prototyping, meta-analysis, work sampling, and a wide range of computer-based models applicable to specific tasks or systems.
Human - Machine Interface
Many occupations involve human interaction with a machine or device, in what is termed a human - machine interface. Examples include computer or keyboard operators (figure 13.1), assembly-line and construction workers, medical technicians and clinicians, and automobile mechanics.
Computer workstation anthropometrics for seated (left) and standing (right) operators.
Learn more about Dynamic Human Anatomy, Second Edition.
Components of muscle function
The control of even the simplest joint movement typically requires the cooperative action of several muscles working together as a single unit. This cooperative action is called muscle synergy.
The control of even the simplest joint movement typically requires the cooperative action of several muscles working together as a single unit. This cooperative action is called muscle synergy. Synergistic muscles work together, but other muscles with opposite functions may work against a particular movement. The overall, or net, effect of all muscles acting at a joint determines the ultimate mechanical effect, or movement.
Several concepts of muscle function are important for understanding how muscles cooperate and compete to control movement: agonists, neutralization, stabilization, antagonists, and coactivation.
- Agonists. Muscles that actively produce or control a single joint movement or maintain a single joint position are called agonists. In most movements, several muscles act together as agonists, with some playing a greater role than others.
- Neutralization. Muscles often perform more than one movement function at a given joint. At the ankle complex, for example, a muscle might act as both a plantar flexor and invertor (e.g., tibialis posterior). To produce pure plantar flexion, another muscle whose action produces plantar flexion and eversion (e.g., peroneus longus) would also need to be involved. The eversion action of the second muscle would cancel out, or neutralize, the inversion action of the first muscle. This process of canceling out an unwanted secondary movement is called neutralization.
- Stabilization. During concentric action, a muscle attempts to shorten by pulling its two bony attachment sites together. In most cases, the bone with the least resistance to movement (inertia) will move. When the inertia of both bones is similar in magnitude, both ends tend to move. If movement of only one end is desired, the other end must be prevented from moving, or stabilized. This stabilization is provided by other muscles or an external force. As an example, consider hip flexion created by the anterior thigh musculature. In attempting to move the femur in flexion, the hip flexors also tilt the pelvis anteriorly. If pelvic tilt is unwanted, then the abdominal musculature must act isometrically to stabilize the pelvis and prevent its movement.
- Antagonists. Muscles acting against a movement or position are called antagonists. To perform a movement most effectively, when the agonists actively shorten in concentric action, the corresponding antagonists passively lengthen. When agonists actively lengthen in eccentric action, the associated antagonists passively shorten. In many movements, then, the agonists and stabilizers are active while the antagonists are passive.
- Coactivation . Simultaneous action of both agonists and antagonists is called coactivation (also co-contraction). Coactivation might occur, for example, when an unskilled performer is unsure of the necessary muscle recruitment strategy. Skilled performers, however, do not exhibit an absence of coactivation. At least four possible explanations exist for coactivation in skilled performers: (1) less overall effort may be required in agonist - antagonist pairings for movements that involve changes of direction when the muscles maintain some level of activity, as opposed to working in an on - off manner; (2) coactivation increases joint stiffness and consequently joint stability, which may be desired for movements involving heavy loads; (3) coactivation of a single-joint muscle (e.g., gluteus maximus) and a two-joint muscle (e.g., rectus femoris) can increase the torque at a joint (e.g., knee) acted on by the two-joint muscle; and (4) given the neural complexities of the forearm and hand, fine movements of the fingers require complex coactivation strategies (Enoka, 2002).
Note that the term coactivation is limited to the concurrent action of agonists and antagonists and should not be used to describe the simultaneous action of multiple agonists. For instance, concurrent activity of the biceps brachii and triceps brachii during an elbow curl exercise would be considered coactivation. On the other hand, if the triceps was passive (i.e., inactive), simultaneous action of the three elbow flexors (biceps brachii, brachialis, brachioradialis) would not be considered coactivation.
With these concepts in mind, we now consider a simple yet fundamental question: How do we determine which muscles are active in producing or controlling a given movement?
Learn more about Dynamic Human Anatomy, Second Edition.
Determine the involved muscles and their action for any joint movement
One of the most fundamental and important goals of movement analysis is identifying which specific muscles are active in producing and controlling movement at a particular joint.
One of the most fundamental and important goals of movement analysis is identifying which specific muscles are active in producing and controlling movement at a particular joint. In chapter 4, we presented specific muscles and their concentric actions. However, we know that muscles can act in three modes: isometric, concentric, and eccentric. The task at hand, therefore, is to determine for a given joint movement (1) the specific muscles involved in controlling the movement and (2) the type of muscle action.
The following muscle control formula provides a step-by-step procedure for determining the involved muscles and their action for any joint movement. This formula may appear a bit cumbersome and complex at first glance. However, with practice, you should be able to get through it quickly. Eventually (with enough practice), the process will become automatic and instinctive, and you will be able to analyze movements without consciously going through each step in the formula. It helps, though, to use the formula until you develop these movement analysis instincts.
Muscle Control Formula
We begin the muscle control formula with a statement of the problem: Given a specific joint movement (or position), identify the name of the movement (or position), the plane of movement, the effect of the external force acting on the system, the type of muscle action (i.e., shortening or concentric, lengthening or eccentric, or isometric), and the muscles involved (i.e., which muscle or muscles are actively involved in producing or controlling the movement or in maintaining a position).
Now, we move on to the formula itself, which involves six steps:
- Step 1: Identify the joint movement (e.g., flexion, abduction) or position.
- Step 2: Identify the effect of the external force (e.g., gravity) on the joint movement or position by asking the following question: What movement would the external force produce in the absence of muscle action (i.e., if there were no active muscles)?
- Step 3: Identify the type of muscle action (concentric, eccentric, isometric) based on the answers to step 1 (#1) and step 2 (#2) as follows:
- If #1 and #2 are in opposite directions, then the muscles are actively shortening in a concentric action. Speed of movement is not a factor.
- If #1 and #2 are in the same direction, then ask yourself, "What is the speed of movement?"
- If the movement is faster than what the external force would produce by itself, then the muscles are actively shortening in a concentric action.
- If the movement is slower than what the external force would produce by itself, then the muscles are actively lengthening in an eccentric action.
- If no movement is occurring, yet the external force would produce movement if acting by itself, then the muscles are performing an isometric action.
- Movements across gravity (i.e., parallel to the ground) are produced by a concentric action. When gravity cannot influence the joint movement in question, shortening (concentric) action is needed to pull the bone against its own inertia. The speed of movement is not a factor.
By this point, we have identified the type of muscle action. The next steps identify which muscles control the movement.
- Step 4: Identify the plane of movement (frontal, sagittal, transverse) and the axis of rotation (i.e., line about which the joint is rotating). The purpose of this step is to identify which side of the joint the muscles controlling the movement cross (e.g., flexors cross one side of a joint, while extensors cross the opposite side).
- Step 5:Ask yourself, "On which side of the joint axis are muscles lengthening and on which side are they shortening during the movement?"
- Step 6: Combine the information from steps 3 and 5 to determine which muscles must be producing or controlling the movement (or position). For example, if a concentric (shortening) action is required (from step 3) and the muscles on the anterior side of the joint are shortening (from step 5), then the anterior muscles must be actively producing the movement. The information in chapter 4 allows us to name the specific muscles.
Learn more about Dynamic Human Anatomy, Second Edition.
Ergonomic concepts
As an interdiscipline, ergonomics spans a variety of disciplines, including human anatomy, biomechanics, physiology, psychology, sociology, medicine, and engineering.
As an interdiscipline, ergonomics spans a variety of disciplines, including human anatomy, biomechanics, physiology, psychology, sociology, medicine, and engineering. Ergonomics is composed of three primary domains: organizational, cognitive, and physical. The organizational domain deals with organizational design, policies, and processes as they relate to workplace communication, work design and systems, networking, and teamwork. The cognitive domain involves mental processes, including perception, memory, reasoning, and motor response.
The physical domain is most relevant to our study of dynamic human anatomy. This domain integrates anthropometric, biomechanical, and physiological concepts as they relate to human movement, primarily in occupational settings. The principles of physical ergonomics have been used extensively in the design of consumer and industrial products, assessment of manual materials handling tasks, development of workplace safety guidelines, workplace design, and diagnosis of work-related medical conditions.
Goals
The primary goals of ergonomics are to improve productivity, improve efficiency, enhance safety, reduce injury risk, and reduce cost. Ergonomic interventions can improve both the quantity and quality of worker output and increase efficiency by facilitating production in a time-effective manner.
Safety enhancement and injury risk reduction are at the core of most ergonomic programs. One of the most common worker risks is a class of conditions collectively known as musculoskeletal disorders(MSDs). MSDs are the risk factor most closely associated with human movement tasks.
Research consistently has shown that ergonomic analysis and intervention can result in significant cost savings by reducing health care costs, lost work time, workers' compensation claims, and human error. Many ergonomic interventions are relatively inexpensive and are therefore cost effective for businesses, agencies, and workers alike.
Many governmental agencies and professional organizations have issued safety guidelines addressing specific ergonomic issues and recommendations. These guidelines cover a multitude of industrial and service areas, including agriculture, apparel and footwear, baggage handling, computer workstations, construction, health care, product manufacturing, metalwork foundries, meatpacking, mining, poultry processing, printing, sewing, shipyards, and telecommunications (U.S. Department of Labor, n.d.).
Methods of Analysis
Ergonomic analyses can be reactive or proactive. A reactive analysis addresses an existing problem or situation. A proactive analysis seeks to anticipate potential problems and make changes that prevent these problems.
An ergonomic analysis typically involves several steps, the first of which is identification of risk factors. General risk factors associated with movement-related ergonomic problems include awkward postures, repetitive motions, forceful exertions, pressure points, and sustained static postures(NIOSH, 2007).
In conducting an ergonomic assessment, the first step is to identify risk factors specific to the situation being assessed. Risk factors may be systematic (i.e., evident in the overall work environment) or specific to an individual. In assessing the work environment of a computer data-entry operator, for example, potential risk factors might include keyboard height and inclination, monitor height (relative to the operator's line of sight), distance, brightness, lack of arm and wrist support, chair design and support, and operator posture.
Once the ergonomic risk factors have been identified, the ergonomist must identify possible changes (e.g., new or adjusted keyboard, monitor, chair) to improve comfort and safety. After the changes have been implemented, the worker should be re-evaluated to ensure that the modifications have achieved the ergonomic goals.
Risk factors that are common to a group of workers can be addressed through either engineering or administrative controls. Engineering controls involve improving worker conditions by modifying tasks, adjusting movement patterns, redesigning workstations or tools, and providing protective equipment, as needed. Administrative controls include development and implementation of procedures and processes that can reduce risk such as job rotation (i.e., varying work tasks) and appropriate work breaks (e.g., rest or stretching breaks).
Numerous analysis approaches have been used to identify ergonomic problems and find solutions. Among those approaches are surveys and questionnaires, iterative prototyping, meta-analysis, work sampling, and a wide range of computer-based models applicable to specific tasks or systems.
Human - Machine Interface
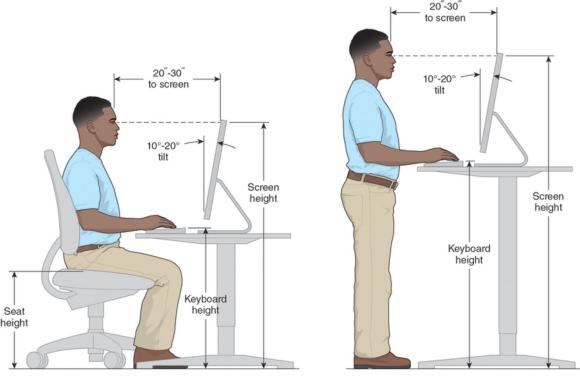
Many occupations involve human interaction with a machine or device, in what is termed a human - machine interface. Examples include computer or keyboard operators (figure 13.1), assembly-line and construction workers, medical technicians and clinicians, and automobile mechanics.
Computer workstation anthropometrics for seated (left) and standing (right) operators.
Learn more about Dynamic Human Anatomy, Second Edition.
Components of muscle function
The control of even the simplest joint movement typically requires the cooperative action of several muscles working together as a single unit. This cooperative action is called muscle synergy.
The control of even the simplest joint movement typically requires the cooperative action of several muscles working together as a single unit. This cooperative action is called muscle synergy. Synergistic muscles work together, but other muscles with opposite functions may work against a particular movement. The overall, or net, effect of all muscles acting at a joint determines the ultimate mechanical effect, or movement.
Several concepts of muscle function are important for understanding how muscles cooperate and compete to control movement: agonists, neutralization, stabilization, antagonists, and coactivation.
- Agonists. Muscles that actively produce or control a single joint movement or maintain a single joint position are called agonists. In most movements, several muscles act together as agonists, with some playing a greater role than others.
- Neutralization. Muscles often perform more than one movement function at a given joint. At the ankle complex, for example, a muscle might act as both a plantar flexor and invertor (e.g., tibialis posterior). To produce pure plantar flexion, another muscle whose action produces plantar flexion and eversion (e.g., peroneus longus) would also need to be involved. The eversion action of the second muscle would cancel out, or neutralize, the inversion action of the first muscle. This process of canceling out an unwanted secondary movement is called neutralization.
- Stabilization. During concentric action, a muscle attempts to shorten by pulling its two bony attachment sites together. In most cases, the bone with the least resistance to movement (inertia) will move. When the inertia of both bones is similar in magnitude, both ends tend to move. If movement of only one end is desired, the other end must be prevented from moving, or stabilized. This stabilization is provided by other muscles or an external force. As an example, consider hip flexion created by the anterior thigh musculature. In attempting to move the femur in flexion, the hip flexors also tilt the pelvis anteriorly. If pelvic tilt is unwanted, then the abdominal musculature must act isometrically to stabilize the pelvis and prevent its movement.
- Antagonists. Muscles acting against a movement or position are called antagonists. To perform a movement most effectively, when the agonists actively shorten in concentric action, the corresponding antagonists passively lengthen. When agonists actively lengthen in eccentric action, the associated antagonists passively shorten. In many movements, then, the agonists and stabilizers are active while the antagonists are passive.
- Coactivation . Simultaneous action of both agonists and antagonists is called coactivation (also co-contraction). Coactivation might occur, for example, when an unskilled performer is unsure of the necessary muscle recruitment strategy. Skilled performers, however, do not exhibit an absence of coactivation. At least four possible explanations exist for coactivation in skilled performers: (1) less overall effort may be required in agonist - antagonist pairings for movements that involve changes of direction when the muscles maintain some level of activity, as opposed to working in an on - off manner; (2) coactivation increases joint stiffness and consequently joint stability, which may be desired for movements involving heavy loads; (3) coactivation of a single-joint muscle (e.g., gluteus maximus) and a two-joint muscle (e.g., rectus femoris) can increase the torque at a joint (e.g., knee) acted on by the two-joint muscle; and (4) given the neural complexities of the forearm and hand, fine movements of the fingers require complex coactivation strategies (Enoka, 2002).
Note that the term coactivation is limited to the concurrent action of agonists and antagonists and should not be used to describe the simultaneous action of multiple agonists. For instance, concurrent activity of the biceps brachii and triceps brachii during an elbow curl exercise would be considered coactivation. On the other hand, if the triceps was passive (i.e., inactive), simultaneous action of the three elbow flexors (biceps brachii, brachialis, brachioradialis) would not be considered coactivation.
With these concepts in mind, we now consider a simple yet fundamental question: How do we determine which muscles are active in producing or controlling a given movement?
Learn more about Dynamic Human Anatomy, Second Edition.
Determine the involved muscles and their action for any joint movement
One of the most fundamental and important goals of movement analysis is identifying which specific muscles are active in producing and controlling movement at a particular joint.
One of the most fundamental and important goals of movement analysis is identifying which specific muscles are active in producing and controlling movement at a particular joint. In chapter 4, we presented specific muscles and their concentric actions. However, we know that muscles can act in three modes: isometric, concentric, and eccentric. The task at hand, therefore, is to determine for a given joint movement (1) the specific muscles involved in controlling the movement and (2) the type of muscle action.
The following muscle control formula provides a step-by-step procedure for determining the involved muscles and their action for any joint movement. This formula may appear a bit cumbersome and complex at first glance. However, with practice, you should be able to get through it quickly. Eventually (with enough practice), the process will become automatic and instinctive, and you will be able to analyze movements without consciously going through each step in the formula. It helps, though, to use the formula until you develop these movement analysis instincts.
Muscle Control Formula
We begin the muscle control formula with a statement of the problem: Given a specific joint movement (or position), identify the name of the movement (or position), the plane of movement, the effect of the external force acting on the system, the type of muscle action (i.e., shortening or concentric, lengthening or eccentric, or isometric), and the muscles involved (i.e., which muscle or muscles are actively involved in producing or controlling the movement or in maintaining a position).
Now, we move on to the formula itself, which involves six steps:
- Step 1: Identify the joint movement (e.g., flexion, abduction) or position.
- Step 2: Identify the effect of the external force (e.g., gravity) on the joint movement or position by asking the following question: What movement would the external force produce in the absence of muscle action (i.e., if there were no active muscles)?
- Step 3: Identify the type of muscle action (concentric, eccentric, isometric) based on the answers to step 1 (#1) and step 2 (#2) as follows:
- If #1 and #2 are in opposite directions, then the muscles are actively shortening in a concentric action. Speed of movement is not a factor.
- If #1 and #2 are in the same direction, then ask yourself, "What is the speed of movement?"
- If the movement is faster than what the external force would produce by itself, then the muscles are actively shortening in a concentric action.
- If the movement is slower than what the external force would produce by itself, then the muscles are actively lengthening in an eccentric action.
- If no movement is occurring, yet the external force would produce movement if acting by itself, then the muscles are performing an isometric action.
- Movements across gravity (i.e., parallel to the ground) are produced by a concentric action. When gravity cannot influence the joint movement in question, shortening (concentric) action is needed to pull the bone against its own inertia. The speed of movement is not a factor.
By this point, we have identified the type of muscle action. The next steps identify which muscles control the movement.
- Step 4: Identify the plane of movement (frontal, sagittal, transverse) and the axis of rotation (i.e., line about which the joint is rotating). The purpose of this step is to identify which side of the joint the muscles controlling the movement cross (e.g., flexors cross one side of a joint, while extensors cross the opposite side).
- Step 5:Ask yourself, "On which side of the joint axis are muscles lengthening and on which side are they shortening during the movement?"
- Step 6: Combine the information from steps 3 and 5 to determine which muscles must be producing or controlling the movement (or position). For example, if a concentric (shortening) action is required (from step 3) and the muscles on the anterior side of the joint are shortening (from step 5), then the anterior muscles must be actively producing the movement. The information in chapter 4 allows us to name the specific muscles.
Learn more about Dynamic Human Anatomy, Second Edition.
Ergonomic concepts
As an interdiscipline, ergonomics spans a variety of disciplines, including human anatomy, biomechanics, physiology, psychology, sociology, medicine, and engineering.
As an interdiscipline, ergonomics spans a variety of disciplines, including human anatomy, biomechanics, physiology, psychology, sociology, medicine, and engineering. Ergonomics is composed of three primary domains: organizational, cognitive, and physical. The organizational domain deals with organizational design, policies, and processes as they relate to workplace communication, work design and systems, networking, and teamwork. The cognitive domain involves mental processes, including perception, memory, reasoning, and motor response.
The physical domain is most relevant to our study of dynamic human anatomy. This domain integrates anthropometric, biomechanical, and physiological concepts as they relate to human movement, primarily in occupational settings. The principles of physical ergonomics have been used extensively in the design of consumer and industrial products, assessment of manual materials handling tasks, development of workplace safety guidelines, workplace design, and diagnosis of work-related medical conditions.
Goals
The primary goals of ergonomics are to improve productivity, improve efficiency, enhance safety, reduce injury risk, and reduce cost. Ergonomic interventions can improve both the quantity and quality of worker output and increase efficiency by facilitating production in a time-effective manner.
Safety enhancement and injury risk reduction are at the core of most ergonomic programs. One of the most common worker risks is a class of conditions collectively known as musculoskeletal disorders(MSDs). MSDs are the risk factor most closely associated with human movement tasks.
Research consistently has shown that ergonomic analysis and intervention can result in significant cost savings by reducing health care costs, lost work time, workers' compensation claims, and human error. Many ergonomic interventions are relatively inexpensive and are therefore cost effective for businesses, agencies, and workers alike.
Many governmental agencies and professional organizations have issued safety guidelines addressing specific ergonomic issues and recommendations. These guidelines cover a multitude of industrial and service areas, including agriculture, apparel and footwear, baggage handling, computer workstations, construction, health care, product manufacturing, metalwork foundries, meatpacking, mining, poultry processing, printing, sewing, shipyards, and telecommunications (U.S. Department of Labor, n.d.).
Methods of Analysis
Ergonomic analyses can be reactive or proactive. A reactive analysis addresses an existing problem or situation. A proactive analysis seeks to anticipate potential problems and make changes that prevent these problems.
An ergonomic analysis typically involves several steps, the first of which is identification of risk factors. General risk factors associated with movement-related ergonomic problems include awkward postures, repetitive motions, forceful exertions, pressure points, and sustained static postures(NIOSH, 2007).
In conducting an ergonomic assessment, the first step is to identify risk factors specific to the situation being assessed. Risk factors may be systematic (i.e., evident in the overall work environment) or specific to an individual. In assessing the work environment of a computer data-entry operator, for example, potential risk factors might include keyboard height and inclination, monitor height (relative to the operator's line of sight), distance, brightness, lack of arm and wrist support, chair design and support, and operator posture.
Once the ergonomic risk factors have been identified, the ergonomist must identify possible changes (e.g., new or adjusted keyboard, monitor, chair) to improve comfort and safety. After the changes have been implemented, the worker should be re-evaluated to ensure that the modifications have achieved the ergonomic goals.
Risk factors that are common to a group of workers can be addressed through either engineering or administrative controls. Engineering controls involve improving worker conditions by modifying tasks, adjusting movement patterns, redesigning workstations or tools, and providing protective equipment, as needed. Administrative controls include development and implementation of procedures and processes that can reduce risk such as job rotation (i.e., varying work tasks) and appropriate work breaks (e.g., rest or stretching breaks).
Numerous analysis approaches have been used to identify ergonomic problems and find solutions. Among those approaches are surveys and questionnaires, iterative prototyping, meta-analysis, work sampling, and a wide range of computer-based models applicable to specific tasks or systems.
Human - Machine Interface
Many occupations involve human interaction with a machine or device, in what is termed a human - machine interface. Examples include computer or keyboard operators (figure 13.1), assembly-line and construction workers, medical technicians and clinicians, and automobile mechanics.
Computer workstation anthropometrics for seated (left) and standing (right) operators.
Learn more about Dynamic Human Anatomy, Second Edition.
Components of muscle function
The control of even the simplest joint movement typically requires the cooperative action of several muscles working together as a single unit. This cooperative action is called muscle synergy.
The control of even the simplest joint movement typically requires the cooperative action of several muscles working together as a single unit. This cooperative action is called muscle synergy. Synergistic muscles work together, but other muscles with opposite functions may work against a particular movement. The overall, or net, effect of all muscles acting at a joint determines the ultimate mechanical effect, or movement.
Several concepts of muscle function are important for understanding how muscles cooperate and compete to control movement: agonists, neutralization, stabilization, antagonists, and coactivation.
- Agonists. Muscles that actively produce or control a single joint movement or maintain a single joint position are called agonists. In most movements, several muscles act together as agonists, with some playing a greater role than others.
- Neutralization. Muscles often perform more than one movement function at a given joint. At the ankle complex, for example, a muscle might act as both a plantar flexor and invertor (e.g., tibialis posterior). To produce pure plantar flexion, another muscle whose action produces plantar flexion and eversion (e.g., peroneus longus) would also need to be involved. The eversion action of the second muscle would cancel out, or neutralize, the inversion action of the first muscle. This process of canceling out an unwanted secondary movement is called neutralization.
- Stabilization. During concentric action, a muscle attempts to shorten by pulling its two bony attachment sites together. In most cases, the bone with the least resistance to movement (inertia) will move. When the inertia of both bones is similar in magnitude, both ends tend to move. If movement of only one end is desired, the other end must be prevented from moving, or stabilized. This stabilization is provided by other muscles or an external force. As an example, consider hip flexion created by the anterior thigh musculature. In attempting to move the femur in flexion, the hip flexors also tilt the pelvis anteriorly. If pelvic tilt is unwanted, then the abdominal musculature must act isometrically to stabilize the pelvis and prevent its movement.
- Antagonists. Muscles acting against a movement or position are called antagonists. To perform a movement most effectively, when the agonists actively shorten in concentric action, the corresponding antagonists passively lengthen. When agonists actively lengthen in eccentric action, the associated antagonists passively shorten. In many movements, then, the agonists and stabilizers are active while the antagonists are passive.
- Coactivation . Simultaneous action of both agonists and antagonists is called coactivation (also co-contraction). Coactivation might occur, for example, when an unskilled performer is unsure of the necessary muscle recruitment strategy. Skilled performers, however, do not exhibit an absence of coactivation. At least four possible explanations exist for coactivation in skilled performers: (1) less overall effort may be required in agonist - antagonist pairings for movements that involve changes of direction when the muscles maintain some level of activity, as opposed to working in an on - off manner; (2) coactivation increases joint stiffness and consequently joint stability, which may be desired for movements involving heavy loads; (3) coactivation of a single-joint muscle (e.g., gluteus maximus) and a two-joint muscle (e.g., rectus femoris) can increase the torque at a joint (e.g., knee) acted on by the two-joint muscle; and (4) given the neural complexities of the forearm and hand, fine movements of the fingers require complex coactivation strategies (Enoka, 2002).
Note that the term coactivation is limited to the concurrent action of agonists and antagonists and should not be used to describe the simultaneous action of multiple agonists. For instance, concurrent activity of the biceps brachii and triceps brachii during an elbow curl exercise would be considered coactivation. On the other hand, if the triceps was passive (i.e., inactive), simultaneous action of the three elbow flexors (biceps brachii, brachialis, brachioradialis) would not be considered coactivation.
With these concepts in mind, we now consider a simple yet fundamental question: How do we determine which muscles are active in producing or controlling a given movement?
Learn more about Dynamic Human Anatomy, Second Edition.
Determine the involved muscles and their action for any joint movement
One of the most fundamental and important goals of movement analysis is identifying which specific muscles are active in producing and controlling movement at a particular joint.
One of the most fundamental and important goals of movement analysis is identifying which specific muscles are active in producing and controlling movement at a particular joint. In chapter 4, we presented specific muscles and their concentric actions. However, we know that muscles can act in three modes: isometric, concentric, and eccentric. The task at hand, therefore, is to determine for a given joint movement (1) the specific muscles involved in controlling the movement and (2) the type of muscle action.
The following muscle control formula provides a step-by-step procedure for determining the involved muscles and their action for any joint movement. This formula may appear a bit cumbersome and complex at first glance. However, with practice, you should be able to get through it quickly. Eventually (with enough practice), the process will become automatic and instinctive, and you will be able to analyze movements without consciously going through each step in the formula. It helps, though, to use the formula until you develop these movement analysis instincts.
Muscle Control Formula
We begin the muscle control formula with a statement of the problem: Given a specific joint movement (or position), identify the name of the movement (or position), the plane of movement, the effect of the external force acting on the system, the type of muscle action (i.e., shortening or concentric, lengthening or eccentric, or isometric), and the muscles involved (i.e., which muscle or muscles are actively involved in producing or controlling the movement or in maintaining a position).
Now, we move on to the formula itself, which involves six steps:
- Step 1: Identify the joint movement (e.g., flexion, abduction) or position.
- Step 2: Identify the effect of the external force (e.g., gravity) on the joint movement or position by asking the following question: What movement would the external force produce in the absence of muscle action (i.e., if there were no active muscles)?
- Step 3: Identify the type of muscle action (concentric, eccentric, isometric) based on the answers to step 1 (#1) and step 2 (#2) as follows:
- If #1 and #2 are in opposite directions, then the muscles are actively shortening in a concentric action. Speed of movement is not a factor.
- If #1 and #2 are in the same direction, then ask yourself, "What is the speed of movement?"
- If the movement is faster than what the external force would produce by itself, then the muscles are actively shortening in a concentric action.
- If the movement is slower than what the external force would produce by itself, then the muscles are actively lengthening in an eccentric action.
- If no movement is occurring, yet the external force would produce movement if acting by itself, then the muscles are performing an isometric action.
- Movements across gravity (i.e., parallel to the ground) are produced by a concentric action. When gravity cannot influence the joint movement in question, shortening (concentric) action is needed to pull the bone against its own inertia. The speed of movement is not a factor.
By this point, we have identified the type of muscle action. The next steps identify which muscles control the movement.
- Step 4: Identify the plane of movement (frontal, sagittal, transverse) and the axis of rotation (i.e., line about which the joint is rotating). The purpose of this step is to identify which side of the joint the muscles controlling the movement cross (e.g., flexors cross one side of a joint, while extensors cross the opposite side).
- Step 5:Ask yourself, "On which side of the joint axis are muscles lengthening and on which side are they shortening during the movement?"
- Step 6: Combine the information from steps 3 and 5 to determine which muscles must be producing or controlling the movement (or position). For example, if a concentric (shortening) action is required (from step 3) and the muscles on the anterior side of the joint are shortening (from step 5), then the anterior muscles must be actively producing the movement. The information in chapter 4 allows us to name the specific muscles.
Learn more about Dynamic Human Anatomy, Second Edition.
Ergonomic concepts
As an interdiscipline, ergonomics spans a variety of disciplines, including human anatomy, biomechanics, physiology, psychology, sociology, medicine, and engineering.
As an interdiscipline, ergonomics spans a variety of disciplines, including human anatomy, biomechanics, physiology, psychology, sociology, medicine, and engineering. Ergonomics is composed of three primary domains: organizational, cognitive, and physical. The organizational domain deals with organizational design, policies, and processes as they relate to workplace communication, work design and systems, networking, and teamwork. The cognitive domain involves mental processes, including perception, memory, reasoning, and motor response.
The physical domain is most relevant to our study of dynamic human anatomy. This domain integrates anthropometric, biomechanical, and physiological concepts as they relate to human movement, primarily in occupational settings. The principles of physical ergonomics have been used extensively in the design of consumer and industrial products, assessment of manual materials handling tasks, development of workplace safety guidelines, workplace design, and diagnosis of work-related medical conditions.
Goals
The primary goals of ergonomics are to improve productivity, improve efficiency, enhance safety, reduce injury risk, and reduce cost. Ergonomic interventions can improve both the quantity and quality of worker output and increase efficiency by facilitating production in a time-effective manner.
Safety enhancement and injury risk reduction are at the core of most ergonomic programs. One of the most common worker risks is a class of conditions collectively known as musculoskeletal disorders(MSDs). MSDs are the risk factor most closely associated with human movement tasks.
Research consistently has shown that ergonomic analysis and intervention can result in significant cost savings by reducing health care costs, lost work time, workers' compensation claims, and human error. Many ergonomic interventions are relatively inexpensive and are therefore cost effective for businesses, agencies, and workers alike.
Many governmental agencies and professional organizations have issued safety guidelines addressing specific ergonomic issues and recommendations. These guidelines cover a multitude of industrial and service areas, including agriculture, apparel and footwear, baggage handling, computer workstations, construction, health care, product manufacturing, metalwork foundries, meatpacking, mining, poultry processing, printing, sewing, shipyards, and telecommunications (U.S. Department of Labor, n.d.).
Methods of Analysis
Ergonomic analyses can be reactive or proactive. A reactive analysis addresses an existing problem or situation. A proactive analysis seeks to anticipate potential problems and make changes that prevent these problems.
An ergonomic analysis typically involves several steps, the first of which is identification of risk factors. General risk factors associated with movement-related ergonomic problems include awkward postures, repetitive motions, forceful exertions, pressure points, and sustained static postures(NIOSH, 2007).
In conducting an ergonomic assessment, the first step is to identify risk factors specific to the situation being assessed. Risk factors may be systematic (i.e., evident in the overall work environment) or specific to an individual. In assessing the work environment of a computer data-entry operator, for example, potential risk factors might include keyboard height and inclination, monitor height (relative to the operator's line of sight), distance, brightness, lack of arm and wrist support, chair design and support, and operator posture.
Once the ergonomic risk factors have been identified, the ergonomist must identify possible changes (e.g., new or adjusted keyboard, monitor, chair) to improve comfort and safety. After the changes have been implemented, the worker should be re-evaluated to ensure that the modifications have achieved the ergonomic goals.
Risk factors that are common to a group of workers can be addressed through either engineering or administrative controls. Engineering controls involve improving worker conditions by modifying tasks, adjusting movement patterns, redesigning workstations or tools, and providing protective equipment, as needed. Administrative controls include development and implementation of procedures and processes that can reduce risk such as job rotation (i.e., varying work tasks) and appropriate work breaks (e.g., rest or stretching breaks).
Numerous analysis approaches have been used to identify ergonomic problems and find solutions. Among those approaches are surveys and questionnaires, iterative prototyping, meta-analysis, work sampling, and a wide range of computer-based models applicable to specific tasks or systems.
Human - Machine Interface
Many occupations involve human interaction with a machine or device, in what is termed a human - machine interface. Examples include computer or keyboard operators (figure 13.1), assembly-line and construction workers, medical technicians and clinicians, and automobile mechanics.
Computer workstation anthropometrics for seated (left) and standing (right) operators.
Learn more about Dynamic Human Anatomy, Second Edition.
Components of muscle function
The control of even the simplest joint movement typically requires the cooperative action of several muscles working together as a single unit. This cooperative action is called muscle synergy.
The control of even the simplest joint movement typically requires the cooperative action of several muscles working together as a single unit. This cooperative action is called muscle synergy. Synergistic muscles work together, but other muscles with opposite functions may work against a particular movement. The overall, or net, effect of all muscles acting at a joint determines the ultimate mechanical effect, or movement.
Several concepts of muscle function are important for understanding how muscles cooperate and compete to control movement: agonists, neutralization, stabilization, antagonists, and coactivation.
- Agonists. Muscles that actively produce or control a single joint movement or maintain a single joint position are called agonists. In most movements, several muscles act together as agonists, with some playing a greater role than others.
- Neutralization. Muscles often perform more than one movement function at a given joint. At the ankle complex, for example, a muscle might act as both a plantar flexor and invertor (e.g., tibialis posterior). To produce pure plantar flexion, another muscle whose action produces plantar flexion and eversion (e.g., peroneus longus) would also need to be involved. The eversion action of the second muscle would cancel out, or neutralize, the inversion action of the first muscle. This process of canceling out an unwanted secondary movement is called neutralization.
- Stabilization. During concentric action, a muscle attempts to shorten by pulling its two bony attachment sites together. In most cases, the bone with the least resistance to movement (inertia) will move. When the inertia of both bones is similar in magnitude, both ends tend to move. If movement of only one end is desired, the other end must be prevented from moving, or stabilized. This stabilization is provided by other muscles or an external force. As an example, consider hip flexion created by the anterior thigh musculature. In attempting to move the femur in flexion, the hip flexors also tilt the pelvis anteriorly. If pelvic tilt is unwanted, then the abdominal musculature must act isometrically to stabilize the pelvis and prevent its movement.
- Antagonists. Muscles acting against a movement or position are called antagonists. To perform a movement most effectively, when the agonists actively shorten in concentric action, the corresponding antagonists passively lengthen. When agonists actively lengthen in eccentric action, the associated antagonists passively shorten. In many movements, then, the agonists and stabilizers are active while the antagonists are passive.
- Coactivation . Simultaneous action of both agonists and antagonists is called coactivation (also co-contraction). Coactivation might occur, for example, when an unskilled performer is unsure of the necessary muscle recruitment strategy. Skilled performers, however, do not exhibit an absence of coactivation. At least four possible explanations exist for coactivation in skilled performers: (1) less overall effort may be required in agonist - antagonist pairings for movements that involve changes of direction when the muscles maintain some level of activity, as opposed to working in an on - off manner; (2) coactivation increases joint stiffness and consequently joint stability, which may be desired for movements involving heavy loads; (3) coactivation of a single-joint muscle (e.g., gluteus maximus) and a two-joint muscle (e.g., rectus femoris) can increase the torque at a joint (e.g., knee) acted on by the two-joint muscle; and (4) given the neural complexities of the forearm and hand, fine movements of the fingers require complex coactivation strategies (Enoka, 2002).
Note that the term coactivation is limited to the concurrent action of agonists and antagonists and should not be used to describe the simultaneous action of multiple agonists. For instance, concurrent activity of the biceps brachii and triceps brachii during an elbow curl exercise would be considered coactivation. On the other hand, if the triceps was passive (i.e., inactive), simultaneous action of the three elbow flexors (biceps brachii, brachialis, brachioradialis) would not be considered coactivation.
With these concepts in mind, we now consider a simple yet fundamental question: How do we determine which muscles are active in producing or controlling a given movement?
Learn more about Dynamic Human Anatomy, Second Edition.
Determine the involved muscles and their action for any joint movement
One of the most fundamental and important goals of movement analysis is identifying which specific muscles are active in producing and controlling movement at a particular joint.
One of the most fundamental and important goals of movement analysis is identifying which specific muscles are active in producing and controlling movement at a particular joint. In chapter 4, we presented specific muscles and their concentric actions. However, we know that muscles can act in three modes: isometric, concentric, and eccentric. The task at hand, therefore, is to determine for a given joint movement (1) the specific muscles involved in controlling the movement and (2) the type of muscle action.
The following muscle control formula provides a step-by-step procedure for determining the involved muscles and their action for any joint movement. This formula may appear a bit cumbersome and complex at first glance. However, with practice, you should be able to get through it quickly. Eventually (with enough practice), the process will become automatic and instinctive, and you will be able to analyze movements without consciously going through each step in the formula. It helps, though, to use the formula until you develop these movement analysis instincts.
Muscle Control Formula
We begin the muscle control formula with a statement of the problem: Given a specific joint movement (or position), identify the name of the movement (or position), the plane of movement, the effect of the external force acting on the system, the type of muscle action (i.e., shortening or concentric, lengthening or eccentric, or isometric), and the muscles involved (i.e., which muscle or muscles are actively involved in producing or controlling the movement or in maintaining a position).
Now, we move on to the formula itself, which involves six steps:
- Step 1: Identify the joint movement (e.g., flexion, abduction) or position.
- Step 2: Identify the effect of the external force (e.g., gravity) on the joint movement or position by asking the following question: What movement would the external force produce in the absence of muscle action (i.e., if there were no active muscles)?
- Step 3: Identify the type of muscle action (concentric, eccentric, isometric) based on the answers to step 1 (#1) and step 2 (#2) as follows:
- If #1 and #2 are in opposite directions, then the muscles are actively shortening in a concentric action. Speed of movement is not a factor.
- If #1 and #2 are in the same direction, then ask yourself, "What is the speed of movement?"
- If the movement is faster than what the external force would produce by itself, then the muscles are actively shortening in a concentric action.
- If the movement is slower than what the external force would produce by itself, then the muscles are actively lengthening in an eccentric action.
- If no movement is occurring, yet the external force would produce movement if acting by itself, then the muscles are performing an isometric action.
- Movements across gravity (i.e., parallel to the ground) are produced by a concentric action. When gravity cannot influence the joint movement in question, shortening (concentric) action is needed to pull the bone against its own inertia. The speed of movement is not a factor.
By this point, we have identified the type of muscle action. The next steps identify which muscles control the movement.
- Step 4: Identify the plane of movement (frontal, sagittal, transverse) and the axis of rotation (i.e., line about which the joint is rotating). The purpose of this step is to identify which side of the joint the muscles controlling the movement cross (e.g., flexors cross one side of a joint, while extensors cross the opposite side).
- Step 5:Ask yourself, "On which side of the joint axis are muscles lengthening and on which side are they shortening during the movement?"
- Step 6: Combine the information from steps 3 and 5 to determine which muscles must be producing or controlling the movement (or position). For example, if a concentric (shortening) action is required (from step 3) and the muscles on the anterior side of the joint are shortening (from step 5), then the anterior muscles must be actively producing the movement. The information in chapter 4 allows us to name the specific muscles.
Learn more about Dynamic Human Anatomy, Second Edition.
Ergonomic concepts
As an interdiscipline, ergonomics spans a variety of disciplines, including human anatomy, biomechanics, physiology, psychology, sociology, medicine, and engineering.
As an interdiscipline, ergonomics spans a variety of disciplines, including human anatomy, biomechanics, physiology, psychology, sociology, medicine, and engineering. Ergonomics is composed of three primary domains: organizational, cognitive, and physical. The organizational domain deals with organizational design, policies, and processes as they relate to workplace communication, work design and systems, networking, and teamwork. The cognitive domain involves mental processes, including perception, memory, reasoning, and motor response.
The physical domain is most relevant to our study of dynamic human anatomy. This domain integrates anthropometric, biomechanical, and physiological concepts as they relate to human movement, primarily in occupational settings. The principles of physical ergonomics have been used extensively in the design of consumer and industrial products, assessment of manual materials handling tasks, development of workplace safety guidelines, workplace design, and diagnosis of work-related medical conditions.
Goals
The primary goals of ergonomics are to improve productivity, improve efficiency, enhance safety, reduce injury risk, and reduce cost. Ergonomic interventions can improve both the quantity and quality of worker output and increase efficiency by facilitating production in a time-effective manner.
Safety enhancement and injury risk reduction are at the core of most ergonomic programs. One of the most common worker risks is a class of conditions collectively known as musculoskeletal disorders(MSDs). MSDs are the risk factor most closely associated with human movement tasks.
Research consistently has shown that ergonomic analysis and intervention can result in significant cost savings by reducing health care costs, lost work time, workers' compensation claims, and human error. Many ergonomic interventions are relatively inexpensive and are therefore cost effective for businesses, agencies, and workers alike.
Many governmental agencies and professional organizations have issued safety guidelines addressing specific ergonomic issues and recommendations. These guidelines cover a multitude of industrial and service areas, including agriculture, apparel and footwear, baggage handling, computer workstations, construction, health care, product manufacturing, metalwork foundries, meatpacking, mining, poultry processing, printing, sewing, shipyards, and telecommunications (U.S. Department of Labor, n.d.).
Methods of Analysis
Ergonomic analyses can be reactive or proactive. A reactive analysis addresses an existing problem or situation. A proactive analysis seeks to anticipate potential problems and make changes that prevent these problems.
An ergonomic analysis typically involves several steps, the first of which is identification of risk factors. General risk factors associated with movement-related ergonomic problems include awkward postures, repetitive motions, forceful exertions, pressure points, and sustained static postures(NIOSH, 2007).
In conducting an ergonomic assessment, the first step is to identify risk factors specific to the situation being assessed. Risk factors may be systematic (i.e., evident in the overall work environment) or specific to an individual. In assessing the work environment of a computer data-entry operator, for example, potential risk factors might include keyboard height and inclination, monitor height (relative to the operator's line of sight), distance, brightness, lack of arm and wrist support, chair design and support, and operator posture.
Once the ergonomic risk factors have been identified, the ergonomist must identify possible changes (e.g., new or adjusted keyboard, monitor, chair) to improve comfort and safety. After the changes have been implemented, the worker should be re-evaluated to ensure that the modifications have achieved the ergonomic goals.
Risk factors that are common to a group of workers can be addressed through either engineering or administrative controls. Engineering controls involve improving worker conditions by modifying tasks, adjusting movement patterns, redesigning workstations or tools, and providing protective equipment, as needed. Administrative controls include development and implementation of procedures and processes that can reduce risk such as job rotation (i.e., varying work tasks) and appropriate work breaks (e.g., rest or stretching breaks).
Numerous analysis approaches have been used to identify ergonomic problems and find solutions. Among those approaches are surveys and questionnaires, iterative prototyping, meta-analysis, work sampling, and a wide range of computer-based models applicable to specific tasks or systems.
Human - Machine Interface
Many occupations involve human interaction with a machine or device, in what is termed a human - machine interface. Examples include computer or keyboard operators (figure 13.1), assembly-line and construction workers, medical technicians and clinicians, and automobile mechanics.
Computer workstation anthropometrics for seated (left) and standing (right) operators.
Learn more about Dynamic Human Anatomy, Second Edition.
Components of muscle function
The control of even the simplest joint movement typically requires the cooperative action of several muscles working together as a single unit. This cooperative action is called muscle synergy.
The control of even the simplest joint movement typically requires the cooperative action of several muscles working together as a single unit. This cooperative action is called muscle synergy. Synergistic muscles work together, but other muscles with opposite functions may work against a particular movement. The overall, or net, effect of all muscles acting at a joint determines the ultimate mechanical effect, or movement.
Several concepts of muscle function are important for understanding how muscles cooperate and compete to control movement: agonists, neutralization, stabilization, antagonists, and coactivation.
- Agonists. Muscles that actively produce or control a single joint movement or maintain a single joint position are called agonists. In most movements, several muscles act together as agonists, with some playing a greater role than others.
- Neutralization. Muscles often perform more than one movement function at a given joint. At the ankle complex, for example, a muscle might act as both a plantar flexor and invertor (e.g., tibialis posterior). To produce pure plantar flexion, another muscle whose action produces plantar flexion and eversion (e.g., peroneus longus) would also need to be involved. The eversion action of the second muscle would cancel out, or neutralize, the inversion action of the first muscle. This process of canceling out an unwanted secondary movement is called neutralization.
- Stabilization. During concentric action, a muscle attempts to shorten by pulling its two bony attachment sites together. In most cases, the bone with the least resistance to movement (inertia) will move. When the inertia of both bones is similar in magnitude, both ends tend to move. If movement of only one end is desired, the other end must be prevented from moving, or stabilized. This stabilization is provided by other muscles or an external force. As an example, consider hip flexion created by the anterior thigh musculature. In attempting to move the femur in flexion, the hip flexors also tilt the pelvis anteriorly. If pelvic tilt is unwanted, then the abdominal musculature must act isometrically to stabilize the pelvis and prevent its movement.
- Antagonists. Muscles acting against a movement or position are called antagonists. To perform a movement most effectively, when the agonists actively shorten in concentric action, the corresponding antagonists passively lengthen. When agonists actively lengthen in eccentric action, the associated antagonists passively shorten. In many movements, then, the agonists and stabilizers are active while the antagonists are passive.
- Coactivation . Simultaneous action of both agonists and antagonists is called coactivation (also co-contraction). Coactivation might occur, for example, when an unskilled performer is unsure of the necessary muscle recruitment strategy. Skilled performers, however, do not exhibit an absence of coactivation. At least four possible explanations exist for coactivation in skilled performers: (1) less overall effort may be required in agonist - antagonist pairings for movements that involve changes of direction when the muscles maintain some level of activity, as opposed to working in an on - off manner; (2) coactivation increases joint stiffness and consequently joint stability, which may be desired for movements involving heavy loads; (3) coactivation of a single-joint muscle (e.g., gluteus maximus) and a two-joint muscle (e.g., rectus femoris) can increase the torque at a joint (e.g., knee) acted on by the two-joint muscle; and (4) given the neural complexities of the forearm and hand, fine movements of the fingers require complex coactivation strategies (Enoka, 2002).
Note that the term coactivation is limited to the concurrent action of agonists and antagonists and should not be used to describe the simultaneous action of multiple agonists. For instance, concurrent activity of the biceps brachii and triceps brachii during an elbow curl exercise would be considered coactivation. On the other hand, if the triceps was passive (i.e., inactive), simultaneous action of the three elbow flexors (biceps brachii, brachialis, brachioradialis) would not be considered coactivation.
With these concepts in mind, we now consider a simple yet fundamental question: How do we determine which muscles are active in producing or controlling a given movement?
Learn more about Dynamic Human Anatomy, Second Edition.
Determine the involved muscles and their action for any joint movement
One of the most fundamental and important goals of movement analysis is identifying which specific muscles are active in producing and controlling movement at a particular joint.
One of the most fundamental and important goals of movement analysis is identifying which specific muscles are active in producing and controlling movement at a particular joint. In chapter 4, we presented specific muscles and their concentric actions. However, we know that muscles can act in three modes: isometric, concentric, and eccentric. The task at hand, therefore, is to determine for a given joint movement (1) the specific muscles involved in controlling the movement and (2) the type of muscle action.
The following muscle control formula provides a step-by-step procedure for determining the involved muscles and their action for any joint movement. This formula may appear a bit cumbersome and complex at first glance. However, with practice, you should be able to get through it quickly. Eventually (with enough practice), the process will become automatic and instinctive, and you will be able to analyze movements without consciously going through each step in the formula. It helps, though, to use the formula until you develop these movement analysis instincts.
Muscle Control Formula
We begin the muscle control formula with a statement of the problem: Given a specific joint movement (or position), identify the name of the movement (or position), the plane of movement, the effect of the external force acting on the system, the type of muscle action (i.e., shortening or concentric, lengthening or eccentric, or isometric), and the muscles involved (i.e., which muscle or muscles are actively involved in producing or controlling the movement or in maintaining a position).
Now, we move on to the formula itself, which involves six steps:
- Step 1: Identify the joint movement (e.g., flexion, abduction) or position.
- Step 2: Identify the effect of the external force (e.g., gravity) on the joint movement or position by asking the following question: What movement would the external force produce in the absence of muscle action (i.e., if there were no active muscles)?
- Step 3: Identify the type of muscle action (concentric, eccentric, isometric) based on the answers to step 1 (#1) and step 2 (#2) as follows:
- If #1 and #2 are in opposite directions, then the muscles are actively shortening in a concentric action. Speed of movement is not a factor.
- If #1 and #2 are in the same direction, then ask yourself, "What is the speed of movement?"
- If the movement is faster than what the external force would produce by itself, then the muscles are actively shortening in a concentric action.
- If the movement is slower than what the external force would produce by itself, then the muscles are actively lengthening in an eccentric action.
- If no movement is occurring, yet the external force would produce movement if acting by itself, then the muscles are performing an isometric action.
- Movements across gravity (i.e., parallel to the ground) are produced by a concentric action. When gravity cannot influence the joint movement in question, shortening (concentric) action is needed to pull the bone against its own inertia. The speed of movement is not a factor.
By this point, we have identified the type of muscle action. The next steps identify which muscles control the movement.
- Step 4: Identify the plane of movement (frontal, sagittal, transverse) and the axis of rotation (i.e., line about which the joint is rotating). The purpose of this step is to identify which side of the joint the muscles controlling the movement cross (e.g., flexors cross one side of a joint, while extensors cross the opposite side).
- Step 5:Ask yourself, "On which side of the joint axis are muscles lengthening and on which side are they shortening during the movement?"
- Step 6: Combine the information from steps 3 and 5 to determine which muscles must be producing or controlling the movement (or position). For example, if a concentric (shortening) action is required (from step 3) and the muscles on the anterior side of the joint are shortening (from step 5), then the anterior muscles must be actively producing the movement. The information in chapter 4 allows us to name the specific muscles.
Learn more about Dynamic Human Anatomy, Second Edition.
Ergonomic concepts
As an interdiscipline, ergonomics spans a variety of disciplines, including human anatomy, biomechanics, physiology, psychology, sociology, medicine, and engineering.
As an interdiscipline, ergonomics spans a variety of disciplines, including human anatomy, biomechanics, physiology, psychology, sociology, medicine, and engineering. Ergonomics is composed of three primary domains: organizational, cognitive, and physical. The organizational domain deals with organizational design, policies, and processes as they relate to workplace communication, work design and systems, networking, and teamwork. The cognitive domain involves mental processes, including perception, memory, reasoning, and motor response.
The physical domain is most relevant to our study of dynamic human anatomy. This domain integrates anthropometric, biomechanical, and physiological concepts as they relate to human movement, primarily in occupational settings. The principles of physical ergonomics have been used extensively in the design of consumer and industrial products, assessment of manual materials handling tasks, development of workplace safety guidelines, workplace design, and diagnosis of work-related medical conditions.
Goals
The primary goals of ergonomics are to improve productivity, improve efficiency, enhance safety, reduce injury risk, and reduce cost. Ergonomic interventions can improve both the quantity and quality of worker output and increase efficiency by facilitating production in a time-effective manner.
Safety enhancement and injury risk reduction are at the core of most ergonomic programs. One of the most common worker risks is a class of conditions collectively known as musculoskeletal disorders(MSDs). MSDs are the risk factor most closely associated with human movement tasks.
Research consistently has shown that ergonomic analysis and intervention can result in significant cost savings by reducing health care costs, lost work time, workers' compensation claims, and human error. Many ergonomic interventions are relatively inexpensive and are therefore cost effective for businesses, agencies, and workers alike.
Many governmental agencies and professional organizations have issued safety guidelines addressing specific ergonomic issues and recommendations. These guidelines cover a multitude of industrial and service areas, including agriculture, apparel and footwear, baggage handling, computer workstations, construction, health care, product manufacturing, metalwork foundries, meatpacking, mining, poultry processing, printing, sewing, shipyards, and telecommunications (U.S. Department of Labor, n.d.).
Methods of Analysis
Ergonomic analyses can be reactive or proactive. A reactive analysis addresses an existing problem or situation. A proactive analysis seeks to anticipate potential problems and make changes that prevent these problems.
An ergonomic analysis typically involves several steps, the first of which is identification of risk factors. General risk factors associated with movement-related ergonomic problems include awkward postures, repetitive motions, forceful exertions, pressure points, and sustained static postures(NIOSH, 2007).
In conducting an ergonomic assessment, the first step is to identify risk factors specific to the situation being assessed. Risk factors may be systematic (i.e., evident in the overall work environment) or specific to an individual. In assessing the work environment of a computer data-entry operator, for example, potential risk factors might include keyboard height and inclination, monitor height (relative to the operator's line of sight), distance, brightness, lack of arm and wrist support, chair design and support, and operator posture.
Once the ergonomic risk factors have been identified, the ergonomist must identify possible changes (e.g., new or adjusted keyboard, monitor, chair) to improve comfort and safety. After the changes have been implemented, the worker should be re-evaluated to ensure that the modifications have achieved the ergonomic goals.
Risk factors that are common to a group of workers can be addressed through either engineering or administrative controls. Engineering controls involve improving worker conditions by modifying tasks, adjusting movement patterns, redesigning workstations or tools, and providing protective equipment, as needed. Administrative controls include development and implementation of procedures and processes that can reduce risk such as job rotation (i.e., varying work tasks) and appropriate work breaks (e.g., rest or stretching breaks).
Numerous analysis approaches have been used to identify ergonomic problems and find solutions. Among those approaches are surveys and questionnaires, iterative prototyping, meta-analysis, work sampling, and a wide range of computer-based models applicable to specific tasks or systems.
Human - Machine Interface
Many occupations involve human interaction with a machine or device, in what is termed a human - machine interface. Examples include computer or keyboard operators (figure 13.1), assembly-line and construction workers, medical technicians and clinicians, and automobile mechanics.
Computer workstation anthropometrics for seated (left) and standing (right) operators.
Learn more about Dynamic Human Anatomy, Second Edition.
Components of muscle function
The control of even the simplest joint movement typically requires the cooperative action of several muscles working together as a single unit. This cooperative action is called muscle synergy.
The control of even the simplest joint movement typically requires the cooperative action of several muscles working together as a single unit. This cooperative action is called muscle synergy. Synergistic muscles work together, but other muscles with opposite functions may work against a particular movement. The overall, or net, effect of all muscles acting at a joint determines the ultimate mechanical effect, or movement.
Several concepts of muscle function are important for understanding how muscles cooperate and compete to control movement: agonists, neutralization, stabilization, antagonists, and coactivation.
- Agonists. Muscles that actively produce or control a single joint movement or maintain a single joint position are called agonists. In most movements, several muscles act together as agonists, with some playing a greater role than others.
- Neutralization. Muscles often perform more than one movement function at a given joint. At the ankle complex, for example, a muscle might act as both a plantar flexor and invertor (e.g., tibialis posterior). To produce pure plantar flexion, another muscle whose action produces plantar flexion and eversion (e.g., peroneus longus) would also need to be involved. The eversion action of the second muscle would cancel out, or neutralize, the inversion action of the first muscle. This process of canceling out an unwanted secondary movement is called neutralization.
- Stabilization. During concentric action, a muscle attempts to shorten by pulling its two bony attachment sites together. In most cases, the bone with the least resistance to movement (inertia) will move. When the inertia of both bones is similar in magnitude, both ends tend to move. If movement of only one end is desired, the other end must be prevented from moving, or stabilized. This stabilization is provided by other muscles or an external force. As an example, consider hip flexion created by the anterior thigh musculature. In attempting to move the femur in flexion, the hip flexors also tilt the pelvis anteriorly. If pelvic tilt is unwanted, then the abdominal musculature must act isometrically to stabilize the pelvis and prevent its movement.
- Antagonists. Muscles acting against a movement or position are called antagonists. To perform a movement most effectively, when the agonists actively shorten in concentric action, the corresponding antagonists passively lengthen. When agonists actively lengthen in eccentric action, the associated antagonists passively shorten. In many movements, then, the agonists and stabilizers are active while the antagonists are passive.
- Coactivation . Simultaneous action of both agonists and antagonists is called coactivation (also co-contraction). Coactivation might occur, for example, when an unskilled performer is unsure of the necessary muscle recruitment strategy. Skilled performers, however, do not exhibit an absence of coactivation. At least four possible explanations exist for coactivation in skilled performers: (1) less overall effort may be required in agonist - antagonist pairings for movements that involve changes of direction when the muscles maintain some level of activity, as opposed to working in an on - off manner; (2) coactivation increases joint stiffness and consequently joint stability, which may be desired for movements involving heavy loads; (3) coactivation of a single-joint muscle (e.g., gluteus maximus) and a two-joint muscle (e.g., rectus femoris) can increase the torque at a joint (e.g., knee) acted on by the two-joint muscle; and (4) given the neural complexities of the forearm and hand, fine movements of the fingers require complex coactivation strategies (Enoka, 2002).
Note that the term coactivation is limited to the concurrent action of agonists and antagonists and should not be used to describe the simultaneous action of multiple agonists. For instance, concurrent activity of the biceps brachii and triceps brachii during an elbow curl exercise would be considered coactivation. On the other hand, if the triceps was passive (i.e., inactive), simultaneous action of the three elbow flexors (biceps brachii, brachialis, brachioradialis) would not be considered coactivation.
With these concepts in mind, we now consider a simple yet fundamental question: How do we determine which muscles are active in producing or controlling a given movement?
Learn more about Dynamic Human Anatomy, Second Edition.
Determine the involved muscles and their action for any joint movement
One of the most fundamental and important goals of movement analysis is identifying which specific muscles are active in producing and controlling movement at a particular joint.
One of the most fundamental and important goals of movement analysis is identifying which specific muscles are active in producing and controlling movement at a particular joint. In chapter 4, we presented specific muscles and their concentric actions. However, we know that muscles can act in three modes: isometric, concentric, and eccentric. The task at hand, therefore, is to determine for a given joint movement (1) the specific muscles involved in controlling the movement and (2) the type of muscle action.
The following muscle control formula provides a step-by-step procedure for determining the involved muscles and their action for any joint movement. This formula may appear a bit cumbersome and complex at first glance. However, with practice, you should be able to get through it quickly. Eventually (with enough practice), the process will become automatic and instinctive, and you will be able to analyze movements without consciously going through each step in the formula. It helps, though, to use the formula until you develop these movement analysis instincts.
Muscle Control Formula
We begin the muscle control formula with a statement of the problem: Given a specific joint movement (or position), identify the name of the movement (or position), the plane of movement, the effect of the external force acting on the system, the type of muscle action (i.e., shortening or concentric, lengthening or eccentric, or isometric), and the muscles involved (i.e., which muscle or muscles are actively involved in producing or controlling the movement or in maintaining a position).
Now, we move on to the formula itself, which involves six steps:
- Step 1: Identify the joint movement (e.g., flexion, abduction) or position.
- Step 2: Identify the effect of the external force (e.g., gravity) on the joint movement or position by asking the following question: What movement would the external force produce in the absence of muscle action (i.e., if there were no active muscles)?
- Step 3: Identify the type of muscle action (concentric, eccentric, isometric) based on the answers to step 1 (#1) and step 2 (#2) as follows:
- If #1 and #2 are in opposite directions, then the muscles are actively shortening in a concentric action. Speed of movement is not a factor.
- If #1 and #2 are in the same direction, then ask yourself, "What is the speed of movement?"
- If the movement is faster than what the external force would produce by itself, then the muscles are actively shortening in a concentric action.
- If the movement is slower than what the external force would produce by itself, then the muscles are actively lengthening in an eccentric action.
- If no movement is occurring, yet the external force would produce movement if acting by itself, then the muscles are performing an isometric action.
- Movements across gravity (i.e., parallel to the ground) are produced by a concentric action. When gravity cannot influence the joint movement in question, shortening (concentric) action is needed to pull the bone against its own inertia. The speed of movement is not a factor.
By this point, we have identified the type of muscle action. The next steps identify which muscles control the movement.
- Step 4: Identify the plane of movement (frontal, sagittal, transverse) and the axis of rotation (i.e., line about which the joint is rotating). The purpose of this step is to identify which side of the joint the muscles controlling the movement cross (e.g., flexors cross one side of a joint, while extensors cross the opposite side).
- Step 5:Ask yourself, "On which side of the joint axis are muscles lengthening and on which side are they shortening during the movement?"
- Step 6: Combine the information from steps 3 and 5 to determine which muscles must be producing or controlling the movement (or position). For example, if a concentric (shortening) action is required (from step 3) and the muscles on the anterior side of the joint are shortening (from step 5), then the anterior muscles must be actively producing the movement. The information in chapter 4 allows us to name the specific muscles.
Learn more about Dynamic Human Anatomy, Second Edition.
Ergonomic concepts
As an interdiscipline, ergonomics spans a variety of disciplines, including human anatomy, biomechanics, physiology, psychology, sociology, medicine, and engineering.
As an interdiscipline, ergonomics spans a variety of disciplines, including human anatomy, biomechanics, physiology, psychology, sociology, medicine, and engineering. Ergonomics is composed of three primary domains: organizational, cognitive, and physical. The organizational domain deals with organizational design, policies, and processes as they relate to workplace communication, work design and systems, networking, and teamwork. The cognitive domain involves mental processes, including perception, memory, reasoning, and motor response.
The physical domain is most relevant to our study of dynamic human anatomy. This domain integrates anthropometric, biomechanical, and physiological concepts as they relate to human movement, primarily in occupational settings. The principles of physical ergonomics have been used extensively in the design of consumer and industrial products, assessment of manual materials handling tasks, development of workplace safety guidelines, workplace design, and diagnosis of work-related medical conditions.
Goals
The primary goals of ergonomics are to improve productivity, improve efficiency, enhance safety, reduce injury risk, and reduce cost. Ergonomic interventions can improve both the quantity and quality of worker output and increase efficiency by facilitating production in a time-effective manner.
Safety enhancement and injury risk reduction are at the core of most ergonomic programs. One of the most common worker risks is a class of conditions collectively known as musculoskeletal disorders(MSDs). MSDs are the risk factor most closely associated with human movement tasks.
Research consistently has shown that ergonomic analysis and intervention can result in significant cost savings by reducing health care costs, lost work time, workers' compensation claims, and human error. Many ergonomic interventions are relatively inexpensive and are therefore cost effective for businesses, agencies, and workers alike.
Many governmental agencies and professional organizations have issued safety guidelines addressing specific ergonomic issues and recommendations. These guidelines cover a multitude of industrial and service areas, including agriculture, apparel and footwear, baggage handling, computer workstations, construction, health care, product manufacturing, metalwork foundries, meatpacking, mining, poultry processing, printing, sewing, shipyards, and telecommunications (U.S. Department of Labor, n.d.).
Methods of Analysis
Ergonomic analyses can be reactive or proactive. A reactive analysis addresses an existing problem or situation. A proactive analysis seeks to anticipate potential problems and make changes that prevent these problems.
An ergonomic analysis typically involves several steps, the first of which is identification of risk factors. General risk factors associated with movement-related ergonomic problems include awkward postures, repetitive motions, forceful exertions, pressure points, and sustained static postures(NIOSH, 2007).
In conducting an ergonomic assessment, the first step is to identify risk factors specific to the situation being assessed. Risk factors may be systematic (i.e., evident in the overall work environment) or specific to an individual. In assessing the work environment of a computer data-entry operator, for example, potential risk factors might include keyboard height and inclination, monitor height (relative to the operator's line of sight), distance, brightness, lack of arm and wrist support, chair design and support, and operator posture.
Once the ergonomic risk factors have been identified, the ergonomist must identify possible changes (e.g., new or adjusted keyboard, monitor, chair) to improve comfort and safety. After the changes have been implemented, the worker should be re-evaluated to ensure that the modifications have achieved the ergonomic goals.
Risk factors that are common to a group of workers can be addressed through either engineering or administrative controls. Engineering controls involve improving worker conditions by modifying tasks, adjusting movement patterns, redesigning workstations or tools, and providing protective equipment, as needed. Administrative controls include development and implementation of procedures and processes that can reduce risk such as job rotation (i.e., varying work tasks) and appropriate work breaks (e.g., rest or stretching breaks).
Numerous analysis approaches have been used to identify ergonomic problems and find solutions. Among those approaches are surveys and questionnaires, iterative prototyping, meta-analysis, work sampling, and a wide range of computer-based models applicable to specific tasks or systems.
Human - Machine Interface
Many occupations involve human interaction with a machine or device, in what is termed a human - machine interface. Examples include computer or keyboard operators (figure 13.1), assembly-line and construction workers, medical technicians and clinicians, and automobile mechanics.
Computer workstation anthropometrics for seated (left) and standing (right) operators.
Learn more about Dynamic Human Anatomy, Second Edition.
Components of muscle function
The control of even the simplest joint movement typically requires the cooperative action of several muscles working together as a single unit. This cooperative action is called muscle synergy.
The control of even the simplest joint movement typically requires the cooperative action of several muscles working together as a single unit. This cooperative action is called muscle synergy. Synergistic muscles work together, but other muscles with opposite functions may work against a particular movement. The overall, or net, effect of all muscles acting at a joint determines the ultimate mechanical effect, or movement.
Several concepts of muscle function are important for understanding how muscles cooperate and compete to control movement: agonists, neutralization, stabilization, antagonists, and coactivation.
- Agonists. Muscles that actively produce or control a single joint movement or maintain a single joint position are called agonists. In most movements, several muscles act together as agonists, with some playing a greater role than others.
- Neutralization. Muscles often perform more than one movement function at a given joint. At the ankle complex, for example, a muscle might act as both a plantar flexor and invertor (e.g., tibialis posterior). To produce pure plantar flexion, another muscle whose action produces plantar flexion and eversion (e.g., peroneus longus) would also need to be involved. The eversion action of the second muscle would cancel out, or neutralize, the inversion action of the first muscle. This process of canceling out an unwanted secondary movement is called neutralization.
- Stabilization. During concentric action, a muscle attempts to shorten by pulling its two bony attachment sites together. In most cases, the bone with the least resistance to movement (inertia) will move. When the inertia of both bones is similar in magnitude, both ends tend to move. If movement of only one end is desired, the other end must be prevented from moving, or stabilized. This stabilization is provided by other muscles or an external force. As an example, consider hip flexion created by the anterior thigh musculature. In attempting to move the femur in flexion, the hip flexors also tilt the pelvis anteriorly. If pelvic tilt is unwanted, then the abdominal musculature must act isometrically to stabilize the pelvis and prevent its movement.
- Antagonists. Muscles acting against a movement or position are called antagonists. To perform a movement most effectively, when the agonists actively shorten in concentric action, the corresponding antagonists passively lengthen. When agonists actively lengthen in eccentric action, the associated antagonists passively shorten. In many movements, then, the agonists and stabilizers are active while the antagonists are passive.
- Coactivation . Simultaneous action of both agonists and antagonists is called coactivation (also co-contraction). Coactivation might occur, for example, when an unskilled performer is unsure of the necessary muscle recruitment strategy. Skilled performers, however, do not exhibit an absence of coactivation. At least four possible explanations exist for coactivation in skilled performers: (1) less overall effort may be required in agonist - antagonist pairings for movements that involve changes of direction when the muscles maintain some level of activity, as opposed to working in an on - off manner; (2) coactivation increases joint stiffness and consequently joint stability, which may be desired for movements involving heavy loads; (3) coactivation of a single-joint muscle (e.g., gluteus maximus) and a two-joint muscle (e.g., rectus femoris) can increase the torque at a joint (e.g., knee) acted on by the two-joint muscle; and (4) given the neural complexities of the forearm and hand, fine movements of the fingers require complex coactivation strategies (Enoka, 2002).
Note that the term coactivation is limited to the concurrent action of agonists and antagonists and should not be used to describe the simultaneous action of multiple agonists. For instance, concurrent activity of the biceps brachii and triceps brachii during an elbow curl exercise would be considered coactivation. On the other hand, if the triceps was passive (i.e., inactive), simultaneous action of the three elbow flexors (biceps brachii, brachialis, brachioradialis) would not be considered coactivation.
With these concepts in mind, we now consider a simple yet fundamental question: How do we determine which muscles are active in producing or controlling a given movement?
Learn more about Dynamic Human Anatomy, Second Edition.
Determine the involved muscles and their action for any joint movement
One of the most fundamental and important goals of movement analysis is identifying which specific muscles are active in producing and controlling movement at a particular joint.
One of the most fundamental and important goals of movement analysis is identifying which specific muscles are active in producing and controlling movement at a particular joint. In chapter 4, we presented specific muscles and their concentric actions. However, we know that muscles can act in three modes: isometric, concentric, and eccentric. The task at hand, therefore, is to determine for a given joint movement (1) the specific muscles involved in controlling the movement and (2) the type of muscle action.
The following muscle control formula provides a step-by-step procedure for determining the involved muscles and their action for any joint movement. This formula may appear a bit cumbersome and complex at first glance. However, with practice, you should be able to get through it quickly. Eventually (with enough practice), the process will become automatic and instinctive, and you will be able to analyze movements without consciously going through each step in the formula. It helps, though, to use the formula until you develop these movement analysis instincts.
Muscle Control Formula
We begin the muscle control formula with a statement of the problem: Given a specific joint movement (or position), identify the name of the movement (or position), the plane of movement, the effect of the external force acting on the system, the type of muscle action (i.e., shortening or concentric, lengthening or eccentric, or isometric), and the muscles involved (i.e., which muscle or muscles are actively involved in producing or controlling the movement or in maintaining a position).
Now, we move on to the formula itself, which involves six steps:
- Step 1: Identify the joint movement (e.g., flexion, abduction) or position.
- Step 2: Identify the effect of the external force (e.g., gravity) on the joint movement or position by asking the following question: What movement would the external force produce in the absence of muscle action (i.e., if there were no active muscles)?
- Step 3: Identify the type of muscle action (concentric, eccentric, isometric) based on the answers to step 1 (#1) and step 2 (#2) as follows:
- If #1 and #2 are in opposite directions, then the muscles are actively shortening in a concentric action. Speed of movement is not a factor.
- If #1 and #2 are in the same direction, then ask yourself, "What is the speed of movement?"
- If the movement is faster than what the external force would produce by itself, then the muscles are actively shortening in a concentric action.
- If the movement is slower than what the external force would produce by itself, then the muscles are actively lengthening in an eccentric action.
- If no movement is occurring, yet the external force would produce movement if acting by itself, then the muscles are performing an isometric action.
- Movements across gravity (i.e., parallel to the ground) are produced by a concentric action. When gravity cannot influence the joint movement in question, shortening (concentric) action is needed to pull the bone against its own inertia. The speed of movement is not a factor.
By this point, we have identified the type of muscle action. The next steps identify which muscles control the movement.
- Step 4: Identify the plane of movement (frontal, sagittal, transverse) and the axis of rotation (i.e., line about which the joint is rotating). The purpose of this step is to identify which side of the joint the muscles controlling the movement cross (e.g., flexors cross one side of a joint, while extensors cross the opposite side).
- Step 5:Ask yourself, "On which side of the joint axis are muscles lengthening and on which side are they shortening during the movement?"
- Step 6: Combine the information from steps 3 and 5 to determine which muscles must be producing or controlling the movement (or position). For example, if a concentric (shortening) action is required (from step 3) and the muscles on the anterior side of the joint are shortening (from step 5), then the anterior muscles must be actively producing the movement. The information in chapter 4 allows us to name the specific muscles.
Learn more about Dynamic Human Anatomy, Second Edition.
Ergonomic concepts
As an interdiscipline, ergonomics spans a variety of disciplines, including human anatomy, biomechanics, physiology, psychology, sociology, medicine, and engineering.
As an interdiscipline, ergonomics spans a variety of disciplines, including human anatomy, biomechanics, physiology, psychology, sociology, medicine, and engineering. Ergonomics is composed of three primary domains: organizational, cognitive, and physical. The organizational domain deals with organizational design, policies, and processes as they relate to workplace communication, work design and systems, networking, and teamwork. The cognitive domain involves mental processes, including perception, memory, reasoning, and motor response.
The physical domain is most relevant to our study of dynamic human anatomy. This domain integrates anthropometric, biomechanical, and physiological concepts as they relate to human movement, primarily in occupational settings. The principles of physical ergonomics have been used extensively in the design of consumer and industrial products, assessment of manual materials handling tasks, development of workplace safety guidelines, workplace design, and diagnosis of work-related medical conditions.
Goals
The primary goals of ergonomics are to improve productivity, improve efficiency, enhance safety, reduce injury risk, and reduce cost. Ergonomic interventions can improve both the quantity and quality of worker output and increase efficiency by facilitating production in a time-effective manner.
Safety enhancement and injury risk reduction are at the core of most ergonomic programs. One of the most common worker risks is a class of conditions collectively known as musculoskeletal disorders(MSDs). MSDs are the risk factor most closely associated with human movement tasks.
Research consistently has shown that ergonomic analysis and intervention can result in significant cost savings by reducing health care costs, lost work time, workers' compensation claims, and human error. Many ergonomic interventions are relatively inexpensive and are therefore cost effective for businesses, agencies, and workers alike.
Many governmental agencies and professional organizations have issued safety guidelines addressing specific ergonomic issues and recommendations. These guidelines cover a multitude of industrial and service areas, including agriculture, apparel and footwear, baggage handling, computer workstations, construction, health care, product manufacturing, metalwork foundries, meatpacking, mining, poultry processing, printing, sewing, shipyards, and telecommunications (U.S. Department of Labor, n.d.).
Methods of Analysis
Ergonomic analyses can be reactive or proactive. A reactive analysis addresses an existing problem or situation. A proactive analysis seeks to anticipate potential problems and make changes that prevent these problems.
An ergonomic analysis typically involves several steps, the first of which is identification of risk factors. General risk factors associated with movement-related ergonomic problems include awkward postures, repetitive motions, forceful exertions, pressure points, and sustained static postures(NIOSH, 2007).
In conducting an ergonomic assessment, the first step is to identify risk factors specific to the situation being assessed. Risk factors may be systematic (i.e., evident in the overall work environment) or specific to an individual. In assessing the work environment of a computer data-entry operator, for example, potential risk factors might include keyboard height and inclination, monitor height (relative to the operator's line of sight), distance, brightness, lack of arm and wrist support, chair design and support, and operator posture.
Once the ergonomic risk factors have been identified, the ergonomist must identify possible changes (e.g., new or adjusted keyboard, monitor, chair) to improve comfort and safety. After the changes have been implemented, the worker should be re-evaluated to ensure that the modifications have achieved the ergonomic goals.
Risk factors that are common to a group of workers can be addressed through either engineering or administrative controls. Engineering controls involve improving worker conditions by modifying tasks, adjusting movement patterns, redesigning workstations or tools, and providing protective equipment, as needed. Administrative controls include development and implementation of procedures and processes that can reduce risk such as job rotation (i.e., varying work tasks) and appropriate work breaks (e.g., rest or stretching breaks).
Numerous analysis approaches have been used to identify ergonomic problems and find solutions. Among those approaches are surveys and questionnaires, iterative prototyping, meta-analysis, work sampling, and a wide range of computer-based models applicable to specific tasks or systems.
Human - Machine Interface
Many occupations involve human interaction with a machine or device, in what is termed a human - machine interface. Examples include computer or keyboard operators (figure 13.1), assembly-line and construction workers, medical technicians and clinicians, and automobile mechanics.
Computer workstation anthropometrics for seated (left) and standing (right) operators.
Learn more about Dynamic Human Anatomy, Second Edition.
Related Books









