- Home
- Medicine in Exercise and Sport
- Health Care in Exercise and Sport
- Cardiopulmonary Rehabilitation
- Health Care for Special Conditions
- Guidelines for Cardiac Rehabilitation Programs

Cardiovascular disease (CVD) is the principal cause of death worldwide. It is projected that by 2035, more than 130 million adults in the United States will have CVD. The challenge to CR professionals is to select, develop, and deliver appropriate rehabilitative and secondary prevention services to each patient tailored to their individual needs. Guidelines for Cardiac Rehabilitation Programs, Sixth Edition, is the definitive resource for developing inpatient and outpatient cardiac rehabilitation programs.
The sixth edition of Guidelines for Cardiac Rehabilitation Programs equips professionals with current scientific and evidence-based models for designing and updating rehabilitation programs. Pedagogical aides such as chapter objectives, bottom line sections, summaries, and sidebars present technical information in an easy-to-follow format. Key features of the sixth edition include the following:
- A new chapter on physical activity and exercise that helps readers understand how to develop and implement exercise programs to CVD patients
- A new chapter on cardiac disease populations that offers readers a deeper understanding of CVD populations, including those with heart valve replacement or repair surgery, left ventricular assist devices, heart transplant, dysrhythmias, and/or peripheral artery disease
- Case studies and discussion questions that challenge readers to consider how concepts from the text apply to real-life scenarios
- An expanded web resource that includes ready-to-use forms, charts, checklists, and logs that are practical for daily use, as well as additional case studies and review questions
Note: The web resource is included with all new print books and some ebooks. For ebook formats that don’t provide access, the web resource is available separately.
Ana Mola, PhD, ANP-BC
CR and Population Health Management
CR and Value-Based Care
CR and Care Coordination
Summary
Chapter 2. The Continuum of Care: From Inpatient and Outpatient CR to Long-Term Secondary Prevention
Cathie Biga, MSN, FACC
CVD Continuum of Care
Efforts to Reduce Gaps in the Continuum of Care
The Role of CR in the Continuum of Care
Putting It All Together
Summary
Chapter 3. CR in Inpatient and Transitional Settings
Mary Dolansky, PhD, RN, FAAN; Ana Mola, PhD, ANP-BC
Assessment, Mobilization, and Risk Factor Management
Discharge Planning
Clinical Pathways
Staffing
Space and Equipment
Transitional Settings
Summary
Chapter 4. Medical Evaluation and Exercise Testing for Outpatient CR
Sherrie Khadanga, MD
Physical Examination
Risk Stratification and Identification of Contraindications for Exercise Training
Summary
Chapter 5. Outpatient CR and SP
Philip A. Ades, MD, FACC, MAACVPR
Structure of CR and SP
Assessment and Management of Risk Factors for CVD Progression
Coaching, Case Management, and Counseling
Innovation in CR
Maintenance CR
Future Directions
Summary
Chapter 6. Physical Activity and Exercise
Jonathan Myers, PhD
Cardiorespiratory Endurance Training
Exercise Recommendations for Patients Without a Recent Exercise Test
PA Outside of CR
Resistance Training
Flexibility Training
Summary
Chapter 7. Nutrition Guidelines
Ellen Schaaf Aberegg, MA, LD, RD, FAACVPR
Key Nutrition Principles
Diet Patterns of Nutrition Intake
Evidence-Based Nutrition Guidelines for CVD Risk Factors
Nutrition in the CR Care Process
Dietitian–CR Professional Partnership
Summary
Chapter 8. Behavior Modification for Risk Factor Reduction: Guiding Principles and Practice
Diann Galeema, PhD
Overview of Health-Related Behavior Change
Summary
Chapter 9. Modifiable CVD Risk Factors
Sheri R. Colberg, PhD, FACSM; Emma Fletcher, MS, MVB; Carly Goldstein, PhD; Paul M. Gordon, PhD, MPH, FACSM; Joel Hughes, PhD, FAACVPR; Jonathan Myers, PhD; Quinn R. Pack, MD, MsC, FAACVPR; Killian Robinson, MD, FAHA, FACC, FACP
Physical Inactivity
Dyslipidemia
Diabetes
Tobacco Use
Hypertension
Overweight and Obesity
Psychosocial Considerations
Environmental Considerations
Summary
Chapter 10. Cardiac Disease Populations
Alison L. Bailey, MD, FACC; Alexis L. Beatty, MD, MAS; Brian Carlin, MD, FCCP, MAACVPR, FAARC; Dennis J. Kerrigan, PhD, FACSM; Steven J. Keteyian, PhD; Kirstine Laerum Sibilitz, MD, PhD; Karen Lui, RN, MS, MAACVPR; Ryan Mays, PhD, MPH; Jonathan Powell, MD; Ray W. Squires, PhD; Diane J. Treat-Jacobson, PhD, RN, FAAN
CR for Patients With CVD
Heart Valve Replacement and Repair Surgery
Dysrhythmias
Heart Failure and Left Ventricular Assist Devices
Heart Transplantation
Peripheral Artery Disease
Chronic Lung Disease
Summary
Chapter 11. Special Demographic Populations
Justin M. Bachmann, MD, MPH, FACC; Daniel Forman, MD; Naomi Gauthier, MD; Alexander Opotowsky, MD, MPH, MMsc; Marta Supervia MD, MSc, CCRP; Carmen Terzic, MD, PhD
Younger Adults
Older Adults
Women and Men
Race and Culture
Socioeconomic Considerations
Summary
Chapter 12. Program Administration
Karen Lui, RN, MS, MAACVPR
Program Priorities
Facilities and Equipment
Organizational Policies and Procedures
Insurance and Reimbursement
Documentation
Personnel
Continuum of Care and Services
Summary
Chapter 13. Outcomes Assessment and Utilization
Sherry L. Grace, PhD, FCCS, FAACVPR, CRFC
Purposes for Measuring Outcomes
Outcomes Matrix
Measuring, Documenting, Analyzing, and Reporting Program Outcomes
Resources
Summary
Chapter 14. Management of Medical Problems and Emergencies
Jason L. Rengo, MS, FAACVPR
Potential Risks in Outpatient CR
Intervention Summary
Phase 3 CR Programs
Alternative Models of SP
Summary
Appendix A. Example of Standing Orders to Initiate Outpatient CR
Appendix B. Example of Outpatient CR Emergency Standing Orders
Appendix C. Cardiac Rehabilitation Untoward Event—Physician Notification
Appendix D. Daily Emergency Cart Checklist
Appendix E. Monthly Emergency Cart Checklist
Appendix F. Emergency Equipment Maintenance Log
Founded in 1985, the American Association of Cardiovascular and Pulmonary Rehabilitation (AACVPR) is a multidisciplinary professional association comprised of health professionals who serve in the field of cardiac and pulmonary rehabilitation. AACVPR is dedicated to improving the quality of life for patients and their families by reducing morbidity, mortality, and disability from cardiovascular and pulmonary disease through education, prevention, rehabilitation, research, and disease management. AACVPR provides educational, networking, and professional development opportunities, such as live webcasts and online modules, an annual conference and affiliate meetings, professional and program certifications, outpatient data registries, legislative advocacy, leadership opportunities, and more. AACVPR membership is comprised of cardiovascular and pulmonary physicians, nurses, clinical exercise physiologists, physical therapists, behavioral scientists, respiratory therapists, dieticians, and nutritionists.
"Readers of this book will obtain up-to-date, evidence-based information to help them provide quality care to their patients."
© Doody’s Review Service, 2020, Saroj Khadka, MD, East Tennessee State University Quillen College of Medicine (4-star review)
Considerations for the prescription of exercise and physical activity
By Jonathan Myers
Guideline 6.1 Considerations for the Prescription of Exercise and Physical Activity
When developing an exercise prescription, consider the following factors:
Safety Factors
- Clinical history
- Risks associated with CVD progression or instability
- Ischemic and angina thresholds
- Cognitive or psychological impairment
Associated Factors
- Vocational or avocational requirements
- Orthopedic limitations
- Previous and current activities
- Personal health and fitness goals
An important initial consideration in exercise planning is safety. Safety considerations apply to both structured exercise training and leisure-time PA. While most patients can engage in exercise without incurring undue risks, appropriate risk stratification should be performed. Guideline 6.1 provides key variables to consider when developing an exercise prescription. Safety and risk stratification are discussed in detail in chapters 4 and 5. Recommendations for supervision and ECG monitoring can be found in chapter 5. Later in this chapter, tables 6.1 and 6.2 present basic principles of exercise prescription. A model for risk stratification for cardiovascular events is outlined in the sidebar Stratification of Risk for Cardiac Events During Exercise Participation in chapter 5. After risk stratification, recommendations for supervision, ECG, monitoring and prescribed intensity and duration of exercise training can be made.
Comprehensive, evidence-based recommendations for structured exercise training in CR are available from several prominent organizations1,3,8 and are only summarized here. A comprehensive exercise program includes cardiorespiratory, musculoskeletal, and flexibility components. Specific elements for each component are summarized in the tables in this chapter and include guidelines for intensity, duration, frequency, and type of exercise for training. Each of the elements should be prescribed relative to one another and in a way that effectively addresses predefined training goals (e.g., increased aerobic or musculoskeletal fitness, weight reduction, control of blood glucose, or resumption of occupation).
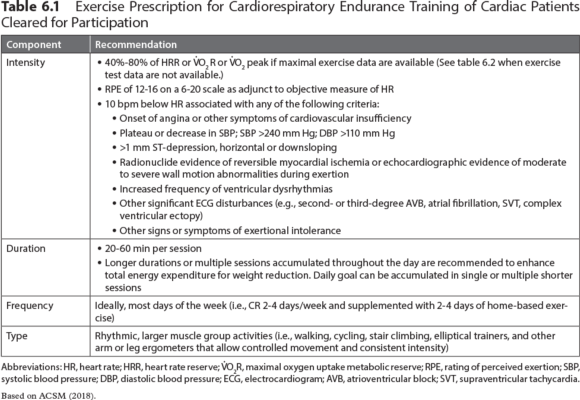
Cardiorespiratory Endurance Training
Cardiorespiratory endurance training should be the foundation of most exercise routines for adults with or at risk for CVD. This type of exercise training is the most effective way to increase CRF. Elements of an exercise prescription for increasing CRF are presented in table 6.1. The relative training intensity may vary between 40% and 80% of maximal heart rate reserve (HRR) or metabolic reserve (V.O2R). Initially, programs should focus on the lower part of the intensity range, with progression to higher intensities as patients adapt to the program.7 RPE (e.g., Borg Scale of Perceived Exertion 6-20; Borg CR10 Scale; Omni Picture System of Perceived Exertion) are considered adjunctive to HR monitoring, but they may become more important as a subjective intensity guide as patients gain experience with exercise training and learn how to use the scale. Exercise training duration varies as a function of the overall energy expenditure goals of the patient. A minimum of 20 continuous minutes of exercise per session is commonly recommended within structured programs, although some patients may follow an intermittent (i.e., interval) exercise regimen. Some patients may need to accumulate shorter bouts (e.g., multiple 10 min bouts) throughout the day due to comorbidities, symptoms such as claudication or musculoskeletal discomfort, or lifestyle factors. Ideally, patients should be active most days of the week,1-7,9 but structured programs are often designed with a frequency of two to four sessions per week.
Once the initial exercise prescription is established, patients should progress gradually toward predefined or redefined program goals. There is no set format with respect to progression because many factors, including fitness level, motivation, and orthopedic limitations, influence the rate at which a patient may progress. In general, it is prudent to change one component and provide some time (a minimum of one exercise session) to assess the adaptation to the new level before progressing further. When time permits, increases in duration and frequency should precede increases in intensity. Modest increases in intensity, when appropriate, are likely to be tolerated and should be based on the observations of the staff and subjective responses of the patient, provided that the changes remain within the limits specified in the most recent evaluation.
A guiding principle should be progression of the total volume or dose of exercise such that the patient achieves desired energy expenditure thresholds within a three- to six-month period. Therefore, given that most patients' participation in CR lasts no longer than three months, it is important to educate and encourage patients to continue exercising even after CR participation has ended. The most appropriate volume of exercise depends on the individual CVD risk profile, training goals, and comorbidities (i.e., diabetes, hypertension, obesity, arthritis). An accumulating body of evidence has affirmed a dose-response relationship between the volume of PA and health outcomes.1,3,6-8 Whether exercise has a role in reversing coronary artery disease is an issue that remains controversial; however, thresholds of approximately 1,500 and 2,200 kcal/week are associated with stability and regression of coronary artery lesions, respectively.18 Notably, multiple studies document that energy expenditure in structured CR does not typically meet either of these thresholds.11-14 Therefore, patients will likely need to engage in PA outside of the structured program to achieve the optimal levels of energy expenditure.
Few studies have supported the efficacy of structured exercise training as a singular strategy to normalize body weight and body composition in patients with CVD. This underscores the importance of multiple behavioral strategies in weight reduction programming for overweight patients. Studies show that achieving weight loss goals requires a simultaneous change in dietary habits in addition to greater physical activity patterns. The volume or dose of exercise associated with the typical CR training session may be a limiting factor, and there is only a 1 to 2 kg weight loss during CR participation. It is likely part of the explanation for a low amount of weight loss during CR is due to a lack of focus on helping patients lose weight. As mentioned previously, numerous studies have shown the weekly dose to be inadequate for weight or fat reduction. As an example, a typical exercise session for an outpatient with a peak functional capacity of 7 METs might be 30 min at a heart rate that would equate with about 4 METs. The following formula provides a method to estimate the caloric costs of the exercise session:
Calories/min = [METs × body weight in kg × 3.5] / 200
It should be noted that the 4 MET value in this example includes the resting energy expenditure component (1 MET). Therefore, the net caloric cost of the exercise would be based on only 3 METs. If the hypothetical patient in this example weighed 100 kg (220 lb) and exercised 3 days per week for 30 min, the net caloric expenditure would be approximately 480 kcal/week (5.3 kcal/min × 30 min × 3 days/week). Although patients can clearly improve exercise tolerance with this regimen, the estimated caloric expenditure falls well short of contemporary recommendations for PA and in most cases would not be effective for weight or fat loss.15 For example, 40 min sessions, five times per week, would result in an expenditure of approximately 1,060 kcal per week. Again, this calculation highlights the importance of increasing PA outside of the structured or in-hospital program. Thus, adjustments must be made about frequency and duration of exercise to allow patients to achieve greater energy expenditures to enhance program outcomes. However, these adjustments must be with the caveat that although it is prudent to increase exercise volume progressively, staff must carefully consider the risk that a higher-volume program may lead to higher dropout rates. Therefore, overweight patients must be educated about the need to develop and maintain fitness as the core of their exercise regimen, with the additional volume of PA facilitating weight loss and other goals. Finally, as CRF improves, patients are able to exercise at a higher metabolic rate (more kcal/min) at a given relative intensity (% maximal HRR). This adjustment allows patients to accumulate a greater caloric deficit over time.
Example of standing orders to initiate outpatient cardiac rehabilitation
Appendix A: Example of Standing Orders to Initiate Outpatient CR
- Initiate monitored exercise program per outpatient CR policies and procedures.
- Determine target heart rate (THR) via sign- or symptom-limited graded exercise testing (GXT) or sign- or symptom-limited responses to submaximal exercise.
- Begin with a training duration of up to 30 min to tolerance, one to five times a week.
- Gradually increase duration of training exercise if patient cardiovascular and physiological responses are within normal limits.
- Observe participant for signs of exercise intolerance and adapt or terminate exercise as indicated in policies and procedures.
- Assess lipid profile approximately six weeks postevent.
- Administer nitroglycerin 0.3 or 0.4 mg sublingually every 5 minutes × 3 as needed for angina discomfort or ischemic symptoms.
- Provide regular, periodic progress reports to the referring physician. Provide copies of reports to other physicians as needed.
- Initiate patient education and counseling sessions as patient needs indicate.
- Consult patient's personal physician or CR supervising physician for any necessary orders.
- Consult with the CR dietitian to provide individualized nutrition education for each participant.
- Enter the patient into a non-ECG-monitored maintenance program upon completion of early outpatient CR program.
__________________________________________________________________________________________
Physician's signature
___________________________________________
Date
From American Association of Cardiovascular and Pulmonary Rehabilitation, Guidelines for Cardiac Rehabilitation Programs, 6th ed.
(Champaign, IL: Human Kinetics, 2021).
Appendix B: Example of Outpatient CR Emergency Standing Orders*
Table of Contents
Protocols for Urgent Situations and Emergency Interventions in the Cardiac Rehabilitation Area
I. Cardiopulmonary arrest
II. Angina pectoris
III. Hypoglycemia
IV. Hyperglycemia
V. Hypotension
VI. Hypertension
VII. Dysrhythmias
VIII. Dyspnea
IX. Cerebrovascular accident
X. Placement of intravenous line
XI. Patient transportation
I. Cardiopulmonary Arrest
A. Identify responsiveness and determine if breathing is absent or abnormal (gasping).
B. Call out for help/activate emergency medical system (EMS).
- Call out for help from coworker. If no one responds and if no other staff member is available to assist, go to the nearest phone and activate EMS. (Emergency numbers with specific scripted instructions are posted at each phone.) Get defibrillator/automated external defibrillator (AED). If no pulse, attach defibrillator/AED and shock if indicated. Begin cardiopulmonary resuscitation (CPR) with compressions.
- If a second responder is available to assist, that person should activate EMS and then get the defibrillator/AED while the first responder stays with the patient to begin compressions.
- Staff will meet the EMS team at the appropriate entrance and direct them to the patient.
First Responder
- Determine responsiveness and absent or abnormal breathing.
- Send someone to activate EMS and get defibrillator/AED.
- If pulseless, begin chest compressions at a depth of at least 2 in. and a rate of at least 100 compressions/min until defibrillator/AED arrives. Allow for complete chest recoil, minimize interruptions to
Second Responder
- After activating EMS, take cart with defibrillator/AED to the patient. Place defibrillator pads or AED on patient and assess cardiac rhythm.
- Shock if indicated, resume compressions. Follow appropriate algorithm according to ACLS guidelines.
Third Responder (if Available)
- Direct remaining patients to another area.
- Direct and control incoming emergency response team and patients.
- Obtain extra supplies and equipment as needed.
- Act as the recorder of events until EMS arrives.
- Prepare records to be sent with patient to the emergency department if needed.
- Notify patient physician/cardiologist and family.
Emergency in Other Locations
7. Protocols should be developed for emergencies occurring in locations other than the cardiac rehabilitation gym including but not limited to:
- Locker room/restrooms
- Lobby/waiting area
- Patient education area
- Parking lots
II. Angina Pectoris
A. If a patient develops unstable angina while in the exercise area, the patient should immediately discontinue exercise and sit or lie down. Note the exercise workload, HR, and BP at which the symptoms occurred.
B. The following protocol should be followed by the CR staff:
- Check pulse, BP, cardiac rhythm (attach telemetry monitor if not already monitored), and oxygen saturation.
- Rate angina on a scale of 1 to 10.
- If no relief with 1 to 3 min of rest, give 1 nitroglycerine (NTG) 0.4 mg SL or spray.
- Obtain 12-lead ECG and call supervising physician.
C. If pain is relieved:
- If this angina is of new onset, the patient should be evaluated by the supervising physician. The primary care physician should be notified of the results of the evaluation and recommended treatment, if any.
- If the patient experiences chronic stable angina, exercise intensity should be decreased or halted until the angina is relieved. Patient may resume exercise at a lower workload dependent on the clinical judgment of the medical director and professional staff.
OR
The patient can be discharged but should be instructed to report any increase in frequency or severity of angina to their physician.
D. If pain is not relieved:
- Monitor pulse, BP, cardiac rhythm, and oxygen saturation closely.
- Place on oxygen at 2 to 4 L per nasal prongs if oxygen saturation is <94%.
- Patient to chew aspirin 160 to 325 mg.
- Repeat NTG 0.4 mg SL or spray every 5 min for unrelieved angina symptoms.
- The supervising physician will evaluate and determine the course of action.
III. Hypoglycemia
A. If patient displays any symptoms of hypoglycemia:
- Obtain finger-stick blood glucose level.
- If BG results are
- Retest BG in 15 min. If BG is not >90 mg/dL, repeat 15 g CHO and recheck BG in 15 min.
- If patient is uncooperative or unconscious, contact supervising physician, give glucose gel or establish IV access and give 50 cc (1 amp) 50% dextrose solution. Arrange for transport to ED.
IV. Hyperglycemia
A. A participant with a BG >300 mg/dL should not exercise unless the patient's referring physician and the program medical director give their consent.
B. Frequency of BG checks should be determined according to the patient profile and ITP.
C. BG evaluations may be performed by rehabilitation staff or the patient according to the ITP.
D. The CR staff may request a blood glucose evaluation on any patient based on suspected signs and symptoms of hyperglycemia (nausea, flushing, polyuria, polydipsia, fruity breath, tachypnea).
V. Hypotension
A. Remove the patient from the exercise area if possible.
B. Place patient in a supine position. Consider elevating legs or placing in Trendelenburg position.
C. Attach a telemetry monitor if not already monitored.
D. Check BP, pulse, cardiac rhythm, and oxygen saturation.
E. If no response to the position change, call the supervising physician. If the patient condition continues to deteriorate or becomes progressively symptomatic, or if BP continues to drop, start an IV of normal saline at 100 mL/h and arrange for transport to the ED. After evaluation and treatment of the patient, the supervising physician should notify the patient's primary care physician of the hypotensive episode and discuss any further treatment if necessary.
F. If patient responds to the supine position, keep supine until SBP is >100, then gradually assist to sitting position. Continue to monitor BP, pulse, and rhythm. Encourage fluids. Notify the patient's primary physician of the episode.
VI. Hypertension
A. Check every patient's BP before exercise and compare with previous recordings.
B. If the SBP reading is >170 mm Hg or the diastolic reading is >100 mm Hg, have the patient sit and recheck the BP in 5 min.
C. If the BP remains elevated, do not have patient exercise. Notify the primary care physician or supervising physician to evaluate and determine course of action.
D. Patients may exercise with elevated BP if directed by the primary care physician and medical director.
E. Investigate whether patient is complying with medications and sodium restrictions.
VII. Dysrhythmias
Premature Ventricular Contractions (PVCs)
A. Observe for the following:
- Frequency
- Whether multifocal or unifocal
- Pairs or runs, sustained or paroxysmal
- Associated signs or symptoms
- Palpate pulse to evaluate for peripheral perfusion
B. Document any new arrhythmias or increase in severity with a rhythm strip and make notation on chart. Notify supervising physician and referring physician, where appropriate, to discuss treatment.
C. Discontinue exercise if PVCs become symptomatic and check pulse, BP, and oxygen saturation. Provide oxygen at 2 to 4 L if hypoxemic, and obtain IV access if directed by a physician.
D. Notify the supervising physician for evaluation and treatment.
Bradycardia
A. If patient develops symptomatic bradycardia, stop exercise.
B. Monitor HR and rhythm, BP, and oximetry. Provide oxygen at 2 to 4 L if hypoxemic. Obtain 12-lead ECG if available.
C. Assess for symptoms of instability or altered mental status, ischemic chest discomfort, HF, or hypotension and notify supervising physician for evaluation and treatment. Notify the supervising physician and if available, obtain IV access, and prepare to administer atropine or external pacing per ACLS guidelines.
D. Prepare for transfer to ED.
Tachycardia
A. If patient develops a new wide or narrow complex tachycardia, stop exercise.
B. Monitor HR and rhythm, BP, and oximetry. Provide oxygen at 2 to 4 L if hypoxemic. Obtain 12-lead ECG if available.
C. Assess for symptoms of instability or altered mental status, ischemic chest discomfort, HF, or hypotension, and notify supervising physician for evaluation and treatment. If directed by a physician, obtain IV access and prepare for synchronized cardioversion. If stable, may utilize vagal maneuvers or antiarrhythmic agents per ACLS guidelines.
D. Prepare for transfer to ED.
VIII. Dyspnea
A. If patient develops acute dyspnea, stop exercise and have patient sit down.
B. Monitor heart rate and rhythm, BP, respiratory rate, lung sounds, and oximetry. Provide oxygen at 2 to 4 L for oxygen saturation <94%.
C. If patient has a metered-dose inhaler, it may be administered as prescribed.
D. If condition deteriorates, notify supervising physician to evaluate for treatment options and possible transfer to ED.
E. If condition improves, notify primary care physician for further recommendations.
IX. Cerebrovascular Accident
A. If patient develops signs and symptoms of a stroke such as sudden arm or leg weakness, confusion, trouble speaking, dizziness, loss of balance or coordination, severe headache, or facial droop, immediately evaluate with rapid out-of-hospital stroke assessment.
B. If stroke is suspected, initiate EMS for immediate transport to a stroke facility.
C. Establish time of last known neurological baseline.
D. Maintain airway, breathing, and circulation.
E. Provide supplemental oxygen if hypoxemic or if oxygen saturation is unknown.
F. Check blood glucose.
G. Alert receiving hospital when patient is in transport.
X. Placement of IV Line
Purpose: To provide immediate access to administer emergency medication and IV fluids.
A. An attempt will be made to notify the supervising physician.
B. Place a saline lock in participant when one or more of the following apply:
- Angina pectoris protocol has been followed and chest pain persists.
- ECG, vital signs or participant appears to be clinically unstable or symptomatic.
- Physician directs the placement of IV line.
XI. Patient Transportation
Staff will meet and direct ambulance personnel to the patient treatment area.
Staff will prepare medical records to be sent with the patient as needed.
Staff will alert the emergency department of the patient transfer.
Cardiac Rehabilitation Department Emergency Procedures and Standing Orders Were Reviewed and Approved
___________________________________________
Physician's name
___________________________________________
Signature
___________________________________________
Date of most recent review
*Appendix B should be used only as an example of standing orders that might be considered and adopted for use in freestanding outpatient or community-based programs.
From American Association of Cardiovascular and Pulmonary Rehabilitation, Guidelines for Cardiac Rehabilitation Programs, 6th ed.
(Champaign, IL: Human Kinetics, 2021).
What are cardiac dysrhythmias?
By Alison L. Bailey, Alexis L. Beatty, Brian Carlin, Dennis J. Kerrigan, Steven J. Keteyian, Kirstine Laerum Sibilitz, Karen Lui, Ryan Mays, Jonathan Powell, Ray W. Squires, Diane J. Treat-Jacobson
Cardiac dysrhythmias are abnormalities in heart rhythm. They are also known as arrhythmias or irregular rhythms. Many CR participants have a history of cardiac dysrhythmias, and some experience dysrhythmias during CR participation.1-3 Symptoms from dysrhythmias may or may not be present and vary from patient to patient. The effects of dysrhythmias can range from generally benign to potentially harmful. Most studies report a cardiac arrest rate of approximately 1/100,000 patient-hours of CR participation.4-7 Although it is rare for dysrhythmias to have life-threatening consequences during exercise in CR programs, it remains important to recognize dysrhythmias and their features.
Bottom Line
Cardiac dysrhythmias are common in CR participants. Life-threatening consequences of cardiac dysrhythmias are rare during exercise in CR programs.
The following are commonly encountered dysrhythmias and symptoms:
Cardiac Dysrhythmias in CR
Generally Benign
- Premature atrial complexes (PACs)
- Isolated premature ventricular complexes (PVCs)
- AF or atrial flutter with controlled ventricular rate (8
- Paroxysmal supraventricular tachycardia (SVT)
- Mild bradycardia (50-60 bpm)
- First-degree atrioventricular (AV) block and asymptomatic type I second-degree (also known as Wenckebach) AV block
Potentially or Likely Harmful
- AF or atrial flutter with a rapid rate (≥110 bpm at rest)
- Symptomatic or severe bradycardia (HR <50)
- Symptomatic or advanced AV block (type II second-degree AV block or complete heart block)
- Ventricular tachycardia
- Ventricular fibrillation
Symptoms Associated With Cardiac Dysrhythmias
Stable Symptoms
- Palpitations
- Dizziness or lightheadedness
- Shortness of breath
- Chest pain or discomfort
Nonspecific or Associated Symptoms
- Weakness or fatigue
- Sweating
- Blurred vision
- Nausea
- Anxiety
- Edema
Unstable Symptoms
- Hypotension
- Near-syncope or loss of consciousness
- HF
- Unstable angina or MI
- Cardiac arrest
Exercise induces many physiologic effects, which can have both direct and indirect effects on cardiac electrophysiology. Exercise intensity can be related to the occurrence of dysrhythmias. Some dysrhythmias diminish or disappear with increasing exercise intensity; others increase or appear with increasing exercise intensity; and still others have no observable relationship to exercise intensity. Factors that can contribute to dysrhythmias during exercise include autonomic nervous system activity, ischemia, genetic abnormalities, structural heart disease, medications with proarrhythmic side effects, electrolyte imbalance, dehydration, and certain environmental factors.
Guideline 10.7 Dysrhythmia Exercise Prescription
For patients with known dysrhythmias, the exercise prescription should be tailored to the individual, with predetermined goals and criteria for exercise termination. Exercise should be terminated when a patient experiences a potentially harmful dysrhythmia or dysrhythmia with unstable symptoms.
Atrial Fibrillation
Light-to-moderate activities, particularly leisure-time activity and walking, are associated with a significantly lower incidence of AF in older adults.9 However, people who participate in extreme endurance training and sports activities may have an increased incidence of AF.10,11 For those diagnosed with AF, regular moderate PA is known to increase exercise capacity and control ventricular rate.12,13 In addition, exercise training increases exercise capacity and may reduce AF burden.14,15 The following information provides specific information about CR participation in patients who have AF.
AF originates in the atrium and is the most common cardiac arrhythmia. It is characterized by irregular contractions of the muscle fibers of the atria resulting in a variable HR. Risk factors associated with developing AF include PA, obesity, advanced age, HTN, HF, diabetes mellitus, CVD and valvular heart disease, left ventricular and atrial enlargement, and hyperthyroidism.43 Paradoxically, despite having few risk factors, athletes are also at increased risk for developing AF.
CR professionals will encounter these two types of patients with AF: patients who experience an initial (acute) onset (often noted during CR check-in or during exercise) and patients previously diagnosed and medically managed. Generally, AF is classified as (1) paroxysmal, (2) persistent, (3) long-standing persistent, or (4) permanent.2
AF should be considered when a patient presents with a rapid (often >110 bpm) “irregularly irregular” (no rhythmic pattern) resting HR. Patients experiencing an abrupt onset of AF may or may not report accompanying symptoms including palpitation, tachycardia, fatigue, shortness of breath, dizziness, and nausea. If AF is suspected, an ECG will confirm a diagnosis.
If new-onset AF is confirmed, the patient's physician should be consulted. Treating new-onset AF has three goals.44,50 The first goal is to mitigate symptoms by initially focusing in on reducing HR. Typical therapeutic HR reduction options include beta-adrenergic and calcium channel blocking agents and antiarrhythmic medication. The second goal is to reduce the risk for the development embolization of a blood clot (which the patient is at risk of developing due to atrial blood stagnation) through anticoagulation therapy. The third goal is to manage the patient's cardiovascular risk factors, which for overweight or obese patients is recommended to include weight loss and risk factor modification.50
Safety and rates of adverse event of exercise in patients have not been well studied. No large randomized control trials of exercise training and AF have assessed safety and efficacy. Guidelines for the treatment of patients with AF do not explicitly endorse specific exercise recommendations. Exercise, however, is not contraindicated in patients with AF. Moreover, exercise is effective treatment in multiple risk factors associated with AF, such as physical inactivity, HTN, diabetes mellitus, and obesity. Therefore, asymptomatic patients with AF who have received medical clearance should be encouraged to participate in an exercise program.
However, AF can profoundly impact the physiologic response to exercise training.45 In particular, the rapid, irregular contraction of the atrium results in reduced ventricular output. To compensate for the reduced cardiac output there is a commensurate increase in the rate and irregularity of ventricular contraction. Despite the negative impact of AF, exercise training studies have demonstrated improvements in functional capacity, health status, and quality of life.46
The special consideration regarding exercise testing and prescription for patients with AF have been detailed elsewhere.3 The following section is a brief review of special considerations regarding exercise testing and prescription for CR participants with AF.
Exercise Testing
As with all patients entering CR, undergoing a symptom-limited exercise tolerance test prior to initiating an exercise training program is optimal but not required. An exercise test is useful to assess for myocardial ischemia, evaluate chronotropic response, identify signs and symptoms, quantify functional capacity, and establish some general parameters for exercise training intensity.
Exercise Prescription for Patients With AF
Currently, no specific recommendations exist regarding exercise training for the treatment of AF. Studies of exercise training in patients with AF have employed a variety of protocols. Components of any exercise prescription include frequency, intensity, duration, modality, progression, and total volume. The exercise prescription for patients with AF should be individualized. A meta-analysis of exercise training studies involving people with AF recommends that a training regimen should include three or more sessions per week of a combination of moderate-intensity aerobic activity and resistance training. Session duration should be approximately 60 minutes, including adequate warm-up and cool-down.
By definition, the HR for a person with AF is irregular. Therefore, use of HR exclusively to assess exercise intensity is problematic. For aerobic training, in lieu of HR, use of RPE scale is an effective means to assess exercise intensity. A rating of 11 to 14 (on the Borg 6-20 scale) is typically associated with a moderate intensity that is approximately 70% to 85% of peak exercise capacity. Notably, very few studies have focused on the safety and efficacy of high-intensity aerobic training in patients with AF.
For overweight patients with AF, weight loss is recommended.47,50 To facilitate weight loss, orienting the exercise prescription to maximize caloric expenditure is indicated. High caloric exercise training (e.g., treadmill walking at a moderate intensity for an extended duration) in CR is well tolerated and an effective strategy to promote weight loss and improve multiple cardiovascular risk factors.48
No specific guidelines exist for resistance training for patients with AF. Given the lack of recommendations, using professional discretion is necessary when providing guidance regarding resistance training. Following the resistance training recommendations for other, non-AF CR participants is advisable. General recommendations for resistance training are found in chapter 6.
Considerations for the prescription of exercise and physical activity
By Jonathan Myers
Guideline 6.1 Considerations for the Prescription of Exercise and Physical Activity
When developing an exercise prescription, consider the following factors:
Safety Factors
- Clinical history
- Risks associated with CVD progression or instability
- Ischemic and angina thresholds
- Cognitive or psychological impairment
Associated Factors
- Vocational or avocational requirements
- Orthopedic limitations
- Previous and current activities
- Personal health and fitness goals
An important initial consideration in exercise planning is safety. Safety considerations apply to both structured exercise training and leisure-time PA. While most patients can engage in exercise without incurring undue risks, appropriate risk stratification should be performed. Guideline 6.1 provides key variables to consider when developing an exercise prescription. Safety and risk stratification are discussed in detail in chapters 4 and 5. Recommendations for supervision and ECG monitoring can be found in chapter 5. Later in this chapter, tables 6.1 and 6.2 present basic principles of exercise prescription. A model for risk stratification for cardiovascular events is outlined in the sidebar Stratification of Risk for Cardiac Events During Exercise Participation in chapter 5. After risk stratification, recommendations for supervision, ECG, monitoring and prescribed intensity and duration of exercise training can be made.
Comprehensive, evidence-based recommendations for structured exercise training in CR are available from several prominent organizations1,3,8 and are only summarized here. A comprehensive exercise program includes cardiorespiratory, musculoskeletal, and flexibility components. Specific elements for each component are summarized in the tables in this chapter and include guidelines for intensity, duration, frequency, and type of exercise for training. Each of the elements should be prescribed relative to one another and in a way that effectively addresses predefined training goals (e.g., increased aerobic or musculoskeletal fitness, weight reduction, control of blood glucose, or resumption of occupation).
Cardiorespiratory Endurance Training
Cardiorespiratory endurance training should be the foundation of most exercise routines for adults with or at risk for CVD. This type of exercise training is the most effective way to increase CRF. Elements of an exercise prescription for increasing CRF are presented in table 6.1. The relative training intensity may vary between 40% and 80% of maximal heart rate reserve (HRR) or metabolic reserve (V.O2R). Initially, programs should focus on the lower part of the intensity range, with progression to higher intensities as patients adapt to the program.7 RPE (e.g., Borg Scale of Perceived Exertion 6-20; Borg CR10 Scale; Omni Picture System of Perceived Exertion) are considered adjunctive to HR monitoring, but they may become more important as a subjective intensity guide as patients gain experience with exercise training and learn how to use the scale. Exercise training duration varies as a function of the overall energy expenditure goals of the patient. A minimum of 20 continuous minutes of exercise per session is commonly recommended within structured programs, although some patients may follow an intermittent (i.e., interval) exercise regimen. Some patients may need to accumulate shorter bouts (e.g., multiple 10 min bouts) throughout the day due to comorbidities, symptoms such as claudication or musculoskeletal discomfort, or lifestyle factors. Ideally, patients should be active most days of the week,1-7,9 but structured programs are often designed with a frequency of two to four sessions per week.
Once the initial exercise prescription is established, patients should progress gradually toward predefined or redefined program goals. There is no set format with respect to progression because many factors, including fitness level, motivation, and orthopedic limitations, influence the rate at which a patient may progress. In general, it is prudent to change one component and provide some time (a minimum of one exercise session) to assess the adaptation to the new level before progressing further. When time permits, increases in duration and frequency should precede increases in intensity. Modest increases in intensity, when appropriate, are likely to be tolerated and should be based on the observations of the staff and subjective responses of the patient, provided that the changes remain within the limits specified in the most recent evaluation.
A guiding principle should be progression of the total volume or dose of exercise such that the patient achieves desired energy expenditure thresholds within a three- to six-month period. Therefore, given that most patients' participation in CR lasts no longer than three months, it is important to educate and encourage patients to continue exercising even after CR participation has ended. The most appropriate volume of exercise depends on the individual CVD risk profile, training goals, and comorbidities (i.e., diabetes, hypertension, obesity, arthritis). An accumulating body of evidence has affirmed a dose-response relationship between the volume of PA and health outcomes.1,3,6-8 Whether exercise has a role in reversing coronary artery disease is an issue that remains controversial; however, thresholds of approximately 1,500 and 2,200 kcal/week are associated with stability and regression of coronary artery lesions, respectively.18 Notably, multiple studies document that energy expenditure in structured CR does not typically meet either of these thresholds.11-14 Therefore, patients will likely need to engage in PA outside of the structured program to achieve the optimal levels of energy expenditure.
Few studies have supported the efficacy of structured exercise training as a singular strategy to normalize body weight and body composition in patients with CVD. This underscores the importance of multiple behavioral strategies in weight reduction programming for overweight patients. Studies show that achieving weight loss goals requires a simultaneous change in dietary habits in addition to greater physical activity patterns. The volume or dose of exercise associated with the typical CR training session may be a limiting factor, and there is only a 1 to 2 kg weight loss during CR participation. It is likely part of the explanation for a low amount of weight loss during CR is due to a lack of focus on helping patients lose weight. As mentioned previously, numerous studies have shown the weekly dose to be inadequate for weight or fat reduction. As an example, a typical exercise session for an outpatient with a peak functional capacity of 7 METs might be 30 min at a heart rate that would equate with about 4 METs. The following formula provides a method to estimate the caloric costs of the exercise session:
Calories/min = [METs × body weight in kg × 3.5] / 200
It should be noted that the 4 MET value in this example includes the resting energy expenditure component (1 MET). Therefore, the net caloric cost of the exercise would be based on only 3 METs. If the hypothetical patient in this example weighed 100 kg (220 lb) and exercised 3 days per week for 30 min, the net caloric expenditure would be approximately 480 kcal/week (5.3 kcal/min × 30 min × 3 days/week). Although patients can clearly improve exercise tolerance with this regimen, the estimated caloric expenditure falls well short of contemporary recommendations for PA and in most cases would not be effective for weight or fat loss.15 For example, 40 min sessions, five times per week, would result in an expenditure of approximately 1,060 kcal per week. Again, this calculation highlights the importance of increasing PA outside of the structured or in-hospital program. Thus, adjustments must be made about frequency and duration of exercise to allow patients to achieve greater energy expenditures to enhance program outcomes. However, these adjustments must be with the caveat that although it is prudent to increase exercise volume progressively, staff must carefully consider the risk that a higher-volume program may lead to higher dropout rates. Therefore, overweight patients must be educated about the need to develop and maintain fitness as the core of their exercise regimen, with the additional volume of PA facilitating weight loss and other goals. Finally, as CRF improves, patients are able to exercise at a higher metabolic rate (more kcal/min) at a given relative intensity (% maximal HRR). This adjustment allows patients to accumulate a greater caloric deficit over time.
Example of standing orders to initiate outpatient cardiac rehabilitation
Appendix A: Example of Standing Orders to Initiate Outpatient CR
- Initiate monitored exercise program per outpatient CR policies and procedures.
- Determine target heart rate (THR) via sign- or symptom-limited graded exercise testing (GXT) or sign- or symptom-limited responses to submaximal exercise.
- Begin with a training duration of up to 30 min to tolerance, one to five times a week.
- Gradually increase duration of training exercise if patient cardiovascular and physiological responses are within normal limits.
- Observe participant for signs of exercise intolerance and adapt or terminate exercise as indicated in policies and procedures.
- Assess lipid profile approximately six weeks postevent.
- Administer nitroglycerin 0.3 or 0.4 mg sublingually every 5 minutes × 3 as needed for angina discomfort or ischemic symptoms.
- Provide regular, periodic progress reports to the referring physician. Provide copies of reports to other physicians as needed.
- Initiate patient education and counseling sessions as patient needs indicate.
- Consult patient's personal physician or CR supervising physician for any necessary orders.
- Consult with the CR dietitian to provide individualized nutrition education for each participant.
- Enter the patient into a non-ECG-monitored maintenance program upon completion of early outpatient CR program.
__________________________________________________________________________________________
Physician's signature
___________________________________________
Date
From American Association of Cardiovascular and Pulmonary Rehabilitation, Guidelines for Cardiac Rehabilitation Programs, 6th ed.
(Champaign, IL: Human Kinetics, 2021).
Appendix B: Example of Outpatient CR Emergency Standing Orders*
Table of Contents
Protocols for Urgent Situations and Emergency Interventions in the Cardiac Rehabilitation Area
I. Cardiopulmonary arrest
II. Angina pectoris
III. Hypoglycemia
IV. Hyperglycemia
V. Hypotension
VI. Hypertension
VII. Dysrhythmias
VIII. Dyspnea
IX. Cerebrovascular accident
X. Placement of intravenous line
XI. Patient transportation
I. Cardiopulmonary Arrest
A. Identify responsiveness and determine if breathing is absent or abnormal (gasping).
B. Call out for help/activate emergency medical system (EMS).
- Call out for help from coworker. If no one responds and if no other staff member is available to assist, go to the nearest phone and activate EMS. (Emergency numbers with specific scripted instructions are posted at each phone.) Get defibrillator/automated external defibrillator (AED). If no pulse, attach defibrillator/AED and shock if indicated. Begin cardiopulmonary resuscitation (CPR) with compressions.
- If a second responder is available to assist, that person should activate EMS and then get the defibrillator/AED while the first responder stays with the patient to begin compressions.
- Staff will meet the EMS team at the appropriate entrance and direct them to the patient.
First Responder
- Determine responsiveness and absent or abnormal breathing.
- Send someone to activate EMS and get defibrillator/AED.
- If pulseless, begin chest compressions at a depth of at least 2 in. and a rate of at least 100 compressions/min until defibrillator/AED arrives. Allow for complete chest recoil, minimize interruptions to
Second Responder
- After activating EMS, take cart with defibrillator/AED to the patient. Place defibrillator pads or AED on patient and assess cardiac rhythm.
- Shock if indicated, resume compressions. Follow appropriate algorithm according to ACLS guidelines.
Third Responder (if Available)
- Direct remaining patients to another area.
- Direct and control incoming emergency response team and patients.
- Obtain extra supplies and equipment as needed.
- Act as the recorder of events until EMS arrives.
- Prepare records to be sent with patient to the emergency department if needed.
- Notify patient physician/cardiologist and family.
Emergency in Other Locations
7. Protocols should be developed for emergencies occurring in locations other than the cardiac rehabilitation gym including but not limited to:
- Locker room/restrooms
- Lobby/waiting area
- Patient education area
- Parking lots
II. Angina Pectoris
A. If a patient develops unstable angina while in the exercise area, the patient should immediately discontinue exercise and sit or lie down. Note the exercise workload, HR, and BP at which the symptoms occurred.
B. The following protocol should be followed by the CR staff:
- Check pulse, BP, cardiac rhythm (attach telemetry monitor if not already monitored), and oxygen saturation.
- Rate angina on a scale of 1 to 10.
- If no relief with 1 to 3 min of rest, give 1 nitroglycerine (NTG) 0.4 mg SL or spray.
- Obtain 12-lead ECG and call supervising physician.
C. If pain is relieved:
- If this angina is of new onset, the patient should be evaluated by the supervising physician. The primary care physician should be notified of the results of the evaluation and recommended treatment, if any.
- If the patient experiences chronic stable angina, exercise intensity should be decreased or halted until the angina is relieved. Patient may resume exercise at a lower workload dependent on the clinical judgment of the medical director and professional staff.
OR
The patient can be discharged but should be instructed to report any increase in frequency or severity of angina to their physician.
D. If pain is not relieved:
- Monitor pulse, BP, cardiac rhythm, and oxygen saturation closely.
- Place on oxygen at 2 to 4 L per nasal prongs if oxygen saturation is <94%.
- Patient to chew aspirin 160 to 325 mg.
- Repeat NTG 0.4 mg SL or spray every 5 min for unrelieved angina symptoms.
- The supervising physician will evaluate and determine the course of action.
III. Hypoglycemia
A. If patient displays any symptoms of hypoglycemia:
- Obtain finger-stick blood glucose level.
- If BG results are
- Retest BG in 15 min. If BG is not >90 mg/dL, repeat 15 g CHO and recheck BG in 15 min.
- If patient is uncooperative or unconscious, contact supervising physician, give glucose gel or establish IV access and give 50 cc (1 amp) 50% dextrose solution. Arrange for transport to ED.
IV. Hyperglycemia
A. A participant with a BG >300 mg/dL should not exercise unless the patient's referring physician and the program medical director give their consent.
B. Frequency of BG checks should be determined according to the patient profile and ITP.
C. BG evaluations may be performed by rehabilitation staff or the patient according to the ITP.
D. The CR staff may request a blood glucose evaluation on any patient based on suspected signs and symptoms of hyperglycemia (nausea, flushing, polyuria, polydipsia, fruity breath, tachypnea).
V. Hypotension
A. Remove the patient from the exercise area if possible.
B. Place patient in a supine position. Consider elevating legs or placing in Trendelenburg position.
C. Attach a telemetry monitor if not already monitored.
D. Check BP, pulse, cardiac rhythm, and oxygen saturation.
E. If no response to the position change, call the supervising physician. If the patient condition continues to deteriorate or becomes progressively symptomatic, or if BP continues to drop, start an IV of normal saline at 100 mL/h and arrange for transport to the ED. After evaluation and treatment of the patient, the supervising physician should notify the patient's primary care physician of the hypotensive episode and discuss any further treatment if necessary.
F. If patient responds to the supine position, keep supine until SBP is >100, then gradually assist to sitting position. Continue to monitor BP, pulse, and rhythm. Encourage fluids. Notify the patient's primary physician of the episode.
VI. Hypertension
A. Check every patient's BP before exercise and compare with previous recordings.
B. If the SBP reading is >170 mm Hg or the diastolic reading is >100 mm Hg, have the patient sit and recheck the BP in 5 min.
C. If the BP remains elevated, do not have patient exercise. Notify the primary care physician or supervising physician to evaluate and determine course of action.
D. Patients may exercise with elevated BP if directed by the primary care physician and medical director.
E. Investigate whether patient is complying with medications and sodium restrictions.
VII. Dysrhythmias
Premature Ventricular Contractions (PVCs)
A. Observe for the following:
- Frequency
- Whether multifocal or unifocal
- Pairs or runs, sustained or paroxysmal
- Associated signs or symptoms
- Palpate pulse to evaluate for peripheral perfusion
B. Document any new arrhythmias or increase in severity with a rhythm strip and make notation on chart. Notify supervising physician and referring physician, where appropriate, to discuss treatment.
C. Discontinue exercise if PVCs become symptomatic and check pulse, BP, and oxygen saturation. Provide oxygen at 2 to 4 L if hypoxemic, and obtain IV access if directed by a physician.
D. Notify the supervising physician for evaluation and treatment.
Bradycardia
A. If patient develops symptomatic bradycardia, stop exercise.
B. Monitor HR and rhythm, BP, and oximetry. Provide oxygen at 2 to 4 L if hypoxemic. Obtain 12-lead ECG if available.
C. Assess for symptoms of instability or altered mental status, ischemic chest discomfort, HF, or hypotension and notify supervising physician for evaluation and treatment. Notify the supervising physician and if available, obtain IV access, and prepare to administer atropine or external pacing per ACLS guidelines.
D. Prepare for transfer to ED.
Tachycardia
A. If patient develops a new wide or narrow complex tachycardia, stop exercise.
B. Monitor HR and rhythm, BP, and oximetry. Provide oxygen at 2 to 4 L if hypoxemic. Obtain 12-lead ECG if available.
C. Assess for symptoms of instability or altered mental status, ischemic chest discomfort, HF, or hypotension, and notify supervising physician for evaluation and treatment. If directed by a physician, obtain IV access and prepare for synchronized cardioversion. If stable, may utilize vagal maneuvers or antiarrhythmic agents per ACLS guidelines.
D. Prepare for transfer to ED.
VIII. Dyspnea
A. If patient develops acute dyspnea, stop exercise and have patient sit down.
B. Monitor heart rate and rhythm, BP, respiratory rate, lung sounds, and oximetry. Provide oxygen at 2 to 4 L for oxygen saturation <94%.
C. If patient has a metered-dose inhaler, it may be administered as prescribed.
D. If condition deteriorates, notify supervising physician to evaluate for treatment options and possible transfer to ED.
E. If condition improves, notify primary care physician for further recommendations.
IX. Cerebrovascular Accident
A. If patient develops signs and symptoms of a stroke such as sudden arm or leg weakness, confusion, trouble speaking, dizziness, loss of balance or coordination, severe headache, or facial droop, immediately evaluate with rapid out-of-hospital stroke assessment.
B. If stroke is suspected, initiate EMS for immediate transport to a stroke facility.
C. Establish time of last known neurological baseline.
D. Maintain airway, breathing, and circulation.
E. Provide supplemental oxygen if hypoxemic or if oxygen saturation is unknown.
F. Check blood glucose.
G. Alert receiving hospital when patient is in transport.
X. Placement of IV Line
Purpose: To provide immediate access to administer emergency medication and IV fluids.
A. An attempt will be made to notify the supervising physician.
B. Place a saline lock in participant when one or more of the following apply:
- Angina pectoris protocol has been followed and chest pain persists.
- ECG, vital signs or participant appears to be clinically unstable or symptomatic.
- Physician directs the placement of IV line.
XI. Patient Transportation
Staff will meet and direct ambulance personnel to the patient treatment area.
Staff will prepare medical records to be sent with the patient as needed.
Staff will alert the emergency department of the patient transfer.
Cardiac Rehabilitation Department Emergency Procedures and Standing Orders Were Reviewed and Approved
___________________________________________
Physician's name
___________________________________________
Signature
___________________________________________
Date of most recent review
*Appendix B should be used only as an example of standing orders that might be considered and adopted for use in freestanding outpatient or community-based programs.
From American Association of Cardiovascular and Pulmonary Rehabilitation, Guidelines for Cardiac Rehabilitation Programs, 6th ed.
(Champaign, IL: Human Kinetics, 2021).
What are cardiac dysrhythmias?
By Alison L. Bailey, Alexis L. Beatty, Brian Carlin, Dennis J. Kerrigan, Steven J. Keteyian, Kirstine Laerum Sibilitz, Karen Lui, Ryan Mays, Jonathan Powell, Ray W. Squires, Diane J. Treat-Jacobson
Cardiac dysrhythmias are abnormalities in heart rhythm. They are also known as arrhythmias or irregular rhythms. Many CR participants have a history of cardiac dysrhythmias, and some experience dysrhythmias during CR participation.1-3 Symptoms from dysrhythmias may or may not be present and vary from patient to patient. The effects of dysrhythmias can range from generally benign to potentially harmful. Most studies report a cardiac arrest rate of approximately 1/100,000 patient-hours of CR participation.4-7 Although it is rare for dysrhythmias to have life-threatening consequences during exercise in CR programs, it remains important to recognize dysrhythmias and their features.
Bottom Line
Cardiac dysrhythmias are common in CR participants. Life-threatening consequences of cardiac dysrhythmias are rare during exercise in CR programs.
The following are commonly encountered dysrhythmias and symptoms:
Cardiac Dysrhythmias in CR
Generally Benign
- Premature atrial complexes (PACs)
- Isolated premature ventricular complexes (PVCs)
- AF or atrial flutter with controlled ventricular rate (8
- Paroxysmal supraventricular tachycardia (SVT)
- Mild bradycardia (50-60 bpm)
- First-degree atrioventricular (AV) block and asymptomatic type I second-degree (also known as Wenckebach) AV block
Potentially or Likely Harmful
- AF or atrial flutter with a rapid rate (≥110 bpm at rest)
- Symptomatic or severe bradycardia (HR <50)
- Symptomatic or advanced AV block (type II second-degree AV block or complete heart block)
- Ventricular tachycardia
- Ventricular fibrillation
Symptoms Associated With Cardiac Dysrhythmias
Stable Symptoms
- Palpitations
- Dizziness or lightheadedness
- Shortness of breath
- Chest pain or discomfort
Nonspecific or Associated Symptoms
- Weakness or fatigue
- Sweating
- Blurred vision
- Nausea
- Anxiety
- Edema
Unstable Symptoms
- Hypotension
- Near-syncope or loss of consciousness
- HF
- Unstable angina or MI
- Cardiac arrest
Exercise induces many physiologic effects, which can have both direct and indirect effects on cardiac electrophysiology. Exercise intensity can be related to the occurrence of dysrhythmias. Some dysrhythmias diminish or disappear with increasing exercise intensity; others increase or appear with increasing exercise intensity; and still others have no observable relationship to exercise intensity. Factors that can contribute to dysrhythmias during exercise include autonomic nervous system activity, ischemia, genetic abnormalities, structural heart disease, medications with proarrhythmic side effects, electrolyte imbalance, dehydration, and certain environmental factors.
Guideline 10.7 Dysrhythmia Exercise Prescription
For patients with known dysrhythmias, the exercise prescription should be tailored to the individual, with predetermined goals and criteria for exercise termination. Exercise should be terminated when a patient experiences a potentially harmful dysrhythmia or dysrhythmia with unstable symptoms.
Atrial Fibrillation
Light-to-moderate activities, particularly leisure-time activity and walking, are associated with a significantly lower incidence of AF in older adults.9 However, people who participate in extreme endurance training and sports activities may have an increased incidence of AF.10,11 For those diagnosed with AF, regular moderate PA is known to increase exercise capacity and control ventricular rate.12,13 In addition, exercise training increases exercise capacity and may reduce AF burden.14,15 The following information provides specific information about CR participation in patients who have AF.
AF originates in the atrium and is the most common cardiac arrhythmia. It is characterized by irregular contractions of the muscle fibers of the atria resulting in a variable HR. Risk factors associated with developing AF include PA, obesity, advanced age, HTN, HF, diabetes mellitus, CVD and valvular heart disease, left ventricular and atrial enlargement, and hyperthyroidism.43 Paradoxically, despite having few risk factors, athletes are also at increased risk for developing AF.
CR professionals will encounter these two types of patients with AF: patients who experience an initial (acute) onset (often noted during CR check-in or during exercise) and patients previously diagnosed and medically managed. Generally, AF is classified as (1) paroxysmal, (2) persistent, (3) long-standing persistent, or (4) permanent.2
AF should be considered when a patient presents with a rapid (often >110 bpm) “irregularly irregular” (no rhythmic pattern) resting HR. Patients experiencing an abrupt onset of AF may or may not report accompanying symptoms including palpitation, tachycardia, fatigue, shortness of breath, dizziness, and nausea. If AF is suspected, an ECG will confirm a diagnosis.
If new-onset AF is confirmed, the patient's physician should be consulted. Treating new-onset AF has three goals.44,50 The first goal is to mitigate symptoms by initially focusing in on reducing HR. Typical therapeutic HR reduction options include beta-adrenergic and calcium channel blocking agents and antiarrhythmic medication. The second goal is to reduce the risk for the development embolization of a blood clot (which the patient is at risk of developing due to atrial blood stagnation) through anticoagulation therapy. The third goal is to manage the patient's cardiovascular risk factors, which for overweight or obese patients is recommended to include weight loss and risk factor modification.50
Safety and rates of adverse event of exercise in patients have not been well studied. No large randomized control trials of exercise training and AF have assessed safety and efficacy. Guidelines for the treatment of patients with AF do not explicitly endorse specific exercise recommendations. Exercise, however, is not contraindicated in patients with AF. Moreover, exercise is effective treatment in multiple risk factors associated with AF, such as physical inactivity, HTN, diabetes mellitus, and obesity. Therefore, asymptomatic patients with AF who have received medical clearance should be encouraged to participate in an exercise program.
However, AF can profoundly impact the physiologic response to exercise training.45 In particular, the rapid, irregular contraction of the atrium results in reduced ventricular output. To compensate for the reduced cardiac output there is a commensurate increase in the rate and irregularity of ventricular contraction. Despite the negative impact of AF, exercise training studies have demonstrated improvements in functional capacity, health status, and quality of life.46
The special consideration regarding exercise testing and prescription for patients with AF have been detailed elsewhere.3 The following section is a brief review of special considerations regarding exercise testing and prescription for CR participants with AF.
Exercise Testing
As with all patients entering CR, undergoing a symptom-limited exercise tolerance test prior to initiating an exercise training program is optimal but not required. An exercise test is useful to assess for myocardial ischemia, evaluate chronotropic response, identify signs and symptoms, quantify functional capacity, and establish some general parameters for exercise training intensity.
Exercise Prescription for Patients With AF
Currently, no specific recommendations exist regarding exercise training for the treatment of AF. Studies of exercise training in patients with AF have employed a variety of protocols. Components of any exercise prescription include frequency, intensity, duration, modality, progression, and total volume. The exercise prescription for patients with AF should be individualized. A meta-analysis of exercise training studies involving people with AF recommends that a training regimen should include three or more sessions per week of a combination of moderate-intensity aerobic activity and resistance training. Session duration should be approximately 60 minutes, including adequate warm-up and cool-down.
By definition, the HR for a person with AF is irregular. Therefore, use of HR exclusively to assess exercise intensity is problematic. For aerobic training, in lieu of HR, use of RPE scale is an effective means to assess exercise intensity. A rating of 11 to 14 (on the Borg 6-20 scale) is typically associated with a moderate intensity that is approximately 70% to 85% of peak exercise capacity. Notably, very few studies have focused on the safety and efficacy of high-intensity aerobic training in patients with AF.
For overweight patients with AF, weight loss is recommended.47,50 To facilitate weight loss, orienting the exercise prescription to maximize caloric expenditure is indicated. High caloric exercise training (e.g., treadmill walking at a moderate intensity for an extended duration) in CR is well tolerated and an effective strategy to promote weight loss and improve multiple cardiovascular risk factors.48
No specific guidelines exist for resistance training for patients with AF. Given the lack of recommendations, using professional discretion is necessary when providing guidance regarding resistance training. Following the resistance training recommendations for other, non-AF CR participants is advisable. General recommendations for resistance training are found in chapter 6.
Considerations for the prescription of exercise and physical activity
By Jonathan Myers
Guideline 6.1 Considerations for the Prescription of Exercise and Physical Activity
When developing an exercise prescription, consider the following factors:
Safety Factors
- Clinical history
- Risks associated with CVD progression or instability
- Ischemic and angina thresholds
- Cognitive or psychological impairment
Associated Factors
- Vocational or avocational requirements
- Orthopedic limitations
- Previous and current activities
- Personal health and fitness goals
An important initial consideration in exercise planning is safety. Safety considerations apply to both structured exercise training and leisure-time PA. While most patients can engage in exercise without incurring undue risks, appropriate risk stratification should be performed. Guideline 6.1 provides key variables to consider when developing an exercise prescription. Safety and risk stratification are discussed in detail in chapters 4 and 5. Recommendations for supervision and ECG monitoring can be found in chapter 5. Later in this chapter, tables 6.1 and 6.2 present basic principles of exercise prescription. A model for risk stratification for cardiovascular events is outlined in the sidebar Stratification of Risk for Cardiac Events During Exercise Participation in chapter 5. After risk stratification, recommendations for supervision, ECG, monitoring and prescribed intensity and duration of exercise training can be made.
Comprehensive, evidence-based recommendations for structured exercise training in CR are available from several prominent organizations1,3,8 and are only summarized here. A comprehensive exercise program includes cardiorespiratory, musculoskeletal, and flexibility components. Specific elements for each component are summarized in the tables in this chapter and include guidelines for intensity, duration, frequency, and type of exercise for training. Each of the elements should be prescribed relative to one another and in a way that effectively addresses predefined training goals (e.g., increased aerobic or musculoskeletal fitness, weight reduction, control of blood glucose, or resumption of occupation).
Cardiorespiratory Endurance Training
Cardiorespiratory endurance training should be the foundation of most exercise routines for adults with or at risk for CVD. This type of exercise training is the most effective way to increase CRF. Elements of an exercise prescription for increasing CRF are presented in table 6.1. The relative training intensity may vary between 40% and 80% of maximal heart rate reserve (HRR) or metabolic reserve (V.O2R). Initially, programs should focus on the lower part of the intensity range, with progression to higher intensities as patients adapt to the program.7 RPE (e.g., Borg Scale of Perceived Exertion 6-20; Borg CR10 Scale; Omni Picture System of Perceived Exertion) are considered adjunctive to HR monitoring, but they may become more important as a subjective intensity guide as patients gain experience with exercise training and learn how to use the scale. Exercise training duration varies as a function of the overall energy expenditure goals of the patient. A minimum of 20 continuous minutes of exercise per session is commonly recommended within structured programs, although some patients may follow an intermittent (i.e., interval) exercise regimen. Some patients may need to accumulate shorter bouts (e.g., multiple 10 min bouts) throughout the day due to comorbidities, symptoms such as claudication or musculoskeletal discomfort, or lifestyle factors. Ideally, patients should be active most days of the week,1-7,9 but structured programs are often designed with a frequency of two to four sessions per week.
Once the initial exercise prescription is established, patients should progress gradually toward predefined or redefined program goals. There is no set format with respect to progression because many factors, including fitness level, motivation, and orthopedic limitations, influence the rate at which a patient may progress. In general, it is prudent to change one component and provide some time (a minimum of one exercise session) to assess the adaptation to the new level before progressing further. When time permits, increases in duration and frequency should precede increases in intensity. Modest increases in intensity, when appropriate, are likely to be tolerated and should be based on the observations of the staff and subjective responses of the patient, provided that the changes remain within the limits specified in the most recent evaluation.
A guiding principle should be progression of the total volume or dose of exercise such that the patient achieves desired energy expenditure thresholds within a three- to six-month period. Therefore, given that most patients' participation in CR lasts no longer than three months, it is important to educate and encourage patients to continue exercising even after CR participation has ended. The most appropriate volume of exercise depends on the individual CVD risk profile, training goals, and comorbidities (i.e., diabetes, hypertension, obesity, arthritis). An accumulating body of evidence has affirmed a dose-response relationship between the volume of PA and health outcomes.1,3,6-8 Whether exercise has a role in reversing coronary artery disease is an issue that remains controversial; however, thresholds of approximately 1,500 and 2,200 kcal/week are associated with stability and regression of coronary artery lesions, respectively.18 Notably, multiple studies document that energy expenditure in structured CR does not typically meet either of these thresholds.11-14 Therefore, patients will likely need to engage in PA outside of the structured program to achieve the optimal levels of energy expenditure.
Few studies have supported the efficacy of structured exercise training as a singular strategy to normalize body weight and body composition in patients with CVD. This underscores the importance of multiple behavioral strategies in weight reduction programming for overweight patients. Studies show that achieving weight loss goals requires a simultaneous change in dietary habits in addition to greater physical activity patterns. The volume or dose of exercise associated with the typical CR training session may be a limiting factor, and there is only a 1 to 2 kg weight loss during CR participation. It is likely part of the explanation for a low amount of weight loss during CR is due to a lack of focus on helping patients lose weight. As mentioned previously, numerous studies have shown the weekly dose to be inadequate for weight or fat reduction. As an example, a typical exercise session for an outpatient with a peak functional capacity of 7 METs might be 30 min at a heart rate that would equate with about 4 METs. The following formula provides a method to estimate the caloric costs of the exercise session:
Calories/min = [METs × body weight in kg × 3.5] / 200
It should be noted that the 4 MET value in this example includes the resting energy expenditure component (1 MET). Therefore, the net caloric cost of the exercise would be based on only 3 METs. If the hypothetical patient in this example weighed 100 kg (220 lb) and exercised 3 days per week for 30 min, the net caloric expenditure would be approximately 480 kcal/week (5.3 kcal/min × 30 min × 3 days/week). Although patients can clearly improve exercise tolerance with this regimen, the estimated caloric expenditure falls well short of contemporary recommendations for PA and in most cases would not be effective for weight or fat loss.15 For example, 40 min sessions, five times per week, would result in an expenditure of approximately 1,060 kcal per week. Again, this calculation highlights the importance of increasing PA outside of the structured or in-hospital program. Thus, adjustments must be made about frequency and duration of exercise to allow patients to achieve greater energy expenditures to enhance program outcomes. However, these adjustments must be with the caveat that although it is prudent to increase exercise volume progressively, staff must carefully consider the risk that a higher-volume program may lead to higher dropout rates. Therefore, overweight patients must be educated about the need to develop and maintain fitness as the core of their exercise regimen, with the additional volume of PA facilitating weight loss and other goals. Finally, as CRF improves, patients are able to exercise at a higher metabolic rate (more kcal/min) at a given relative intensity (% maximal HRR). This adjustment allows patients to accumulate a greater caloric deficit over time.
Example of standing orders to initiate outpatient cardiac rehabilitation
Appendix A: Example of Standing Orders to Initiate Outpatient CR
- Initiate monitored exercise program per outpatient CR policies and procedures.
- Determine target heart rate (THR) via sign- or symptom-limited graded exercise testing (GXT) or sign- or symptom-limited responses to submaximal exercise.
- Begin with a training duration of up to 30 min to tolerance, one to five times a week.
- Gradually increase duration of training exercise if patient cardiovascular and physiological responses are within normal limits.
- Observe participant for signs of exercise intolerance and adapt or terminate exercise as indicated in policies and procedures.
- Assess lipid profile approximately six weeks postevent.
- Administer nitroglycerin 0.3 or 0.4 mg sublingually every 5 minutes × 3 as needed for angina discomfort or ischemic symptoms.
- Provide regular, periodic progress reports to the referring physician. Provide copies of reports to other physicians as needed.
- Initiate patient education and counseling sessions as patient needs indicate.
- Consult patient's personal physician or CR supervising physician for any necessary orders.
- Consult with the CR dietitian to provide individualized nutrition education for each participant.
- Enter the patient into a non-ECG-monitored maintenance program upon completion of early outpatient CR program.
__________________________________________________________________________________________
Physician's signature
___________________________________________
Date
From American Association of Cardiovascular and Pulmonary Rehabilitation, Guidelines for Cardiac Rehabilitation Programs, 6th ed.
(Champaign, IL: Human Kinetics, 2021).
Appendix B: Example of Outpatient CR Emergency Standing Orders*
Table of Contents
Protocols for Urgent Situations and Emergency Interventions in the Cardiac Rehabilitation Area
I. Cardiopulmonary arrest
II. Angina pectoris
III. Hypoglycemia
IV. Hyperglycemia
V. Hypotension
VI. Hypertension
VII. Dysrhythmias
VIII. Dyspnea
IX. Cerebrovascular accident
X. Placement of intravenous line
XI. Patient transportation
I. Cardiopulmonary Arrest
A. Identify responsiveness and determine if breathing is absent or abnormal (gasping).
B. Call out for help/activate emergency medical system (EMS).
- Call out for help from coworker. If no one responds and if no other staff member is available to assist, go to the nearest phone and activate EMS. (Emergency numbers with specific scripted instructions are posted at each phone.) Get defibrillator/automated external defibrillator (AED). If no pulse, attach defibrillator/AED and shock if indicated. Begin cardiopulmonary resuscitation (CPR) with compressions.
- If a second responder is available to assist, that person should activate EMS and then get the defibrillator/AED while the first responder stays with the patient to begin compressions.
- Staff will meet the EMS team at the appropriate entrance and direct them to the patient.
First Responder
- Determine responsiveness and absent or abnormal breathing.
- Send someone to activate EMS and get defibrillator/AED.
- If pulseless, begin chest compressions at a depth of at least 2 in. and a rate of at least 100 compressions/min until defibrillator/AED arrives. Allow for complete chest recoil, minimize interruptions to
Second Responder
- After activating EMS, take cart with defibrillator/AED to the patient. Place defibrillator pads or AED on patient and assess cardiac rhythm.
- Shock if indicated, resume compressions. Follow appropriate algorithm according to ACLS guidelines.
Third Responder (if Available)
- Direct remaining patients to another area.
- Direct and control incoming emergency response team and patients.
- Obtain extra supplies and equipment as needed.
- Act as the recorder of events until EMS arrives.
- Prepare records to be sent with patient to the emergency department if needed.
- Notify patient physician/cardiologist and family.
Emergency in Other Locations
7. Protocols should be developed for emergencies occurring in locations other than the cardiac rehabilitation gym including but not limited to:
- Locker room/restrooms
- Lobby/waiting area
- Patient education area
- Parking lots
II. Angina Pectoris
A. If a patient develops unstable angina while in the exercise area, the patient should immediately discontinue exercise and sit or lie down. Note the exercise workload, HR, and BP at which the symptoms occurred.
B. The following protocol should be followed by the CR staff:
- Check pulse, BP, cardiac rhythm (attach telemetry monitor if not already monitored), and oxygen saturation.
- Rate angina on a scale of 1 to 10.
- If no relief with 1 to 3 min of rest, give 1 nitroglycerine (NTG) 0.4 mg SL or spray.
- Obtain 12-lead ECG and call supervising physician.
C. If pain is relieved:
- If this angina is of new onset, the patient should be evaluated by the supervising physician. The primary care physician should be notified of the results of the evaluation and recommended treatment, if any.
- If the patient experiences chronic stable angina, exercise intensity should be decreased or halted until the angina is relieved. Patient may resume exercise at a lower workload dependent on the clinical judgment of the medical director and professional staff.
OR
The patient can be discharged but should be instructed to report any increase in frequency or severity of angina to their physician.
D. If pain is not relieved:
- Monitor pulse, BP, cardiac rhythm, and oxygen saturation closely.
- Place on oxygen at 2 to 4 L per nasal prongs if oxygen saturation is <94%.
- Patient to chew aspirin 160 to 325 mg.
- Repeat NTG 0.4 mg SL or spray every 5 min for unrelieved angina symptoms.
- The supervising physician will evaluate and determine the course of action.
III. Hypoglycemia
A. If patient displays any symptoms of hypoglycemia:
- Obtain finger-stick blood glucose level.
- If BG results are
- Retest BG in 15 min. If BG is not >90 mg/dL, repeat 15 g CHO and recheck BG in 15 min.
- If patient is uncooperative or unconscious, contact supervising physician, give glucose gel or establish IV access and give 50 cc (1 amp) 50% dextrose solution. Arrange for transport to ED.
IV. Hyperglycemia
A. A participant with a BG >300 mg/dL should not exercise unless the patient's referring physician and the program medical director give their consent.
B. Frequency of BG checks should be determined according to the patient profile and ITP.
C. BG evaluations may be performed by rehabilitation staff or the patient according to the ITP.
D. The CR staff may request a blood glucose evaluation on any patient based on suspected signs and symptoms of hyperglycemia (nausea, flushing, polyuria, polydipsia, fruity breath, tachypnea).
V. Hypotension
A. Remove the patient from the exercise area if possible.
B. Place patient in a supine position. Consider elevating legs or placing in Trendelenburg position.
C. Attach a telemetry monitor if not already monitored.
D. Check BP, pulse, cardiac rhythm, and oxygen saturation.
E. If no response to the position change, call the supervising physician. If the patient condition continues to deteriorate or becomes progressively symptomatic, or if BP continues to drop, start an IV of normal saline at 100 mL/h and arrange for transport to the ED. After evaluation and treatment of the patient, the supervising physician should notify the patient's primary care physician of the hypotensive episode and discuss any further treatment if necessary.
F. If patient responds to the supine position, keep supine until SBP is >100, then gradually assist to sitting position. Continue to monitor BP, pulse, and rhythm. Encourage fluids. Notify the patient's primary physician of the episode.
VI. Hypertension
A. Check every patient's BP before exercise and compare with previous recordings.
B. If the SBP reading is >170 mm Hg or the diastolic reading is >100 mm Hg, have the patient sit and recheck the BP in 5 min.
C. If the BP remains elevated, do not have patient exercise. Notify the primary care physician or supervising physician to evaluate and determine course of action.
D. Patients may exercise with elevated BP if directed by the primary care physician and medical director.
E. Investigate whether patient is complying with medications and sodium restrictions.
VII. Dysrhythmias
Premature Ventricular Contractions (PVCs)
A. Observe for the following:
- Frequency
- Whether multifocal or unifocal
- Pairs or runs, sustained or paroxysmal
- Associated signs or symptoms
- Palpate pulse to evaluate for peripheral perfusion
B. Document any new arrhythmias or increase in severity with a rhythm strip and make notation on chart. Notify supervising physician and referring physician, where appropriate, to discuss treatment.
C. Discontinue exercise if PVCs become symptomatic and check pulse, BP, and oxygen saturation. Provide oxygen at 2 to 4 L if hypoxemic, and obtain IV access if directed by a physician.
D. Notify the supervising physician for evaluation and treatment.
Bradycardia
A. If patient develops symptomatic bradycardia, stop exercise.
B. Monitor HR and rhythm, BP, and oximetry. Provide oxygen at 2 to 4 L if hypoxemic. Obtain 12-lead ECG if available.
C. Assess for symptoms of instability or altered mental status, ischemic chest discomfort, HF, or hypotension and notify supervising physician for evaluation and treatment. Notify the supervising physician and if available, obtain IV access, and prepare to administer atropine or external pacing per ACLS guidelines.
D. Prepare for transfer to ED.
Tachycardia
A. If patient develops a new wide or narrow complex tachycardia, stop exercise.
B. Monitor HR and rhythm, BP, and oximetry. Provide oxygen at 2 to 4 L if hypoxemic. Obtain 12-lead ECG if available.
C. Assess for symptoms of instability or altered mental status, ischemic chest discomfort, HF, or hypotension, and notify supervising physician for evaluation and treatment. If directed by a physician, obtain IV access and prepare for synchronized cardioversion. If stable, may utilize vagal maneuvers or antiarrhythmic agents per ACLS guidelines.
D. Prepare for transfer to ED.
VIII. Dyspnea
A. If patient develops acute dyspnea, stop exercise and have patient sit down.
B. Monitor heart rate and rhythm, BP, respiratory rate, lung sounds, and oximetry. Provide oxygen at 2 to 4 L for oxygen saturation <94%.
C. If patient has a metered-dose inhaler, it may be administered as prescribed.
D. If condition deteriorates, notify supervising physician to evaluate for treatment options and possible transfer to ED.
E. If condition improves, notify primary care physician for further recommendations.
IX. Cerebrovascular Accident
A. If patient develops signs and symptoms of a stroke such as sudden arm or leg weakness, confusion, trouble speaking, dizziness, loss of balance or coordination, severe headache, or facial droop, immediately evaluate with rapid out-of-hospital stroke assessment.
B. If stroke is suspected, initiate EMS for immediate transport to a stroke facility.
C. Establish time of last known neurological baseline.
D. Maintain airway, breathing, and circulation.
E. Provide supplemental oxygen if hypoxemic or if oxygen saturation is unknown.
F. Check blood glucose.
G. Alert receiving hospital when patient is in transport.
X. Placement of IV Line
Purpose: To provide immediate access to administer emergency medication and IV fluids.
A. An attempt will be made to notify the supervising physician.
B. Place a saline lock in participant when one or more of the following apply:
- Angina pectoris protocol has been followed and chest pain persists.
- ECG, vital signs or participant appears to be clinically unstable or symptomatic.
- Physician directs the placement of IV line.
XI. Patient Transportation
Staff will meet and direct ambulance personnel to the patient treatment area.
Staff will prepare medical records to be sent with the patient as needed.
Staff will alert the emergency department of the patient transfer.
Cardiac Rehabilitation Department Emergency Procedures and Standing Orders Were Reviewed and Approved
___________________________________________
Physician's name
___________________________________________
Signature
___________________________________________
Date of most recent review
*Appendix B should be used only as an example of standing orders that might be considered and adopted for use in freestanding outpatient or community-based programs.
From American Association of Cardiovascular and Pulmonary Rehabilitation, Guidelines for Cardiac Rehabilitation Programs, 6th ed.
(Champaign, IL: Human Kinetics, 2021).
What are cardiac dysrhythmias?
By Alison L. Bailey, Alexis L. Beatty, Brian Carlin, Dennis J. Kerrigan, Steven J. Keteyian, Kirstine Laerum Sibilitz, Karen Lui, Ryan Mays, Jonathan Powell, Ray W. Squires, Diane J. Treat-Jacobson
Cardiac dysrhythmias are abnormalities in heart rhythm. They are also known as arrhythmias or irregular rhythms. Many CR participants have a history of cardiac dysrhythmias, and some experience dysrhythmias during CR participation.1-3 Symptoms from dysrhythmias may or may not be present and vary from patient to patient. The effects of dysrhythmias can range from generally benign to potentially harmful. Most studies report a cardiac arrest rate of approximately 1/100,000 patient-hours of CR participation.4-7 Although it is rare for dysrhythmias to have life-threatening consequences during exercise in CR programs, it remains important to recognize dysrhythmias and their features.
Bottom Line
Cardiac dysrhythmias are common in CR participants. Life-threatening consequences of cardiac dysrhythmias are rare during exercise in CR programs.
The following are commonly encountered dysrhythmias and symptoms:
Cardiac Dysrhythmias in CR
Generally Benign
- Premature atrial complexes (PACs)
- Isolated premature ventricular complexes (PVCs)
- AF or atrial flutter with controlled ventricular rate (8
- Paroxysmal supraventricular tachycardia (SVT)
- Mild bradycardia (50-60 bpm)
- First-degree atrioventricular (AV) block and asymptomatic type I second-degree (also known as Wenckebach) AV block
Potentially or Likely Harmful
- AF or atrial flutter with a rapid rate (≥110 bpm at rest)
- Symptomatic or severe bradycardia (HR <50)
- Symptomatic or advanced AV block (type II second-degree AV block or complete heart block)
- Ventricular tachycardia
- Ventricular fibrillation
Symptoms Associated With Cardiac Dysrhythmias
Stable Symptoms
- Palpitations
- Dizziness or lightheadedness
- Shortness of breath
- Chest pain or discomfort
Nonspecific or Associated Symptoms
- Weakness or fatigue
- Sweating
- Blurred vision
- Nausea
- Anxiety
- Edema
Unstable Symptoms
- Hypotension
- Near-syncope or loss of consciousness
- HF
- Unstable angina or MI
- Cardiac arrest
Exercise induces many physiologic effects, which can have both direct and indirect effects on cardiac electrophysiology. Exercise intensity can be related to the occurrence of dysrhythmias. Some dysrhythmias diminish or disappear with increasing exercise intensity; others increase or appear with increasing exercise intensity; and still others have no observable relationship to exercise intensity. Factors that can contribute to dysrhythmias during exercise include autonomic nervous system activity, ischemia, genetic abnormalities, structural heart disease, medications with proarrhythmic side effects, electrolyte imbalance, dehydration, and certain environmental factors.
Guideline 10.7 Dysrhythmia Exercise Prescription
For patients with known dysrhythmias, the exercise prescription should be tailored to the individual, with predetermined goals and criteria for exercise termination. Exercise should be terminated when a patient experiences a potentially harmful dysrhythmia or dysrhythmia with unstable symptoms.
Atrial Fibrillation
Light-to-moderate activities, particularly leisure-time activity and walking, are associated with a significantly lower incidence of AF in older adults.9 However, people who participate in extreme endurance training and sports activities may have an increased incidence of AF.10,11 For those diagnosed with AF, regular moderate PA is known to increase exercise capacity and control ventricular rate.12,13 In addition, exercise training increases exercise capacity and may reduce AF burden.14,15 The following information provides specific information about CR participation in patients who have AF.
AF originates in the atrium and is the most common cardiac arrhythmia. It is characterized by irregular contractions of the muscle fibers of the atria resulting in a variable HR. Risk factors associated with developing AF include PA, obesity, advanced age, HTN, HF, diabetes mellitus, CVD and valvular heart disease, left ventricular and atrial enlargement, and hyperthyroidism.43 Paradoxically, despite having few risk factors, athletes are also at increased risk for developing AF.
CR professionals will encounter these two types of patients with AF: patients who experience an initial (acute) onset (often noted during CR check-in or during exercise) and patients previously diagnosed and medically managed. Generally, AF is classified as (1) paroxysmal, (2) persistent, (3) long-standing persistent, or (4) permanent.2
AF should be considered when a patient presents with a rapid (often >110 bpm) “irregularly irregular” (no rhythmic pattern) resting HR. Patients experiencing an abrupt onset of AF may or may not report accompanying symptoms including palpitation, tachycardia, fatigue, shortness of breath, dizziness, and nausea. If AF is suspected, an ECG will confirm a diagnosis.
If new-onset AF is confirmed, the patient's physician should be consulted. Treating new-onset AF has three goals.44,50 The first goal is to mitigate symptoms by initially focusing in on reducing HR. Typical therapeutic HR reduction options include beta-adrenergic and calcium channel blocking agents and antiarrhythmic medication. The second goal is to reduce the risk for the development embolization of a blood clot (which the patient is at risk of developing due to atrial blood stagnation) through anticoagulation therapy. The third goal is to manage the patient's cardiovascular risk factors, which for overweight or obese patients is recommended to include weight loss and risk factor modification.50
Safety and rates of adverse event of exercise in patients have not been well studied. No large randomized control trials of exercise training and AF have assessed safety and efficacy. Guidelines for the treatment of patients with AF do not explicitly endorse specific exercise recommendations. Exercise, however, is not contraindicated in patients with AF. Moreover, exercise is effective treatment in multiple risk factors associated with AF, such as physical inactivity, HTN, diabetes mellitus, and obesity. Therefore, asymptomatic patients with AF who have received medical clearance should be encouraged to participate in an exercise program.
However, AF can profoundly impact the physiologic response to exercise training.45 In particular, the rapid, irregular contraction of the atrium results in reduced ventricular output. To compensate for the reduced cardiac output there is a commensurate increase in the rate and irregularity of ventricular contraction. Despite the negative impact of AF, exercise training studies have demonstrated improvements in functional capacity, health status, and quality of life.46
The special consideration regarding exercise testing and prescription for patients with AF have been detailed elsewhere.3 The following section is a brief review of special considerations regarding exercise testing and prescription for CR participants with AF.
Exercise Testing
As with all patients entering CR, undergoing a symptom-limited exercise tolerance test prior to initiating an exercise training program is optimal but not required. An exercise test is useful to assess for myocardial ischemia, evaluate chronotropic response, identify signs and symptoms, quantify functional capacity, and establish some general parameters for exercise training intensity.
Exercise Prescription for Patients With AF
Currently, no specific recommendations exist regarding exercise training for the treatment of AF. Studies of exercise training in patients with AF have employed a variety of protocols. Components of any exercise prescription include frequency, intensity, duration, modality, progression, and total volume. The exercise prescription for patients with AF should be individualized. A meta-analysis of exercise training studies involving people with AF recommends that a training regimen should include three or more sessions per week of a combination of moderate-intensity aerobic activity and resistance training. Session duration should be approximately 60 minutes, including adequate warm-up and cool-down.
By definition, the HR for a person with AF is irregular. Therefore, use of HR exclusively to assess exercise intensity is problematic. For aerobic training, in lieu of HR, use of RPE scale is an effective means to assess exercise intensity. A rating of 11 to 14 (on the Borg 6-20 scale) is typically associated with a moderate intensity that is approximately 70% to 85% of peak exercise capacity. Notably, very few studies have focused on the safety and efficacy of high-intensity aerobic training in patients with AF.
For overweight patients with AF, weight loss is recommended.47,50 To facilitate weight loss, orienting the exercise prescription to maximize caloric expenditure is indicated. High caloric exercise training (e.g., treadmill walking at a moderate intensity for an extended duration) in CR is well tolerated and an effective strategy to promote weight loss and improve multiple cardiovascular risk factors.48
No specific guidelines exist for resistance training for patients with AF. Given the lack of recommendations, using professional discretion is necessary when providing guidance regarding resistance training. Following the resistance training recommendations for other, non-AF CR participants is advisable. General recommendations for resistance training are found in chapter 6.
Considerations for the prescription of exercise and physical activity
By Jonathan Myers
Guideline 6.1 Considerations for the Prescription of Exercise and Physical Activity
When developing an exercise prescription, consider the following factors:
Safety Factors
- Clinical history
- Risks associated with CVD progression or instability
- Ischemic and angina thresholds
- Cognitive or psychological impairment
Associated Factors
- Vocational or avocational requirements
- Orthopedic limitations
- Previous and current activities
- Personal health and fitness goals
An important initial consideration in exercise planning is safety. Safety considerations apply to both structured exercise training and leisure-time PA. While most patients can engage in exercise without incurring undue risks, appropriate risk stratification should be performed. Guideline 6.1 provides key variables to consider when developing an exercise prescription. Safety and risk stratification are discussed in detail in chapters 4 and 5. Recommendations for supervision and ECG monitoring can be found in chapter 5. Later in this chapter, tables 6.1 and 6.2 present basic principles of exercise prescription. A model for risk stratification for cardiovascular events is outlined in the sidebar Stratification of Risk for Cardiac Events During Exercise Participation in chapter 5. After risk stratification, recommendations for supervision, ECG, monitoring and prescribed intensity and duration of exercise training can be made.
Comprehensive, evidence-based recommendations for structured exercise training in CR are available from several prominent organizations1,3,8 and are only summarized here. A comprehensive exercise program includes cardiorespiratory, musculoskeletal, and flexibility components. Specific elements for each component are summarized in the tables in this chapter and include guidelines for intensity, duration, frequency, and type of exercise for training. Each of the elements should be prescribed relative to one another and in a way that effectively addresses predefined training goals (e.g., increased aerobic or musculoskeletal fitness, weight reduction, control of blood glucose, or resumption of occupation).
Cardiorespiratory Endurance Training
Cardiorespiratory endurance training should be the foundation of most exercise routines for adults with or at risk for CVD. This type of exercise training is the most effective way to increase CRF. Elements of an exercise prescription for increasing CRF are presented in table 6.1. The relative training intensity may vary between 40% and 80% of maximal heart rate reserve (HRR) or metabolic reserve (V.O2R). Initially, programs should focus on the lower part of the intensity range, with progression to higher intensities as patients adapt to the program.7 RPE (e.g., Borg Scale of Perceived Exertion 6-20; Borg CR10 Scale; Omni Picture System of Perceived Exertion) are considered adjunctive to HR monitoring, but they may become more important as a subjective intensity guide as patients gain experience with exercise training and learn how to use the scale. Exercise training duration varies as a function of the overall energy expenditure goals of the patient. A minimum of 20 continuous minutes of exercise per session is commonly recommended within structured programs, although some patients may follow an intermittent (i.e., interval) exercise regimen. Some patients may need to accumulate shorter bouts (e.g., multiple 10 min bouts) throughout the day due to comorbidities, symptoms such as claudication or musculoskeletal discomfort, or lifestyle factors. Ideally, patients should be active most days of the week,1-7,9 but structured programs are often designed with a frequency of two to four sessions per week.
Once the initial exercise prescription is established, patients should progress gradually toward predefined or redefined program goals. There is no set format with respect to progression because many factors, including fitness level, motivation, and orthopedic limitations, influence the rate at which a patient may progress. In general, it is prudent to change one component and provide some time (a minimum of one exercise session) to assess the adaptation to the new level before progressing further. When time permits, increases in duration and frequency should precede increases in intensity. Modest increases in intensity, when appropriate, are likely to be tolerated and should be based on the observations of the staff and subjective responses of the patient, provided that the changes remain within the limits specified in the most recent evaluation.
A guiding principle should be progression of the total volume or dose of exercise such that the patient achieves desired energy expenditure thresholds within a three- to six-month period. Therefore, given that most patients' participation in CR lasts no longer than three months, it is important to educate and encourage patients to continue exercising even after CR participation has ended. The most appropriate volume of exercise depends on the individual CVD risk profile, training goals, and comorbidities (i.e., diabetes, hypertension, obesity, arthritis). An accumulating body of evidence has affirmed a dose-response relationship between the volume of PA and health outcomes.1,3,6-8 Whether exercise has a role in reversing coronary artery disease is an issue that remains controversial; however, thresholds of approximately 1,500 and 2,200 kcal/week are associated with stability and regression of coronary artery lesions, respectively.18 Notably, multiple studies document that energy expenditure in structured CR does not typically meet either of these thresholds.11-14 Therefore, patients will likely need to engage in PA outside of the structured program to achieve the optimal levels of energy expenditure.
Few studies have supported the efficacy of structured exercise training as a singular strategy to normalize body weight and body composition in patients with CVD. This underscores the importance of multiple behavioral strategies in weight reduction programming for overweight patients. Studies show that achieving weight loss goals requires a simultaneous change in dietary habits in addition to greater physical activity patterns. The volume or dose of exercise associated with the typical CR training session may be a limiting factor, and there is only a 1 to 2 kg weight loss during CR participation. It is likely part of the explanation for a low amount of weight loss during CR is due to a lack of focus on helping patients lose weight. As mentioned previously, numerous studies have shown the weekly dose to be inadequate for weight or fat reduction. As an example, a typical exercise session for an outpatient with a peak functional capacity of 7 METs might be 30 min at a heart rate that would equate with about 4 METs. The following formula provides a method to estimate the caloric costs of the exercise session:
Calories/min = [METs × body weight in kg × 3.5] / 200
It should be noted that the 4 MET value in this example includes the resting energy expenditure component (1 MET). Therefore, the net caloric cost of the exercise would be based on only 3 METs. If the hypothetical patient in this example weighed 100 kg (220 lb) and exercised 3 days per week for 30 min, the net caloric expenditure would be approximately 480 kcal/week (5.3 kcal/min × 30 min × 3 days/week). Although patients can clearly improve exercise tolerance with this regimen, the estimated caloric expenditure falls well short of contemporary recommendations for PA and in most cases would not be effective for weight or fat loss.15 For example, 40 min sessions, five times per week, would result in an expenditure of approximately 1,060 kcal per week. Again, this calculation highlights the importance of increasing PA outside of the structured or in-hospital program. Thus, adjustments must be made about frequency and duration of exercise to allow patients to achieve greater energy expenditures to enhance program outcomes. However, these adjustments must be with the caveat that although it is prudent to increase exercise volume progressively, staff must carefully consider the risk that a higher-volume program may lead to higher dropout rates. Therefore, overweight patients must be educated about the need to develop and maintain fitness as the core of their exercise regimen, with the additional volume of PA facilitating weight loss and other goals. Finally, as CRF improves, patients are able to exercise at a higher metabolic rate (more kcal/min) at a given relative intensity (% maximal HRR). This adjustment allows patients to accumulate a greater caloric deficit over time.
Example of standing orders to initiate outpatient cardiac rehabilitation
Appendix A: Example of Standing Orders to Initiate Outpatient CR
- Initiate monitored exercise program per outpatient CR policies and procedures.
- Determine target heart rate (THR) via sign- or symptom-limited graded exercise testing (GXT) or sign- or symptom-limited responses to submaximal exercise.
- Begin with a training duration of up to 30 min to tolerance, one to five times a week.
- Gradually increase duration of training exercise if patient cardiovascular and physiological responses are within normal limits.
- Observe participant for signs of exercise intolerance and adapt or terminate exercise as indicated in policies and procedures.
- Assess lipid profile approximately six weeks postevent.
- Administer nitroglycerin 0.3 or 0.4 mg sublingually every 5 minutes × 3 as needed for angina discomfort or ischemic symptoms.
- Provide regular, periodic progress reports to the referring physician. Provide copies of reports to other physicians as needed.
- Initiate patient education and counseling sessions as patient needs indicate.
- Consult patient's personal physician or CR supervising physician for any necessary orders.
- Consult with the CR dietitian to provide individualized nutrition education for each participant.
- Enter the patient into a non-ECG-monitored maintenance program upon completion of early outpatient CR program.
__________________________________________________________________________________________
Physician's signature
___________________________________________
Date
From American Association of Cardiovascular and Pulmonary Rehabilitation, Guidelines for Cardiac Rehabilitation Programs, 6th ed.
(Champaign, IL: Human Kinetics, 2021).
Appendix B: Example of Outpatient CR Emergency Standing Orders*
Table of Contents
Protocols for Urgent Situations and Emergency Interventions in the Cardiac Rehabilitation Area
I. Cardiopulmonary arrest
II. Angina pectoris
III. Hypoglycemia
IV. Hyperglycemia
V. Hypotension
VI. Hypertension
VII. Dysrhythmias
VIII. Dyspnea
IX. Cerebrovascular accident
X. Placement of intravenous line
XI. Patient transportation
I. Cardiopulmonary Arrest
A. Identify responsiveness and determine if breathing is absent or abnormal (gasping).
B. Call out for help/activate emergency medical system (EMS).
- Call out for help from coworker. If no one responds and if no other staff member is available to assist, go to the nearest phone and activate EMS. (Emergency numbers with specific scripted instructions are posted at each phone.) Get defibrillator/automated external defibrillator (AED). If no pulse, attach defibrillator/AED and shock if indicated. Begin cardiopulmonary resuscitation (CPR) with compressions.
- If a second responder is available to assist, that person should activate EMS and then get the defibrillator/AED while the first responder stays with the patient to begin compressions.
- Staff will meet the EMS team at the appropriate entrance and direct them to the patient.
First Responder
- Determine responsiveness and absent or abnormal breathing.
- Send someone to activate EMS and get defibrillator/AED.
- If pulseless, begin chest compressions at a depth of at least 2 in. and a rate of at least 100 compressions/min until defibrillator/AED arrives. Allow for complete chest recoil, minimize interruptions to
Second Responder
- After activating EMS, take cart with defibrillator/AED to the patient. Place defibrillator pads or AED on patient and assess cardiac rhythm.
- Shock if indicated, resume compressions. Follow appropriate algorithm according to ACLS guidelines.
Third Responder (if Available)
- Direct remaining patients to another area.
- Direct and control incoming emergency response team and patients.
- Obtain extra supplies and equipment as needed.
- Act as the recorder of events until EMS arrives.
- Prepare records to be sent with patient to the emergency department if needed.
- Notify patient physician/cardiologist and family.
Emergency in Other Locations
7. Protocols should be developed for emergencies occurring in locations other than the cardiac rehabilitation gym including but not limited to:
- Locker room/restrooms
- Lobby/waiting area
- Patient education area
- Parking lots
II. Angina Pectoris
A. If a patient develops unstable angina while in the exercise area, the patient should immediately discontinue exercise and sit or lie down. Note the exercise workload, HR, and BP at which the symptoms occurred.
B. The following protocol should be followed by the CR staff:
- Check pulse, BP, cardiac rhythm (attach telemetry monitor if not already monitored), and oxygen saturation.
- Rate angina on a scale of 1 to 10.
- If no relief with 1 to 3 min of rest, give 1 nitroglycerine (NTG) 0.4 mg SL or spray.
- Obtain 12-lead ECG and call supervising physician.
C. If pain is relieved:
- If this angina is of new onset, the patient should be evaluated by the supervising physician. The primary care physician should be notified of the results of the evaluation and recommended treatment, if any.
- If the patient experiences chronic stable angina, exercise intensity should be decreased or halted until the angina is relieved. Patient may resume exercise at a lower workload dependent on the clinical judgment of the medical director and professional staff.
OR
The patient can be discharged but should be instructed to report any increase in frequency or severity of angina to their physician.
D. If pain is not relieved:
- Monitor pulse, BP, cardiac rhythm, and oxygen saturation closely.
- Place on oxygen at 2 to 4 L per nasal prongs if oxygen saturation is <94%.
- Patient to chew aspirin 160 to 325 mg.
- Repeat NTG 0.4 mg SL or spray every 5 min for unrelieved angina symptoms.
- The supervising physician will evaluate and determine the course of action.
III. Hypoglycemia
A. If patient displays any symptoms of hypoglycemia:
- Obtain finger-stick blood glucose level.
- If BG results are
- Retest BG in 15 min. If BG is not >90 mg/dL, repeat 15 g CHO and recheck BG in 15 min.
- If patient is uncooperative or unconscious, contact supervising physician, give glucose gel or establish IV access and give 50 cc (1 amp) 50% dextrose solution. Arrange for transport to ED.
IV. Hyperglycemia
A. A participant with a BG >300 mg/dL should not exercise unless the patient's referring physician and the program medical director give their consent.
B. Frequency of BG checks should be determined according to the patient profile and ITP.
C. BG evaluations may be performed by rehabilitation staff or the patient according to the ITP.
D. The CR staff may request a blood glucose evaluation on any patient based on suspected signs and symptoms of hyperglycemia (nausea, flushing, polyuria, polydipsia, fruity breath, tachypnea).
V. Hypotension
A. Remove the patient from the exercise area if possible.
B. Place patient in a supine position. Consider elevating legs or placing in Trendelenburg position.
C. Attach a telemetry monitor if not already monitored.
D. Check BP, pulse, cardiac rhythm, and oxygen saturation.
E. If no response to the position change, call the supervising physician. If the patient condition continues to deteriorate or becomes progressively symptomatic, or if BP continues to drop, start an IV of normal saline at 100 mL/h and arrange for transport to the ED. After evaluation and treatment of the patient, the supervising physician should notify the patient's primary care physician of the hypotensive episode and discuss any further treatment if necessary.
F. If patient responds to the supine position, keep supine until SBP is >100, then gradually assist to sitting position. Continue to monitor BP, pulse, and rhythm. Encourage fluids. Notify the patient's primary physician of the episode.
VI. Hypertension
A. Check every patient's BP before exercise and compare with previous recordings.
B. If the SBP reading is >170 mm Hg or the diastolic reading is >100 mm Hg, have the patient sit and recheck the BP in 5 min.
C. If the BP remains elevated, do not have patient exercise. Notify the primary care physician or supervising physician to evaluate and determine course of action.
D. Patients may exercise with elevated BP if directed by the primary care physician and medical director.
E. Investigate whether patient is complying with medications and sodium restrictions.
VII. Dysrhythmias
Premature Ventricular Contractions (PVCs)
A. Observe for the following:
- Frequency
- Whether multifocal or unifocal
- Pairs or runs, sustained or paroxysmal
- Associated signs or symptoms
- Palpate pulse to evaluate for peripheral perfusion
B. Document any new arrhythmias or increase in severity with a rhythm strip and make notation on chart. Notify supervising physician and referring physician, where appropriate, to discuss treatment.
C. Discontinue exercise if PVCs become symptomatic and check pulse, BP, and oxygen saturation. Provide oxygen at 2 to 4 L if hypoxemic, and obtain IV access if directed by a physician.
D. Notify the supervising physician for evaluation and treatment.
Bradycardia
A. If patient develops symptomatic bradycardia, stop exercise.
B. Monitor HR and rhythm, BP, and oximetry. Provide oxygen at 2 to 4 L if hypoxemic. Obtain 12-lead ECG if available.
C. Assess for symptoms of instability or altered mental status, ischemic chest discomfort, HF, or hypotension and notify supervising physician for evaluation and treatment. Notify the supervising physician and if available, obtain IV access, and prepare to administer atropine or external pacing per ACLS guidelines.
D. Prepare for transfer to ED.
Tachycardia
A. If patient develops a new wide or narrow complex tachycardia, stop exercise.
B. Monitor HR and rhythm, BP, and oximetry. Provide oxygen at 2 to 4 L if hypoxemic. Obtain 12-lead ECG if available.
C. Assess for symptoms of instability or altered mental status, ischemic chest discomfort, HF, or hypotension, and notify supervising physician for evaluation and treatment. If directed by a physician, obtain IV access and prepare for synchronized cardioversion. If stable, may utilize vagal maneuvers or antiarrhythmic agents per ACLS guidelines.
D. Prepare for transfer to ED.
VIII. Dyspnea
A. If patient develops acute dyspnea, stop exercise and have patient sit down.
B. Monitor heart rate and rhythm, BP, respiratory rate, lung sounds, and oximetry. Provide oxygen at 2 to 4 L for oxygen saturation <94%.
C. If patient has a metered-dose inhaler, it may be administered as prescribed.
D. If condition deteriorates, notify supervising physician to evaluate for treatment options and possible transfer to ED.
E. If condition improves, notify primary care physician for further recommendations.
IX. Cerebrovascular Accident
A. If patient develops signs and symptoms of a stroke such as sudden arm or leg weakness, confusion, trouble speaking, dizziness, loss of balance or coordination, severe headache, or facial droop, immediately evaluate with rapid out-of-hospital stroke assessment.
B. If stroke is suspected, initiate EMS for immediate transport to a stroke facility.
C. Establish time of last known neurological baseline.
D. Maintain airway, breathing, and circulation.
E. Provide supplemental oxygen if hypoxemic or if oxygen saturation is unknown.
F. Check blood glucose.
G. Alert receiving hospital when patient is in transport.
X. Placement of IV Line
Purpose: To provide immediate access to administer emergency medication and IV fluids.
A. An attempt will be made to notify the supervising physician.
B. Place a saline lock in participant when one or more of the following apply:
- Angina pectoris protocol has been followed and chest pain persists.
- ECG, vital signs or participant appears to be clinically unstable or symptomatic.
- Physician directs the placement of IV line.
XI. Patient Transportation
Staff will meet and direct ambulance personnel to the patient treatment area.
Staff will prepare medical records to be sent with the patient as needed.
Staff will alert the emergency department of the patient transfer.
Cardiac Rehabilitation Department Emergency Procedures and Standing Orders Were Reviewed and Approved
___________________________________________
Physician's name
___________________________________________
Signature
___________________________________________
Date of most recent review
*Appendix B should be used only as an example of standing orders that might be considered and adopted for use in freestanding outpatient or community-based programs.
From American Association of Cardiovascular and Pulmonary Rehabilitation, Guidelines for Cardiac Rehabilitation Programs, 6th ed.
(Champaign, IL: Human Kinetics, 2021).
What are cardiac dysrhythmias?
By Alison L. Bailey, Alexis L. Beatty, Brian Carlin, Dennis J. Kerrigan, Steven J. Keteyian, Kirstine Laerum Sibilitz, Karen Lui, Ryan Mays, Jonathan Powell, Ray W. Squires, Diane J. Treat-Jacobson
Cardiac dysrhythmias are abnormalities in heart rhythm. They are also known as arrhythmias or irregular rhythms. Many CR participants have a history of cardiac dysrhythmias, and some experience dysrhythmias during CR participation.1-3 Symptoms from dysrhythmias may or may not be present and vary from patient to patient. The effects of dysrhythmias can range from generally benign to potentially harmful. Most studies report a cardiac arrest rate of approximately 1/100,000 patient-hours of CR participation.4-7 Although it is rare for dysrhythmias to have life-threatening consequences during exercise in CR programs, it remains important to recognize dysrhythmias and their features.
Bottom Line
Cardiac dysrhythmias are common in CR participants. Life-threatening consequences of cardiac dysrhythmias are rare during exercise in CR programs.
The following are commonly encountered dysrhythmias and symptoms:
Cardiac Dysrhythmias in CR
Generally Benign
- Premature atrial complexes (PACs)
- Isolated premature ventricular complexes (PVCs)
- AF or atrial flutter with controlled ventricular rate (8
- Paroxysmal supraventricular tachycardia (SVT)
- Mild bradycardia (50-60 bpm)
- First-degree atrioventricular (AV) block and asymptomatic type I second-degree (also known as Wenckebach) AV block
Potentially or Likely Harmful
- AF or atrial flutter with a rapid rate (≥110 bpm at rest)
- Symptomatic or severe bradycardia (HR <50)
- Symptomatic or advanced AV block (type II second-degree AV block or complete heart block)
- Ventricular tachycardia
- Ventricular fibrillation
Symptoms Associated With Cardiac Dysrhythmias
Stable Symptoms
- Palpitations
- Dizziness or lightheadedness
- Shortness of breath
- Chest pain or discomfort
Nonspecific or Associated Symptoms
- Weakness or fatigue
- Sweating
- Blurred vision
- Nausea
- Anxiety
- Edema
Unstable Symptoms
- Hypotension
- Near-syncope or loss of consciousness
- HF
- Unstable angina or MI
- Cardiac arrest
Exercise induces many physiologic effects, which can have both direct and indirect effects on cardiac electrophysiology. Exercise intensity can be related to the occurrence of dysrhythmias. Some dysrhythmias diminish or disappear with increasing exercise intensity; others increase or appear with increasing exercise intensity; and still others have no observable relationship to exercise intensity. Factors that can contribute to dysrhythmias during exercise include autonomic nervous system activity, ischemia, genetic abnormalities, structural heart disease, medications with proarrhythmic side effects, electrolyte imbalance, dehydration, and certain environmental factors.
Guideline 10.7 Dysrhythmia Exercise Prescription
For patients with known dysrhythmias, the exercise prescription should be tailored to the individual, with predetermined goals and criteria for exercise termination. Exercise should be terminated when a patient experiences a potentially harmful dysrhythmia or dysrhythmia with unstable symptoms.
Atrial Fibrillation
Light-to-moderate activities, particularly leisure-time activity and walking, are associated with a significantly lower incidence of AF in older adults.9 However, people who participate in extreme endurance training and sports activities may have an increased incidence of AF.10,11 For those diagnosed with AF, regular moderate PA is known to increase exercise capacity and control ventricular rate.12,13 In addition, exercise training increases exercise capacity and may reduce AF burden.14,15 The following information provides specific information about CR participation in patients who have AF.
AF originates in the atrium and is the most common cardiac arrhythmia. It is characterized by irregular contractions of the muscle fibers of the atria resulting in a variable HR. Risk factors associated with developing AF include PA, obesity, advanced age, HTN, HF, diabetes mellitus, CVD and valvular heart disease, left ventricular and atrial enlargement, and hyperthyroidism.43 Paradoxically, despite having few risk factors, athletes are also at increased risk for developing AF.
CR professionals will encounter these two types of patients with AF: patients who experience an initial (acute) onset (often noted during CR check-in or during exercise) and patients previously diagnosed and medically managed. Generally, AF is classified as (1) paroxysmal, (2) persistent, (3) long-standing persistent, or (4) permanent.2
AF should be considered when a patient presents with a rapid (often >110 bpm) “irregularly irregular” (no rhythmic pattern) resting HR. Patients experiencing an abrupt onset of AF may or may not report accompanying symptoms including palpitation, tachycardia, fatigue, shortness of breath, dizziness, and nausea. If AF is suspected, an ECG will confirm a diagnosis.
If new-onset AF is confirmed, the patient's physician should be consulted. Treating new-onset AF has three goals.44,50 The first goal is to mitigate symptoms by initially focusing in on reducing HR. Typical therapeutic HR reduction options include beta-adrenergic and calcium channel blocking agents and antiarrhythmic medication. The second goal is to reduce the risk for the development embolization of a blood clot (which the patient is at risk of developing due to atrial blood stagnation) through anticoagulation therapy. The third goal is to manage the patient's cardiovascular risk factors, which for overweight or obese patients is recommended to include weight loss and risk factor modification.50
Safety and rates of adverse event of exercise in patients have not been well studied. No large randomized control trials of exercise training and AF have assessed safety and efficacy. Guidelines for the treatment of patients with AF do not explicitly endorse specific exercise recommendations. Exercise, however, is not contraindicated in patients with AF. Moreover, exercise is effective treatment in multiple risk factors associated with AF, such as physical inactivity, HTN, diabetes mellitus, and obesity. Therefore, asymptomatic patients with AF who have received medical clearance should be encouraged to participate in an exercise program.
However, AF can profoundly impact the physiologic response to exercise training.45 In particular, the rapid, irregular contraction of the atrium results in reduced ventricular output. To compensate for the reduced cardiac output there is a commensurate increase in the rate and irregularity of ventricular contraction. Despite the negative impact of AF, exercise training studies have demonstrated improvements in functional capacity, health status, and quality of life.46
The special consideration regarding exercise testing and prescription for patients with AF have been detailed elsewhere.3 The following section is a brief review of special considerations regarding exercise testing and prescription for CR participants with AF.
Exercise Testing
As with all patients entering CR, undergoing a symptom-limited exercise tolerance test prior to initiating an exercise training program is optimal but not required. An exercise test is useful to assess for myocardial ischemia, evaluate chronotropic response, identify signs and symptoms, quantify functional capacity, and establish some general parameters for exercise training intensity.
Exercise Prescription for Patients With AF
Currently, no specific recommendations exist regarding exercise training for the treatment of AF. Studies of exercise training in patients with AF have employed a variety of protocols. Components of any exercise prescription include frequency, intensity, duration, modality, progression, and total volume. The exercise prescription for patients with AF should be individualized. A meta-analysis of exercise training studies involving people with AF recommends that a training regimen should include three or more sessions per week of a combination of moderate-intensity aerobic activity and resistance training. Session duration should be approximately 60 minutes, including adequate warm-up and cool-down.
By definition, the HR for a person with AF is irregular. Therefore, use of HR exclusively to assess exercise intensity is problematic. For aerobic training, in lieu of HR, use of RPE scale is an effective means to assess exercise intensity. A rating of 11 to 14 (on the Borg 6-20 scale) is typically associated with a moderate intensity that is approximately 70% to 85% of peak exercise capacity. Notably, very few studies have focused on the safety and efficacy of high-intensity aerobic training in patients with AF.
For overweight patients with AF, weight loss is recommended.47,50 To facilitate weight loss, orienting the exercise prescription to maximize caloric expenditure is indicated. High caloric exercise training (e.g., treadmill walking at a moderate intensity for an extended duration) in CR is well tolerated and an effective strategy to promote weight loss and improve multiple cardiovascular risk factors.48
No specific guidelines exist for resistance training for patients with AF. Given the lack of recommendations, using professional discretion is necessary when providing guidance regarding resistance training. Following the resistance training recommendations for other, non-AF CR participants is advisable. General recommendations for resistance training are found in chapter 6.
Considerations for the prescription of exercise and physical activity
By Jonathan Myers
Guideline 6.1 Considerations for the Prescription of Exercise and Physical Activity
When developing an exercise prescription, consider the following factors:
Safety Factors
- Clinical history
- Risks associated with CVD progression or instability
- Ischemic and angina thresholds
- Cognitive or psychological impairment
Associated Factors
- Vocational or avocational requirements
- Orthopedic limitations
- Previous and current activities
- Personal health and fitness goals
An important initial consideration in exercise planning is safety. Safety considerations apply to both structured exercise training and leisure-time PA. While most patients can engage in exercise without incurring undue risks, appropriate risk stratification should be performed. Guideline 6.1 provides key variables to consider when developing an exercise prescription. Safety and risk stratification are discussed in detail in chapters 4 and 5. Recommendations for supervision and ECG monitoring can be found in chapter 5. Later in this chapter, tables 6.1 and 6.2 present basic principles of exercise prescription. A model for risk stratification for cardiovascular events is outlined in the sidebar Stratification of Risk for Cardiac Events During Exercise Participation in chapter 5. After risk stratification, recommendations for supervision, ECG, monitoring and prescribed intensity and duration of exercise training can be made.
Comprehensive, evidence-based recommendations for structured exercise training in CR are available from several prominent organizations1,3,8 and are only summarized here. A comprehensive exercise program includes cardiorespiratory, musculoskeletal, and flexibility components. Specific elements for each component are summarized in the tables in this chapter and include guidelines for intensity, duration, frequency, and type of exercise for training. Each of the elements should be prescribed relative to one another and in a way that effectively addresses predefined training goals (e.g., increased aerobic or musculoskeletal fitness, weight reduction, control of blood glucose, or resumption of occupation).
Cardiorespiratory Endurance Training
Cardiorespiratory endurance training should be the foundation of most exercise routines for adults with or at risk for CVD. This type of exercise training is the most effective way to increase CRF. Elements of an exercise prescription for increasing CRF are presented in table 6.1. The relative training intensity may vary between 40% and 80% of maximal heart rate reserve (HRR) or metabolic reserve (V.O2R). Initially, programs should focus on the lower part of the intensity range, with progression to higher intensities as patients adapt to the program.7 RPE (e.g., Borg Scale of Perceived Exertion 6-20; Borg CR10 Scale; Omni Picture System of Perceived Exertion) are considered adjunctive to HR monitoring, but they may become more important as a subjective intensity guide as patients gain experience with exercise training and learn how to use the scale. Exercise training duration varies as a function of the overall energy expenditure goals of the patient. A minimum of 20 continuous minutes of exercise per session is commonly recommended within structured programs, although some patients may follow an intermittent (i.e., interval) exercise regimen. Some patients may need to accumulate shorter bouts (e.g., multiple 10 min bouts) throughout the day due to comorbidities, symptoms such as claudication or musculoskeletal discomfort, or lifestyle factors. Ideally, patients should be active most days of the week,1-7,9 but structured programs are often designed with a frequency of two to four sessions per week.
Once the initial exercise prescription is established, patients should progress gradually toward predefined or redefined program goals. There is no set format with respect to progression because many factors, including fitness level, motivation, and orthopedic limitations, influence the rate at which a patient may progress. In general, it is prudent to change one component and provide some time (a minimum of one exercise session) to assess the adaptation to the new level before progressing further. When time permits, increases in duration and frequency should precede increases in intensity. Modest increases in intensity, when appropriate, are likely to be tolerated and should be based on the observations of the staff and subjective responses of the patient, provided that the changes remain within the limits specified in the most recent evaluation.
A guiding principle should be progression of the total volume or dose of exercise such that the patient achieves desired energy expenditure thresholds within a three- to six-month period. Therefore, given that most patients' participation in CR lasts no longer than three months, it is important to educate and encourage patients to continue exercising even after CR participation has ended. The most appropriate volume of exercise depends on the individual CVD risk profile, training goals, and comorbidities (i.e., diabetes, hypertension, obesity, arthritis). An accumulating body of evidence has affirmed a dose-response relationship between the volume of PA and health outcomes.1,3,6-8 Whether exercise has a role in reversing coronary artery disease is an issue that remains controversial; however, thresholds of approximately 1,500 and 2,200 kcal/week are associated with stability and regression of coronary artery lesions, respectively.18 Notably, multiple studies document that energy expenditure in structured CR does not typically meet either of these thresholds.11-14 Therefore, patients will likely need to engage in PA outside of the structured program to achieve the optimal levels of energy expenditure.
Few studies have supported the efficacy of structured exercise training as a singular strategy to normalize body weight and body composition in patients with CVD. This underscores the importance of multiple behavioral strategies in weight reduction programming for overweight patients. Studies show that achieving weight loss goals requires a simultaneous change in dietary habits in addition to greater physical activity patterns. The volume or dose of exercise associated with the typical CR training session may be a limiting factor, and there is only a 1 to 2 kg weight loss during CR participation. It is likely part of the explanation for a low amount of weight loss during CR is due to a lack of focus on helping patients lose weight. As mentioned previously, numerous studies have shown the weekly dose to be inadequate for weight or fat reduction. As an example, a typical exercise session for an outpatient with a peak functional capacity of 7 METs might be 30 min at a heart rate that would equate with about 4 METs. The following formula provides a method to estimate the caloric costs of the exercise session:
Calories/min = [METs × body weight in kg × 3.5] / 200
It should be noted that the 4 MET value in this example includes the resting energy expenditure component (1 MET). Therefore, the net caloric cost of the exercise would be based on only 3 METs. If the hypothetical patient in this example weighed 100 kg (220 lb) and exercised 3 days per week for 30 min, the net caloric expenditure would be approximately 480 kcal/week (5.3 kcal/min × 30 min × 3 days/week). Although patients can clearly improve exercise tolerance with this regimen, the estimated caloric expenditure falls well short of contemporary recommendations for PA and in most cases would not be effective for weight or fat loss.15 For example, 40 min sessions, five times per week, would result in an expenditure of approximately 1,060 kcal per week. Again, this calculation highlights the importance of increasing PA outside of the structured or in-hospital program. Thus, adjustments must be made about frequency and duration of exercise to allow patients to achieve greater energy expenditures to enhance program outcomes. However, these adjustments must be with the caveat that although it is prudent to increase exercise volume progressively, staff must carefully consider the risk that a higher-volume program may lead to higher dropout rates. Therefore, overweight patients must be educated about the need to develop and maintain fitness as the core of their exercise regimen, with the additional volume of PA facilitating weight loss and other goals. Finally, as CRF improves, patients are able to exercise at a higher metabolic rate (more kcal/min) at a given relative intensity (% maximal HRR). This adjustment allows patients to accumulate a greater caloric deficit over time.
Example of standing orders to initiate outpatient cardiac rehabilitation
Appendix A: Example of Standing Orders to Initiate Outpatient CR
- Initiate monitored exercise program per outpatient CR policies and procedures.
- Determine target heart rate (THR) via sign- or symptom-limited graded exercise testing (GXT) or sign- or symptom-limited responses to submaximal exercise.
- Begin with a training duration of up to 30 min to tolerance, one to five times a week.
- Gradually increase duration of training exercise if patient cardiovascular and physiological responses are within normal limits.
- Observe participant for signs of exercise intolerance and adapt or terminate exercise as indicated in policies and procedures.
- Assess lipid profile approximately six weeks postevent.
- Administer nitroglycerin 0.3 or 0.4 mg sublingually every 5 minutes × 3 as needed for angina discomfort or ischemic symptoms.
- Provide regular, periodic progress reports to the referring physician. Provide copies of reports to other physicians as needed.
- Initiate patient education and counseling sessions as patient needs indicate.
- Consult patient's personal physician or CR supervising physician for any necessary orders.
- Consult with the CR dietitian to provide individualized nutrition education for each participant.
- Enter the patient into a non-ECG-monitored maintenance program upon completion of early outpatient CR program.
__________________________________________________________________________________________
Physician's signature
___________________________________________
Date
From American Association of Cardiovascular and Pulmonary Rehabilitation, Guidelines for Cardiac Rehabilitation Programs, 6th ed.
(Champaign, IL: Human Kinetics, 2021).
Appendix B: Example of Outpatient CR Emergency Standing Orders*
Table of Contents
Protocols for Urgent Situations and Emergency Interventions in the Cardiac Rehabilitation Area
I. Cardiopulmonary arrest
II. Angina pectoris
III. Hypoglycemia
IV. Hyperglycemia
V. Hypotension
VI. Hypertension
VII. Dysrhythmias
VIII. Dyspnea
IX. Cerebrovascular accident
X. Placement of intravenous line
XI. Patient transportation
I. Cardiopulmonary Arrest
A. Identify responsiveness and determine if breathing is absent or abnormal (gasping).
B. Call out for help/activate emergency medical system (EMS).
- Call out for help from coworker. If no one responds and if no other staff member is available to assist, go to the nearest phone and activate EMS. (Emergency numbers with specific scripted instructions are posted at each phone.) Get defibrillator/automated external defibrillator (AED). If no pulse, attach defibrillator/AED and shock if indicated. Begin cardiopulmonary resuscitation (CPR) with compressions.
- If a second responder is available to assist, that person should activate EMS and then get the defibrillator/AED while the first responder stays with the patient to begin compressions.
- Staff will meet the EMS team at the appropriate entrance and direct them to the patient.
First Responder
- Determine responsiveness and absent or abnormal breathing.
- Send someone to activate EMS and get defibrillator/AED.
- If pulseless, begin chest compressions at a depth of at least 2 in. and a rate of at least 100 compressions/min until defibrillator/AED arrives. Allow for complete chest recoil, minimize interruptions to
Second Responder
- After activating EMS, take cart with defibrillator/AED to the patient. Place defibrillator pads or AED on patient and assess cardiac rhythm.
- Shock if indicated, resume compressions. Follow appropriate algorithm according to ACLS guidelines.
Third Responder (if Available)
- Direct remaining patients to another area.
- Direct and control incoming emergency response team and patients.
- Obtain extra supplies and equipment as needed.
- Act as the recorder of events until EMS arrives.
- Prepare records to be sent with patient to the emergency department if needed.
- Notify patient physician/cardiologist and family.
Emergency in Other Locations
7. Protocols should be developed for emergencies occurring in locations other than the cardiac rehabilitation gym including but not limited to:
- Locker room/restrooms
- Lobby/waiting area
- Patient education area
- Parking lots
II. Angina Pectoris
A. If a patient develops unstable angina while in the exercise area, the patient should immediately discontinue exercise and sit or lie down. Note the exercise workload, HR, and BP at which the symptoms occurred.
B. The following protocol should be followed by the CR staff:
- Check pulse, BP, cardiac rhythm (attach telemetry monitor if not already monitored), and oxygen saturation.
- Rate angina on a scale of 1 to 10.
- If no relief with 1 to 3 min of rest, give 1 nitroglycerine (NTG) 0.4 mg SL or spray.
- Obtain 12-lead ECG and call supervising physician.
C. If pain is relieved:
- If this angina is of new onset, the patient should be evaluated by the supervising physician. The primary care physician should be notified of the results of the evaluation and recommended treatment, if any.
- If the patient experiences chronic stable angina, exercise intensity should be decreased or halted until the angina is relieved. Patient may resume exercise at a lower workload dependent on the clinical judgment of the medical director and professional staff.
OR
The patient can be discharged but should be instructed to report any increase in frequency or severity of angina to their physician.
D. If pain is not relieved:
- Monitor pulse, BP, cardiac rhythm, and oxygen saturation closely.
- Place on oxygen at 2 to 4 L per nasal prongs if oxygen saturation is <94%.
- Patient to chew aspirin 160 to 325 mg.
- Repeat NTG 0.4 mg SL or spray every 5 min for unrelieved angina symptoms.
- The supervising physician will evaluate and determine the course of action.
III. Hypoglycemia
A. If patient displays any symptoms of hypoglycemia:
- Obtain finger-stick blood glucose level.
- If BG results are
- Retest BG in 15 min. If BG is not >90 mg/dL, repeat 15 g CHO and recheck BG in 15 min.
- If patient is uncooperative or unconscious, contact supervising physician, give glucose gel or establish IV access and give 50 cc (1 amp) 50% dextrose solution. Arrange for transport to ED.
IV. Hyperglycemia
A. A participant with a BG >300 mg/dL should not exercise unless the patient's referring physician and the program medical director give their consent.
B. Frequency of BG checks should be determined according to the patient profile and ITP.
C. BG evaluations may be performed by rehabilitation staff or the patient according to the ITP.
D. The CR staff may request a blood glucose evaluation on any patient based on suspected signs and symptoms of hyperglycemia (nausea, flushing, polyuria, polydipsia, fruity breath, tachypnea).
V. Hypotension
A. Remove the patient from the exercise area if possible.
B. Place patient in a supine position. Consider elevating legs or placing in Trendelenburg position.
C. Attach a telemetry monitor if not already monitored.
D. Check BP, pulse, cardiac rhythm, and oxygen saturation.
E. If no response to the position change, call the supervising physician. If the patient condition continues to deteriorate or becomes progressively symptomatic, or if BP continues to drop, start an IV of normal saline at 100 mL/h and arrange for transport to the ED. After evaluation and treatment of the patient, the supervising physician should notify the patient's primary care physician of the hypotensive episode and discuss any further treatment if necessary.
F. If patient responds to the supine position, keep supine until SBP is >100, then gradually assist to sitting position. Continue to monitor BP, pulse, and rhythm. Encourage fluids. Notify the patient's primary physician of the episode.
VI. Hypertension
A. Check every patient's BP before exercise and compare with previous recordings.
B. If the SBP reading is >170 mm Hg or the diastolic reading is >100 mm Hg, have the patient sit and recheck the BP in 5 min.
C. If the BP remains elevated, do not have patient exercise. Notify the primary care physician or supervising physician to evaluate and determine course of action.
D. Patients may exercise with elevated BP if directed by the primary care physician and medical director.
E. Investigate whether patient is complying with medications and sodium restrictions.
VII. Dysrhythmias
Premature Ventricular Contractions (PVCs)
A. Observe for the following:
- Frequency
- Whether multifocal or unifocal
- Pairs or runs, sustained or paroxysmal
- Associated signs or symptoms
- Palpate pulse to evaluate for peripheral perfusion
B. Document any new arrhythmias or increase in severity with a rhythm strip and make notation on chart. Notify supervising physician and referring physician, where appropriate, to discuss treatment.
C. Discontinue exercise if PVCs become symptomatic and check pulse, BP, and oxygen saturation. Provide oxygen at 2 to 4 L if hypoxemic, and obtain IV access if directed by a physician.
D. Notify the supervising physician for evaluation and treatment.
Bradycardia
A. If patient develops symptomatic bradycardia, stop exercise.
B. Monitor HR and rhythm, BP, and oximetry. Provide oxygen at 2 to 4 L if hypoxemic. Obtain 12-lead ECG if available.
C. Assess for symptoms of instability or altered mental status, ischemic chest discomfort, HF, or hypotension and notify supervising physician for evaluation and treatment. Notify the supervising physician and if available, obtain IV access, and prepare to administer atropine or external pacing per ACLS guidelines.
D. Prepare for transfer to ED.
Tachycardia
A. If patient develops a new wide or narrow complex tachycardia, stop exercise.
B. Monitor HR and rhythm, BP, and oximetry. Provide oxygen at 2 to 4 L if hypoxemic. Obtain 12-lead ECG if available.
C. Assess for symptoms of instability or altered mental status, ischemic chest discomfort, HF, or hypotension, and notify supervising physician for evaluation and treatment. If directed by a physician, obtain IV access and prepare for synchronized cardioversion. If stable, may utilize vagal maneuvers or antiarrhythmic agents per ACLS guidelines.
D. Prepare for transfer to ED.
VIII. Dyspnea
A. If patient develops acute dyspnea, stop exercise and have patient sit down.
B. Monitor heart rate and rhythm, BP, respiratory rate, lung sounds, and oximetry. Provide oxygen at 2 to 4 L for oxygen saturation <94%.
C. If patient has a metered-dose inhaler, it may be administered as prescribed.
D. If condition deteriorates, notify supervising physician to evaluate for treatment options and possible transfer to ED.
E. If condition improves, notify primary care physician for further recommendations.
IX. Cerebrovascular Accident
A. If patient develops signs and symptoms of a stroke such as sudden arm or leg weakness, confusion, trouble speaking, dizziness, loss of balance or coordination, severe headache, or facial droop, immediately evaluate with rapid out-of-hospital stroke assessment.
B. If stroke is suspected, initiate EMS for immediate transport to a stroke facility.
C. Establish time of last known neurological baseline.
D. Maintain airway, breathing, and circulation.
E. Provide supplemental oxygen if hypoxemic or if oxygen saturation is unknown.
F. Check blood glucose.
G. Alert receiving hospital when patient is in transport.
X. Placement of IV Line
Purpose: To provide immediate access to administer emergency medication and IV fluids.
A. An attempt will be made to notify the supervising physician.
B. Place a saline lock in participant when one or more of the following apply:
- Angina pectoris protocol has been followed and chest pain persists.
- ECG, vital signs or participant appears to be clinically unstable or symptomatic.
- Physician directs the placement of IV line.
XI. Patient Transportation
Staff will meet and direct ambulance personnel to the patient treatment area.
Staff will prepare medical records to be sent with the patient as needed.
Staff will alert the emergency department of the patient transfer.
Cardiac Rehabilitation Department Emergency Procedures and Standing Orders Were Reviewed and Approved
___________________________________________
Physician's name
___________________________________________
Signature
___________________________________________
Date of most recent review
*Appendix B should be used only as an example of standing orders that might be considered and adopted for use in freestanding outpatient or community-based programs.
From American Association of Cardiovascular and Pulmonary Rehabilitation, Guidelines for Cardiac Rehabilitation Programs, 6th ed.
(Champaign, IL: Human Kinetics, 2021).
What are cardiac dysrhythmias?
By Alison L. Bailey, Alexis L. Beatty, Brian Carlin, Dennis J. Kerrigan, Steven J. Keteyian, Kirstine Laerum Sibilitz, Karen Lui, Ryan Mays, Jonathan Powell, Ray W. Squires, Diane J. Treat-Jacobson
Cardiac dysrhythmias are abnormalities in heart rhythm. They are also known as arrhythmias or irregular rhythms. Many CR participants have a history of cardiac dysrhythmias, and some experience dysrhythmias during CR participation.1-3 Symptoms from dysrhythmias may or may not be present and vary from patient to patient. The effects of dysrhythmias can range from generally benign to potentially harmful. Most studies report a cardiac arrest rate of approximately 1/100,000 patient-hours of CR participation.4-7 Although it is rare for dysrhythmias to have life-threatening consequences during exercise in CR programs, it remains important to recognize dysrhythmias and their features.
Bottom Line
Cardiac dysrhythmias are common in CR participants. Life-threatening consequences of cardiac dysrhythmias are rare during exercise in CR programs.
The following are commonly encountered dysrhythmias and symptoms:
Cardiac Dysrhythmias in CR
Generally Benign
- Premature atrial complexes (PACs)
- Isolated premature ventricular complexes (PVCs)
- AF or atrial flutter with controlled ventricular rate (8
- Paroxysmal supraventricular tachycardia (SVT)
- Mild bradycardia (50-60 bpm)
- First-degree atrioventricular (AV) block and asymptomatic type I second-degree (also known as Wenckebach) AV block
Potentially or Likely Harmful
- AF or atrial flutter with a rapid rate (≥110 bpm at rest)
- Symptomatic or severe bradycardia (HR <50)
- Symptomatic or advanced AV block (type II second-degree AV block or complete heart block)
- Ventricular tachycardia
- Ventricular fibrillation
Symptoms Associated With Cardiac Dysrhythmias
Stable Symptoms
- Palpitations
- Dizziness or lightheadedness
- Shortness of breath
- Chest pain or discomfort
Nonspecific or Associated Symptoms
- Weakness or fatigue
- Sweating
- Blurred vision
- Nausea
- Anxiety
- Edema
Unstable Symptoms
- Hypotension
- Near-syncope or loss of consciousness
- HF
- Unstable angina or MI
- Cardiac arrest
Exercise induces many physiologic effects, which can have both direct and indirect effects on cardiac electrophysiology. Exercise intensity can be related to the occurrence of dysrhythmias. Some dysrhythmias diminish or disappear with increasing exercise intensity; others increase or appear with increasing exercise intensity; and still others have no observable relationship to exercise intensity. Factors that can contribute to dysrhythmias during exercise include autonomic nervous system activity, ischemia, genetic abnormalities, structural heart disease, medications with proarrhythmic side effects, electrolyte imbalance, dehydration, and certain environmental factors.
Guideline 10.7 Dysrhythmia Exercise Prescription
For patients with known dysrhythmias, the exercise prescription should be tailored to the individual, with predetermined goals and criteria for exercise termination. Exercise should be terminated when a patient experiences a potentially harmful dysrhythmia or dysrhythmia with unstable symptoms.
Atrial Fibrillation
Light-to-moderate activities, particularly leisure-time activity and walking, are associated with a significantly lower incidence of AF in older adults.9 However, people who participate in extreme endurance training and sports activities may have an increased incidence of AF.10,11 For those diagnosed with AF, regular moderate PA is known to increase exercise capacity and control ventricular rate.12,13 In addition, exercise training increases exercise capacity and may reduce AF burden.14,15 The following information provides specific information about CR participation in patients who have AF.
AF originates in the atrium and is the most common cardiac arrhythmia. It is characterized by irregular contractions of the muscle fibers of the atria resulting in a variable HR. Risk factors associated with developing AF include PA, obesity, advanced age, HTN, HF, diabetes mellitus, CVD and valvular heart disease, left ventricular and atrial enlargement, and hyperthyroidism.43 Paradoxically, despite having few risk factors, athletes are also at increased risk for developing AF.
CR professionals will encounter these two types of patients with AF: patients who experience an initial (acute) onset (often noted during CR check-in or during exercise) and patients previously diagnosed and medically managed. Generally, AF is classified as (1) paroxysmal, (2) persistent, (3) long-standing persistent, or (4) permanent.2
AF should be considered when a patient presents with a rapid (often >110 bpm) “irregularly irregular” (no rhythmic pattern) resting HR. Patients experiencing an abrupt onset of AF may or may not report accompanying symptoms including palpitation, tachycardia, fatigue, shortness of breath, dizziness, and nausea. If AF is suspected, an ECG will confirm a diagnosis.
If new-onset AF is confirmed, the patient's physician should be consulted. Treating new-onset AF has three goals.44,50 The first goal is to mitigate symptoms by initially focusing in on reducing HR. Typical therapeutic HR reduction options include beta-adrenergic and calcium channel blocking agents and antiarrhythmic medication. The second goal is to reduce the risk for the development embolization of a blood clot (which the patient is at risk of developing due to atrial blood stagnation) through anticoagulation therapy. The third goal is to manage the patient's cardiovascular risk factors, which for overweight or obese patients is recommended to include weight loss and risk factor modification.50
Safety and rates of adverse event of exercise in patients have not been well studied. No large randomized control trials of exercise training and AF have assessed safety and efficacy. Guidelines for the treatment of patients with AF do not explicitly endorse specific exercise recommendations. Exercise, however, is not contraindicated in patients with AF. Moreover, exercise is effective treatment in multiple risk factors associated with AF, such as physical inactivity, HTN, diabetes mellitus, and obesity. Therefore, asymptomatic patients with AF who have received medical clearance should be encouraged to participate in an exercise program.
However, AF can profoundly impact the physiologic response to exercise training.45 In particular, the rapid, irregular contraction of the atrium results in reduced ventricular output. To compensate for the reduced cardiac output there is a commensurate increase in the rate and irregularity of ventricular contraction. Despite the negative impact of AF, exercise training studies have demonstrated improvements in functional capacity, health status, and quality of life.46
The special consideration regarding exercise testing and prescription for patients with AF have been detailed elsewhere.3 The following section is a brief review of special considerations regarding exercise testing and prescription for CR participants with AF.
Exercise Testing
As with all patients entering CR, undergoing a symptom-limited exercise tolerance test prior to initiating an exercise training program is optimal but not required. An exercise test is useful to assess for myocardial ischemia, evaluate chronotropic response, identify signs and symptoms, quantify functional capacity, and establish some general parameters for exercise training intensity.
Exercise Prescription for Patients With AF
Currently, no specific recommendations exist regarding exercise training for the treatment of AF. Studies of exercise training in patients with AF have employed a variety of protocols. Components of any exercise prescription include frequency, intensity, duration, modality, progression, and total volume. The exercise prescription for patients with AF should be individualized. A meta-analysis of exercise training studies involving people with AF recommends that a training regimen should include three or more sessions per week of a combination of moderate-intensity aerobic activity and resistance training. Session duration should be approximately 60 minutes, including adequate warm-up and cool-down.
By definition, the HR for a person with AF is irregular. Therefore, use of HR exclusively to assess exercise intensity is problematic. For aerobic training, in lieu of HR, use of RPE scale is an effective means to assess exercise intensity. A rating of 11 to 14 (on the Borg 6-20 scale) is typically associated with a moderate intensity that is approximately 70% to 85% of peak exercise capacity. Notably, very few studies have focused on the safety and efficacy of high-intensity aerobic training in patients with AF.
For overweight patients with AF, weight loss is recommended.47,50 To facilitate weight loss, orienting the exercise prescription to maximize caloric expenditure is indicated. High caloric exercise training (e.g., treadmill walking at a moderate intensity for an extended duration) in CR is well tolerated and an effective strategy to promote weight loss and improve multiple cardiovascular risk factors.48
No specific guidelines exist for resistance training for patients with AF. Given the lack of recommendations, using professional discretion is necessary when providing guidance regarding resistance training. Following the resistance training recommendations for other, non-AF CR participants is advisable. General recommendations for resistance training are found in chapter 6.
Considerations for the prescription of exercise and physical activity
By Jonathan Myers
Guideline 6.1 Considerations for the Prescription of Exercise and Physical Activity
When developing an exercise prescription, consider the following factors:
Safety Factors
- Clinical history
- Risks associated with CVD progression or instability
- Ischemic and angina thresholds
- Cognitive or psychological impairment
Associated Factors
- Vocational or avocational requirements
- Orthopedic limitations
- Previous and current activities
- Personal health and fitness goals
An important initial consideration in exercise planning is safety. Safety considerations apply to both structured exercise training and leisure-time PA. While most patients can engage in exercise without incurring undue risks, appropriate risk stratification should be performed. Guideline 6.1 provides key variables to consider when developing an exercise prescription. Safety and risk stratification are discussed in detail in chapters 4 and 5. Recommendations for supervision and ECG monitoring can be found in chapter 5. Later in this chapter, tables 6.1 and 6.2 present basic principles of exercise prescription. A model for risk stratification for cardiovascular events is outlined in the sidebar Stratification of Risk for Cardiac Events During Exercise Participation in chapter 5. After risk stratification, recommendations for supervision, ECG, monitoring and prescribed intensity and duration of exercise training can be made.
Comprehensive, evidence-based recommendations for structured exercise training in CR are available from several prominent organizations1,3,8 and are only summarized here. A comprehensive exercise program includes cardiorespiratory, musculoskeletal, and flexibility components. Specific elements for each component are summarized in the tables in this chapter and include guidelines for intensity, duration, frequency, and type of exercise for training. Each of the elements should be prescribed relative to one another and in a way that effectively addresses predefined training goals (e.g., increased aerobic or musculoskeletal fitness, weight reduction, control of blood glucose, or resumption of occupation).
Cardiorespiratory Endurance Training
Cardiorespiratory endurance training should be the foundation of most exercise routines for adults with or at risk for CVD. This type of exercise training is the most effective way to increase CRF. Elements of an exercise prescription for increasing CRF are presented in table 6.1. The relative training intensity may vary between 40% and 80% of maximal heart rate reserve (HRR) or metabolic reserve (V.O2R). Initially, programs should focus on the lower part of the intensity range, with progression to higher intensities as patients adapt to the program.7 RPE (e.g., Borg Scale of Perceived Exertion 6-20; Borg CR10 Scale; Omni Picture System of Perceived Exertion) are considered adjunctive to HR monitoring, but they may become more important as a subjective intensity guide as patients gain experience with exercise training and learn how to use the scale. Exercise training duration varies as a function of the overall energy expenditure goals of the patient. A minimum of 20 continuous minutes of exercise per session is commonly recommended within structured programs, although some patients may follow an intermittent (i.e., interval) exercise regimen. Some patients may need to accumulate shorter bouts (e.g., multiple 10 min bouts) throughout the day due to comorbidities, symptoms such as claudication or musculoskeletal discomfort, or lifestyle factors. Ideally, patients should be active most days of the week,1-7,9 but structured programs are often designed with a frequency of two to four sessions per week.
Once the initial exercise prescription is established, patients should progress gradually toward predefined or redefined program goals. There is no set format with respect to progression because many factors, including fitness level, motivation, and orthopedic limitations, influence the rate at which a patient may progress. In general, it is prudent to change one component and provide some time (a minimum of one exercise session) to assess the adaptation to the new level before progressing further. When time permits, increases in duration and frequency should precede increases in intensity. Modest increases in intensity, when appropriate, are likely to be tolerated and should be based on the observations of the staff and subjective responses of the patient, provided that the changes remain within the limits specified in the most recent evaluation.
A guiding principle should be progression of the total volume or dose of exercise such that the patient achieves desired energy expenditure thresholds within a three- to six-month period. Therefore, given that most patients' participation in CR lasts no longer than three months, it is important to educate and encourage patients to continue exercising even after CR participation has ended. The most appropriate volume of exercise depends on the individual CVD risk profile, training goals, and comorbidities (i.e., diabetes, hypertension, obesity, arthritis). An accumulating body of evidence has affirmed a dose-response relationship between the volume of PA and health outcomes.1,3,6-8 Whether exercise has a role in reversing coronary artery disease is an issue that remains controversial; however, thresholds of approximately 1,500 and 2,200 kcal/week are associated with stability and regression of coronary artery lesions, respectively.18 Notably, multiple studies document that energy expenditure in structured CR does not typically meet either of these thresholds.11-14 Therefore, patients will likely need to engage in PA outside of the structured program to achieve the optimal levels of energy expenditure.
Few studies have supported the efficacy of structured exercise training as a singular strategy to normalize body weight and body composition in patients with CVD. This underscores the importance of multiple behavioral strategies in weight reduction programming for overweight patients. Studies show that achieving weight loss goals requires a simultaneous change in dietary habits in addition to greater physical activity patterns. The volume or dose of exercise associated with the typical CR training session may be a limiting factor, and there is only a 1 to 2 kg weight loss during CR participation. It is likely part of the explanation for a low amount of weight loss during CR is due to a lack of focus on helping patients lose weight. As mentioned previously, numerous studies have shown the weekly dose to be inadequate for weight or fat reduction. As an example, a typical exercise session for an outpatient with a peak functional capacity of 7 METs might be 30 min at a heart rate that would equate with about 4 METs. The following formula provides a method to estimate the caloric costs of the exercise session:
Calories/min = [METs × body weight in kg × 3.5] / 200
It should be noted that the 4 MET value in this example includes the resting energy expenditure component (1 MET). Therefore, the net caloric cost of the exercise would be based on only 3 METs. If the hypothetical patient in this example weighed 100 kg (220 lb) and exercised 3 days per week for 30 min, the net caloric expenditure would be approximately 480 kcal/week (5.3 kcal/min × 30 min × 3 days/week). Although patients can clearly improve exercise tolerance with this regimen, the estimated caloric expenditure falls well short of contemporary recommendations for PA and in most cases would not be effective for weight or fat loss.15 For example, 40 min sessions, five times per week, would result in an expenditure of approximately 1,060 kcal per week. Again, this calculation highlights the importance of increasing PA outside of the structured or in-hospital program. Thus, adjustments must be made about frequency and duration of exercise to allow patients to achieve greater energy expenditures to enhance program outcomes. However, these adjustments must be with the caveat that although it is prudent to increase exercise volume progressively, staff must carefully consider the risk that a higher-volume program may lead to higher dropout rates. Therefore, overweight patients must be educated about the need to develop and maintain fitness as the core of their exercise regimen, with the additional volume of PA facilitating weight loss and other goals. Finally, as CRF improves, patients are able to exercise at a higher metabolic rate (more kcal/min) at a given relative intensity (% maximal HRR). This adjustment allows patients to accumulate a greater caloric deficit over time.
Example of standing orders to initiate outpatient cardiac rehabilitation
Appendix A: Example of Standing Orders to Initiate Outpatient CR
- Initiate monitored exercise program per outpatient CR policies and procedures.
- Determine target heart rate (THR) via sign- or symptom-limited graded exercise testing (GXT) or sign- or symptom-limited responses to submaximal exercise.
- Begin with a training duration of up to 30 min to tolerance, one to five times a week.
- Gradually increase duration of training exercise if patient cardiovascular and physiological responses are within normal limits.
- Observe participant for signs of exercise intolerance and adapt or terminate exercise as indicated in policies and procedures.
- Assess lipid profile approximately six weeks postevent.
- Administer nitroglycerin 0.3 or 0.4 mg sublingually every 5 minutes × 3 as needed for angina discomfort or ischemic symptoms.
- Provide regular, periodic progress reports to the referring physician. Provide copies of reports to other physicians as needed.
- Initiate patient education and counseling sessions as patient needs indicate.
- Consult patient's personal physician or CR supervising physician for any necessary orders.
- Consult with the CR dietitian to provide individualized nutrition education for each participant.
- Enter the patient into a non-ECG-monitored maintenance program upon completion of early outpatient CR program.
__________________________________________________________________________________________
Physician's signature
___________________________________________
Date
From American Association of Cardiovascular and Pulmonary Rehabilitation, Guidelines for Cardiac Rehabilitation Programs, 6th ed.
(Champaign, IL: Human Kinetics, 2021).
Appendix B: Example of Outpatient CR Emergency Standing Orders*
Table of Contents
Protocols for Urgent Situations and Emergency Interventions in the Cardiac Rehabilitation Area
I. Cardiopulmonary arrest
II. Angina pectoris
III. Hypoglycemia
IV. Hyperglycemia
V. Hypotension
VI. Hypertension
VII. Dysrhythmias
VIII. Dyspnea
IX. Cerebrovascular accident
X. Placement of intravenous line
XI. Patient transportation
I. Cardiopulmonary Arrest
A. Identify responsiveness and determine if breathing is absent or abnormal (gasping).
B. Call out for help/activate emergency medical system (EMS).
- Call out for help from coworker. If no one responds and if no other staff member is available to assist, go to the nearest phone and activate EMS. (Emergency numbers with specific scripted instructions are posted at each phone.) Get defibrillator/automated external defibrillator (AED). If no pulse, attach defibrillator/AED and shock if indicated. Begin cardiopulmonary resuscitation (CPR) with compressions.
- If a second responder is available to assist, that person should activate EMS and then get the defibrillator/AED while the first responder stays with the patient to begin compressions.
- Staff will meet the EMS team at the appropriate entrance and direct them to the patient.
First Responder
- Determine responsiveness and absent or abnormal breathing.
- Send someone to activate EMS and get defibrillator/AED.
- If pulseless, begin chest compressions at a depth of at least 2 in. and a rate of at least 100 compressions/min until defibrillator/AED arrives. Allow for complete chest recoil, minimize interruptions to
Second Responder
- After activating EMS, take cart with defibrillator/AED to the patient. Place defibrillator pads or AED on patient and assess cardiac rhythm.
- Shock if indicated, resume compressions. Follow appropriate algorithm according to ACLS guidelines.
Third Responder (if Available)
- Direct remaining patients to another area.
- Direct and control incoming emergency response team and patients.
- Obtain extra supplies and equipment as needed.
- Act as the recorder of events until EMS arrives.
- Prepare records to be sent with patient to the emergency department if needed.
- Notify patient physician/cardiologist and family.
Emergency in Other Locations
7. Protocols should be developed for emergencies occurring in locations other than the cardiac rehabilitation gym including but not limited to:
- Locker room/restrooms
- Lobby/waiting area
- Patient education area
- Parking lots
II. Angina Pectoris
A. If a patient develops unstable angina while in the exercise area, the patient should immediately discontinue exercise and sit or lie down. Note the exercise workload, HR, and BP at which the symptoms occurred.
B. The following protocol should be followed by the CR staff:
- Check pulse, BP, cardiac rhythm (attach telemetry monitor if not already monitored), and oxygen saturation.
- Rate angina on a scale of 1 to 10.
- If no relief with 1 to 3 min of rest, give 1 nitroglycerine (NTG) 0.4 mg SL or spray.
- Obtain 12-lead ECG and call supervising physician.
C. If pain is relieved:
- If this angina is of new onset, the patient should be evaluated by the supervising physician. The primary care physician should be notified of the results of the evaluation and recommended treatment, if any.
- If the patient experiences chronic stable angina, exercise intensity should be decreased or halted until the angina is relieved. Patient may resume exercise at a lower workload dependent on the clinical judgment of the medical director and professional staff.
OR
The patient can be discharged but should be instructed to report any increase in frequency or severity of angina to their physician.
D. If pain is not relieved:
- Monitor pulse, BP, cardiac rhythm, and oxygen saturation closely.
- Place on oxygen at 2 to 4 L per nasal prongs if oxygen saturation is <94%.
- Patient to chew aspirin 160 to 325 mg.
- Repeat NTG 0.4 mg SL or spray every 5 min for unrelieved angina symptoms.
- The supervising physician will evaluate and determine the course of action.
III. Hypoglycemia
A. If patient displays any symptoms of hypoglycemia:
- Obtain finger-stick blood glucose level.
- If BG results are
- Retest BG in 15 min. If BG is not >90 mg/dL, repeat 15 g CHO and recheck BG in 15 min.
- If patient is uncooperative or unconscious, contact supervising physician, give glucose gel or establish IV access and give 50 cc (1 amp) 50% dextrose solution. Arrange for transport to ED.
IV. Hyperglycemia
A. A participant with a BG >300 mg/dL should not exercise unless the patient's referring physician and the program medical director give their consent.
B. Frequency of BG checks should be determined according to the patient profile and ITP.
C. BG evaluations may be performed by rehabilitation staff or the patient according to the ITP.
D. The CR staff may request a blood glucose evaluation on any patient based on suspected signs and symptoms of hyperglycemia (nausea, flushing, polyuria, polydipsia, fruity breath, tachypnea).
V. Hypotension
A. Remove the patient from the exercise area if possible.
B. Place patient in a supine position. Consider elevating legs or placing in Trendelenburg position.
C. Attach a telemetry monitor if not already monitored.
D. Check BP, pulse, cardiac rhythm, and oxygen saturation.
E. If no response to the position change, call the supervising physician. If the patient condition continues to deteriorate or becomes progressively symptomatic, or if BP continues to drop, start an IV of normal saline at 100 mL/h and arrange for transport to the ED. After evaluation and treatment of the patient, the supervising physician should notify the patient's primary care physician of the hypotensive episode and discuss any further treatment if necessary.
F. If patient responds to the supine position, keep supine until SBP is >100, then gradually assist to sitting position. Continue to monitor BP, pulse, and rhythm. Encourage fluids. Notify the patient's primary physician of the episode.
VI. Hypertension
A. Check every patient's BP before exercise and compare with previous recordings.
B. If the SBP reading is >170 mm Hg or the diastolic reading is >100 mm Hg, have the patient sit and recheck the BP in 5 min.
C. If the BP remains elevated, do not have patient exercise. Notify the primary care physician or supervising physician to evaluate and determine course of action.
D. Patients may exercise with elevated BP if directed by the primary care physician and medical director.
E. Investigate whether patient is complying with medications and sodium restrictions.
VII. Dysrhythmias
Premature Ventricular Contractions (PVCs)
A. Observe for the following:
- Frequency
- Whether multifocal or unifocal
- Pairs or runs, sustained or paroxysmal
- Associated signs or symptoms
- Palpate pulse to evaluate for peripheral perfusion
B. Document any new arrhythmias or increase in severity with a rhythm strip and make notation on chart. Notify supervising physician and referring physician, where appropriate, to discuss treatment.
C. Discontinue exercise if PVCs become symptomatic and check pulse, BP, and oxygen saturation. Provide oxygen at 2 to 4 L if hypoxemic, and obtain IV access if directed by a physician.
D. Notify the supervising physician for evaluation and treatment.
Bradycardia
A. If patient develops symptomatic bradycardia, stop exercise.
B. Monitor HR and rhythm, BP, and oximetry. Provide oxygen at 2 to 4 L if hypoxemic. Obtain 12-lead ECG if available.
C. Assess for symptoms of instability or altered mental status, ischemic chest discomfort, HF, or hypotension and notify supervising physician for evaluation and treatment. Notify the supervising physician and if available, obtain IV access, and prepare to administer atropine or external pacing per ACLS guidelines.
D. Prepare for transfer to ED.
Tachycardia
A. If patient develops a new wide or narrow complex tachycardia, stop exercise.
B. Monitor HR and rhythm, BP, and oximetry. Provide oxygen at 2 to 4 L if hypoxemic. Obtain 12-lead ECG if available.
C. Assess for symptoms of instability or altered mental status, ischemic chest discomfort, HF, or hypotension, and notify supervising physician for evaluation and treatment. If directed by a physician, obtain IV access and prepare for synchronized cardioversion. If stable, may utilize vagal maneuvers or antiarrhythmic agents per ACLS guidelines.
D. Prepare for transfer to ED.
VIII. Dyspnea
A. If patient develops acute dyspnea, stop exercise and have patient sit down.
B. Monitor heart rate and rhythm, BP, respiratory rate, lung sounds, and oximetry. Provide oxygen at 2 to 4 L for oxygen saturation <94%.
C. If patient has a metered-dose inhaler, it may be administered as prescribed.
D. If condition deteriorates, notify supervising physician to evaluate for treatment options and possible transfer to ED.
E. If condition improves, notify primary care physician for further recommendations.
IX. Cerebrovascular Accident
A. If patient develops signs and symptoms of a stroke such as sudden arm or leg weakness, confusion, trouble speaking, dizziness, loss of balance or coordination, severe headache, or facial droop, immediately evaluate with rapid out-of-hospital stroke assessment.
B. If stroke is suspected, initiate EMS for immediate transport to a stroke facility.
C. Establish time of last known neurological baseline.
D. Maintain airway, breathing, and circulation.
E. Provide supplemental oxygen if hypoxemic or if oxygen saturation is unknown.
F. Check blood glucose.
G. Alert receiving hospital when patient is in transport.
X. Placement of IV Line
Purpose: To provide immediate access to administer emergency medication and IV fluids.
A. An attempt will be made to notify the supervising physician.
B. Place a saline lock in participant when one or more of the following apply:
- Angina pectoris protocol has been followed and chest pain persists.
- ECG, vital signs or participant appears to be clinically unstable or symptomatic.
- Physician directs the placement of IV line.
XI. Patient Transportation
Staff will meet and direct ambulance personnel to the patient treatment area.
Staff will prepare medical records to be sent with the patient as needed.
Staff will alert the emergency department of the patient transfer.
Cardiac Rehabilitation Department Emergency Procedures and Standing Orders Were Reviewed and Approved
___________________________________________
Physician's name
___________________________________________
Signature
___________________________________________
Date of most recent review
*Appendix B should be used only as an example of standing orders that might be considered and adopted for use in freestanding outpatient or community-based programs.
From American Association of Cardiovascular and Pulmonary Rehabilitation, Guidelines for Cardiac Rehabilitation Programs, 6th ed.
(Champaign, IL: Human Kinetics, 2021).
What are cardiac dysrhythmias?
By Alison L. Bailey, Alexis L. Beatty, Brian Carlin, Dennis J. Kerrigan, Steven J. Keteyian, Kirstine Laerum Sibilitz, Karen Lui, Ryan Mays, Jonathan Powell, Ray W. Squires, Diane J. Treat-Jacobson
Cardiac dysrhythmias are abnormalities in heart rhythm. They are also known as arrhythmias or irregular rhythms. Many CR participants have a history of cardiac dysrhythmias, and some experience dysrhythmias during CR participation.1-3 Symptoms from dysrhythmias may or may not be present and vary from patient to patient. The effects of dysrhythmias can range from generally benign to potentially harmful. Most studies report a cardiac arrest rate of approximately 1/100,000 patient-hours of CR participation.4-7 Although it is rare for dysrhythmias to have life-threatening consequences during exercise in CR programs, it remains important to recognize dysrhythmias and their features.
Bottom Line
Cardiac dysrhythmias are common in CR participants. Life-threatening consequences of cardiac dysrhythmias are rare during exercise in CR programs.
The following are commonly encountered dysrhythmias and symptoms:
Cardiac Dysrhythmias in CR
Generally Benign
- Premature atrial complexes (PACs)
- Isolated premature ventricular complexes (PVCs)
- AF or atrial flutter with controlled ventricular rate (8
- Paroxysmal supraventricular tachycardia (SVT)
- Mild bradycardia (50-60 bpm)
- First-degree atrioventricular (AV) block and asymptomatic type I second-degree (also known as Wenckebach) AV block
Potentially or Likely Harmful
- AF or atrial flutter with a rapid rate (≥110 bpm at rest)
- Symptomatic or severe bradycardia (HR <50)
- Symptomatic or advanced AV block (type II second-degree AV block or complete heart block)
- Ventricular tachycardia
- Ventricular fibrillation
Symptoms Associated With Cardiac Dysrhythmias
Stable Symptoms
- Palpitations
- Dizziness or lightheadedness
- Shortness of breath
- Chest pain or discomfort
Nonspecific or Associated Symptoms
- Weakness or fatigue
- Sweating
- Blurred vision
- Nausea
- Anxiety
- Edema
Unstable Symptoms
- Hypotension
- Near-syncope or loss of consciousness
- HF
- Unstable angina or MI
- Cardiac arrest
Exercise induces many physiologic effects, which can have both direct and indirect effects on cardiac electrophysiology. Exercise intensity can be related to the occurrence of dysrhythmias. Some dysrhythmias diminish or disappear with increasing exercise intensity; others increase or appear with increasing exercise intensity; and still others have no observable relationship to exercise intensity. Factors that can contribute to dysrhythmias during exercise include autonomic nervous system activity, ischemia, genetic abnormalities, structural heart disease, medications with proarrhythmic side effects, electrolyte imbalance, dehydration, and certain environmental factors.
Guideline 10.7 Dysrhythmia Exercise Prescription
For patients with known dysrhythmias, the exercise prescription should be tailored to the individual, with predetermined goals and criteria for exercise termination. Exercise should be terminated when a patient experiences a potentially harmful dysrhythmia or dysrhythmia with unstable symptoms.
Atrial Fibrillation
Light-to-moderate activities, particularly leisure-time activity and walking, are associated with a significantly lower incidence of AF in older adults.9 However, people who participate in extreme endurance training and sports activities may have an increased incidence of AF.10,11 For those diagnosed with AF, regular moderate PA is known to increase exercise capacity and control ventricular rate.12,13 In addition, exercise training increases exercise capacity and may reduce AF burden.14,15 The following information provides specific information about CR participation in patients who have AF.
AF originates in the atrium and is the most common cardiac arrhythmia. It is characterized by irregular contractions of the muscle fibers of the atria resulting in a variable HR. Risk factors associated with developing AF include PA, obesity, advanced age, HTN, HF, diabetes mellitus, CVD and valvular heart disease, left ventricular and atrial enlargement, and hyperthyroidism.43 Paradoxically, despite having few risk factors, athletes are also at increased risk for developing AF.
CR professionals will encounter these two types of patients with AF: patients who experience an initial (acute) onset (often noted during CR check-in or during exercise) and patients previously diagnosed and medically managed. Generally, AF is classified as (1) paroxysmal, (2) persistent, (3) long-standing persistent, or (4) permanent.2
AF should be considered when a patient presents with a rapid (often >110 bpm) “irregularly irregular” (no rhythmic pattern) resting HR. Patients experiencing an abrupt onset of AF may or may not report accompanying symptoms including palpitation, tachycardia, fatigue, shortness of breath, dizziness, and nausea. If AF is suspected, an ECG will confirm a diagnosis.
If new-onset AF is confirmed, the patient's physician should be consulted. Treating new-onset AF has three goals.44,50 The first goal is to mitigate symptoms by initially focusing in on reducing HR. Typical therapeutic HR reduction options include beta-adrenergic and calcium channel blocking agents and antiarrhythmic medication. The second goal is to reduce the risk for the development embolization of a blood clot (which the patient is at risk of developing due to atrial blood stagnation) through anticoagulation therapy. The third goal is to manage the patient's cardiovascular risk factors, which for overweight or obese patients is recommended to include weight loss and risk factor modification.50
Safety and rates of adverse event of exercise in patients have not been well studied. No large randomized control trials of exercise training and AF have assessed safety and efficacy. Guidelines for the treatment of patients with AF do not explicitly endorse specific exercise recommendations. Exercise, however, is not contraindicated in patients with AF. Moreover, exercise is effective treatment in multiple risk factors associated with AF, such as physical inactivity, HTN, diabetes mellitus, and obesity. Therefore, asymptomatic patients with AF who have received medical clearance should be encouraged to participate in an exercise program.
However, AF can profoundly impact the physiologic response to exercise training.45 In particular, the rapid, irregular contraction of the atrium results in reduced ventricular output. To compensate for the reduced cardiac output there is a commensurate increase in the rate and irregularity of ventricular contraction. Despite the negative impact of AF, exercise training studies have demonstrated improvements in functional capacity, health status, and quality of life.46
The special consideration regarding exercise testing and prescription for patients with AF have been detailed elsewhere.3 The following section is a brief review of special considerations regarding exercise testing and prescription for CR participants with AF.
Exercise Testing
As with all patients entering CR, undergoing a symptom-limited exercise tolerance test prior to initiating an exercise training program is optimal but not required. An exercise test is useful to assess for myocardial ischemia, evaluate chronotropic response, identify signs and symptoms, quantify functional capacity, and establish some general parameters for exercise training intensity.
Exercise Prescription for Patients With AF
Currently, no specific recommendations exist regarding exercise training for the treatment of AF. Studies of exercise training in patients with AF have employed a variety of protocols. Components of any exercise prescription include frequency, intensity, duration, modality, progression, and total volume. The exercise prescription for patients with AF should be individualized. A meta-analysis of exercise training studies involving people with AF recommends that a training regimen should include three or more sessions per week of a combination of moderate-intensity aerobic activity and resistance training. Session duration should be approximately 60 minutes, including adequate warm-up and cool-down.
By definition, the HR for a person with AF is irregular. Therefore, use of HR exclusively to assess exercise intensity is problematic. For aerobic training, in lieu of HR, use of RPE scale is an effective means to assess exercise intensity. A rating of 11 to 14 (on the Borg 6-20 scale) is typically associated with a moderate intensity that is approximately 70% to 85% of peak exercise capacity. Notably, very few studies have focused on the safety and efficacy of high-intensity aerobic training in patients with AF.
For overweight patients with AF, weight loss is recommended.47,50 To facilitate weight loss, orienting the exercise prescription to maximize caloric expenditure is indicated. High caloric exercise training (e.g., treadmill walking at a moderate intensity for an extended duration) in CR is well tolerated and an effective strategy to promote weight loss and improve multiple cardiovascular risk factors.48
No specific guidelines exist for resistance training for patients with AF. Given the lack of recommendations, using professional discretion is necessary when providing guidance regarding resistance training. Following the resistance training recommendations for other, non-AF CR participants is advisable. General recommendations for resistance training are found in chapter 6.
Considerations for the prescription of exercise and physical activity
By Jonathan Myers
Guideline 6.1 Considerations for the Prescription of Exercise and Physical Activity
When developing an exercise prescription, consider the following factors:
Safety Factors
- Clinical history
- Risks associated with CVD progression or instability
- Ischemic and angina thresholds
- Cognitive or psychological impairment
Associated Factors
- Vocational or avocational requirements
- Orthopedic limitations
- Previous and current activities
- Personal health and fitness goals
An important initial consideration in exercise planning is safety. Safety considerations apply to both structured exercise training and leisure-time PA. While most patients can engage in exercise without incurring undue risks, appropriate risk stratification should be performed. Guideline 6.1 provides key variables to consider when developing an exercise prescription. Safety and risk stratification are discussed in detail in chapters 4 and 5. Recommendations for supervision and ECG monitoring can be found in chapter 5. Later in this chapter, tables 6.1 and 6.2 present basic principles of exercise prescription. A model for risk stratification for cardiovascular events is outlined in the sidebar Stratification of Risk for Cardiac Events During Exercise Participation in chapter 5. After risk stratification, recommendations for supervision, ECG, monitoring and prescribed intensity and duration of exercise training can be made.
Comprehensive, evidence-based recommendations for structured exercise training in CR are available from several prominent organizations1,3,8 and are only summarized here. A comprehensive exercise program includes cardiorespiratory, musculoskeletal, and flexibility components. Specific elements for each component are summarized in the tables in this chapter and include guidelines for intensity, duration, frequency, and type of exercise for training. Each of the elements should be prescribed relative to one another and in a way that effectively addresses predefined training goals (e.g., increased aerobic or musculoskeletal fitness, weight reduction, control of blood glucose, or resumption of occupation).
Cardiorespiratory Endurance Training
Cardiorespiratory endurance training should be the foundation of most exercise routines for adults with or at risk for CVD. This type of exercise training is the most effective way to increase CRF. Elements of an exercise prescription for increasing CRF are presented in table 6.1. The relative training intensity may vary between 40% and 80% of maximal heart rate reserve (HRR) or metabolic reserve (V.O2R). Initially, programs should focus on the lower part of the intensity range, with progression to higher intensities as patients adapt to the program.7 RPE (e.g., Borg Scale of Perceived Exertion 6-20; Borg CR10 Scale; Omni Picture System of Perceived Exertion) are considered adjunctive to HR monitoring, but they may become more important as a subjective intensity guide as patients gain experience with exercise training and learn how to use the scale. Exercise training duration varies as a function of the overall energy expenditure goals of the patient. A minimum of 20 continuous minutes of exercise per session is commonly recommended within structured programs, although some patients may follow an intermittent (i.e., interval) exercise regimen. Some patients may need to accumulate shorter bouts (e.g., multiple 10 min bouts) throughout the day due to comorbidities, symptoms such as claudication or musculoskeletal discomfort, or lifestyle factors. Ideally, patients should be active most days of the week,1-7,9 but structured programs are often designed with a frequency of two to four sessions per week.
Once the initial exercise prescription is established, patients should progress gradually toward predefined or redefined program goals. There is no set format with respect to progression because many factors, including fitness level, motivation, and orthopedic limitations, influence the rate at which a patient may progress. In general, it is prudent to change one component and provide some time (a minimum of one exercise session) to assess the adaptation to the new level before progressing further. When time permits, increases in duration and frequency should precede increases in intensity. Modest increases in intensity, when appropriate, are likely to be tolerated and should be based on the observations of the staff and subjective responses of the patient, provided that the changes remain within the limits specified in the most recent evaluation.
A guiding principle should be progression of the total volume or dose of exercise such that the patient achieves desired energy expenditure thresholds within a three- to six-month period. Therefore, given that most patients' participation in CR lasts no longer than three months, it is important to educate and encourage patients to continue exercising even after CR participation has ended. The most appropriate volume of exercise depends on the individual CVD risk profile, training goals, and comorbidities (i.e., diabetes, hypertension, obesity, arthritis). An accumulating body of evidence has affirmed a dose-response relationship between the volume of PA and health outcomes.1,3,6-8 Whether exercise has a role in reversing coronary artery disease is an issue that remains controversial; however, thresholds of approximately 1,500 and 2,200 kcal/week are associated with stability and regression of coronary artery lesions, respectively.18 Notably, multiple studies document that energy expenditure in structured CR does not typically meet either of these thresholds.11-14 Therefore, patients will likely need to engage in PA outside of the structured program to achieve the optimal levels of energy expenditure.
Few studies have supported the efficacy of structured exercise training as a singular strategy to normalize body weight and body composition in patients with CVD. This underscores the importance of multiple behavioral strategies in weight reduction programming for overweight patients. Studies show that achieving weight loss goals requires a simultaneous change in dietary habits in addition to greater physical activity patterns. The volume or dose of exercise associated with the typical CR training session may be a limiting factor, and there is only a 1 to 2 kg weight loss during CR participation. It is likely part of the explanation for a low amount of weight loss during CR is due to a lack of focus on helping patients lose weight. As mentioned previously, numerous studies have shown the weekly dose to be inadequate for weight or fat reduction. As an example, a typical exercise session for an outpatient with a peak functional capacity of 7 METs might be 30 min at a heart rate that would equate with about 4 METs. The following formula provides a method to estimate the caloric costs of the exercise session:
Calories/min = [METs × body weight in kg × 3.5] / 200
It should be noted that the 4 MET value in this example includes the resting energy expenditure component (1 MET). Therefore, the net caloric cost of the exercise would be based on only 3 METs. If the hypothetical patient in this example weighed 100 kg (220 lb) and exercised 3 days per week for 30 min, the net caloric expenditure would be approximately 480 kcal/week (5.3 kcal/min × 30 min × 3 days/week). Although patients can clearly improve exercise tolerance with this regimen, the estimated caloric expenditure falls well short of contemporary recommendations for PA and in most cases would not be effective for weight or fat loss.15 For example, 40 min sessions, five times per week, would result in an expenditure of approximately 1,060 kcal per week. Again, this calculation highlights the importance of increasing PA outside of the structured or in-hospital program. Thus, adjustments must be made about frequency and duration of exercise to allow patients to achieve greater energy expenditures to enhance program outcomes. However, these adjustments must be with the caveat that although it is prudent to increase exercise volume progressively, staff must carefully consider the risk that a higher-volume program may lead to higher dropout rates. Therefore, overweight patients must be educated about the need to develop and maintain fitness as the core of their exercise regimen, with the additional volume of PA facilitating weight loss and other goals. Finally, as CRF improves, patients are able to exercise at a higher metabolic rate (more kcal/min) at a given relative intensity (% maximal HRR). This adjustment allows patients to accumulate a greater caloric deficit over time.
Example of standing orders to initiate outpatient cardiac rehabilitation
Appendix A: Example of Standing Orders to Initiate Outpatient CR
- Initiate monitored exercise program per outpatient CR policies and procedures.
- Determine target heart rate (THR) via sign- or symptom-limited graded exercise testing (GXT) or sign- or symptom-limited responses to submaximal exercise.
- Begin with a training duration of up to 30 min to tolerance, one to five times a week.
- Gradually increase duration of training exercise if patient cardiovascular and physiological responses are within normal limits.
- Observe participant for signs of exercise intolerance and adapt or terminate exercise as indicated in policies and procedures.
- Assess lipid profile approximately six weeks postevent.
- Administer nitroglycerin 0.3 or 0.4 mg sublingually every 5 minutes × 3 as needed for angina discomfort or ischemic symptoms.
- Provide regular, periodic progress reports to the referring physician. Provide copies of reports to other physicians as needed.
- Initiate patient education and counseling sessions as patient needs indicate.
- Consult patient's personal physician or CR supervising physician for any necessary orders.
- Consult with the CR dietitian to provide individualized nutrition education for each participant.
- Enter the patient into a non-ECG-monitored maintenance program upon completion of early outpatient CR program.
__________________________________________________________________________________________
Physician's signature
___________________________________________
Date
From American Association of Cardiovascular and Pulmonary Rehabilitation, Guidelines for Cardiac Rehabilitation Programs, 6th ed.
(Champaign, IL: Human Kinetics, 2021).
Appendix B: Example of Outpatient CR Emergency Standing Orders*
Table of Contents
Protocols for Urgent Situations and Emergency Interventions in the Cardiac Rehabilitation Area
I. Cardiopulmonary arrest
II. Angina pectoris
III. Hypoglycemia
IV. Hyperglycemia
V. Hypotension
VI. Hypertension
VII. Dysrhythmias
VIII. Dyspnea
IX. Cerebrovascular accident
X. Placement of intravenous line
XI. Patient transportation
I. Cardiopulmonary Arrest
A. Identify responsiveness and determine if breathing is absent or abnormal (gasping).
B. Call out for help/activate emergency medical system (EMS).
- Call out for help from coworker. If no one responds and if no other staff member is available to assist, go to the nearest phone and activate EMS. (Emergency numbers with specific scripted instructions are posted at each phone.) Get defibrillator/automated external defibrillator (AED). If no pulse, attach defibrillator/AED and shock if indicated. Begin cardiopulmonary resuscitation (CPR) with compressions.
- If a second responder is available to assist, that person should activate EMS and then get the defibrillator/AED while the first responder stays with the patient to begin compressions.
- Staff will meet the EMS team at the appropriate entrance and direct them to the patient.
First Responder
- Determine responsiveness and absent or abnormal breathing.
- Send someone to activate EMS and get defibrillator/AED.
- If pulseless, begin chest compressions at a depth of at least 2 in. and a rate of at least 100 compressions/min until defibrillator/AED arrives. Allow for complete chest recoil, minimize interruptions to
Second Responder
- After activating EMS, take cart with defibrillator/AED to the patient. Place defibrillator pads or AED on patient and assess cardiac rhythm.
- Shock if indicated, resume compressions. Follow appropriate algorithm according to ACLS guidelines.
Third Responder (if Available)
- Direct remaining patients to another area.
- Direct and control incoming emergency response team and patients.
- Obtain extra supplies and equipment as needed.
- Act as the recorder of events until EMS arrives.
- Prepare records to be sent with patient to the emergency department if needed.
- Notify patient physician/cardiologist and family.
Emergency in Other Locations
7. Protocols should be developed for emergencies occurring in locations other than the cardiac rehabilitation gym including but not limited to:
- Locker room/restrooms
- Lobby/waiting area
- Patient education area
- Parking lots
II. Angina Pectoris
A. If a patient develops unstable angina while in the exercise area, the patient should immediately discontinue exercise and sit or lie down. Note the exercise workload, HR, and BP at which the symptoms occurred.
B. The following protocol should be followed by the CR staff:
- Check pulse, BP, cardiac rhythm (attach telemetry monitor if not already monitored), and oxygen saturation.
- Rate angina on a scale of 1 to 10.
- If no relief with 1 to 3 min of rest, give 1 nitroglycerine (NTG) 0.4 mg SL or spray.
- Obtain 12-lead ECG and call supervising physician.
C. If pain is relieved:
- If this angina is of new onset, the patient should be evaluated by the supervising physician. The primary care physician should be notified of the results of the evaluation and recommended treatment, if any.
- If the patient experiences chronic stable angina, exercise intensity should be decreased or halted until the angina is relieved. Patient may resume exercise at a lower workload dependent on the clinical judgment of the medical director and professional staff.
OR
The patient can be discharged but should be instructed to report any increase in frequency or severity of angina to their physician.
D. If pain is not relieved:
- Monitor pulse, BP, cardiac rhythm, and oxygen saturation closely.
- Place on oxygen at 2 to 4 L per nasal prongs if oxygen saturation is <94%.
- Patient to chew aspirin 160 to 325 mg.
- Repeat NTG 0.4 mg SL or spray every 5 min for unrelieved angina symptoms.
- The supervising physician will evaluate and determine the course of action.
III. Hypoglycemia
A. If patient displays any symptoms of hypoglycemia:
- Obtain finger-stick blood glucose level.
- If BG results are
- Retest BG in 15 min. If BG is not >90 mg/dL, repeat 15 g CHO and recheck BG in 15 min.
- If patient is uncooperative or unconscious, contact supervising physician, give glucose gel or establish IV access and give 50 cc (1 amp) 50% dextrose solution. Arrange for transport to ED.
IV. Hyperglycemia
A. A participant with a BG >300 mg/dL should not exercise unless the patient's referring physician and the program medical director give their consent.
B. Frequency of BG checks should be determined according to the patient profile and ITP.
C. BG evaluations may be performed by rehabilitation staff or the patient according to the ITP.
D. The CR staff may request a blood glucose evaluation on any patient based on suspected signs and symptoms of hyperglycemia (nausea, flushing, polyuria, polydipsia, fruity breath, tachypnea).
V. Hypotension
A. Remove the patient from the exercise area if possible.
B. Place patient in a supine position. Consider elevating legs or placing in Trendelenburg position.
C. Attach a telemetry monitor if not already monitored.
D. Check BP, pulse, cardiac rhythm, and oxygen saturation.
E. If no response to the position change, call the supervising physician. If the patient condition continues to deteriorate or becomes progressively symptomatic, or if BP continues to drop, start an IV of normal saline at 100 mL/h and arrange for transport to the ED. After evaluation and treatment of the patient, the supervising physician should notify the patient's primary care physician of the hypotensive episode and discuss any further treatment if necessary.
F. If patient responds to the supine position, keep supine until SBP is >100, then gradually assist to sitting position. Continue to monitor BP, pulse, and rhythm. Encourage fluids. Notify the patient's primary physician of the episode.
VI. Hypertension
A. Check every patient's BP before exercise and compare with previous recordings.
B. If the SBP reading is >170 mm Hg or the diastolic reading is >100 mm Hg, have the patient sit and recheck the BP in 5 min.
C. If the BP remains elevated, do not have patient exercise. Notify the primary care physician or supervising physician to evaluate and determine course of action.
D. Patients may exercise with elevated BP if directed by the primary care physician and medical director.
E. Investigate whether patient is complying with medications and sodium restrictions.
VII. Dysrhythmias
Premature Ventricular Contractions (PVCs)
A. Observe for the following:
- Frequency
- Whether multifocal or unifocal
- Pairs or runs, sustained or paroxysmal
- Associated signs or symptoms
- Palpate pulse to evaluate for peripheral perfusion
B. Document any new arrhythmias or increase in severity with a rhythm strip and make notation on chart. Notify supervising physician and referring physician, where appropriate, to discuss treatment.
C. Discontinue exercise if PVCs become symptomatic and check pulse, BP, and oxygen saturation. Provide oxygen at 2 to 4 L if hypoxemic, and obtain IV access if directed by a physician.
D. Notify the supervising physician for evaluation and treatment.
Bradycardia
A. If patient develops symptomatic bradycardia, stop exercise.
B. Monitor HR and rhythm, BP, and oximetry. Provide oxygen at 2 to 4 L if hypoxemic. Obtain 12-lead ECG if available.
C. Assess for symptoms of instability or altered mental status, ischemic chest discomfort, HF, or hypotension and notify supervising physician for evaluation and treatment. Notify the supervising physician and if available, obtain IV access, and prepare to administer atropine or external pacing per ACLS guidelines.
D. Prepare for transfer to ED.
Tachycardia
A. If patient develops a new wide or narrow complex tachycardia, stop exercise.
B. Monitor HR and rhythm, BP, and oximetry. Provide oxygen at 2 to 4 L if hypoxemic. Obtain 12-lead ECG if available.
C. Assess for symptoms of instability or altered mental status, ischemic chest discomfort, HF, or hypotension, and notify supervising physician for evaluation and treatment. If directed by a physician, obtain IV access and prepare for synchronized cardioversion. If stable, may utilize vagal maneuvers or antiarrhythmic agents per ACLS guidelines.
D. Prepare for transfer to ED.
VIII. Dyspnea
A. If patient develops acute dyspnea, stop exercise and have patient sit down.
B. Monitor heart rate and rhythm, BP, respiratory rate, lung sounds, and oximetry. Provide oxygen at 2 to 4 L for oxygen saturation <94%.
C. If patient has a metered-dose inhaler, it may be administered as prescribed.
D. If condition deteriorates, notify supervising physician to evaluate for treatment options and possible transfer to ED.
E. If condition improves, notify primary care physician for further recommendations.
IX. Cerebrovascular Accident
A. If patient develops signs and symptoms of a stroke such as sudden arm or leg weakness, confusion, trouble speaking, dizziness, loss of balance or coordination, severe headache, or facial droop, immediately evaluate with rapid out-of-hospital stroke assessment.
B. If stroke is suspected, initiate EMS for immediate transport to a stroke facility.
C. Establish time of last known neurological baseline.
D. Maintain airway, breathing, and circulation.
E. Provide supplemental oxygen if hypoxemic or if oxygen saturation is unknown.
F. Check blood glucose.
G. Alert receiving hospital when patient is in transport.
X. Placement of IV Line
Purpose: To provide immediate access to administer emergency medication and IV fluids.
A. An attempt will be made to notify the supervising physician.
B. Place a saline lock in participant when one or more of the following apply:
- Angina pectoris protocol has been followed and chest pain persists.
- ECG, vital signs or participant appears to be clinically unstable or symptomatic.
- Physician directs the placement of IV line.
XI. Patient Transportation
Staff will meet and direct ambulance personnel to the patient treatment area.
Staff will prepare medical records to be sent with the patient as needed.
Staff will alert the emergency department of the patient transfer.
Cardiac Rehabilitation Department Emergency Procedures and Standing Orders Were Reviewed and Approved
___________________________________________
Physician's name
___________________________________________
Signature
___________________________________________
Date of most recent review
*Appendix B should be used only as an example of standing orders that might be considered and adopted for use in freestanding outpatient or community-based programs.
From American Association of Cardiovascular and Pulmonary Rehabilitation, Guidelines for Cardiac Rehabilitation Programs, 6th ed.
(Champaign, IL: Human Kinetics, 2021).
What are cardiac dysrhythmias?
By Alison L. Bailey, Alexis L. Beatty, Brian Carlin, Dennis J. Kerrigan, Steven J. Keteyian, Kirstine Laerum Sibilitz, Karen Lui, Ryan Mays, Jonathan Powell, Ray W. Squires, Diane J. Treat-Jacobson
Cardiac dysrhythmias are abnormalities in heart rhythm. They are also known as arrhythmias or irregular rhythms. Many CR participants have a history of cardiac dysrhythmias, and some experience dysrhythmias during CR participation.1-3 Symptoms from dysrhythmias may or may not be present and vary from patient to patient. The effects of dysrhythmias can range from generally benign to potentially harmful. Most studies report a cardiac arrest rate of approximately 1/100,000 patient-hours of CR participation.4-7 Although it is rare for dysrhythmias to have life-threatening consequences during exercise in CR programs, it remains important to recognize dysrhythmias and their features.
Bottom Line
Cardiac dysrhythmias are common in CR participants. Life-threatening consequences of cardiac dysrhythmias are rare during exercise in CR programs.
The following are commonly encountered dysrhythmias and symptoms:
Cardiac Dysrhythmias in CR
Generally Benign
- Premature atrial complexes (PACs)
- Isolated premature ventricular complexes (PVCs)
- AF or atrial flutter with controlled ventricular rate (8
- Paroxysmal supraventricular tachycardia (SVT)
- Mild bradycardia (50-60 bpm)
- First-degree atrioventricular (AV) block and asymptomatic type I second-degree (also known as Wenckebach) AV block
Potentially or Likely Harmful
- AF or atrial flutter with a rapid rate (≥110 bpm at rest)
- Symptomatic or severe bradycardia (HR <50)
- Symptomatic or advanced AV block (type II second-degree AV block or complete heart block)
- Ventricular tachycardia
- Ventricular fibrillation
Symptoms Associated With Cardiac Dysrhythmias
Stable Symptoms
- Palpitations
- Dizziness or lightheadedness
- Shortness of breath
- Chest pain or discomfort
Nonspecific or Associated Symptoms
- Weakness or fatigue
- Sweating
- Blurred vision
- Nausea
- Anxiety
- Edema
Unstable Symptoms
- Hypotension
- Near-syncope or loss of consciousness
- HF
- Unstable angina or MI
- Cardiac arrest
Exercise induces many physiologic effects, which can have both direct and indirect effects on cardiac electrophysiology. Exercise intensity can be related to the occurrence of dysrhythmias. Some dysrhythmias diminish or disappear with increasing exercise intensity; others increase or appear with increasing exercise intensity; and still others have no observable relationship to exercise intensity. Factors that can contribute to dysrhythmias during exercise include autonomic nervous system activity, ischemia, genetic abnormalities, structural heart disease, medications with proarrhythmic side effects, electrolyte imbalance, dehydration, and certain environmental factors.
Guideline 10.7 Dysrhythmia Exercise Prescription
For patients with known dysrhythmias, the exercise prescription should be tailored to the individual, with predetermined goals and criteria for exercise termination. Exercise should be terminated when a patient experiences a potentially harmful dysrhythmia or dysrhythmia with unstable symptoms.
Atrial Fibrillation
Light-to-moderate activities, particularly leisure-time activity and walking, are associated with a significantly lower incidence of AF in older adults.9 However, people who participate in extreme endurance training and sports activities may have an increased incidence of AF.10,11 For those diagnosed with AF, regular moderate PA is known to increase exercise capacity and control ventricular rate.12,13 In addition, exercise training increases exercise capacity and may reduce AF burden.14,15 The following information provides specific information about CR participation in patients who have AF.
AF originates in the atrium and is the most common cardiac arrhythmia. It is characterized by irregular contractions of the muscle fibers of the atria resulting in a variable HR. Risk factors associated with developing AF include PA, obesity, advanced age, HTN, HF, diabetes mellitus, CVD and valvular heart disease, left ventricular and atrial enlargement, and hyperthyroidism.43 Paradoxically, despite having few risk factors, athletes are also at increased risk for developing AF.
CR professionals will encounter these two types of patients with AF: patients who experience an initial (acute) onset (often noted during CR check-in or during exercise) and patients previously diagnosed and medically managed. Generally, AF is classified as (1) paroxysmal, (2) persistent, (3) long-standing persistent, or (4) permanent.2
AF should be considered when a patient presents with a rapid (often >110 bpm) “irregularly irregular” (no rhythmic pattern) resting HR. Patients experiencing an abrupt onset of AF may or may not report accompanying symptoms including palpitation, tachycardia, fatigue, shortness of breath, dizziness, and nausea. If AF is suspected, an ECG will confirm a diagnosis.
If new-onset AF is confirmed, the patient's physician should be consulted. Treating new-onset AF has three goals.44,50 The first goal is to mitigate symptoms by initially focusing in on reducing HR. Typical therapeutic HR reduction options include beta-adrenergic and calcium channel blocking agents and antiarrhythmic medication. The second goal is to reduce the risk for the development embolization of a blood clot (which the patient is at risk of developing due to atrial blood stagnation) through anticoagulation therapy. The third goal is to manage the patient's cardiovascular risk factors, which for overweight or obese patients is recommended to include weight loss and risk factor modification.50
Safety and rates of adverse event of exercise in patients have not been well studied. No large randomized control trials of exercise training and AF have assessed safety and efficacy. Guidelines for the treatment of patients with AF do not explicitly endorse specific exercise recommendations. Exercise, however, is not contraindicated in patients with AF. Moreover, exercise is effective treatment in multiple risk factors associated with AF, such as physical inactivity, HTN, diabetes mellitus, and obesity. Therefore, asymptomatic patients with AF who have received medical clearance should be encouraged to participate in an exercise program.
However, AF can profoundly impact the physiologic response to exercise training.45 In particular, the rapid, irregular contraction of the atrium results in reduced ventricular output. To compensate for the reduced cardiac output there is a commensurate increase in the rate and irregularity of ventricular contraction. Despite the negative impact of AF, exercise training studies have demonstrated improvements in functional capacity, health status, and quality of life.46
The special consideration regarding exercise testing and prescription for patients with AF have been detailed elsewhere.3 The following section is a brief review of special considerations regarding exercise testing and prescription for CR participants with AF.
Exercise Testing
As with all patients entering CR, undergoing a symptom-limited exercise tolerance test prior to initiating an exercise training program is optimal but not required. An exercise test is useful to assess for myocardial ischemia, evaluate chronotropic response, identify signs and symptoms, quantify functional capacity, and establish some general parameters for exercise training intensity.
Exercise Prescription for Patients With AF
Currently, no specific recommendations exist regarding exercise training for the treatment of AF. Studies of exercise training in patients with AF have employed a variety of protocols. Components of any exercise prescription include frequency, intensity, duration, modality, progression, and total volume. The exercise prescription for patients with AF should be individualized. A meta-analysis of exercise training studies involving people with AF recommends that a training regimen should include three or more sessions per week of a combination of moderate-intensity aerobic activity and resistance training. Session duration should be approximately 60 minutes, including adequate warm-up and cool-down.
By definition, the HR for a person with AF is irregular. Therefore, use of HR exclusively to assess exercise intensity is problematic. For aerobic training, in lieu of HR, use of RPE scale is an effective means to assess exercise intensity. A rating of 11 to 14 (on the Borg 6-20 scale) is typically associated with a moderate intensity that is approximately 70% to 85% of peak exercise capacity. Notably, very few studies have focused on the safety and efficacy of high-intensity aerobic training in patients with AF.
For overweight patients with AF, weight loss is recommended.47,50 To facilitate weight loss, orienting the exercise prescription to maximize caloric expenditure is indicated. High caloric exercise training (e.g., treadmill walking at a moderate intensity for an extended duration) in CR is well tolerated and an effective strategy to promote weight loss and improve multiple cardiovascular risk factors.48
No specific guidelines exist for resistance training for patients with AF. Given the lack of recommendations, using professional discretion is necessary when providing guidance regarding resistance training. Following the resistance training recommendations for other, non-AF CR participants is advisable. General recommendations for resistance training are found in chapter 6.
Considerations for the prescription of exercise and physical activity
By Jonathan Myers
Guideline 6.1 Considerations for the Prescription of Exercise and Physical Activity
When developing an exercise prescription, consider the following factors:
Safety Factors
- Clinical history
- Risks associated with CVD progression or instability
- Ischemic and angina thresholds
- Cognitive or psychological impairment
Associated Factors
- Vocational or avocational requirements
- Orthopedic limitations
- Previous and current activities
- Personal health and fitness goals
An important initial consideration in exercise planning is safety. Safety considerations apply to both structured exercise training and leisure-time PA. While most patients can engage in exercise without incurring undue risks, appropriate risk stratification should be performed. Guideline 6.1 provides key variables to consider when developing an exercise prescription. Safety and risk stratification are discussed in detail in chapters 4 and 5. Recommendations for supervision and ECG monitoring can be found in chapter 5. Later in this chapter, tables 6.1 and 6.2 present basic principles of exercise prescription. A model for risk stratification for cardiovascular events is outlined in the sidebar Stratification of Risk for Cardiac Events During Exercise Participation in chapter 5. After risk stratification, recommendations for supervision, ECG, monitoring and prescribed intensity and duration of exercise training can be made.
Comprehensive, evidence-based recommendations for structured exercise training in CR are available from several prominent organizations1,3,8 and are only summarized here. A comprehensive exercise program includes cardiorespiratory, musculoskeletal, and flexibility components. Specific elements for each component are summarized in the tables in this chapter and include guidelines for intensity, duration, frequency, and type of exercise for training. Each of the elements should be prescribed relative to one another and in a way that effectively addresses predefined training goals (e.g., increased aerobic or musculoskeletal fitness, weight reduction, control of blood glucose, or resumption of occupation).
Cardiorespiratory Endurance Training
Cardiorespiratory endurance training should be the foundation of most exercise routines for adults with or at risk for CVD. This type of exercise training is the most effective way to increase CRF. Elements of an exercise prescription for increasing CRF are presented in table 6.1. The relative training intensity may vary between 40% and 80% of maximal heart rate reserve (HRR) or metabolic reserve (V.O2R). Initially, programs should focus on the lower part of the intensity range, with progression to higher intensities as patients adapt to the program.7 RPE (e.g., Borg Scale of Perceived Exertion 6-20; Borg CR10 Scale; Omni Picture System of Perceived Exertion) are considered adjunctive to HR monitoring, but they may become more important as a subjective intensity guide as patients gain experience with exercise training and learn how to use the scale. Exercise training duration varies as a function of the overall energy expenditure goals of the patient. A minimum of 20 continuous minutes of exercise per session is commonly recommended within structured programs, although some patients may follow an intermittent (i.e., interval) exercise regimen. Some patients may need to accumulate shorter bouts (e.g., multiple 10 min bouts) throughout the day due to comorbidities, symptoms such as claudication or musculoskeletal discomfort, or lifestyle factors. Ideally, patients should be active most days of the week,1-7,9 but structured programs are often designed with a frequency of two to four sessions per week.
Once the initial exercise prescription is established, patients should progress gradually toward predefined or redefined program goals. There is no set format with respect to progression because many factors, including fitness level, motivation, and orthopedic limitations, influence the rate at which a patient may progress. In general, it is prudent to change one component and provide some time (a minimum of one exercise session) to assess the adaptation to the new level before progressing further. When time permits, increases in duration and frequency should precede increases in intensity. Modest increases in intensity, when appropriate, are likely to be tolerated and should be based on the observations of the staff and subjective responses of the patient, provided that the changes remain within the limits specified in the most recent evaluation.
A guiding principle should be progression of the total volume or dose of exercise such that the patient achieves desired energy expenditure thresholds within a three- to six-month period. Therefore, given that most patients' participation in CR lasts no longer than three months, it is important to educate and encourage patients to continue exercising even after CR participation has ended. The most appropriate volume of exercise depends on the individual CVD risk profile, training goals, and comorbidities (i.e., diabetes, hypertension, obesity, arthritis). An accumulating body of evidence has affirmed a dose-response relationship between the volume of PA and health outcomes.1,3,6-8 Whether exercise has a role in reversing coronary artery disease is an issue that remains controversial; however, thresholds of approximately 1,500 and 2,200 kcal/week are associated with stability and regression of coronary artery lesions, respectively.18 Notably, multiple studies document that energy expenditure in structured CR does not typically meet either of these thresholds.11-14 Therefore, patients will likely need to engage in PA outside of the structured program to achieve the optimal levels of energy expenditure.
Few studies have supported the efficacy of structured exercise training as a singular strategy to normalize body weight and body composition in patients with CVD. This underscores the importance of multiple behavioral strategies in weight reduction programming for overweight patients. Studies show that achieving weight loss goals requires a simultaneous change in dietary habits in addition to greater physical activity patterns. The volume or dose of exercise associated with the typical CR training session may be a limiting factor, and there is only a 1 to 2 kg weight loss during CR participation. It is likely part of the explanation for a low amount of weight loss during CR is due to a lack of focus on helping patients lose weight. As mentioned previously, numerous studies have shown the weekly dose to be inadequate for weight or fat reduction. As an example, a typical exercise session for an outpatient with a peak functional capacity of 7 METs might be 30 min at a heart rate that would equate with about 4 METs. The following formula provides a method to estimate the caloric costs of the exercise session:
Calories/min = [METs × body weight in kg × 3.5] / 200
It should be noted that the 4 MET value in this example includes the resting energy expenditure component (1 MET). Therefore, the net caloric cost of the exercise would be based on only 3 METs. If the hypothetical patient in this example weighed 100 kg (220 lb) and exercised 3 days per week for 30 min, the net caloric expenditure would be approximately 480 kcal/week (5.3 kcal/min × 30 min × 3 days/week). Although patients can clearly improve exercise tolerance with this regimen, the estimated caloric expenditure falls well short of contemporary recommendations for PA and in most cases would not be effective for weight or fat loss.15 For example, 40 min sessions, five times per week, would result in an expenditure of approximately 1,060 kcal per week. Again, this calculation highlights the importance of increasing PA outside of the structured or in-hospital program. Thus, adjustments must be made about frequency and duration of exercise to allow patients to achieve greater energy expenditures to enhance program outcomes. However, these adjustments must be with the caveat that although it is prudent to increase exercise volume progressively, staff must carefully consider the risk that a higher-volume program may lead to higher dropout rates. Therefore, overweight patients must be educated about the need to develop and maintain fitness as the core of their exercise regimen, with the additional volume of PA facilitating weight loss and other goals. Finally, as CRF improves, patients are able to exercise at a higher metabolic rate (more kcal/min) at a given relative intensity (% maximal HRR). This adjustment allows patients to accumulate a greater caloric deficit over time.
Example of standing orders to initiate outpatient cardiac rehabilitation
Appendix A: Example of Standing Orders to Initiate Outpatient CR
- Initiate monitored exercise program per outpatient CR policies and procedures.
- Determine target heart rate (THR) via sign- or symptom-limited graded exercise testing (GXT) or sign- or symptom-limited responses to submaximal exercise.
- Begin with a training duration of up to 30 min to tolerance, one to five times a week.
- Gradually increase duration of training exercise if patient cardiovascular and physiological responses are within normal limits.
- Observe participant for signs of exercise intolerance and adapt or terminate exercise as indicated in policies and procedures.
- Assess lipid profile approximately six weeks postevent.
- Administer nitroglycerin 0.3 or 0.4 mg sublingually every 5 minutes × 3 as needed for angina discomfort or ischemic symptoms.
- Provide regular, periodic progress reports to the referring physician. Provide copies of reports to other physicians as needed.
- Initiate patient education and counseling sessions as patient needs indicate.
- Consult patient's personal physician or CR supervising physician for any necessary orders.
- Consult with the CR dietitian to provide individualized nutrition education for each participant.
- Enter the patient into a non-ECG-monitored maintenance program upon completion of early outpatient CR program.
__________________________________________________________________________________________
Physician's signature
___________________________________________
Date
From American Association of Cardiovascular and Pulmonary Rehabilitation, Guidelines for Cardiac Rehabilitation Programs, 6th ed.
(Champaign, IL: Human Kinetics, 2021).
Appendix B: Example of Outpatient CR Emergency Standing Orders*
Table of Contents
Protocols for Urgent Situations and Emergency Interventions in the Cardiac Rehabilitation Area
I. Cardiopulmonary arrest
II. Angina pectoris
III. Hypoglycemia
IV. Hyperglycemia
V. Hypotension
VI. Hypertension
VII. Dysrhythmias
VIII. Dyspnea
IX. Cerebrovascular accident
X. Placement of intravenous line
XI. Patient transportation
I. Cardiopulmonary Arrest
A. Identify responsiveness and determine if breathing is absent or abnormal (gasping).
B. Call out for help/activate emergency medical system (EMS).
- Call out for help from coworker. If no one responds and if no other staff member is available to assist, go to the nearest phone and activate EMS. (Emergency numbers with specific scripted instructions are posted at each phone.) Get defibrillator/automated external defibrillator (AED). If no pulse, attach defibrillator/AED and shock if indicated. Begin cardiopulmonary resuscitation (CPR) with compressions.
- If a second responder is available to assist, that person should activate EMS and then get the defibrillator/AED while the first responder stays with the patient to begin compressions.
- Staff will meet the EMS team at the appropriate entrance and direct them to the patient.
First Responder
- Determine responsiveness and absent or abnormal breathing.
- Send someone to activate EMS and get defibrillator/AED.
- If pulseless, begin chest compressions at a depth of at least 2 in. and a rate of at least 100 compressions/min until defibrillator/AED arrives. Allow for complete chest recoil, minimize interruptions to
Second Responder
- After activating EMS, take cart with defibrillator/AED to the patient. Place defibrillator pads or AED on patient and assess cardiac rhythm.
- Shock if indicated, resume compressions. Follow appropriate algorithm according to ACLS guidelines.
Third Responder (if Available)
- Direct remaining patients to another area.
- Direct and control incoming emergency response team and patients.
- Obtain extra supplies and equipment as needed.
- Act as the recorder of events until EMS arrives.
- Prepare records to be sent with patient to the emergency department if needed.
- Notify patient physician/cardiologist and family.
Emergency in Other Locations
7. Protocols should be developed for emergencies occurring in locations other than the cardiac rehabilitation gym including but not limited to:
- Locker room/restrooms
- Lobby/waiting area
- Patient education area
- Parking lots
II. Angina Pectoris
A. If a patient develops unstable angina while in the exercise area, the patient should immediately discontinue exercise and sit or lie down. Note the exercise workload, HR, and BP at which the symptoms occurred.
B. The following protocol should be followed by the CR staff:
- Check pulse, BP, cardiac rhythm (attach telemetry monitor if not already monitored), and oxygen saturation.
- Rate angina on a scale of 1 to 10.
- If no relief with 1 to 3 min of rest, give 1 nitroglycerine (NTG) 0.4 mg SL or spray.
- Obtain 12-lead ECG and call supervising physician.
C. If pain is relieved:
- If this angina is of new onset, the patient should be evaluated by the supervising physician. The primary care physician should be notified of the results of the evaluation and recommended treatment, if any.
- If the patient experiences chronic stable angina, exercise intensity should be decreased or halted until the angina is relieved. Patient may resume exercise at a lower workload dependent on the clinical judgment of the medical director and professional staff.
OR
The patient can be discharged but should be instructed to report any increase in frequency or severity of angina to their physician.
D. If pain is not relieved:
- Monitor pulse, BP, cardiac rhythm, and oxygen saturation closely.
- Place on oxygen at 2 to 4 L per nasal prongs if oxygen saturation is <94%.
- Patient to chew aspirin 160 to 325 mg.
- Repeat NTG 0.4 mg SL or spray every 5 min for unrelieved angina symptoms.
- The supervising physician will evaluate and determine the course of action.
III. Hypoglycemia
A. If patient displays any symptoms of hypoglycemia:
- Obtain finger-stick blood glucose level.
- If BG results are
- Retest BG in 15 min. If BG is not >90 mg/dL, repeat 15 g CHO and recheck BG in 15 min.
- If patient is uncooperative or unconscious, contact supervising physician, give glucose gel or establish IV access and give 50 cc (1 amp) 50% dextrose solution. Arrange for transport to ED.
IV. Hyperglycemia
A. A participant with a BG >300 mg/dL should not exercise unless the patient's referring physician and the program medical director give their consent.
B. Frequency of BG checks should be determined according to the patient profile and ITP.
C. BG evaluations may be performed by rehabilitation staff or the patient according to the ITP.
D. The CR staff may request a blood glucose evaluation on any patient based on suspected signs and symptoms of hyperglycemia (nausea, flushing, polyuria, polydipsia, fruity breath, tachypnea).
V. Hypotension
A. Remove the patient from the exercise area if possible.
B. Place patient in a supine position. Consider elevating legs or placing in Trendelenburg position.
C. Attach a telemetry monitor if not already monitored.
D. Check BP, pulse, cardiac rhythm, and oxygen saturation.
E. If no response to the position change, call the supervising physician. If the patient condition continues to deteriorate or becomes progressively symptomatic, or if BP continues to drop, start an IV of normal saline at 100 mL/h and arrange for transport to the ED. After evaluation and treatment of the patient, the supervising physician should notify the patient's primary care physician of the hypotensive episode and discuss any further treatment if necessary.
F. If patient responds to the supine position, keep supine until SBP is >100, then gradually assist to sitting position. Continue to monitor BP, pulse, and rhythm. Encourage fluids. Notify the patient's primary physician of the episode.
VI. Hypertension
A. Check every patient's BP before exercise and compare with previous recordings.
B. If the SBP reading is >170 mm Hg or the diastolic reading is >100 mm Hg, have the patient sit and recheck the BP in 5 min.
C. If the BP remains elevated, do not have patient exercise. Notify the primary care physician or supervising physician to evaluate and determine course of action.
D. Patients may exercise with elevated BP if directed by the primary care physician and medical director.
E. Investigate whether patient is complying with medications and sodium restrictions.
VII. Dysrhythmias
Premature Ventricular Contractions (PVCs)
A. Observe for the following:
- Frequency
- Whether multifocal or unifocal
- Pairs or runs, sustained or paroxysmal
- Associated signs or symptoms
- Palpate pulse to evaluate for peripheral perfusion
B. Document any new arrhythmias or increase in severity with a rhythm strip and make notation on chart. Notify supervising physician and referring physician, where appropriate, to discuss treatment.
C. Discontinue exercise if PVCs become symptomatic and check pulse, BP, and oxygen saturation. Provide oxygen at 2 to 4 L if hypoxemic, and obtain IV access if directed by a physician.
D. Notify the supervising physician for evaluation and treatment.
Bradycardia
A. If patient develops symptomatic bradycardia, stop exercise.
B. Monitor HR and rhythm, BP, and oximetry. Provide oxygen at 2 to 4 L if hypoxemic. Obtain 12-lead ECG if available.
C. Assess for symptoms of instability or altered mental status, ischemic chest discomfort, HF, or hypotension and notify supervising physician for evaluation and treatment. Notify the supervising physician and if available, obtain IV access, and prepare to administer atropine or external pacing per ACLS guidelines.
D. Prepare for transfer to ED.
Tachycardia
A. If patient develops a new wide or narrow complex tachycardia, stop exercise.
B. Monitor HR and rhythm, BP, and oximetry. Provide oxygen at 2 to 4 L if hypoxemic. Obtain 12-lead ECG if available.
C. Assess for symptoms of instability or altered mental status, ischemic chest discomfort, HF, or hypotension, and notify supervising physician for evaluation and treatment. If directed by a physician, obtain IV access and prepare for synchronized cardioversion. If stable, may utilize vagal maneuvers or antiarrhythmic agents per ACLS guidelines.
D. Prepare for transfer to ED.
VIII. Dyspnea
A. If patient develops acute dyspnea, stop exercise and have patient sit down.
B. Monitor heart rate and rhythm, BP, respiratory rate, lung sounds, and oximetry. Provide oxygen at 2 to 4 L for oxygen saturation <94%.
C. If patient has a metered-dose inhaler, it may be administered as prescribed.
D. If condition deteriorates, notify supervising physician to evaluate for treatment options and possible transfer to ED.
E. If condition improves, notify primary care physician for further recommendations.
IX. Cerebrovascular Accident
A. If patient develops signs and symptoms of a stroke such as sudden arm or leg weakness, confusion, trouble speaking, dizziness, loss of balance or coordination, severe headache, or facial droop, immediately evaluate with rapid out-of-hospital stroke assessment.
B. If stroke is suspected, initiate EMS for immediate transport to a stroke facility.
C. Establish time of last known neurological baseline.
D. Maintain airway, breathing, and circulation.
E. Provide supplemental oxygen if hypoxemic or if oxygen saturation is unknown.
F. Check blood glucose.
G. Alert receiving hospital when patient is in transport.
X. Placement of IV Line
Purpose: To provide immediate access to administer emergency medication and IV fluids.
A. An attempt will be made to notify the supervising physician.
B. Place a saline lock in participant when one or more of the following apply:
- Angina pectoris protocol has been followed and chest pain persists.
- ECG, vital signs or participant appears to be clinically unstable or symptomatic.
- Physician directs the placement of IV line.
XI. Patient Transportation
Staff will meet and direct ambulance personnel to the patient treatment area.
Staff will prepare medical records to be sent with the patient as needed.
Staff will alert the emergency department of the patient transfer.
Cardiac Rehabilitation Department Emergency Procedures and Standing Orders Were Reviewed and Approved
___________________________________________
Physician's name
___________________________________________
Signature
___________________________________________
Date of most recent review
*Appendix B should be used only as an example of standing orders that might be considered and adopted for use in freestanding outpatient or community-based programs.
From American Association of Cardiovascular and Pulmonary Rehabilitation, Guidelines for Cardiac Rehabilitation Programs, 6th ed.
(Champaign, IL: Human Kinetics, 2021).
What are cardiac dysrhythmias?
By Alison L. Bailey, Alexis L. Beatty, Brian Carlin, Dennis J. Kerrigan, Steven J. Keteyian, Kirstine Laerum Sibilitz, Karen Lui, Ryan Mays, Jonathan Powell, Ray W. Squires, Diane J. Treat-Jacobson
Cardiac dysrhythmias are abnormalities in heart rhythm. They are also known as arrhythmias or irregular rhythms. Many CR participants have a history of cardiac dysrhythmias, and some experience dysrhythmias during CR participation.1-3 Symptoms from dysrhythmias may or may not be present and vary from patient to patient. The effects of dysrhythmias can range from generally benign to potentially harmful. Most studies report a cardiac arrest rate of approximately 1/100,000 patient-hours of CR participation.4-7 Although it is rare for dysrhythmias to have life-threatening consequences during exercise in CR programs, it remains important to recognize dysrhythmias and their features.
Bottom Line
Cardiac dysrhythmias are common in CR participants. Life-threatening consequences of cardiac dysrhythmias are rare during exercise in CR programs.
The following are commonly encountered dysrhythmias and symptoms:
Cardiac Dysrhythmias in CR
Generally Benign
- Premature atrial complexes (PACs)
- Isolated premature ventricular complexes (PVCs)
- AF or atrial flutter with controlled ventricular rate (8
- Paroxysmal supraventricular tachycardia (SVT)
- Mild bradycardia (50-60 bpm)
- First-degree atrioventricular (AV) block and asymptomatic type I second-degree (also known as Wenckebach) AV block
Potentially or Likely Harmful
- AF or atrial flutter with a rapid rate (≥110 bpm at rest)
- Symptomatic or severe bradycardia (HR <50)
- Symptomatic or advanced AV block (type II second-degree AV block or complete heart block)
- Ventricular tachycardia
- Ventricular fibrillation
Symptoms Associated With Cardiac Dysrhythmias
Stable Symptoms
- Palpitations
- Dizziness or lightheadedness
- Shortness of breath
- Chest pain or discomfort
Nonspecific or Associated Symptoms
- Weakness or fatigue
- Sweating
- Blurred vision
- Nausea
- Anxiety
- Edema
Unstable Symptoms
- Hypotension
- Near-syncope or loss of consciousness
- HF
- Unstable angina or MI
- Cardiac arrest
Exercise induces many physiologic effects, which can have both direct and indirect effects on cardiac electrophysiology. Exercise intensity can be related to the occurrence of dysrhythmias. Some dysrhythmias diminish or disappear with increasing exercise intensity; others increase or appear with increasing exercise intensity; and still others have no observable relationship to exercise intensity. Factors that can contribute to dysrhythmias during exercise include autonomic nervous system activity, ischemia, genetic abnormalities, structural heart disease, medications with proarrhythmic side effects, electrolyte imbalance, dehydration, and certain environmental factors.
Guideline 10.7 Dysrhythmia Exercise Prescription
For patients with known dysrhythmias, the exercise prescription should be tailored to the individual, with predetermined goals and criteria for exercise termination. Exercise should be terminated when a patient experiences a potentially harmful dysrhythmia or dysrhythmia with unstable symptoms.
Atrial Fibrillation
Light-to-moderate activities, particularly leisure-time activity and walking, are associated with a significantly lower incidence of AF in older adults.9 However, people who participate in extreme endurance training and sports activities may have an increased incidence of AF.10,11 For those diagnosed with AF, regular moderate PA is known to increase exercise capacity and control ventricular rate.12,13 In addition, exercise training increases exercise capacity and may reduce AF burden.14,15 The following information provides specific information about CR participation in patients who have AF.
AF originates in the atrium and is the most common cardiac arrhythmia. It is characterized by irregular contractions of the muscle fibers of the atria resulting in a variable HR. Risk factors associated with developing AF include PA, obesity, advanced age, HTN, HF, diabetes mellitus, CVD and valvular heart disease, left ventricular and atrial enlargement, and hyperthyroidism.43 Paradoxically, despite having few risk factors, athletes are also at increased risk for developing AF.
CR professionals will encounter these two types of patients with AF: patients who experience an initial (acute) onset (often noted during CR check-in or during exercise) and patients previously diagnosed and medically managed. Generally, AF is classified as (1) paroxysmal, (2) persistent, (3) long-standing persistent, or (4) permanent.2
AF should be considered when a patient presents with a rapid (often >110 bpm) “irregularly irregular” (no rhythmic pattern) resting HR. Patients experiencing an abrupt onset of AF may or may not report accompanying symptoms including palpitation, tachycardia, fatigue, shortness of breath, dizziness, and nausea. If AF is suspected, an ECG will confirm a diagnosis.
If new-onset AF is confirmed, the patient's physician should be consulted. Treating new-onset AF has three goals.44,50 The first goal is to mitigate symptoms by initially focusing in on reducing HR. Typical therapeutic HR reduction options include beta-adrenergic and calcium channel blocking agents and antiarrhythmic medication. The second goal is to reduce the risk for the development embolization of a blood clot (which the patient is at risk of developing due to atrial blood stagnation) through anticoagulation therapy. The third goal is to manage the patient's cardiovascular risk factors, which for overweight or obese patients is recommended to include weight loss and risk factor modification.50
Safety and rates of adverse event of exercise in patients have not been well studied. No large randomized control trials of exercise training and AF have assessed safety and efficacy. Guidelines for the treatment of patients with AF do not explicitly endorse specific exercise recommendations. Exercise, however, is not contraindicated in patients with AF. Moreover, exercise is effective treatment in multiple risk factors associated with AF, such as physical inactivity, HTN, diabetes mellitus, and obesity. Therefore, asymptomatic patients with AF who have received medical clearance should be encouraged to participate in an exercise program.
However, AF can profoundly impact the physiologic response to exercise training.45 In particular, the rapid, irregular contraction of the atrium results in reduced ventricular output. To compensate for the reduced cardiac output there is a commensurate increase in the rate and irregularity of ventricular contraction. Despite the negative impact of AF, exercise training studies have demonstrated improvements in functional capacity, health status, and quality of life.46
The special consideration regarding exercise testing and prescription for patients with AF have been detailed elsewhere.3 The following section is a brief review of special considerations regarding exercise testing and prescription for CR participants with AF.
Exercise Testing
As with all patients entering CR, undergoing a symptom-limited exercise tolerance test prior to initiating an exercise training program is optimal but not required. An exercise test is useful to assess for myocardial ischemia, evaluate chronotropic response, identify signs and symptoms, quantify functional capacity, and establish some general parameters for exercise training intensity.
Exercise Prescription for Patients With AF
Currently, no specific recommendations exist regarding exercise training for the treatment of AF. Studies of exercise training in patients with AF have employed a variety of protocols. Components of any exercise prescription include frequency, intensity, duration, modality, progression, and total volume. The exercise prescription for patients with AF should be individualized. A meta-analysis of exercise training studies involving people with AF recommends that a training regimen should include three or more sessions per week of a combination of moderate-intensity aerobic activity and resistance training. Session duration should be approximately 60 minutes, including adequate warm-up and cool-down.
By definition, the HR for a person with AF is irregular. Therefore, use of HR exclusively to assess exercise intensity is problematic. For aerobic training, in lieu of HR, use of RPE scale is an effective means to assess exercise intensity. A rating of 11 to 14 (on the Borg 6-20 scale) is typically associated with a moderate intensity that is approximately 70% to 85% of peak exercise capacity. Notably, very few studies have focused on the safety and efficacy of high-intensity aerobic training in patients with AF.
For overweight patients with AF, weight loss is recommended.47,50 To facilitate weight loss, orienting the exercise prescription to maximize caloric expenditure is indicated. High caloric exercise training (e.g., treadmill walking at a moderate intensity for an extended duration) in CR is well tolerated and an effective strategy to promote weight loss and improve multiple cardiovascular risk factors.48
No specific guidelines exist for resistance training for patients with AF. Given the lack of recommendations, using professional discretion is necessary when providing guidance regarding resistance training. Following the resistance training recommendations for other, non-AF CR participants is advisable. General recommendations for resistance training are found in chapter 6.
Considerations for the prescription of exercise and physical activity
By Jonathan Myers
Guideline 6.1 Considerations for the Prescription of Exercise and Physical Activity
When developing an exercise prescription, consider the following factors:
Safety Factors
- Clinical history
- Risks associated with CVD progression or instability
- Ischemic and angina thresholds
- Cognitive or psychological impairment
Associated Factors
- Vocational or avocational requirements
- Orthopedic limitations
- Previous and current activities
- Personal health and fitness goals
An important initial consideration in exercise planning is safety. Safety considerations apply to both structured exercise training and leisure-time PA. While most patients can engage in exercise without incurring undue risks, appropriate risk stratification should be performed. Guideline 6.1 provides key variables to consider when developing an exercise prescription. Safety and risk stratification are discussed in detail in chapters 4 and 5. Recommendations for supervision and ECG monitoring can be found in chapter 5. Later in this chapter, tables 6.1 and 6.2 present basic principles of exercise prescription. A model for risk stratification for cardiovascular events is outlined in the sidebar Stratification of Risk for Cardiac Events During Exercise Participation in chapter 5. After risk stratification, recommendations for supervision, ECG, monitoring and prescribed intensity and duration of exercise training can be made.
Comprehensive, evidence-based recommendations for structured exercise training in CR are available from several prominent organizations1,3,8 and are only summarized here. A comprehensive exercise program includes cardiorespiratory, musculoskeletal, and flexibility components. Specific elements for each component are summarized in the tables in this chapter and include guidelines for intensity, duration, frequency, and type of exercise for training. Each of the elements should be prescribed relative to one another and in a way that effectively addresses predefined training goals (e.g., increased aerobic or musculoskeletal fitness, weight reduction, control of blood glucose, or resumption of occupation).
Cardiorespiratory Endurance Training
Cardiorespiratory endurance training should be the foundation of most exercise routines for adults with or at risk for CVD. This type of exercise training is the most effective way to increase CRF. Elements of an exercise prescription for increasing CRF are presented in table 6.1. The relative training intensity may vary between 40% and 80% of maximal heart rate reserve (HRR) or metabolic reserve (V.O2R). Initially, programs should focus on the lower part of the intensity range, with progression to higher intensities as patients adapt to the program.7 RPE (e.g., Borg Scale of Perceived Exertion 6-20; Borg CR10 Scale; Omni Picture System of Perceived Exertion) are considered adjunctive to HR monitoring, but they may become more important as a subjective intensity guide as patients gain experience with exercise training and learn how to use the scale. Exercise training duration varies as a function of the overall energy expenditure goals of the patient. A minimum of 20 continuous minutes of exercise per session is commonly recommended within structured programs, although some patients may follow an intermittent (i.e., interval) exercise regimen. Some patients may need to accumulate shorter bouts (e.g., multiple 10 min bouts) throughout the day due to comorbidities, symptoms such as claudication or musculoskeletal discomfort, or lifestyle factors. Ideally, patients should be active most days of the week,1-7,9 but structured programs are often designed with a frequency of two to four sessions per week.
Once the initial exercise prescription is established, patients should progress gradually toward predefined or redefined program goals. There is no set format with respect to progression because many factors, including fitness level, motivation, and orthopedic limitations, influence the rate at which a patient may progress. In general, it is prudent to change one component and provide some time (a minimum of one exercise session) to assess the adaptation to the new level before progressing further. When time permits, increases in duration and frequency should precede increases in intensity. Modest increases in intensity, when appropriate, are likely to be tolerated and should be based on the observations of the staff and subjective responses of the patient, provided that the changes remain within the limits specified in the most recent evaluation.
A guiding principle should be progression of the total volume or dose of exercise such that the patient achieves desired energy expenditure thresholds within a three- to six-month period. Therefore, given that most patients' participation in CR lasts no longer than three months, it is important to educate and encourage patients to continue exercising even after CR participation has ended. The most appropriate volume of exercise depends on the individual CVD risk profile, training goals, and comorbidities (i.e., diabetes, hypertension, obesity, arthritis). An accumulating body of evidence has affirmed a dose-response relationship between the volume of PA and health outcomes.1,3,6-8 Whether exercise has a role in reversing coronary artery disease is an issue that remains controversial; however, thresholds of approximately 1,500 and 2,200 kcal/week are associated with stability and regression of coronary artery lesions, respectively.18 Notably, multiple studies document that energy expenditure in structured CR does not typically meet either of these thresholds.11-14 Therefore, patients will likely need to engage in PA outside of the structured program to achieve the optimal levels of energy expenditure.
Few studies have supported the efficacy of structured exercise training as a singular strategy to normalize body weight and body composition in patients with CVD. This underscores the importance of multiple behavioral strategies in weight reduction programming for overweight patients. Studies show that achieving weight loss goals requires a simultaneous change in dietary habits in addition to greater physical activity patterns. The volume or dose of exercise associated with the typical CR training session may be a limiting factor, and there is only a 1 to 2 kg weight loss during CR participation. It is likely part of the explanation for a low amount of weight loss during CR is due to a lack of focus on helping patients lose weight. As mentioned previously, numerous studies have shown the weekly dose to be inadequate for weight or fat reduction. As an example, a typical exercise session for an outpatient with a peak functional capacity of 7 METs might be 30 min at a heart rate that would equate with about 4 METs. The following formula provides a method to estimate the caloric costs of the exercise session:
Calories/min = [METs × body weight in kg × 3.5] / 200
It should be noted that the 4 MET value in this example includes the resting energy expenditure component (1 MET). Therefore, the net caloric cost of the exercise would be based on only 3 METs. If the hypothetical patient in this example weighed 100 kg (220 lb) and exercised 3 days per week for 30 min, the net caloric expenditure would be approximately 480 kcal/week (5.3 kcal/min × 30 min × 3 days/week). Although patients can clearly improve exercise tolerance with this regimen, the estimated caloric expenditure falls well short of contemporary recommendations for PA and in most cases would not be effective for weight or fat loss.15 For example, 40 min sessions, five times per week, would result in an expenditure of approximately 1,060 kcal per week. Again, this calculation highlights the importance of increasing PA outside of the structured or in-hospital program. Thus, adjustments must be made about frequency and duration of exercise to allow patients to achieve greater energy expenditures to enhance program outcomes. However, these adjustments must be with the caveat that although it is prudent to increase exercise volume progressively, staff must carefully consider the risk that a higher-volume program may lead to higher dropout rates. Therefore, overweight patients must be educated about the need to develop and maintain fitness as the core of their exercise regimen, with the additional volume of PA facilitating weight loss and other goals. Finally, as CRF improves, patients are able to exercise at a higher metabolic rate (more kcal/min) at a given relative intensity (% maximal HRR). This adjustment allows patients to accumulate a greater caloric deficit over time.
Example of standing orders to initiate outpatient cardiac rehabilitation
Appendix A: Example of Standing Orders to Initiate Outpatient CR
- Initiate monitored exercise program per outpatient CR policies and procedures.
- Determine target heart rate (THR) via sign- or symptom-limited graded exercise testing (GXT) or sign- or symptom-limited responses to submaximal exercise.
- Begin with a training duration of up to 30 min to tolerance, one to five times a week.
- Gradually increase duration of training exercise if patient cardiovascular and physiological responses are within normal limits.
- Observe participant for signs of exercise intolerance and adapt or terminate exercise as indicated in policies and procedures.
- Assess lipid profile approximately six weeks postevent.
- Administer nitroglycerin 0.3 or 0.4 mg sublingually every 5 minutes × 3 as needed for angina discomfort or ischemic symptoms.
- Provide regular, periodic progress reports to the referring physician. Provide copies of reports to other physicians as needed.
- Initiate patient education and counseling sessions as patient needs indicate.
- Consult patient's personal physician or CR supervising physician for any necessary orders.
- Consult with the CR dietitian to provide individualized nutrition education for each participant.
- Enter the patient into a non-ECG-monitored maintenance program upon completion of early outpatient CR program.
__________________________________________________________________________________________
Physician's signature
___________________________________________
Date
From American Association of Cardiovascular and Pulmonary Rehabilitation, Guidelines for Cardiac Rehabilitation Programs, 6th ed.
(Champaign, IL: Human Kinetics, 2021).
Appendix B: Example of Outpatient CR Emergency Standing Orders*
Table of Contents
Protocols for Urgent Situations and Emergency Interventions in the Cardiac Rehabilitation Area
I. Cardiopulmonary arrest
II. Angina pectoris
III. Hypoglycemia
IV. Hyperglycemia
V. Hypotension
VI. Hypertension
VII. Dysrhythmias
VIII. Dyspnea
IX. Cerebrovascular accident
X. Placement of intravenous line
XI. Patient transportation
I. Cardiopulmonary Arrest
A. Identify responsiveness and determine if breathing is absent or abnormal (gasping).
B. Call out for help/activate emergency medical system (EMS).
- Call out for help from coworker. If no one responds and if no other staff member is available to assist, go to the nearest phone and activate EMS. (Emergency numbers with specific scripted instructions are posted at each phone.) Get defibrillator/automated external defibrillator (AED). If no pulse, attach defibrillator/AED and shock if indicated. Begin cardiopulmonary resuscitation (CPR) with compressions.
- If a second responder is available to assist, that person should activate EMS and then get the defibrillator/AED while the first responder stays with the patient to begin compressions.
- Staff will meet the EMS team at the appropriate entrance and direct them to the patient.
First Responder
- Determine responsiveness and absent or abnormal breathing.
- Send someone to activate EMS and get defibrillator/AED.
- If pulseless, begin chest compressions at a depth of at least 2 in. and a rate of at least 100 compressions/min until defibrillator/AED arrives. Allow for complete chest recoil, minimize interruptions to
Second Responder
- After activating EMS, take cart with defibrillator/AED to the patient. Place defibrillator pads or AED on patient and assess cardiac rhythm.
- Shock if indicated, resume compressions. Follow appropriate algorithm according to ACLS guidelines.
Third Responder (if Available)
- Direct remaining patients to another area.
- Direct and control incoming emergency response team and patients.
- Obtain extra supplies and equipment as needed.
- Act as the recorder of events until EMS arrives.
- Prepare records to be sent with patient to the emergency department if needed.
- Notify patient physician/cardiologist and family.
Emergency in Other Locations
7. Protocols should be developed for emergencies occurring in locations other than the cardiac rehabilitation gym including but not limited to:
- Locker room/restrooms
- Lobby/waiting area
- Patient education area
- Parking lots
II. Angina Pectoris
A. If a patient develops unstable angina while in the exercise area, the patient should immediately discontinue exercise and sit or lie down. Note the exercise workload, HR, and BP at which the symptoms occurred.
B. The following protocol should be followed by the CR staff:
- Check pulse, BP, cardiac rhythm (attach telemetry monitor if not already monitored), and oxygen saturation.
- Rate angina on a scale of 1 to 10.
- If no relief with 1 to 3 min of rest, give 1 nitroglycerine (NTG) 0.4 mg SL or spray.
- Obtain 12-lead ECG and call supervising physician.
C. If pain is relieved:
- If this angina is of new onset, the patient should be evaluated by the supervising physician. The primary care physician should be notified of the results of the evaluation and recommended treatment, if any.
- If the patient experiences chronic stable angina, exercise intensity should be decreased or halted until the angina is relieved. Patient may resume exercise at a lower workload dependent on the clinical judgment of the medical director and professional staff.
OR
The patient can be discharged but should be instructed to report any increase in frequency or severity of angina to their physician.
D. If pain is not relieved:
- Monitor pulse, BP, cardiac rhythm, and oxygen saturation closely.
- Place on oxygen at 2 to 4 L per nasal prongs if oxygen saturation is <94%.
- Patient to chew aspirin 160 to 325 mg.
- Repeat NTG 0.4 mg SL or spray every 5 min for unrelieved angina symptoms.
- The supervising physician will evaluate and determine the course of action.
III. Hypoglycemia
A. If patient displays any symptoms of hypoglycemia:
- Obtain finger-stick blood glucose level.
- If BG results are
- Retest BG in 15 min. If BG is not >90 mg/dL, repeat 15 g CHO and recheck BG in 15 min.
- If patient is uncooperative or unconscious, contact supervising physician, give glucose gel or establish IV access and give 50 cc (1 amp) 50% dextrose solution. Arrange for transport to ED.
IV. Hyperglycemia
A. A participant with a BG >300 mg/dL should not exercise unless the patient's referring physician and the program medical director give their consent.
B. Frequency of BG checks should be determined according to the patient profile and ITP.
C. BG evaluations may be performed by rehabilitation staff or the patient according to the ITP.
D. The CR staff may request a blood glucose evaluation on any patient based on suspected signs and symptoms of hyperglycemia (nausea, flushing, polyuria, polydipsia, fruity breath, tachypnea).
V. Hypotension
A. Remove the patient from the exercise area if possible.
B. Place patient in a supine position. Consider elevating legs or placing in Trendelenburg position.
C. Attach a telemetry monitor if not already monitored.
D. Check BP, pulse, cardiac rhythm, and oxygen saturation.
E. If no response to the position change, call the supervising physician. If the patient condition continues to deteriorate or becomes progressively symptomatic, or if BP continues to drop, start an IV of normal saline at 100 mL/h and arrange for transport to the ED. After evaluation and treatment of the patient, the supervising physician should notify the patient's primary care physician of the hypotensive episode and discuss any further treatment if necessary.
F. If patient responds to the supine position, keep supine until SBP is >100, then gradually assist to sitting position. Continue to monitor BP, pulse, and rhythm. Encourage fluids. Notify the patient's primary physician of the episode.
VI. Hypertension
A. Check every patient's BP before exercise and compare with previous recordings.
B. If the SBP reading is >170 mm Hg or the diastolic reading is >100 mm Hg, have the patient sit and recheck the BP in 5 min.
C. If the BP remains elevated, do not have patient exercise. Notify the primary care physician or supervising physician to evaluate and determine course of action.
D. Patients may exercise with elevated BP if directed by the primary care physician and medical director.
E. Investigate whether patient is complying with medications and sodium restrictions.
VII. Dysrhythmias
Premature Ventricular Contractions (PVCs)
A. Observe for the following:
- Frequency
- Whether multifocal or unifocal
- Pairs or runs, sustained or paroxysmal
- Associated signs or symptoms
- Palpate pulse to evaluate for peripheral perfusion
B. Document any new arrhythmias or increase in severity with a rhythm strip and make notation on chart. Notify supervising physician and referring physician, where appropriate, to discuss treatment.
C. Discontinue exercise if PVCs become symptomatic and check pulse, BP, and oxygen saturation. Provide oxygen at 2 to 4 L if hypoxemic, and obtain IV access if directed by a physician.
D. Notify the supervising physician for evaluation and treatment.
Bradycardia
A. If patient develops symptomatic bradycardia, stop exercise.
B. Monitor HR and rhythm, BP, and oximetry. Provide oxygen at 2 to 4 L if hypoxemic. Obtain 12-lead ECG if available.
C. Assess for symptoms of instability or altered mental status, ischemic chest discomfort, HF, or hypotension and notify supervising physician for evaluation and treatment. Notify the supervising physician and if available, obtain IV access, and prepare to administer atropine or external pacing per ACLS guidelines.
D. Prepare for transfer to ED.
Tachycardia
A. If patient develops a new wide or narrow complex tachycardia, stop exercise.
B. Monitor HR and rhythm, BP, and oximetry. Provide oxygen at 2 to 4 L if hypoxemic. Obtain 12-lead ECG if available.
C. Assess for symptoms of instability or altered mental status, ischemic chest discomfort, HF, or hypotension, and notify supervising physician for evaluation and treatment. If directed by a physician, obtain IV access and prepare for synchronized cardioversion. If stable, may utilize vagal maneuvers or antiarrhythmic agents per ACLS guidelines.
D. Prepare for transfer to ED.
VIII. Dyspnea
A. If patient develops acute dyspnea, stop exercise and have patient sit down.
B. Monitor heart rate and rhythm, BP, respiratory rate, lung sounds, and oximetry. Provide oxygen at 2 to 4 L for oxygen saturation <94%.
C. If patient has a metered-dose inhaler, it may be administered as prescribed.
D. If condition deteriorates, notify supervising physician to evaluate for treatment options and possible transfer to ED.
E. If condition improves, notify primary care physician for further recommendations.
IX. Cerebrovascular Accident
A. If patient develops signs and symptoms of a stroke such as sudden arm or leg weakness, confusion, trouble speaking, dizziness, loss of balance or coordination, severe headache, or facial droop, immediately evaluate with rapid out-of-hospital stroke assessment.
B. If stroke is suspected, initiate EMS for immediate transport to a stroke facility.
C. Establish time of last known neurological baseline.
D. Maintain airway, breathing, and circulation.
E. Provide supplemental oxygen if hypoxemic or if oxygen saturation is unknown.
F. Check blood glucose.
G. Alert receiving hospital when patient is in transport.
X. Placement of IV Line
Purpose: To provide immediate access to administer emergency medication and IV fluids.
A. An attempt will be made to notify the supervising physician.
B. Place a saline lock in participant when one or more of the following apply:
- Angina pectoris protocol has been followed and chest pain persists.
- ECG, vital signs or participant appears to be clinically unstable or symptomatic.
- Physician directs the placement of IV line.
XI. Patient Transportation
Staff will meet and direct ambulance personnel to the patient treatment area.
Staff will prepare medical records to be sent with the patient as needed.
Staff will alert the emergency department of the patient transfer.
Cardiac Rehabilitation Department Emergency Procedures and Standing Orders Were Reviewed and Approved
___________________________________________
Physician's name
___________________________________________
Signature
___________________________________________
Date of most recent review
*Appendix B should be used only as an example of standing orders that might be considered and adopted for use in freestanding outpatient or community-based programs.
From American Association of Cardiovascular and Pulmonary Rehabilitation, Guidelines for Cardiac Rehabilitation Programs, 6th ed.
(Champaign, IL: Human Kinetics, 2021).
What are cardiac dysrhythmias?
By Alison L. Bailey, Alexis L. Beatty, Brian Carlin, Dennis J. Kerrigan, Steven J. Keteyian, Kirstine Laerum Sibilitz, Karen Lui, Ryan Mays, Jonathan Powell, Ray W. Squires, Diane J. Treat-Jacobson
Cardiac dysrhythmias are abnormalities in heart rhythm. They are also known as arrhythmias or irregular rhythms. Many CR participants have a history of cardiac dysrhythmias, and some experience dysrhythmias during CR participation.1-3 Symptoms from dysrhythmias may or may not be present and vary from patient to patient. The effects of dysrhythmias can range from generally benign to potentially harmful. Most studies report a cardiac arrest rate of approximately 1/100,000 patient-hours of CR participation.4-7 Although it is rare for dysrhythmias to have life-threatening consequences during exercise in CR programs, it remains important to recognize dysrhythmias and their features.
Bottom Line
Cardiac dysrhythmias are common in CR participants. Life-threatening consequences of cardiac dysrhythmias are rare during exercise in CR programs.
The following are commonly encountered dysrhythmias and symptoms:
Cardiac Dysrhythmias in CR
Generally Benign
- Premature atrial complexes (PACs)
- Isolated premature ventricular complexes (PVCs)
- AF or atrial flutter with controlled ventricular rate (8
- Paroxysmal supraventricular tachycardia (SVT)
- Mild bradycardia (50-60 bpm)
- First-degree atrioventricular (AV) block and asymptomatic type I second-degree (also known as Wenckebach) AV block
Potentially or Likely Harmful
- AF or atrial flutter with a rapid rate (≥110 bpm at rest)
- Symptomatic or severe bradycardia (HR <50)
- Symptomatic or advanced AV block (type II second-degree AV block or complete heart block)
- Ventricular tachycardia
- Ventricular fibrillation
Symptoms Associated With Cardiac Dysrhythmias
Stable Symptoms
- Palpitations
- Dizziness or lightheadedness
- Shortness of breath
- Chest pain or discomfort
Nonspecific or Associated Symptoms
- Weakness or fatigue
- Sweating
- Blurred vision
- Nausea
- Anxiety
- Edema
Unstable Symptoms
- Hypotension
- Near-syncope or loss of consciousness
- HF
- Unstable angina or MI
- Cardiac arrest
Exercise induces many physiologic effects, which can have both direct and indirect effects on cardiac electrophysiology. Exercise intensity can be related to the occurrence of dysrhythmias. Some dysrhythmias diminish or disappear with increasing exercise intensity; others increase or appear with increasing exercise intensity; and still others have no observable relationship to exercise intensity. Factors that can contribute to dysrhythmias during exercise include autonomic nervous system activity, ischemia, genetic abnormalities, structural heart disease, medications with proarrhythmic side effects, electrolyte imbalance, dehydration, and certain environmental factors.
Guideline 10.7 Dysrhythmia Exercise Prescription
For patients with known dysrhythmias, the exercise prescription should be tailored to the individual, with predetermined goals and criteria for exercise termination. Exercise should be terminated when a patient experiences a potentially harmful dysrhythmia or dysrhythmia with unstable symptoms.
Atrial Fibrillation
Light-to-moderate activities, particularly leisure-time activity and walking, are associated with a significantly lower incidence of AF in older adults.9 However, people who participate in extreme endurance training and sports activities may have an increased incidence of AF.10,11 For those diagnosed with AF, regular moderate PA is known to increase exercise capacity and control ventricular rate.12,13 In addition, exercise training increases exercise capacity and may reduce AF burden.14,15 The following information provides specific information about CR participation in patients who have AF.
AF originates in the atrium and is the most common cardiac arrhythmia. It is characterized by irregular contractions of the muscle fibers of the atria resulting in a variable HR. Risk factors associated with developing AF include PA, obesity, advanced age, HTN, HF, diabetes mellitus, CVD and valvular heart disease, left ventricular and atrial enlargement, and hyperthyroidism.43 Paradoxically, despite having few risk factors, athletes are also at increased risk for developing AF.
CR professionals will encounter these two types of patients with AF: patients who experience an initial (acute) onset (often noted during CR check-in or during exercise) and patients previously diagnosed and medically managed. Generally, AF is classified as (1) paroxysmal, (2) persistent, (3) long-standing persistent, or (4) permanent.2
AF should be considered when a patient presents with a rapid (often >110 bpm) “irregularly irregular” (no rhythmic pattern) resting HR. Patients experiencing an abrupt onset of AF may or may not report accompanying symptoms including palpitation, tachycardia, fatigue, shortness of breath, dizziness, and nausea. If AF is suspected, an ECG will confirm a diagnosis.
If new-onset AF is confirmed, the patient's physician should be consulted. Treating new-onset AF has three goals.44,50 The first goal is to mitigate symptoms by initially focusing in on reducing HR. Typical therapeutic HR reduction options include beta-adrenergic and calcium channel blocking agents and antiarrhythmic medication. The second goal is to reduce the risk for the development embolization of a blood clot (which the patient is at risk of developing due to atrial blood stagnation) through anticoagulation therapy. The third goal is to manage the patient's cardiovascular risk factors, which for overweight or obese patients is recommended to include weight loss and risk factor modification.50
Safety and rates of adverse event of exercise in patients have not been well studied. No large randomized control trials of exercise training and AF have assessed safety and efficacy. Guidelines for the treatment of patients with AF do not explicitly endorse specific exercise recommendations. Exercise, however, is not contraindicated in patients with AF. Moreover, exercise is effective treatment in multiple risk factors associated with AF, such as physical inactivity, HTN, diabetes mellitus, and obesity. Therefore, asymptomatic patients with AF who have received medical clearance should be encouraged to participate in an exercise program.
However, AF can profoundly impact the physiologic response to exercise training.45 In particular, the rapid, irregular contraction of the atrium results in reduced ventricular output. To compensate for the reduced cardiac output there is a commensurate increase in the rate and irregularity of ventricular contraction. Despite the negative impact of AF, exercise training studies have demonstrated improvements in functional capacity, health status, and quality of life.46
The special consideration regarding exercise testing and prescription for patients with AF have been detailed elsewhere.3 The following section is a brief review of special considerations regarding exercise testing and prescription for CR participants with AF.
Exercise Testing
As with all patients entering CR, undergoing a symptom-limited exercise tolerance test prior to initiating an exercise training program is optimal but not required. An exercise test is useful to assess for myocardial ischemia, evaluate chronotropic response, identify signs and symptoms, quantify functional capacity, and establish some general parameters for exercise training intensity.
Exercise Prescription for Patients With AF
Currently, no specific recommendations exist regarding exercise training for the treatment of AF. Studies of exercise training in patients with AF have employed a variety of protocols. Components of any exercise prescription include frequency, intensity, duration, modality, progression, and total volume. The exercise prescription for patients with AF should be individualized. A meta-analysis of exercise training studies involving people with AF recommends that a training regimen should include three or more sessions per week of a combination of moderate-intensity aerobic activity and resistance training. Session duration should be approximately 60 minutes, including adequate warm-up and cool-down.
By definition, the HR for a person with AF is irregular. Therefore, use of HR exclusively to assess exercise intensity is problematic. For aerobic training, in lieu of HR, use of RPE scale is an effective means to assess exercise intensity. A rating of 11 to 14 (on the Borg 6-20 scale) is typically associated with a moderate intensity that is approximately 70% to 85% of peak exercise capacity. Notably, very few studies have focused on the safety and efficacy of high-intensity aerobic training in patients with AF.
For overweight patients with AF, weight loss is recommended.47,50 To facilitate weight loss, orienting the exercise prescription to maximize caloric expenditure is indicated. High caloric exercise training (e.g., treadmill walking at a moderate intensity for an extended duration) in CR is well tolerated and an effective strategy to promote weight loss and improve multiple cardiovascular risk factors.48
No specific guidelines exist for resistance training for patients with AF. Given the lack of recommendations, using professional discretion is necessary when providing guidance regarding resistance training. Following the resistance training recommendations for other, non-AF CR participants is advisable. General recommendations for resistance training are found in chapter 6.
Related Books