
- Home
- Medicine in Exercise and Sport
- Health Care in Exercise and Sport
- Health Care for Special Conditions
- The Athlete’s Guide to Diabetes

The Athlete’s Guide to Diabetes
392 Pages
Renowned researcher and diabetes expert Dr. Sheri Colberg offers best practices and tips for managing blood glucose levels for athletes of all ages with type 1 and type 2 diabetes. She provides the most up-to-date information on
- insulin and other medications and their effects on exercise,
- nutritional practices and supplements, including low-carbohydrate eating,
- the latest technologies used to manage glucose, including continuous glucose monitoring (CGM),
- injury prevention and treatment as well as tactics for diabetes-related joint issues, and
- mental strategies for maximizing performance and optimizing health.
The Athlete’s Guide to Diabetes adheres to latest guidelines from such trusted sources as the American Diabetes Association and the American College of Sports Medicine. It is the one resource you can’t be without if you want to stay healthy and active, train smarter, and reach new levels of athletic success without losing control of your blood glucose management.
Earn continuing education credits/units! A continuing education exam that uses this book is also available. It may be purchased separately or as part of a package that includes both the book and exam.
Chapter 1. Training Basics for Fitness & Sports
Chapter 2. Balancing Exercise Blood Glucose
Chapter 3. Ups and Downs of Insulin and Other Medications
Chapter 4. Eating Right and Supplementing for Activity
Chapter 5. Using Technology and Monitoring to Enhance Performance
Chapter 6. Thinking and Acting Like an Athlete
Chapter 7. Preventing and Treating Athletic Injuries
Part II. Guidelines for Specific Activities
Chapter 8. Fitness Activities
Chapter 9. Endurance Sports
Chapter 10. Endurance–Power Sports
Chapter 11. Power Sports
Chapter 12. Outdoor Recreation and Sports
Appendix A. Diabetes, Sports, and Related Organizations
Appendix B. Diabetes, Sports, and Nutrition Websites
Sheri R. Colberg, PhD, FACSM, is an author, exercise physiologist, lecturer, consultant, and professor emerita of exercise science (Old Dominion University in Norfolk, Virginia). In 2016, she was the recipient of the American Diabetes Association’s Outstanding Educator in Diabetes award. A respected researcher and lecturer, she has authored more than 400 articles on exercise, diabetes, and health; 27 book chapters; and over a dozen books, including Diabetes-Free Kids, The 7 Step Diabetes Fitness Plan, 50 Secrets of the Longest Living People With Diabetes, The Science of Staying Young, Diabetic Athlete’s Handbook, The Diabetes Breakthrough, and Diabetes & Keeping Fit for Dummies.
A distinguished graduate of Stanford University (BA), University of California at Davis (MA), and University of California at Berkeley (PhD), Colberg consults professionally for the American Diabetes Association (ADA), American College of Sports Medicine (ACSM), Juvenile Diabetes Research Foundation (JDRF), American Association of Diabetes Educators (AADE), and Academy of Nutrition and Dietetics (AND) on numerous committees and projects. As a world-renowned expert and opinion leader, she has developed the exercise guidelines related to diabetes for most of these premier professional organizations, and she is interviewed frequently by various media outlets. In addition, she continues to be involved in consulting and in clinical research on exercise, diabetes, and healthy lifestyles.
With over 50 years of personal experience as an exerciser living with type 1 diabetes, Colberg continues to live a healthy, active lifestyle and serve as a role model for others who want to live long and well with (or without) diabetes. She enjoys working out regularly on conditioning machines, swimming, biking, fitness walking, weight training, and hiking with her husband and family in coastal California.
“In The Athlete’s Guide to Diabetes Sheri Colberg provides a wealth of information and guidance about exercise and diabetes—not just for elite athletes but for anyone living with diabetes who is involved in sports. Sheri includes advice about insulin (including the newer biosimilars), CGMs, pumps (including hybrid closed loops), other diabetes medications, and better food choices for exercise, including good options for snacks and hypoglycemia treatment. Furthermore, Sheri includes personal accounts from several athletes, with tips and tricks that have helped them be successful. The Athlete's Guide to Diabetes is a must-have for everyone with diabetes who takes exercise and sports seriously.”
—Jeff Hitchcock, President of Children With Diabetes
“Exercise is the billion-dollar drug that rarely gets prescribed. The Athlete’s Guide to Diabetes provides people with diabetes with the knowledge and tools to exercise safely and successfully. This book will serve as a priceless tool for anyone with diabetes. Thanks to Sheri for all her great work and helping get people with diabetes more active!”
—Phil Southerland, CEO and Cofounder of Team Novo Nordisk, President and Founder of Team Type 1 Foundation
Getting the most from diabetes technologies
Technology and software related to diabetes and health management are advancing faster than most people can keep up with.
Technology and software related to diabetes and health management are advancing faster than most people can keep up with. Every day a new app seems to come out to keep track of something, be it your blood glucose levels, insulin on board, and carbohydrate counting or your calories, daily steps, and fitness goals. In the diabetes world, the latest management technologies guide people in making more informed and effective regimen change decisions—the most important of which are integrated systems that can take charge of the decision making by combining delivery of insulin via pumps, continuous glucose monitoring (CGM), and a control system with potential artificial intelligence(AI) capabilities. Next down the pike is integration of wearable technologies, which can add information related to heart rate and more. More improvements will make AI even more capable of “learning” and updating algorithms to match the changes and patterns in your metabolic state.
Given the challenges of exercising with diabetes, the latest technologies can be beneficial for managing your blood glucose and maximizing the benefits of physical activity. Insulin pumps (covered fully in chapter 3) offer a more fine-tuned ability to regulate basal insulin levels and bolus doses. Blood glucose meters give immediate feedback on where your glucose is starting and how you are responding to an activity. The CGM devices provide an added level of safety by offering the opportunity for improved decision making in real-time and retrospectively. Closed-loop systems that integrate a pump and CGM manage the decision making for you; they can potentially improve your blood glucose management before and during exercise and allow you to avoid any unwanted rises and falls in your blood glucose after workouts. All forms of technology have inherent drawbacks and limitations, but you can overcome most of their issues with planning and knowledge.
Blood Glucose Meters (and Their Precursors)
If you began your journey with diabetes after the advent of home blood glucose meters, consider yourself lucky. Back in 1968 when I began my life with diabetes, no one had blood glucose meters to use for self-monitoring, much less target blood glucose ranges for exercise. All we had were urine tests, which measured the excess glucose and ketones in urine. You would pee in a cup, then put 5 drops of urine with 10 drops of water into a test tube with a tablet. The test tube mixture changed color in a range from cool blue (no glucose) to flaming orange (4+glucose). It did not give you the foggiest idea of what your blood glucose was doing right then; it only told you whether you had been higher than optimal a few hours before. In other words, you could be shaking with the symptoms of a low while watching your urine turn bright orange, the indication of being very high. The ketone test strips merely confirmed what you already knew: you had some ketones in your urine (and therefore your blood) most of the time because the diabetes management tools were lacking.
The next generation of urine test strips eliminated the precise drops and test tubes, but they were not necessarily an improvement. After dipping the test strip in your urine, you had to match the color of the strip to a chart on the side of a bottle. Your six choices ranged from light blue to dark brown, corresponding to negative (0), 100, 250, 500, 1,000, and 2,000 mg/dL or more. This still did not give you a clue about the level of your blood glucose.
The blood glucose test strips of the early 1980s would only estimate your blood glucose within maybe 40 mg/dL (2.2 mmol/L), assuming your glucose was under 200 mg/dL (11.1 mmol/L). Over that range, from one color block to the next, the number jumped up by 100 to 200 mg/dL or more. In other words, blood glucose strips still were not remotely precise enough to allow anyone to safely make regimen changes.
Relatively small and affordable blood glucose meters did not become widely available to individuals until the mid-1980s. I got my first one in 1986 after I had already been living with type 1 diabetes for 18 years. My first meter still had significant potential for user error because you had to blot the blood off the strip halfway through the 2-minute testing period. Even with access to reasonably accurate blood glucose measurements for the first time, we all experienced a steep learning curve while figuring out what to do with our food or insulin in response to the readings.
The moral of this story is that we have come a long way with diabetes technology, even if all you use currently is a blood glucose meter that gives you feedback in only 5 seconds. Appreciate having the ability to check what your blood glucose is doing at any given moment and learn to use that vital information to expertly manipulate your medication doses and diet.
With access to a blood glucose meter, you have the primary tool you need to manage your diabetes effectively, especially with exercise as an added variable. Check as frequently as you need to, with the goal of avoiding both lows and highs.
Even if you do not normally get low during exercise, checking frequently is still advisable, especially before you start and after you finish working out. Once you learn your usual responses to activities, you can usually anticipate how to react to keep your blood glucose in an optimal range to perform well.
Continuous Glucose Monitors
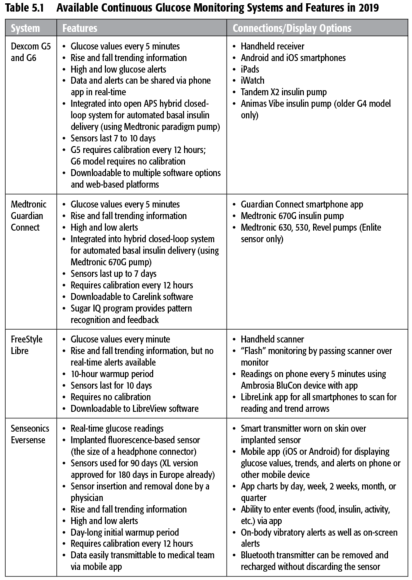
In the past decade or so, a number of continuous glucose monitoring (CGM) devices have received approval from the U.S. Food and Drug Administration (FDA), the European Commission, and across the world. To date, all of them are still invasive: they require that you place and keep a probe of some sort under your skin to get readings. While many innovators are working on noninvasive CGM devices, none have been approved or are available yet for use. At least one company (Senseonics) has FDA approval for an implantable CGM device called Eversense, which lasts for 3 months at a time, and they are seeking approval for up to 180 days. (I have heard that their sensors go in easily during an office visit, but they are more difficult to remove after 90 or 180 days. That is not surprising: that time span is more than sufficient for your body to develop an inflammation and grow new tissue around a foreign object embedded in your skin.)
These monitors by themselves only give you information—much like a blood glucose meter does—but you still have to check the readings and make regimen adjustments yourself. However, getting feedback in real-time or at least every 1 to 5 minutes, 24 hours a day, can be extremely useful when you are trying to learn your patterns, see the trends, or keep your blood glucose in a tighter range with less hypoglycemia. The accuracy of these meters has been improving over time, but they are all still limited by their physiological methods: there is a lag of at least 6 to 20 minutes between the glucose they measure (in interstitialspaces between cells in the skin) and your actual blood glucose. This lag can be even greater during times when your blood glucose levels are often changing rapidly, such as after a meal or during exercise.
The CGM devices and models approved and available in the United States as of the publication of this book are shown in table 5.1. “Flash” glucose monitoring (as offered by the FreeStyle Libre device) is a recent innovation, possessing some but not all features of traditional CGM. Flash monitors can provide instantaneous glucose values and recent trends, but they lack the alerts for lows and highs.
Insurance reimbursement also has become more reasonable since CGM devices were first introduced over a decade ago. (I paid $35 out of pocket for each 3-day sensor for the first-generation Dexcom CGM I tried.) Currently, at least one model is covered by Medicare for anyone with type 1 diabetes age 65 and over. Studies have shown that people with type 2 diabetes—especially those using insulin—can also benefit from using CGM, but coverage for them has been an even harder sell to insurance companies so far. In any case, the number of model choices has declined recently, and their cost is still prohibitive for people who lack the insurance coverage.
What's more, CGM technology is not infallible. As I have noted, a major drawback of CGM devices used during exercise is that their glucose readings are not fully real-time because they measure glucose levels in your skin rather than in your blood, and it takes some time for glucose to move between these two parts of your body. Also, CGM users may have problems getting the device to stay put, similar to the issues experienced by pump users with their infusion sites. (Refer back to table 3.2 for solutions on resolving adhesion issues and to the list of strategies used by athletes in chapter 12; most of the tactics used to secure a pump infusion site will also work for CGM devices.) Other reported challenges include variable sensor accuracy, variable performance between sensors, breakage of sensor filaments, transportation of the sensor display, and inability to calibrate CGM during exercise. (If you have the option, you may want to use an integrated watch to display your values.) Although technical failures during exercise are possible even with the newer versions of these monitors, CGM is still the wave of the future when it comes to monitoring and managing blood glucose.
Exercisers have reported a compression effect when wearing the CGM sensor in areas underneath compression shorts, resulting in a greater lag time in readings due to reduced blood flow to areas with compressed skin. This can also happen when you lie directly on the sensors.
If you have access to CGM, you may be able to use either traditional CGM or Flash monitors to enhance your exercise experience in a variety of ways.
- Seeing your glucose values before exercise tells you whether you are likely to need extra carbohydrates, insulin reductions, or an insulin bolus.
- Knowing your glucose trends before you start to work out can also help you make more informed decisions about any necessary changes in your food or medications.
- High and low alerts during and after exercise can help you avoid dangerous glucose extremes, particularly if you set your alerts at preemptive or conservative levels.
- Reviewing your trend graph reports after working out can show you the patterns of your exercise highs and lows, particularly if you use event markers or workout logs.
Many exercisers swear by their CGM devices and do not want to have to live without them (and hopefully they will not ever have to). But if you do not have access to CGM due to lack of insurance coverage, availability in your country, or other reasons, do not despair—you can still learn your glucose patterns by using frequent checks with a blood glucose meter, as most of us have done. In general, most athletes using CGM have found that observing their glucose trends (shown by up, steady, or down arrows) can be helpful during exercise, even when the readings lag behind actual blood glucose or are sometimes inaccurate.
Troubleshooting your performance like an athlete
As you have come to realize in this chapter, being an athlete is mostly a state of mind. However, sometimes your performance when you are an athlete with diabetes also depends on overcoming some regimen obstacles and other physical issues.
As you have come to realize in this chapter, being an athlete is mostly a state of mind. However, sometimes your performance when you are an athlete with diabetes also depends on overcoming some regimen obstacles and other physical issues. In this final section, you will learn all you need to perform like a professional athlete.
As discussed back in chapter 2, many different factors can impact your blood glucose responses, and the more you know about them, the better equipped you are to figure out what works best for you in almost every situation. Regardless of how knowledgeable you are, this process always takes some trial and error. Consider using some of the following strategies if you are experiencing any of these issues with being active.
Managing Exercise-Associated Hypoglycemia
Having to slow down or stop during an activity due to low blood glucose is annoying even to recreational athletes. It can also compromise your ability to complete your event, competition, or just your daily workout. It is worth keeping this from happening if you can. If you have been having any exercise-related lows, consider taking some of these actions or precautions to avoid them, especially if you use insulin.
Lows During and After Exercise—Food Intake
- Treat lows with glucose or other rapidly absorbed carbohydrate first, and follow that up with other balanced foods and drinks if needed to keep from dropping later.
- Choose pre-exercise foods that require the smallest amount of (or no) insulin to cover them to keep your circulating insulin lower during activities.
- Take in extra carbohydrate before, during, and after activities (depending on your exercise intensity and duration, starting blood glucose, normal diet, and other factors).
- Consider using protein and/or fat intake during prolonged activities to help prevent lows, especially past the first hour of activity, because they take longer to digest.
- Consume some protein and/or fat shortly after exercise and possibly also at bedtime to counteract lows later on and overnight.
Lows During and After Exercise—Insulin Adjustments
- Exercise when your insulin levels are lower, such as before meals or first thing in the morning before taking any bolus insulin.
- Before doing longer duration exercise, lower your insulin levels in anticipation by cutting back on your dose(s) of bolus and/or basal insulin.
- Lower the dose of any rapid-acting insulin you take within 2 to 3 hours before doing an activity (or set a lower basal rate on your insulin pump, if you use one).
- If using an insulin pump, consider lowering your basal rate for up to 2 hours before the start of exercise as well as during (and likely after) the activity.
- If you are prone to lows after exercise, reduce your dose of rapid-acting insulin given after any activity, or set a temporary lower basal rate on your pump for 4 to 12 hours.
- If you inject your basal insulin (Lantus, Basaglar, Levemir, or Toujeo), consider splitting the dose (although not necessarily evenly) to give it twice daily to allow for easier dose reductions before and after activity.
- If you use an even longer-acting basal insulin like Tresiba, watch out for possible insulin “stacking” on subsequent days, particularly when you are more active than normal.
Training Effects and Other Considerations
- Check your blood glucose more often when doing a new activity or unaccustomed exercise because both are more likely to result in lows, both during and afterward.
- Check frequently if you have had a bad low or exercised hard in the 24 hours before your latest workout because both may blunt your release of glucose-raising hormones.
- Try doing an all-out sprint for 10 to 30 seconds to help counteract most lows during exercise, but only if your insulin levels are not too high.
- If you plan on doing both aerobic and resistance training during a workout, vary the order based on whether you want your glucose to stay more stable (during resistance work) or possibly decrease (during moderate aerobic work, although intense training may raise it).
- Keep in mind that the rate of insulin absorption from skin depots depends on the size of the dose: smaller doses (1 to 3 units) are absorbed more rapidly than larger ones (5 or more units), which linger longer while you are active.
- Do not forget that your overall insulin needs are lower when you are regularly active; you may need permanently lower basal (and mealtime bolus) insulin doses.
- Avoid massaging the area where you just gave some insulin—massaging it can speed up its absorption.
- Remember that getting in a hot tub or having other prolonged heat exposure can speed up the absorption of any insulin taken (causing lows first, then highs later).
Dealing With Exercise Hyperglycemia
If you have experienced high blood glucose related to being active, it can be hard to always pinpoint the source of the rise and take actions to prevent or manage it. Consider these possible scenarios and some solutions for troubleshooting.
Highs Before Exercise
- If your blood glucose is over 250 mg/dL (13.9 mmol/L) and has been elevated for a few hours, consider giving yourself some insulin and waiting for the level to decrease before starting to exercise (especially with moderate or higher blood and urine ketones).
- If you take a dose of insulin to lower your glucose with a plan to start exercising shortly thereafter, take less than you normally would (50 percent or less) to prevent your blood glucose from dropping too rapidly during the activity.
- If your blood glucose is over 300 mg/dL (16.7 mmol/L) with no ketones, exercise only if you feel well and use caution because you can dehydrate more easily.
Highs During or After Exercise
- Cut back on your carbohydrate intake during exercise, reduce your insulin less, or take extra insulin after exercise (albeit less than normal).
- Remember that eating a full meal within an hour of starting exercise can slow digestion and result in high blood glucose for 1 to 2 hours afterward, particularly when you have consumed lower glycemic index items (refer to chapter 4 for a discussion of the glycemic index).
- If you disconnect your pump during activities and your blood glucose starts to rise, reconnect at least once an hour and take at least a portion of your missed basal.
- Consider giving yourself some of your “missed” basal insulin in advance in some cases, such as when you have disconnected from your pump before a swim.
- Consider using an “untethered” pump regimen—that is, giving some of your insulin as an injection of long-acting insulin (e.g., Lantus, Levemir, Tresiba) and the rest via pump with a reduced basal rate; then if you disconnect, you still have some basal on board.
- For early morning exercise before eating, consider giving yourself a small dose of insulin (less than normal) and/or a small snack to break your fast to reduce cortisol levels that can lead to elevations at that time of day.
- If the stress or intensity of competitions affects you, keep your basal insulin higher and only give yourself 50 percent or less of your usual correction dose to lower glucose.
- Stay hydrated during activities because dehydration can make blood glucose seem higher (due to being more concentrated) and lead to excess correction dosing.
- Consider doing some easy aerobic exercise after more intense workouts to lower blood glucose naturally.
Training Effects and Other Considerations
- After you have trained for a few weeks doing an activity, you may need fewer carbohydrates or smaller insulin reductions than before training due to a greater use of fat.
- Both endurance training and fat adaptation (from a low-carbohydrate diet) increase your body's efficiency at using fat as a fuel during aerobic activities that are submaximal.
- When you get very sore from exercise (peaking 2 or 3 days afterward), you may be more insulin resistant because you cannot restore muscle glycogen until your muscle damage from the activity is repaired.
- If you load up on carbohydrates before events, you should take enough insulin to cover them; otherwise, loading can raise your blood glucose and limit glycogen storage (check out the discussion on carbohydrate loading in chapter 3).
- You should keep your insulin from getting too hot or too cold; otherwise, its action may diminish and cause your usual doses to inadequately cover your insulin needs.
- Injected or pumped bolus insulin is absorbed faster in smaller doses; after a larger dose, you may end up too high first and then too low later on.
- Smaller doses of injected basal insulin are also absorbed more rapidly than larger ones (think 5 units versus 20), and they often do not last as long as expected.
Understand hormonal responses to exercise
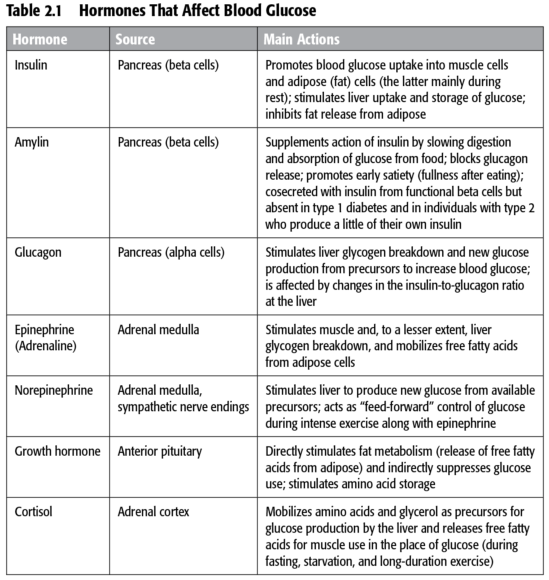
The human body only has insulin to lower blood glucose but has five hormones that raise it (with some overlap).
The human body only has insulin to lower blood glucose but has five hormones that raise it (with some overlap). This hormone redundancy tells you that, at least from a survival standpoint, your body is desperate to make sure you do not run out of blood glucose; it is not as concerned about you having too much. Insulin is an important hormone for regulating your body's storage of fuels (carbohydrate, fat, and protein) after you eat. It tells your insulin-sensitive cells (mainly your muscle and fat cells but also your liver) to take up glucose and fat to store them for later as muscle and liver glycogen (the storage form of glucose) as well as stored fat. During exercise, any insulin in your bloodstream can make your muscles take up extra blood glucose. In people who have a pancreas that functions normally, insulin levels typically decrease during exercise, and levels of a hormone called glucagon (released from the alpha cells of the pancreas) rise to stimulate glucose release.
Your blood glucose levels are managed by your liver, which would normally respond to the relative amounts of insulin and glucagon (table 2.1). Insulin and glucagon released from the pancreas go directly to the liver via the portal circulation. After a meal, high insulin and glucose levels tell the liver to store glucose for later use; fasting overnight or doing extended exercise leads to glucagon signaling the liver to release glucose. How people with type 1 diabetes respond hormonally to exercise is a major issue: the insulin and glucagon at the level of the liver are seldom perfectly normal because their insulin is injected or pumped under the skin rather than released directly from the pancreas.
People with type 1 diabetes have an altered hormonal response to exercise when their peripheral insulin is relatively high; lowering the circulating level of insulin helps normalize their hormone response.
All exercise causes the release of hormones that increase the production of glucose by your liver and lower your muscular use, based on how long and hard you exercise. Easy and moderate activities only release a small amount of glucose-raising hormones (unless you do them for a very long duration), but intense exercise such as heavy resistance training, sprinting, or high-intensity intervals causes an immediate rise in your blood glucose and leads to an exaggerated release of hormones. These hormones include adrenaline (formally known as epinephrine) and norepinephrine, which are released by the sympathetic nervous system (allowing your body to respond to physical or mental stressors with an increased heart rate), as well as glucagon, growth hormone, and cortisol (see table 2.1). The effects of these glucose-raising hormones can easily exceed your body's immediate need for glucose, especially because high-intensity exercise may not last long. As a result, your blood glucose often rises during and after short bouts of intense activity.
Intense exercise can cause a large increase in blood glucose because of your body's exaggerated release of glucose-raising hormones such as adrenaline and glucagon.
You may be more insulin resistant immediately after intense exercise and for a few hours due to these hormones. In one study, after near-maximal cycling to exhaustion, one group of people with type 1 diabetes on insulin pumps experienced elevated blood glucose levels for nearly 2 hours. Similarly, in exercisers with type 2 diabetes, blood glucose also rose for 1 hour in response to maximal cycling, as did their insulin levels (because their bodies still produced their own insulin). You may need some supplemental insulin to bring your blood glucose back down (albeit less than normal), or it may drop slowly over time on its own. After these hormones wane, your blood glucose may easily drop later when your body is working hard to restore the muscle glycogen you used during the activity. Be on the lookout for later-onset lows in these cases.
Getting the most from diabetes technologies
Technology and software related to diabetes and health management are advancing faster than most people can keep up with.
Technology and software related to diabetes and health management are advancing faster than most people can keep up with. Every day a new app seems to come out to keep track of something, be it your blood glucose levels, insulin on board, and carbohydrate counting or your calories, daily steps, and fitness goals. In the diabetes world, the latest management technologies guide people in making more informed and effective regimen change decisions—the most important of which are integrated systems that can take charge of the decision making by combining delivery of insulin via pumps, continuous glucose monitoring (CGM), and a control system with potential artificial intelligence(AI) capabilities. Next down the pike is integration of wearable technologies, which can add information related to heart rate and more. More improvements will make AI even more capable of “learning” and updating algorithms to match the changes and patterns in your metabolic state.
Given the challenges of exercising with diabetes, the latest technologies can be beneficial for managing your blood glucose and maximizing the benefits of physical activity. Insulin pumps (covered fully in chapter 3) offer a more fine-tuned ability to regulate basal insulin levels and bolus doses. Blood glucose meters give immediate feedback on where your glucose is starting and how you are responding to an activity. The CGM devices provide an added level of safety by offering the opportunity for improved decision making in real-time and retrospectively. Closed-loop systems that integrate a pump and CGM manage the decision making for you; they can potentially improve your blood glucose management before and during exercise and allow you to avoid any unwanted rises and falls in your blood glucose after workouts. All forms of technology have inherent drawbacks and limitations, but you can overcome most of their issues with planning and knowledge.
Blood Glucose Meters (and Their Precursors)
If you began your journey with diabetes after the advent of home blood glucose meters, consider yourself lucky. Back in 1968 when I began my life with diabetes, no one had blood glucose meters to use for self-monitoring, much less target blood glucose ranges for exercise. All we had were urine tests, which measured the excess glucose and ketones in urine. You would pee in a cup, then put 5 drops of urine with 10 drops of water into a test tube with a tablet. The test tube mixture changed color in a range from cool blue (no glucose) to flaming orange (4+glucose). It did not give you the foggiest idea of what your blood glucose was doing right then; it only told you whether you had been higher than optimal a few hours before. In other words, you could be shaking with the symptoms of a low while watching your urine turn bright orange, the indication of being very high. The ketone test strips merely confirmed what you already knew: you had some ketones in your urine (and therefore your blood) most of the time because the diabetes management tools were lacking.
The next generation of urine test strips eliminated the precise drops and test tubes, but they were not necessarily an improvement. After dipping the test strip in your urine, you had to match the color of the strip to a chart on the side of a bottle. Your six choices ranged from light blue to dark brown, corresponding to negative (0), 100, 250, 500, 1,000, and 2,000 mg/dL or more. This still did not give you a clue about the level of your blood glucose.
The blood glucose test strips of the early 1980s would only estimate your blood glucose within maybe 40 mg/dL (2.2 mmol/L), assuming your glucose was under 200 mg/dL (11.1 mmol/L). Over that range, from one color block to the next, the number jumped up by 100 to 200 mg/dL or more. In other words, blood glucose strips still were not remotely precise enough to allow anyone to safely make regimen changes.
Relatively small and affordable blood glucose meters did not become widely available to individuals until the mid-1980s. I got my first one in 1986 after I had already been living with type 1 diabetes for 18 years. My first meter still had significant potential for user error because you had to blot the blood off the strip halfway through the 2-minute testing period. Even with access to reasonably accurate blood glucose measurements for the first time, we all experienced a steep learning curve while figuring out what to do with our food or insulin in response to the readings.
The moral of this story is that we have come a long way with diabetes technology, even if all you use currently is a blood glucose meter that gives you feedback in only 5 seconds. Appreciate having the ability to check what your blood glucose is doing at any given moment and learn to use that vital information to expertly manipulate your medication doses and diet.
With access to a blood glucose meter, you have the primary tool you need to manage your diabetes effectively, especially with exercise as an added variable. Check as frequently as you need to, with the goal of avoiding both lows and highs.
Even if you do not normally get low during exercise, checking frequently is still advisable, especially before you start and after you finish working out. Once you learn your usual responses to activities, you can usually anticipate how to react to keep your blood glucose in an optimal range to perform well.
Continuous Glucose Monitors
In the past decade or so, a number of continuous glucose monitoring (CGM) devices have received approval from the U.S. Food and Drug Administration (FDA), the European Commission, and across the world. To date, all of them are still invasive: they require that you place and keep a probe of some sort under your skin to get readings. While many innovators are working on noninvasive CGM devices, none have been approved or are available yet for use. At least one company (Senseonics) has FDA approval for an implantable CGM device called Eversense, which lasts for 3 months at a time, and they are seeking approval for up to 180 days. (I have heard that their sensors go in easily during an office visit, but they are more difficult to remove after 90 or 180 days. That is not surprising: that time span is more than sufficient for your body to develop an inflammation and grow new tissue around a foreign object embedded in your skin.)
These monitors by themselves only give you information—much like a blood glucose meter does—but you still have to check the readings and make regimen adjustments yourself. However, getting feedback in real-time or at least every 1 to 5 minutes, 24 hours a day, can be extremely useful when you are trying to learn your patterns, see the trends, or keep your blood glucose in a tighter range with less hypoglycemia. The accuracy of these meters has been improving over time, but they are all still limited by their physiological methods: there is a lag of at least 6 to 20 minutes between the glucose they measure (in interstitialspaces between cells in the skin) and your actual blood glucose. This lag can be even greater during times when your blood glucose levels are often changing rapidly, such as after a meal or during exercise.
The CGM devices and models approved and available in the United States as of the publication of this book are shown in table 5.1. “Flash” glucose monitoring (as offered by the FreeStyle Libre device) is a recent innovation, possessing some but not all features of traditional CGM. Flash monitors can provide instantaneous glucose values and recent trends, but they lack the alerts for lows and highs.
Insurance reimbursement also has become more reasonable since CGM devices were first introduced over a decade ago. (I paid $35 out of pocket for each 3-day sensor for the first-generation Dexcom CGM I tried.) Currently, at least one model is covered by Medicare for anyone with type 1 diabetes age 65 and over. Studies have shown that people with type 2 diabetes—especially those using insulin—can also benefit from using CGM, but coverage for them has been an even harder sell to insurance companies so far. In any case, the number of model choices has declined recently, and their cost is still prohibitive for people who lack the insurance coverage.
What's more, CGM technology is not infallible. As I have noted, a major drawback of CGM devices used during exercise is that their glucose readings are not fully real-time because they measure glucose levels in your skin rather than in your blood, and it takes some time for glucose to move between these two parts of your body. Also, CGM users may have problems getting the device to stay put, similar to the issues experienced by pump users with their infusion sites. (Refer back to table 3.2 for solutions on resolving adhesion issues and to the list of strategies used by athletes in chapter 12; most of the tactics used to secure a pump infusion site will also work for CGM devices.) Other reported challenges include variable sensor accuracy, variable performance between sensors, breakage of sensor filaments, transportation of the sensor display, and inability to calibrate CGM during exercise. (If you have the option, you may want to use an integrated watch to display your values.) Although technical failures during exercise are possible even with the newer versions of these monitors, CGM is still the wave of the future when it comes to monitoring and managing blood glucose.
Exercisers have reported a compression effect when wearing the CGM sensor in areas underneath compression shorts, resulting in a greater lag time in readings due to reduced blood flow to areas with compressed skin. This can also happen when you lie directly on the sensors.
If you have access to CGM, you may be able to use either traditional CGM or Flash monitors to enhance your exercise experience in a variety of ways.
- Seeing your glucose values before exercise tells you whether you are likely to need extra carbohydrates, insulin reductions, or an insulin bolus.
- Knowing your glucose trends before you start to work out can also help you make more informed decisions about any necessary changes in your food or medications.
- High and low alerts during and after exercise can help you avoid dangerous glucose extremes, particularly if you set your alerts at preemptive or conservative levels.
- Reviewing your trend graph reports after working out can show you the patterns of your exercise highs and lows, particularly if you use event markers or workout logs.
Many exercisers swear by their CGM devices and do not want to have to live without them (and hopefully they will not ever have to). But if you do not have access to CGM due to lack of insurance coverage, availability in your country, or other reasons, do not despair—you can still learn your glucose patterns by using frequent checks with a blood glucose meter, as most of us have done. In general, most athletes using CGM have found that observing their glucose trends (shown by up, steady, or down arrows) can be helpful during exercise, even when the readings lag behind actual blood glucose or are sometimes inaccurate.
Troubleshooting your performance like an athlete
As you have come to realize in this chapter, being an athlete is mostly a state of mind. However, sometimes your performance when you are an athlete with diabetes also depends on overcoming some regimen obstacles and other physical issues.
As you have come to realize in this chapter, being an athlete is mostly a state of mind. However, sometimes your performance when you are an athlete with diabetes also depends on overcoming some regimen obstacles and other physical issues. In this final section, you will learn all you need to perform like a professional athlete.
As discussed back in chapter 2, many different factors can impact your blood glucose responses, and the more you know about them, the better equipped you are to figure out what works best for you in almost every situation. Regardless of how knowledgeable you are, this process always takes some trial and error. Consider using some of the following strategies if you are experiencing any of these issues with being active.
Managing Exercise-Associated Hypoglycemia
Having to slow down or stop during an activity due to low blood glucose is annoying even to recreational athletes. It can also compromise your ability to complete your event, competition, or just your daily workout. It is worth keeping this from happening if you can. If you have been having any exercise-related lows, consider taking some of these actions or precautions to avoid them, especially if you use insulin.
Lows During and After Exercise—Food Intake
- Treat lows with glucose or other rapidly absorbed carbohydrate first, and follow that up with other balanced foods and drinks if needed to keep from dropping later.
- Choose pre-exercise foods that require the smallest amount of (or no) insulin to cover them to keep your circulating insulin lower during activities.
- Take in extra carbohydrate before, during, and after activities (depending on your exercise intensity and duration, starting blood glucose, normal diet, and other factors).
- Consider using protein and/or fat intake during prolonged activities to help prevent lows, especially past the first hour of activity, because they take longer to digest.
- Consume some protein and/or fat shortly after exercise and possibly also at bedtime to counteract lows later on and overnight.
Lows During and After Exercise—Insulin Adjustments
- Exercise when your insulin levels are lower, such as before meals or first thing in the morning before taking any bolus insulin.
- Before doing longer duration exercise, lower your insulin levels in anticipation by cutting back on your dose(s) of bolus and/or basal insulin.
- Lower the dose of any rapid-acting insulin you take within 2 to 3 hours before doing an activity (or set a lower basal rate on your insulin pump, if you use one).
- If using an insulin pump, consider lowering your basal rate for up to 2 hours before the start of exercise as well as during (and likely after) the activity.
- If you are prone to lows after exercise, reduce your dose of rapid-acting insulin given after any activity, or set a temporary lower basal rate on your pump for 4 to 12 hours.
- If you inject your basal insulin (Lantus, Basaglar, Levemir, or Toujeo), consider splitting the dose (although not necessarily evenly) to give it twice daily to allow for easier dose reductions before and after activity.
- If you use an even longer-acting basal insulin like Tresiba, watch out for possible insulin “stacking” on subsequent days, particularly when you are more active than normal.
Training Effects and Other Considerations
- Check your blood glucose more often when doing a new activity or unaccustomed exercise because both are more likely to result in lows, both during and afterward.
- Check frequently if you have had a bad low or exercised hard in the 24 hours before your latest workout because both may blunt your release of glucose-raising hormones.
- Try doing an all-out sprint for 10 to 30 seconds to help counteract most lows during exercise, but only if your insulin levels are not too high.
- If you plan on doing both aerobic and resistance training during a workout, vary the order based on whether you want your glucose to stay more stable (during resistance work) or possibly decrease (during moderate aerobic work, although intense training may raise it).
- Keep in mind that the rate of insulin absorption from skin depots depends on the size of the dose: smaller doses (1 to 3 units) are absorbed more rapidly than larger ones (5 or more units), which linger longer while you are active.
- Do not forget that your overall insulin needs are lower when you are regularly active; you may need permanently lower basal (and mealtime bolus) insulin doses.
- Avoid massaging the area where you just gave some insulin—massaging it can speed up its absorption.
- Remember that getting in a hot tub or having other prolonged heat exposure can speed up the absorption of any insulin taken (causing lows first, then highs later).
Dealing With Exercise Hyperglycemia
If you have experienced high blood glucose related to being active, it can be hard to always pinpoint the source of the rise and take actions to prevent or manage it. Consider these possible scenarios and some solutions for troubleshooting.
Highs Before Exercise
- If your blood glucose is over 250 mg/dL (13.9 mmol/L) and has been elevated for a few hours, consider giving yourself some insulin and waiting for the level to decrease before starting to exercise (especially with moderate or higher blood and urine ketones).
- If you take a dose of insulin to lower your glucose with a plan to start exercising shortly thereafter, take less than you normally would (50 percent or less) to prevent your blood glucose from dropping too rapidly during the activity.
- If your blood glucose is over 300 mg/dL (16.7 mmol/L) with no ketones, exercise only if you feel well and use caution because you can dehydrate more easily.
Highs During or After Exercise
- Cut back on your carbohydrate intake during exercise, reduce your insulin less, or take extra insulin after exercise (albeit less than normal).
- Remember that eating a full meal within an hour of starting exercise can slow digestion and result in high blood glucose for 1 to 2 hours afterward, particularly when you have consumed lower glycemic index items (refer to chapter 4 for a discussion of the glycemic index).
- If you disconnect your pump during activities and your blood glucose starts to rise, reconnect at least once an hour and take at least a portion of your missed basal.
- Consider giving yourself some of your “missed” basal insulin in advance in some cases, such as when you have disconnected from your pump before a swim.
- Consider using an “untethered” pump regimen—that is, giving some of your insulin as an injection of long-acting insulin (e.g., Lantus, Levemir, Tresiba) and the rest via pump with a reduced basal rate; then if you disconnect, you still have some basal on board.
- For early morning exercise before eating, consider giving yourself a small dose of insulin (less than normal) and/or a small snack to break your fast to reduce cortisol levels that can lead to elevations at that time of day.
- If the stress or intensity of competitions affects you, keep your basal insulin higher and only give yourself 50 percent or less of your usual correction dose to lower glucose.
- Stay hydrated during activities because dehydration can make blood glucose seem higher (due to being more concentrated) and lead to excess correction dosing.
- Consider doing some easy aerobic exercise after more intense workouts to lower blood glucose naturally.
Training Effects and Other Considerations
- After you have trained for a few weeks doing an activity, you may need fewer carbohydrates or smaller insulin reductions than before training due to a greater use of fat.
- Both endurance training and fat adaptation (from a low-carbohydrate diet) increase your body's efficiency at using fat as a fuel during aerobic activities that are submaximal.
- When you get very sore from exercise (peaking 2 or 3 days afterward), you may be more insulin resistant because you cannot restore muscle glycogen until your muscle damage from the activity is repaired.
- If you load up on carbohydrates before events, you should take enough insulin to cover them; otherwise, loading can raise your blood glucose and limit glycogen storage (check out the discussion on carbohydrate loading in chapter 3).
- You should keep your insulin from getting too hot or too cold; otherwise, its action may diminish and cause your usual doses to inadequately cover your insulin needs.
- Injected or pumped bolus insulin is absorbed faster in smaller doses; after a larger dose, you may end up too high first and then too low later on.
- Smaller doses of injected basal insulin are also absorbed more rapidly than larger ones (think 5 units versus 20), and they often do not last as long as expected.
Understand hormonal responses to exercise
The human body only has insulin to lower blood glucose but has five hormones that raise it (with some overlap).
The human body only has insulin to lower blood glucose but has five hormones that raise it (with some overlap). This hormone redundancy tells you that, at least from a survival standpoint, your body is desperate to make sure you do not run out of blood glucose; it is not as concerned about you having too much. Insulin is an important hormone for regulating your body's storage of fuels (carbohydrate, fat, and protein) after you eat. It tells your insulin-sensitive cells (mainly your muscle and fat cells but also your liver) to take up glucose and fat to store them for later as muscle and liver glycogen (the storage form of glucose) as well as stored fat. During exercise, any insulin in your bloodstream can make your muscles take up extra blood glucose. In people who have a pancreas that functions normally, insulin levels typically decrease during exercise, and levels of a hormone called glucagon (released from the alpha cells of the pancreas) rise to stimulate glucose release.
Your blood glucose levels are managed by your liver, which would normally respond to the relative amounts of insulin and glucagon (table 2.1). Insulin and glucagon released from the pancreas go directly to the liver via the portal circulation. After a meal, high insulin and glucose levels tell the liver to store glucose for later use; fasting overnight or doing extended exercise leads to glucagon signaling the liver to release glucose. How people with type 1 diabetes respond hormonally to exercise is a major issue: the insulin and glucagon at the level of the liver are seldom perfectly normal because their insulin is injected or pumped under the skin rather than released directly from the pancreas.
People with type 1 diabetes have an altered hormonal response to exercise when their peripheral insulin is relatively high; lowering the circulating level of insulin helps normalize their hormone response.
All exercise causes the release of hormones that increase the production of glucose by your liver and lower your muscular use, based on how long and hard you exercise. Easy and moderate activities only release a small amount of glucose-raising hormones (unless you do them for a very long duration), but intense exercise such as heavy resistance training, sprinting, or high-intensity intervals causes an immediate rise in your blood glucose and leads to an exaggerated release of hormones. These hormones include adrenaline (formally known as epinephrine) and norepinephrine, which are released by the sympathetic nervous system (allowing your body to respond to physical or mental stressors with an increased heart rate), as well as glucagon, growth hormone, and cortisol (see table 2.1). The effects of these glucose-raising hormones can easily exceed your body's immediate need for glucose, especially because high-intensity exercise may not last long. As a result, your blood glucose often rises during and after short bouts of intense activity.
Intense exercise can cause a large increase in blood glucose because of your body's exaggerated release of glucose-raising hormones such as adrenaline and glucagon.
You may be more insulin resistant immediately after intense exercise and for a few hours due to these hormones. In one study, after near-maximal cycling to exhaustion, one group of people with type 1 diabetes on insulin pumps experienced elevated blood glucose levels for nearly 2 hours. Similarly, in exercisers with type 2 diabetes, blood glucose also rose for 1 hour in response to maximal cycling, as did their insulin levels (because their bodies still produced their own insulin). You may need some supplemental insulin to bring your blood glucose back down (albeit less than normal), or it may drop slowly over time on its own. After these hormones wane, your blood glucose may easily drop later when your body is working hard to restore the muscle glycogen you used during the activity. Be on the lookout for later-onset lows in these cases.
Getting the most from diabetes technologies
Technology and software related to diabetes and health management are advancing faster than most people can keep up with.
Technology and software related to diabetes and health management are advancing faster than most people can keep up with. Every day a new app seems to come out to keep track of something, be it your blood glucose levels, insulin on board, and carbohydrate counting or your calories, daily steps, and fitness goals. In the diabetes world, the latest management technologies guide people in making more informed and effective regimen change decisions—the most important of which are integrated systems that can take charge of the decision making by combining delivery of insulin via pumps, continuous glucose monitoring (CGM), and a control system with potential artificial intelligence(AI) capabilities. Next down the pike is integration of wearable technologies, which can add information related to heart rate and more. More improvements will make AI even more capable of “learning” and updating algorithms to match the changes and patterns in your metabolic state.
Given the challenges of exercising with diabetes, the latest technologies can be beneficial for managing your blood glucose and maximizing the benefits of physical activity. Insulin pumps (covered fully in chapter 3) offer a more fine-tuned ability to regulate basal insulin levels and bolus doses. Blood glucose meters give immediate feedback on where your glucose is starting and how you are responding to an activity. The CGM devices provide an added level of safety by offering the opportunity for improved decision making in real-time and retrospectively. Closed-loop systems that integrate a pump and CGM manage the decision making for you; they can potentially improve your blood glucose management before and during exercise and allow you to avoid any unwanted rises and falls in your blood glucose after workouts. All forms of technology have inherent drawbacks and limitations, but you can overcome most of their issues with planning and knowledge.
Blood Glucose Meters (and Their Precursors)
If you began your journey with diabetes after the advent of home blood glucose meters, consider yourself lucky. Back in 1968 when I began my life with diabetes, no one had blood glucose meters to use for self-monitoring, much less target blood glucose ranges for exercise. All we had were urine tests, which measured the excess glucose and ketones in urine. You would pee in a cup, then put 5 drops of urine with 10 drops of water into a test tube with a tablet. The test tube mixture changed color in a range from cool blue (no glucose) to flaming orange (4+glucose). It did not give you the foggiest idea of what your blood glucose was doing right then; it only told you whether you had been higher than optimal a few hours before. In other words, you could be shaking with the symptoms of a low while watching your urine turn bright orange, the indication of being very high. The ketone test strips merely confirmed what you already knew: you had some ketones in your urine (and therefore your blood) most of the time because the diabetes management tools were lacking.
The next generation of urine test strips eliminated the precise drops and test tubes, but they were not necessarily an improvement. After dipping the test strip in your urine, you had to match the color of the strip to a chart on the side of a bottle. Your six choices ranged from light blue to dark brown, corresponding to negative (0), 100, 250, 500, 1,000, and 2,000 mg/dL or more. This still did not give you a clue about the level of your blood glucose.
The blood glucose test strips of the early 1980s would only estimate your blood glucose within maybe 40 mg/dL (2.2 mmol/L), assuming your glucose was under 200 mg/dL (11.1 mmol/L). Over that range, from one color block to the next, the number jumped up by 100 to 200 mg/dL or more. In other words, blood glucose strips still were not remotely precise enough to allow anyone to safely make regimen changes.
Relatively small and affordable blood glucose meters did not become widely available to individuals until the mid-1980s. I got my first one in 1986 after I had already been living with type 1 diabetes for 18 years. My first meter still had significant potential for user error because you had to blot the blood off the strip halfway through the 2-minute testing period. Even with access to reasonably accurate blood glucose measurements for the first time, we all experienced a steep learning curve while figuring out what to do with our food or insulin in response to the readings.
The moral of this story is that we have come a long way with diabetes technology, even if all you use currently is a blood glucose meter that gives you feedback in only 5 seconds. Appreciate having the ability to check what your blood glucose is doing at any given moment and learn to use that vital information to expertly manipulate your medication doses and diet.
With access to a blood glucose meter, you have the primary tool you need to manage your diabetes effectively, especially with exercise as an added variable. Check as frequently as you need to, with the goal of avoiding both lows and highs.
Even if you do not normally get low during exercise, checking frequently is still advisable, especially before you start and after you finish working out. Once you learn your usual responses to activities, you can usually anticipate how to react to keep your blood glucose in an optimal range to perform well.
Continuous Glucose Monitors
In the past decade or so, a number of continuous glucose monitoring (CGM) devices have received approval from the U.S. Food and Drug Administration (FDA), the European Commission, and across the world. To date, all of them are still invasive: they require that you place and keep a probe of some sort under your skin to get readings. While many innovators are working on noninvasive CGM devices, none have been approved or are available yet for use. At least one company (Senseonics) has FDA approval for an implantable CGM device called Eversense, which lasts for 3 months at a time, and they are seeking approval for up to 180 days. (I have heard that their sensors go in easily during an office visit, but they are more difficult to remove after 90 or 180 days. That is not surprising: that time span is more than sufficient for your body to develop an inflammation and grow new tissue around a foreign object embedded in your skin.)
These monitors by themselves only give you information—much like a blood glucose meter does—but you still have to check the readings and make regimen adjustments yourself. However, getting feedback in real-time or at least every 1 to 5 minutes, 24 hours a day, can be extremely useful when you are trying to learn your patterns, see the trends, or keep your blood glucose in a tighter range with less hypoglycemia. The accuracy of these meters has been improving over time, but they are all still limited by their physiological methods: there is a lag of at least 6 to 20 minutes between the glucose they measure (in interstitialspaces between cells in the skin) and your actual blood glucose. This lag can be even greater during times when your blood glucose levels are often changing rapidly, such as after a meal or during exercise.
The CGM devices and models approved and available in the United States as of the publication of this book are shown in table 5.1. “Flash” glucose monitoring (as offered by the FreeStyle Libre device) is a recent innovation, possessing some but not all features of traditional CGM. Flash monitors can provide instantaneous glucose values and recent trends, but they lack the alerts for lows and highs.
Insurance reimbursement also has become more reasonable since CGM devices were first introduced over a decade ago. (I paid $35 out of pocket for each 3-day sensor for the first-generation Dexcom CGM I tried.) Currently, at least one model is covered by Medicare for anyone with type 1 diabetes age 65 and over. Studies have shown that people with type 2 diabetes—especially those using insulin—can also benefit from using CGM, but coverage for them has been an even harder sell to insurance companies so far. In any case, the number of model choices has declined recently, and their cost is still prohibitive for people who lack the insurance coverage.
What's more, CGM technology is not infallible. As I have noted, a major drawback of CGM devices used during exercise is that their glucose readings are not fully real-time because they measure glucose levels in your skin rather than in your blood, and it takes some time for glucose to move between these two parts of your body. Also, CGM users may have problems getting the device to stay put, similar to the issues experienced by pump users with their infusion sites. (Refer back to table 3.2 for solutions on resolving adhesion issues and to the list of strategies used by athletes in chapter 12; most of the tactics used to secure a pump infusion site will also work for CGM devices.) Other reported challenges include variable sensor accuracy, variable performance between sensors, breakage of sensor filaments, transportation of the sensor display, and inability to calibrate CGM during exercise. (If you have the option, you may want to use an integrated watch to display your values.) Although technical failures during exercise are possible even with the newer versions of these monitors, CGM is still the wave of the future when it comes to monitoring and managing blood glucose.
Exercisers have reported a compression effect when wearing the CGM sensor in areas underneath compression shorts, resulting in a greater lag time in readings due to reduced blood flow to areas with compressed skin. This can also happen when you lie directly on the sensors.
If you have access to CGM, you may be able to use either traditional CGM or Flash monitors to enhance your exercise experience in a variety of ways.
- Seeing your glucose values before exercise tells you whether you are likely to need extra carbohydrates, insulin reductions, or an insulin bolus.
- Knowing your glucose trends before you start to work out can also help you make more informed decisions about any necessary changes in your food or medications.
- High and low alerts during and after exercise can help you avoid dangerous glucose extremes, particularly if you set your alerts at preemptive or conservative levels.
- Reviewing your trend graph reports after working out can show you the patterns of your exercise highs and lows, particularly if you use event markers or workout logs.
Many exercisers swear by their CGM devices and do not want to have to live without them (and hopefully they will not ever have to). But if you do not have access to CGM due to lack of insurance coverage, availability in your country, or other reasons, do not despair—you can still learn your glucose patterns by using frequent checks with a blood glucose meter, as most of us have done. In general, most athletes using CGM have found that observing their glucose trends (shown by up, steady, or down arrows) can be helpful during exercise, even when the readings lag behind actual blood glucose or are sometimes inaccurate.
Troubleshooting your performance like an athlete
As you have come to realize in this chapter, being an athlete is mostly a state of mind. However, sometimes your performance when you are an athlete with diabetes also depends on overcoming some regimen obstacles and other physical issues.
As you have come to realize in this chapter, being an athlete is mostly a state of mind. However, sometimes your performance when you are an athlete with diabetes also depends on overcoming some regimen obstacles and other physical issues. In this final section, you will learn all you need to perform like a professional athlete.
As discussed back in chapter 2, many different factors can impact your blood glucose responses, and the more you know about them, the better equipped you are to figure out what works best for you in almost every situation. Regardless of how knowledgeable you are, this process always takes some trial and error. Consider using some of the following strategies if you are experiencing any of these issues with being active.
Managing Exercise-Associated Hypoglycemia
Having to slow down or stop during an activity due to low blood glucose is annoying even to recreational athletes. It can also compromise your ability to complete your event, competition, or just your daily workout. It is worth keeping this from happening if you can. If you have been having any exercise-related lows, consider taking some of these actions or precautions to avoid them, especially if you use insulin.
Lows During and After Exercise—Food Intake
- Treat lows with glucose or other rapidly absorbed carbohydrate first, and follow that up with other balanced foods and drinks if needed to keep from dropping later.
- Choose pre-exercise foods that require the smallest amount of (or no) insulin to cover them to keep your circulating insulin lower during activities.
- Take in extra carbohydrate before, during, and after activities (depending on your exercise intensity and duration, starting blood glucose, normal diet, and other factors).
- Consider using protein and/or fat intake during prolonged activities to help prevent lows, especially past the first hour of activity, because they take longer to digest.
- Consume some protein and/or fat shortly after exercise and possibly also at bedtime to counteract lows later on and overnight.
Lows During and After Exercise—Insulin Adjustments
- Exercise when your insulin levels are lower, such as before meals or first thing in the morning before taking any bolus insulin.
- Before doing longer duration exercise, lower your insulin levels in anticipation by cutting back on your dose(s) of bolus and/or basal insulin.
- Lower the dose of any rapid-acting insulin you take within 2 to 3 hours before doing an activity (or set a lower basal rate on your insulin pump, if you use one).
- If using an insulin pump, consider lowering your basal rate for up to 2 hours before the start of exercise as well as during (and likely after) the activity.
- If you are prone to lows after exercise, reduce your dose of rapid-acting insulin given after any activity, or set a temporary lower basal rate on your pump for 4 to 12 hours.
- If you inject your basal insulin (Lantus, Basaglar, Levemir, or Toujeo), consider splitting the dose (although not necessarily evenly) to give it twice daily to allow for easier dose reductions before and after activity.
- If you use an even longer-acting basal insulin like Tresiba, watch out for possible insulin “stacking” on subsequent days, particularly when you are more active than normal.
Training Effects and Other Considerations
- Check your blood glucose more often when doing a new activity or unaccustomed exercise because both are more likely to result in lows, both during and afterward.
- Check frequently if you have had a bad low or exercised hard in the 24 hours before your latest workout because both may blunt your release of glucose-raising hormones.
- Try doing an all-out sprint for 10 to 30 seconds to help counteract most lows during exercise, but only if your insulin levels are not too high.
- If you plan on doing both aerobic and resistance training during a workout, vary the order based on whether you want your glucose to stay more stable (during resistance work) or possibly decrease (during moderate aerobic work, although intense training may raise it).
- Keep in mind that the rate of insulin absorption from skin depots depends on the size of the dose: smaller doses (1 to 3 units) are absorbed more rapidly than larger ones (5 or more units), which linger longer while you are active.
- Do not forget that your overall insulin needs are lower when you are regularly active; you may need permanently lower basal (and mealtime bolus) insulin doses.
- Avoid massaging the area where you just gave some insulin—massaging it can speed up its absorption.
- Remember that getting in a hot tub or having other prolonged heat exposure can speed up the absorption of any insulin taken (causing lows first, then highs later).
Dealing With Exercise Hyperglycemia
If you have experienced high blood glucose related to being active, it can be hard to always pinpoint the source of the rise and take actions to prevent or manage it. Consider these possible scenarios and some solutions for troubleshooting.
Highs Before Exercise
- If your blood glucose is over 250 mg/dL (13.9 mmol/L) and has been elevated for a few hours, consider giving yourself some insulin and waiting for the level to decrease before starting to exercise (especially with moderate or higher blood and urine ketones).
- If you take a dose of insulin to lower your glucose with a plan to start exercising shortly thereafter, take less than you normally would (50 percent or less) to prevent your blood glucose from dropping too rapidly during the activity.
- If your blood glucose is over 300 mg/dL (16.7 mmol/L) with no ketones, exercise only if you feel well and use caution because you can dehydrate more easily.
Highs During or After Exercise
- Cut back on your carbohydrate intake during exercise, reduce your insulin less, or take extra insulin after exercise (albeit less than normal).
- Remember that eating a full meal within an hour of starting exercise can slow digestion and result in high blood glucose for 1 to 2 hours afterward, particularly when you have consumed lower glycemic index items (refer to chapter 4 for a discussion of the glycemic index).
- If you disconnect your pump during activities and your blood glucose starts to rise, reconnect at least once an hour and take at least a portion of your missed basal.
- Consider giving yourself some of your “missed” basal insulin in advance in some cases, such as when you have disconnected from your pump before a swim.
- Consider using an “untethered” pump regimen—that is, giving some of your insulin as an injection of long-acting insulin (e.g., Lantus, Levemir, Tresiba) and the rest via pump with a reduced basal rate; then if you disconnect, you still have some basal on board.
- For early morning exercise before eating, consider giving yourself a small dose of insulin (less than normal) and/or a small snack to break your fast to reduce cortisol levels that can lead to elevations at that time of day.
- If the stress or intensity of competitions affects you, keep your basal insulin higher and only give yourself 50 percent or less of your usual correction dose to lower glucose.
- Stay hydrated during activities because dehydration can make blood glucose seem higher (due to being more concentrated) and lead to excess correction dosing.
- Consider doing some easy aerobic exercise after more intense workouts to lower blood glucose naturally.
Training Effects and Other Considerations
- After you have trained for a few weeks doing an activity, you may need fewer carbohydrates or smaller insulin reductions than before training due to a greater use of fat.
- Both endurance training and fat adaptation (from a low-carbohydrate diet) increase your body's efficiency at using fat as a fuel during aerobic activities that are submaximal.
- When you get very sore from exercise (peaking 2 or 3 days afterward), you may be more insulin resistant because you cannot restore muscle glycogen until your muscle damage from the activity is repaired.
- If you load up on carbohydrates before events, you should take enough insulin to cover them; otherwise, loading can raise your blood glucose and limit glycogen storage (check out the discussion on carbohydrate loading in chapter 3).
- You should keep your insulin from getting too hot or too cold; otherwise, its action may diminish and cause your usual doses to inadequately cover your insulin needs.
- Injected or pumped bolus insulin is absorbed faster in smaller doses; after a larger dose, you may end up too high first and then too low later on.
- Smaller doses of injected basal insulin are also absorbed more rapidly than larger ones (think 5 units versus 20), and they often do not last as long as expected.
Understand hormonal responses to exercise
The human body only has insulin to lower blood glucose but has five hormones that raise it (with some overlap).
The human body only has insulin to lower blood glucose but has five hormones that raise it (with some overlap). This hormone redundancy tells you that, at least from a survival standpoint, your body is desperate to make sure you do not run out of blood glucose; it is not as concerned about you having too much. Insulin is an important hormone for regulating your body's storage of fuels (carbohydrate, fat, and protein) after you eat. It tells your insulin-sensitive cells (mainly your muscle and fat cells but also your liver) to take up glucose and fat to store them for later as muscle and liver glycogen (the storage form of glucose) as well as stored fat. During exercise, any insulin in your bloodstream can make your muscles take up extra blood glucose. In people who have a pancreas that functions normally, insulin levels typically decrease during exercise, and levels of a hormone called glucagon (released from the alpha cells of the pancreas) rise to stimulate glucose release.
Your blood glucose levels are managed by your liver, which would normally respond to the relative amounts of insulin and glucagon (table 2.1). Insulin and glucagon released from the pancreas go directly to the liver via the portal circulation. After a meal, high insulin and glucose levels tell the liver to store glucose for later use; fasting overnight or doing extended exercise leads to glucagon signaling the liver to release glucose. How people with type 1 diabetes respond hormonally to exercise is a major issue: the insulin and glucagon at the level of the liver are seldom perfectly normal because their insulin is injected or pumped under the skin rather than released directly from the pancreas.
People with type 1 diabetes have an altered hormonal response to exercise when their peripheral insulin is relatively high; lowering the circulating level of insulin helps normalize their hormone response.
All exercise causes the release of hormones that increase the production of glucose by your liver and lower your muscular use, based on how long and hard you exercise. Easy and moderate activities only release a small amount of glucose-raising hormones (unless you do them for a very long duration), but intense exercise such as heavy resistance training, sprinting, or high-intensity intervals causes an immediate rise in your blood glucose and leads to an exaggerated release of hormones. These hormones include adrenaline (formally known as epinephrine) and norepinephrine, which are released by the sympathetic nervous system (allowing your body to respond to physical or mental stressors with an increased heart rate), as well as glucagon, growth hormone, and cortisol (see table 2.1). The effects of these glucose-raising hormones can easily exceed your body's immediate need for glucose, especially because high-intensity exercise may not last long. As a result, your blood glucose often rises during and after short bouts of intense activity.
Intense exercise can cause a large increase in blood glucose because of your body's exaggerated release of glucose-raising hormones such as adrenaline and glucagon.
You may be more insulin resistant immediately after intense exercise and for a few hours due to these hormones. In one study, after near-maximal cycling to exhaustion, one group of people with type 1 diabetes on insulin pumps experienced elevated blood glucose levels for nearly 2 hours. Similarly, in exercisers with type 2 diabetes, blood glucose also rose for 1 hour in response to maximal cycling, as did their insulin levels (because their bodies still produced their own insulin). You may need some supplemental insulin to bring your blood glucose back down (albeit less than normal), or it may drop slowly over time on its own. After these hormones wane, your blood glucose may easily drop later when your body is working hard to restore the muscle glycogen you used during the activity. Be on the lookout for later-onset lows in these cases.
Getting the most from diabetes technologies
Technology and software related to diabetes and health management are advancing faster than most people can keep up with.
Technology and software related to diabetes and health management are advancing faster than most people can keep up with. Every day a new app seems to come out to keep track of something, be it your blood glucose levels, insulin on board, and carbohydrate counting or your calories, daily steps, and fitness goals. In the diabetes world, the latest management technologies guide people in making more informed and effective regimen change decisions—the most important of which are integrated systems that can take charge of the decision making by combining delivery of insulin via pumps, continuous glucose monitoring (CGM), and a control system with potential artificial intelligence(AI) capabilities. Next down the pike is integration of wearable technologies, which can add information related to heart rate and more. More improvements will make AI even more capable of “learning” and updating algorithms to match the changes and patterns in your metabolic state.
Given the challenges of exercising with diabetes, the latest technologies can be beneficial for managing your blood glucose and maximizing the benefits of physical activity. Insulin pumps (covered fully in chapter 3) offer a more fine-tuned ability to regulate basal insulin levels and bolus doses. Blood glucose meters give immediate feedback on where your glucose is starting and how you are responding to an activity. The CGM devices provide an added level of safety by offering the opportunity for improved decision making in real-time and retrospectively. Closed-loop systems that integrate a pump and CGM manage the decision making for you; they can potentially improve your blood glucose management before and during exercise and allow you to avoid any unwanted rises and falls in your blood glucose after workouts. All forms of technology have inherent drawbacks and limitations, but you can overcome most of their issues with planning and knowledge.
Blood Glucose Meters (and Their Precursors)
If you began your journey with diabetes after the advent of home blood glucose meters, consider yourself lucky. Back in 1968 when I began my life with diabetes, no one had blood glucose meters to use for self-monitoring, much less target blood glucose ranges for exercise. All we had were urine tests, which measured the excess glucose and ketones in urine. You would pee in a cup, then put 5 drops of urine with 10 drops of water into a test tube with a tablet. The test tube mixture changed color in a range from cool blue (no glucose) to flaming orange (4+glucose). It did not give you the foggiest idea of what your blood glucose was doing right then; it only told you whether you had been higher than optimal a few hours before. In other words, you could be shaking with the symptoms of a low while watching your urine turn bright orange, the indication of being very high. The ketone test strips merely confirmed what you already knew: you had some ketones in your urine (and therefore your blood) most of the time because the diabetes management tools were lacking.
The next generation of urine test strips eliminated the precise drops and test tubes, but they were not necessarily an improvement. After dipping the test strip in your urine, you had to match the color of the strip to a chart on the side of a bottle. Your six choices ranged from light blue to dark brown, corresponding to negative (0), 100, 250, 500, 1,000, and 2,000 mg/dL or more. This still did not give you a clue about the level of your blood glucose.
The blood glucose test strips of the early 1980s would only estimate your blood glucose within maybe 40 mg/dL (2.2 mmol/L), assuming your glucose was under 200 mg/dL (11.1 mmol/L). Over that range, from one color block to the next, the number jumped up by 100 to 200 mg/dL or more. In other words, blood glucose strips still were not remotely precise enough to allow anyone to safely make regimen changes.
Relatively small and affordable blood glucose meters did not become widely available to individuals until the mid-1980s. I got my first one in 1986 after I had already been living with type 1 diabetes for 18 years. My first meter still had significant potential for user error because you had to blot the blood off the strip halfway through the 2-minute testing period. Even with access to reasonably accurate blood glucose measurements for the first time, we all experienced a steep learning curve while figuring out what to do with our food or insulin in response to the readings.
The moral of this story is that we have come a long way with diabetes technology, even if all you use currently is a blood glucose meter that gives you feedback in only 5 seconds. Appreciate having the ability to check what your blood glucose is doing at any given moment and learn to use that vital information to expertly manipulate your medication doses and diet.
With access to a blood glucose meter, you have the primary tool you need to manage your diabetes effectively, especially with exercise as an added variable. Check as frequently as you need to, with the goal of avoiding both lows and highs.
Even if you do not normally get low during exercise, checking frequently is still advisable, especially before you start and after you finish working out. Once you learn your usual responses to activities, you can usually anticipate how to react to keep your blood glucose in an optimal range to perform well.
Continuous Glucose Monitors
In the past decade or so, a number of continuous glucose monitoring (CGM) devices have received approval from the U.S. Food and Drug Administration (FDA), the European Commission, and across the world. To date, all of them are still invasive: they require that you place and keep a probe of some sort under your skin to get readings. While many innovators are working on noninvasive CGM devices, none have been approved or are available yet for use. At least one company (Senseonics) has FDA approval for an implantable CGM device called Eversense, which lasts for 3 months at a time, and they are seeking approval for up to 180 days. (I have heard that their sensors go in easily during an office visit, but they are more difficult to remove after 90 or 180 days. That is not surprising: that time span is more than sufficient for your body to develop an inflammation and grow new tissue around a foreign object embedded in your skin.)
These monitors by themselves only give you information—much like a blood glucose meter does—but you still have to check the readings and make regimen adjustments yourself. However, getting feedback in real-time or at least every 1 to 5 minutes, 24 hours a day, can be extremely useful when you are trying to learn your patterns, see the trends, or keep your blood glucose in a tighter range with less hypoglycemia. The accuracy of these meters has been improving over time, but they are all still limited by their physiological methods: there is a lag of at least 6 to 20 minutes between the glucose they measure (in interstitialspaces between cells in the skin) and your actual blood glucose. This lag can be even greater during times when your blood glucose levels are often changing rapidly, such as after a meal or during exercise.
The CGM devices and models approved and available in the United States as of the publication of this book are shown in table 5.1. “Flash” glucose monitoring (as offered by the FreeStyle Libre device) is a recent innovation, possessing some but not all features of traditional CGM. Flash monitors can provide instantaneous glucose values and recent trends, but they lack the alerts for lows and highs.
Insurance reimbursement also has become more reasonable since CGM devices were first introduced over a decade ago. (I paid $35 out of pocket for each 3-day sensor for the first-generation Dexcom CGM I tried.) Currently, at least one model is covered by Medicare for anyone with type 1 diabetes age 65 and over. Studies have shown that people with type 2 diabetes—especially those using insulin—can also benefit from using CGM, but coverage for them has been an even harder sell to insurance companies so far. In any case, the number of model choices has declined recently, and their cost is still prohibitive for people who lack the insurance coverage.
What's more, CGM technology is not infallible. As I have noted, a major drawback of CGM devices used during exercise is that their glucose readings are not fully real-time because they measure glucose levels in your skin rather than in your blood, and it takes some time for glucose to move between these two parts of your body. Also, CGM users may have problems getting the device to stay put, similar to the issues experienced by pump users with their infusion sites. (Refer back to table 3.2 for solutions on resolving adhesion issues and to the list of strategies used by athletes in chapter 12; most of the tactics used to secure a pump infusion site will also work for CGM devices.) Other reported challenges include variable sensor accuracy, variable performance between sensors, breakage of sensor filaments, transportation of the sensor display, and inability to calibrate CGM during exercise. (If you have the option, you may want to use an integrated watch to display your values.) Although technical failures during exercise are possible even with the newer versions of these monitors, CGM is still the wave of the future when it comes to monitoring and managing blood glucose.
Exercisers have reported a compression effect when wearing the CGM sensor in areas underneath compression shorts, resulting in a greater lag time in readings due to reduced blood flow to areas with compressed skin. This can also happen when you lie directly on the sensors.
If you have access to CGM, you may be able to use either traditional CGM or Flash monitors to enhance your exercise experience in a variety of ways.
- Seeing your glucose values before exercise tells you whether you are likely to need extra carbohydrates, insulin reductions, or an insulin bolus.
- Knowing your glucose trends before you start to work out can also help you make more informed decisions about any necessary changes in your food or medications.
- High and low alerts during and after exercise can help you avoid dangerous glucose extremes, particularly if you set your alerts at preemptive or conservative levels.
- Reviewing your trend graph reports after working out can show you the patterns of your exercise highs and lows, particularly if you use event markers or workout logs.
Many exercisers swear by their CGM devices and do not want to have to live without them (and hopefully they will not ever have to). But if you do not have access to CGM due to lack of insurance coverage, availability in your country, or other reasons, do not despair—you can still learn your glucose patterns by using frequent checks with a blood glucose meter, as most of us have done. In general, most athletes using CGM have found that observing their glucose trends (shown by up, steady, or down arrows) can be helpful during exercise, even when the readings lag behind actual blood glucose or are sometimes inaccurate.
Troubleshooting your performance like an athlete
As you have come to realize in this chapter, being an athlete is mostly a state of mind. However, sometimes your performance when you are an athlete with diabetes also depends on overcoming some regimen obstacles and other physical issues.
As you have come to realize in this chapter, being an athlete is mostly a state of mind. However, sometimes your performance when you are an athlete with diabetes also depends on overcoming some regimen obstacles and other physical issues. In this final section, you will learn all you need to perform like a professional athlete.
As discussed back in chapter 2, many different factors can impact your blood glucose responses, and the more you know about them, the better equipped you are to figure out what works best for you in almost every situation. Regardless of how knowledgeable you are, this process always takes some trial and error. Consider using some of the following strategies if you are experiencing any of these issues with being active.
Managing Exercise-Associated Hypoglycemia
Having to slow down or stop during an activity due to low blood glucose is annoying even to recreational athletes. It can also compromise your ability to complete your event, competition, or just your daily workout. It is worth keeping this from happening if you can. If you have been having any exercise-related lows, consider taking some of these actions or precautions to avoid them, especially if you use insulin.
Lows During and After Exercise—Food Intake
- Treat lows with glucose or other rapidly absorbed carbohydrate first, and follow that up with other balanced foods and drinks if needed to keep from dropping later.
- Choose pre-exercise foods that require the smallest amount of (or no) insulin to cover them to keep your circulating insulin lower during activities.
- Take in extra carbohydrate before, during, and after activities (depending on your exercise intensity and duration, starting blood glucose, normal diet, and other factors).
- Consider using protein and/or fat intake during prolonged activities to help prevent lows, especially past the first hour of activity, because they take longer to digest.
- Consume some protein and/or fat shortly after exercise and possibly also at bedtime to counteract lows later on and overnight.
Lows During and After Exercise—Insulin Adjustments
- Exercise when your insulin levels are lower, such as before meals or first thing in the morning before taking any bolus insulin.
- Before doing longer duration exercise, lower your insulin levels in anticipation by cutting back on your dose(s) of bolus and/or basal insulin.
- Lower the dose of any rapid-acting insulin you take within 2 to 3 hours before doing an activity (or set a lower basal rate on your insulin pump, if you use one).
- If using an insulin pump, consider lowering your basal rate for up to 2 hours before the start of exercise as well as during (and likely after) the activity.
- If you are prone to lows after exercise, reduce your dose of rapid-acting insulin given after any activity, or set a temporary lower basal rate on your pump for 4 to 12 hours.
- If you inject your basal insulin (Lantus, Basaglar, Levemir, or Toujeo), consider splitting the dose (although not necessarily evenly) to give it twice daily to allow for easier dose reductions before and after activity.
- If you use an even longer-acting basal insulin like Tresiba, watch out for possible insulin “stacking” on subsequent days, particularly when you are more active than normal.
Training Effects and Other Considerations
- Check your blood glucose more often when doing a new activity or unaccustomed exercise because both are more likely to result in lows, both during and afterward.
- Check frequently if you have had a bad low or exercised hard in the 24 hours before your latest workout because both may blunt your release of glucose-raising hormones.
- Try doing an all-out sprint for 10 to 30 seconds to help counteract most lows during exercise, but only if your insulin levels are not too high.
- If you plan on doing both aerobic and resistance training during a workout, vary the order based on whether you want your glucose to stay more stable (during resistance work) or possibly decrease (during moderate aerobic work, although intense training may raise it).
- Keep in mind that the rate of insulin absorption from skin depots depends on the size of the dose: smaller doses (1 to 3 units) are absorbed more rapidly than larger ones (5 or more units), which linger longer while you are active.
- Do not forget that your overall insulin needs are lower when you are regularly active; you may need permanently lower basal (and mealtime bolus) insulin doses.
- Avoid massaging the area where you just gave some insulin—massaging it can speed up its absorption.
- Remember that getting in a hot tub or having other prolonged heat exposure can speed up the absorption of any insulin taken (causing lows first, then highs later).
Dealing With Exercise Hyperglycemia
If you have experienced high blood glucose related to being active, it can be hard to always pinpoint the source of the rise and take actions to prevent or manage it. Consider these possible scenarios and some solutions for troubleshooting.
Highs Before Exercise
- If your blood glucose is over 250 mg/dL (13.9 mmol/L) and has been elevated for a few hours, consider giving yourself some insulin and waiting for the level to decrease before starting to exercise (especially with moderate or higher blood and urine ketones).
- If you take a dose of insulin to lower your glucose with a plan to start exercising shortly thereafter, take less than you normally would (50 percent or less) to prevent your blood glucose from dropping too rapidly during the activity.
- If your blood glucose is over 300 mg/dL (16.7 mmol/L) with no ketones, exercise only if you feel well and use caution because you can dehydrate more easily.
Highs During or After Exercise
- Cut back on your carbohydrate intake during exercise, reduce your insulin less, or take extra insulin after exercise (albeit less than normal).
- Remember that eating a full meal within an hour of starting exercise can slow digestion and result in high blood glucose for 1 to 2 hours afterward, particularly when you have consumed lower glycemic index items (refer to chapter 4 for a discussion of the glycemic index).
- If you disconnect your pump during activities and your blood glucose starts to rise, reconnect at least once an hour and take at least a portion of your missed basal.
- Consider giving yourself some of your “missed” basal insulin in advance in some cases, such as when you have disconnected from your pump before a swim.
- Consider using an “untethered” pump regimen—that is, giving some of your insulin as an injection of long-acting insulin (e.g., Lantus, Levemir, Tresiba) and the rest via pump with a reduced basal rate; then if you disconnect, you still have some basal on board.
- For early morning exercise before eating, consider giving yourself a small dose of insulin (less than normal) and/or a small snack to break your fast to reduce cortisol levels that can lead to elevations at that time of day.
- If the stress or intensity of competitions affects you, keep your basal insulin higher and only give yourself 50 percent or less of your usual correction dose to lower glucose.
- Stay hydrated during activities because dehydration can make blood glucose seem higher (due to being more concentrated) and lead to excess correction dosing.
- Consider doing some easy aerobic exercise after more intense workouts to lower blood glucose naturally.
Training Effects and Other Considerations
- After you have trained for a few weeks doing an activity, you may need fewer carbohydrates or smaller insulin reductions than before training due to a greater use of fat.
- Both endurance training and fat adaptation (from a low-carbohydrate diet) increase your body's efficiency at using fat as a fuel during aerobic activities that are submaximal.
- When you get very sore from exercise (peaking 2 or 3 days afterward), you may be more insulin resistant because you cannot restore muscle glycogen until your muscle damage from the activity is repaired.
- If you load up on carbohydrates before events, you should take enough insulin to cover them; otherwise, loading can raise your blood glucose and limit glycogen storage (check out the discussion on carbohydrate loading in chapter 3).
- You should keep your insulin from getting too hot or too cold; otherwise, its action may diminish and cause your usual doses to inadequately cover your insulin needs.
- Injected or pumped bolus insulin is absorbed faster in smaller doses; after a larger dose, you may end up too high first and then too low later on.
- Smaller doses of injected basal insulin are also absorbed more rapidly than larger ones (think 5 units versus 20), and they often do not last as long as expected.
Understand hormonal responses to exercise
The human body only has insulin to lower blood glucose but has five hormones that raise it (with some overlap).
The human body only has insulin to lower blood glucose but has five hormones that raise it (with some overlap). This hormone redundancy tells you that, at least from a survival standpoint, your body is desperate to make sure you do not run out of blood glucose; it is not as concerned about you having too much. Insulin is an important hormone for regulating your body's storage of fuels (carbohydrate, fat, and protein) after you eat. It tells your insulin-sensitive cells (mainly your muscle and fat cells but also your liver) to take up glucose and fat to store them for later as muscle and liver glycogen (the storage form of glucose) as well as stored fat. During exercise, any insulin in your bloodstream can make your muscles take up extra blood glucose. In people who have a pancreas that functions normally, insulin levels typically decrease during exercise, and levels of a hormone called glucagon (released from the alpha cells of the pancreas) rise to stimulate glucose release.
Your blood glucose levels are managed by your liver, which would normally respond to the relative amounts of insulin and glucagon (table 2.1). Insulin and glucagon released from the pancreas go directly to the liver via the portal circulation. After a meal, high insulin and glucose levels tell the liver to store glucose for later use; fasting overnight or doing extended exercise leads to glucagon signaling the liver to release glucose. How people with type 1 diabetes respond hormonally to exercise is a major issue: the insulin and glucagon at the level of the liver are seldom perfectly normal because their insulin is injected or pumped under the skin rather than released directly from the pancreas.
People with type 1 diabetes have an altered hormonal response to exercise when their peripheral insulin is relatively high; lowering the circulating level of insulin helps normalize their hormone response.
All exercise causes the release of hormones that increase the production of glucose by your liver and lower your muscular use, based on how long and hard you exercise. Easy and moderate activities only release a small amount of glucose-raising hormones (unless you do them for a very long duration), but intense exercise such as heavy resistance training, sprinting, or high-intensity intervals causes an immediate rise in your blood glucose and leads to an exaggerated release of hormones. These hormones include adrenaline (formally known as epinephrine) and norepinephrine, which are released by the sympathetic nervous system (allowing your body to respond to physical or mental stressors with an increased heart rate), as well as glucagon, growth hormone, and cortisol (see table 2.1). The effects of these glucose-raising hormones can easily exceed your body's immediate need for glucose, especially because high-intensity exercise may not last long. As a result, your blood glucose often rises during and after short bouts of intense activity.
Intense exercise can cause a large increase in blood glucose because of your body's exaggerated release of glucose-raising hormones such as adrenaline and glucagon.
You may be more insulin resistant immediately after intense exercise and for a few hours due to these hormones. In one study, after near-maximal cycling to exhaustion, one group of people with type 1 diabetes on insulin pumps experienced elevated blood glucose levels for nearly 2 hours. Similarly, in exercisers with type 2 diabetes, blood glucose also rose for 1 hour in response to maximal cycling, as did their insulin levels (because their bodies still produced their own insulin). You may need some supplemental insulin to bring your blood glucose back down (albeit less than normal), or it may drop slowly over time on its own. After these hormones wane, your blood glucose may easily drop later when your body is working hard to restore the muscle glycogen you used during the activity. Be on the lookout for later-onset lows in these cases.
Getting the most from diabetes technologies
Technology and software related to diabetes and health management are advancing faster than most people can keep up with.
Technology and software related to diabetes and health management are advancing faster than most people can keep up with. Every day a new app seems to come out to keep track of something, be it your blood glucose levels, insulin on board, and carbohydrate counting or your calories, daily steps, and fitness goals. In the diabetes world, the latest management technologies guide people in making more informed and effective regimen change decisions—the most important of which are integrated systems that can take charge of the decision making by combining delivery of insulin via pumps, continuous glucose monitoring (CGM), and a control system with potential artificial intelligence(AI) capabilities. Next down the pike is integration of wearable technologies, which can add information related to heart rate and more. More improvements will make AI even more capable of “learning” and updating algorithms to match the changes and patterns in your metabolic state.
Given the challenges of exercising with diabetes, the latest technologies can be beneficial for managing your blood glucose and maximizing the benefits of physical activity. Insulin pumps (covered fully in chapter 3) offer a more fine-tuned ability to regulate basal insulin levels and bolus doses. Blood glucose meters give immediate feedback on where your glucose is starting and how you are responding to an activity. The CGM devices provide an added level of safety by offering the opportunity for improved decision making in real-time and retrospectively. Closed-loop systems that integrate a pump and CGM manage the decision making for you; they can potentially improve your blood glucose management before and during exercise and allow you to avoid any unwanted rises and falls in your blood glucose after workouts. All forms of technology have inherent drawbacks and limitations, but you can overcome most of their issues with planning and knowledge.
Blood Glucose Meters (and Their Precursors)
If you began your journey with diabetes after the advent of home blood glucose meters, consider yourself lucky. Back in 1968 when I began my life with diabetes, no one had blood glucose meters to use for self-monitoring, much less target blood glucose ranges for exercise. All we had were urine tests, which measured the excess glucose and ketones in urine. You would pee in a cup, then put 5 drops of urine with 10 drops of water into a test tube with a tablet. The test tube mixture changed color in a range from cool blue (no glucose) to flaming orange (4+glucose). It did not give you the foggiest idea of what your blood glucose was doing right then; it only told you whether you had been higher than optimal a few hours before. In other words, you could be shaking with the symptoms of a low while watching your urine turn bright orange, the indication of being very high. The ketone test strips merely confirmed what you already knew: you had some ketones in your urine (and therefore your blood) most of the time because the diabetes management tools were lacking.
The next generation of urine test strips eliminated the precise drops and test tubes, but they were not necessarily an improvement. After dipping the test strip in your urine, you had to match the color of the strip to a chart on the side of a bottle. Your six choices ranged from light blue to dark brown, corresponding to negative (0), 100, 250, 500, 1,000, and 2,000 mg/dL or more. This still did not give you a clue about the level of your blood glucose.
The blood glucose test strips of the early 1980s would only estimate your blood glucose within maybe 40 mg/dL (2.2 mmol/L), assuming your glucose was under 200 mg/dL (11.1 mmol/L). Over that range, from one color block to the next, the number jumped up by 100 to 200 mg/dL or more. In other words, blood glucose strips still were not remotely precise enough to allow anyone to safely make regimen changes.
Relatively small and affordable blood glucose meters did not become widely available to individuals until the mid-1980s. I got my first one in 1986 after I had already been living with type 1 diabetes for 18 years. My first meter still had significant potential for user error because you had to blot the blood off the strip halfway through the 2-minute testing period. Even with access to reasonably accurate blood glucose measurements for the first time, we all experienced a steep learning curve while figuring out what to do with our food or insulin in response to the readings.
The moral of this story is that we have come a long way with diabetes technology, even if all you use currently is a blood glucose meter that gives you feedback in only 5 seconds. Appreciate having the ability to check what your blood glucose is doing at any given moment and learn to use that vital information to expertly manipulate your medication doses and diet.
With access to a blood glucose meter, you have the primary tool you need to manage your diabetes effectively, especially with exercise as an added variable. Check as frequently as you need to, with the goal of avoiding both lows and highs.
Even if you do not normally get low during exercise, checking frequently is still advisable, especially before you start and after you finish working out. Once you learn your usual responses to activities, you can usually anticipate how to react to keep your blood glucose in an optimal range to perform well.
Continuous Glucose Monitors
In the past decade or so, a number of continuous glucose monitoring (CGM) devices have received approval from the U.S. Food and Drug Administration (FDA), the European Commission, and across the world. To date, all of them are still invasive: they require that you place and keep a probe of some sort under your skin to get readings. While many innovators are working on noninvasive CGM devices, none have been approved or are available yet for use. At least one company (Senseonics) has FDA approval for an implantable CGM device called Eversense, which lasts for 3 months at a time, and they are seeking approval for up to 180 days. (I have heard that their sensors go in easily during an office visit, but they are more difficult to remove after 90 or 180 days. That is not surprising: that time span is more than sufficient for your body to develop an inflammation and grow new tissue around a foreign object embedded in your skin.)
These monitors by themselves only give you information—much like a blood glucose meter does—but you still have to check the readings and make regimen adjustments yourself. However, getting feedback in real-time or at least every 1 to 5 minutes, 24 hours a day, can be extremely useful when you are trying to learn your patterns, see the trends, or keep your blood glucose in a tighter range with less hypoglycemia. The accuracy of these meters has been improving over time, but they are all still limited by their physiological methods: there is a lag of at least 6 to 20 minutes between the glucose they measure (in interstitialspaces between cells in the skin) and your actual blood glucose. This lag can be even greater during times when your blood glucose levels are often changing rapidly, such as after a meal or during exercise.
The CGM devices and models approved and available in the United States as of the publication of this book are shown in table 5.1. “Flash” glucose monitoring (as offered by the FreeStyle Libre device) is a recent innovation, possessing some but not all features of traditional CGM. Flash monitors can provide instantaneous glucose values and recent trends, but they lack the alerts for lows and highs.
Insurance reimbursement also has become more reasonable since CGM devices were first introduced over a decade ago. (I paid $35 out of pocket for each 3-day sensor for the first-generation Dexcom CGM I tried.) Currently, at least one model is covered by Medicare for anyone with type 1 diabetes age 65 and over. Studies have shown that people with type 2 diabetes—especially those using insulin—can also benefit from using CGM, but coverage for them has been an even harder sell to insurance companies so far. In any case, the number of model choices has declined recently, and their cost is still prohibitive for people who lack the insurance coverage.
What's more, CGM technology is not infallible. As I have noted, a major drawback of CGM devices used during exercise is that their glucose readings are not fully real-time because they measure glucose levels in your skin rather than in your blood, and it takes some time for glucose to move between these two parts of your body. Also, CGM users may have problems getting the device to stay put, similar to the issues experienced by pump users with their infusion sites. (Refer back to table 3.2 for solutions on resolving adhesion issues and to the list of strategies used by athletes in chapter 12; most of the tactics used to secure a pump infusion site will also work for CGM devices.) Other reported challenges include variable sensor accuracy, variable performance between sensors, breakage of sensor filaments, transportation of the sensor display, and inability to calibrate CGM during exercise. (If you have the option, you may want to use an integrated watch to display your values.) Although technical failures during exercise are possible even with the newer versions of these monitors, CGM is still the wave of the future when it comes to monitoring and managing blood glucose.
Exercisers have reported a compression effect when wearing the CGM sensor in areas underneath compression shorts, resulting in a greater lag time in readings due to reduced blood flow to areas with compressed skin. This can also happen when you lie directly on the sensors.
If you have access to CGM, you may be able to use either traditional CGM or Flash monitors to enhance your exercise experience in a variety of ways.
- Seeing your glucose values before exercise tells you whether you are likely to need extra carbohydrates, insulin reductions, or an insulin bolus.
- Knowing your glucose trends before you start to work out can also help you make more informed decisions about any necessary changes in your food or medications.
- High and low alerts during and after exercise can help you avoid dangerous glucose extremes, particularly if you set your alerts at preemptive or conservative levels.
- Reviewing your trend graph reports after working out can show you the patterns of your exercise highs and lows, particularly if you use event markers or workout logs.
Many exercisers swear by their CGM devices and do not want to have to live without them (and hopefully they will not ever have to). But if you do not have access to CGM due to lack of insurance coverage, availability in your country, or other reasons, do not despair—you can still learn your glucose patterns by using frequent checks with a blood glucose meter, as most of us have done. In general, most athletes using CGM have found that observing their glucose trends (shown by up, steady, or down arrows) can be helpful during exercise, even when the readings lag behind actual blood glucose or are sometimes inaccurate.
Troubleshooting your performance like an athlete
As you have come to realize in this chapter, being an athlete is mostly a state of mind. However, sometimes your performance when you are an athlete with diabetes also depends on overcoming some regimen obstacles and other physical issues.
As you have come to realize in this chapter, being an athlete is mostly a state of mind. However, sometimes your performance when you are an athlete with diabetes also depends on overcoming some regimen obstacles and other physical issues. In this final section, you will learn all you need to perform like a professional athlete.
As discussed back in chapter 2, many different factors can impact your blood glucose responses, and the more you know about them, the better equipped you are to figure out what works best for you in almost every situation. Regardless of how knowledgeable you are, this process always takes some trial and error. Consider using some of the following strategies if you are experiencing any of these issues with being active.
Managing Exercise-Associated Hypoglycemia
Having to slow down or stop during an activity due to low blood glucose is annoying even to recreational athletes. It can also compromise your ability to complete your event, competition, or just your daily workout. It is worth keeping this from happening if you can. If you have been having any exercise-related lows, consider taking some of these actions or precautions to avoid them, especially if you use insulin.
Lows During and After Exercise—Food Intake
- Treat lows with glucose or other rapidly absorbed carbohydrate first, and follow that up with other balanced foods and drinks if needed to keep from dropping later.
- Choose pre-exercise foods that require the smallest amount of (or no) insulin to cover them to keep your circulating insulin lower during activities.
- Take in extra carbohydrate before, during, and after activities (depending on your exercise intensity and duration, starting blood glucose, normal diet, and other factors).
- Consider using protein and/or fat intake during prolonged activities to help prevent lows, especially past the first hour of activity, because they take longer to digest.
- Consume some protein and/or fat shortly after exercise and possibly also at bedtime to counteract lows later on and overnight.
Lows During and After Exercise—Insulin Adjustments
- Exercise when your insulin levels are lower, such as before meals or first thing in the morning before taking any bolus insulin.
- Before doing longer duration exercise, lower your insulin levels in anticipation by cutting back on your dose(s) of bolus and/or basal insulin.
- Lower the dose of any rapid-acting insulin you take within 2 to 3 hours before doing an activity (or set a lower basal rate on your insulin pump, if you use one).
- If using an insulin pump, consider lowering your basal rate for up to 2 hours before the start of exercise as well as during (and likely after) the activity.
- If you are prone to lows after exercise, reduce your dose of rapid-acting insulin given after any activity, or set a temporary lower basal rate on your pump for 4 to 12 hours.
- If you inject your basal insulin (Lantus, Basaglar, Levemir, or Toujeo), consider splitting the dose (although not necessarily evenly) to give it twice daily to allow for easier dose reductions before and after activity.
- If you use an even longer-acting basal insulin like Tresiba, watch out for possible insulin “stacking” on subsequent days, particularly when you are more active than normal.
Training Effects and Other Considerations
- Check your blood glucose more often when doing a new activity or unaccustomed exercise because both are more likely to result in lows, both during and afterward.
- Check frequently if you have had a bad low or exercised hard in the 24 hours before your latest workout because both may blunt your release of glucose-raising hormones.
- Try doing an all-out sprint for 10 to 30 seconds to help counteract most lows during exercise, but only if your insulin levels are not too high.
- If you plan on doing both aerobic and resistance training during a workout, vary the order based on whether you want your glucose to stay more stable (during resistance work) or possibly decrease (during moderate aerobic work, although intense training may raise it).
- Keep in mind that the rate of insulin absorption from skin depots depends on the size of the dose: smaller doses (1 to 3 units) are absorbed more rapidly than larger ones (5 or more units), which linger longer while you are active.
- Do not forget that your overall insulin needs are lower when you are regularly active; you may need permanently lower basal (and mealtime bolus) insulin doses.
- Avoid massaging the area where you just gave some insulin—massaging it can speed up its absorption.
- Remember that getting in a hot tub or having other prolonged heat exposure can speed up the absorption of any insulin taken (causing lows first, then highs later).
Dealing With Exercise Hyperglycemia
If you have experienced high blood glucose related to being active, it can be hard to always pinpoint the source of the rise and take actions to prevent or manage it. Consider these possible scenarios and some solutions for troubleshooting.
Highs Before Exercise
- If your blood glucose is over 250 mg/dL (13.9 mmol/L) and has been elevated for a few hours, consider giving yourself some insulin and waiting for the level to decrease before starting to exercise (especially with moderate or higher blood and urine ketones).
- If you take a dose of insulin to lower your glucose with a plan to start exercising shortly thereafter, take less than you normally would (50 percent or less) to prevent your blood glucose from dropping too rapidly during the activity.
- If your blood glucose is over 300 mg/dL (16.7 mmol/L) with no ketones, exercise only if you feel well and use caution because you can dehydrate more easily.
Highs During or After Exercise
- Cut back on your carbohydrate intake during exercise, reduce your insulin less, or take extra insulin after exercise (albeit less than normal).
- Remember that eating a full meal within an hour of starting exercise can slow digestion and result in high blood glucose for 1 to 2 hours afterward, particularly when you have consumed lower glycemic index items (refer to chapter 4 for a discussion of the glycemic index).
- If you disconnect your pump during activities and your blood glucose starts to rise, reconnect at least once an hour and take at least a portion of your missed basal.
- Consider giving yourself some of your “missed” basal insulin in advance in some cases, such as when you have disconnected from your pump before a swim.
- Consider using an “untethered” pump regimen—that is, giving some of your insulin as an injection of long-acting insulin (e.g., Lantus, Levemir, Tresiba) and the rest via pump with a reduced basal rate; then if you disconnect, you still have some basal on board.
- For early morning exercise before eating, consider giving yourself a small dose of insulin (less than normal) and/or a small snack to break your fast to reduce cortisol levels that can lead to elevations at that time of day.
- If the stress or intensity of competitions affects you, keep your basal insulin higher and only give yourself 50 percent or less of your usual correction dose to lower glucose.
- Stay hydrated during activities because dehydration can make blood glucose seem higher (due to being more concentrated) and lead to excess correction dosing.
- Consider doing some easy aerobic exercise after more intense workouts to lower blood glucose naturally.
Training Effects and Other Considerations
- After you have trained for a few weeks doing an activity, you may need fewer carbohydrates or smaller insulin reductions than before training due to a greater use of fat.
- Both endurance training and fat adaptation (from a low-carbohydrate diet) increase your body's efficiency at using fat as a fuel during aerobic activities that are submaximal.
- When you get very sore from exercise (peaking 2 or 3 days afterward), you may be more insulin resistant because you cannot restore muscle glycogen until your muscle damage from the activity is repaired.
- If you load up on carbohydrates before events, you should take enough insulin to cover them; otherwise, loading can raise your blood glucose and limit glycogen storage (check out the discussion on carbohydrate loading in chapter 3).
- You should keep your insulin from getting too hot or too cold; otherwise, its action may diminish and cause your usual doses to inadequately cover your insulin needs.
- Injected or pumped bolus insulin is absorbed faster in smaller doses; after a larger dose, you may end up too high first and then too low later on.
- Smaller doses of injected basal insulin are also absorbed more rapidly than larger ones (think 5 units versus 20), and they often do not last as long as expected.
Understand hormonal responses to exercise
The human body only has insulin to lower blood glucose but has five hormones that raise it (with some overlap).
The human body only has insulin to lower blood glucose but has five hormones that raise it (with some overlap). This hormone redundancy tells you that, at least from a survival standpoint, your body is desperate to make sure you do not run out of blood glucose; it is not as concerned about you having too much. Insulin is an important hormone for regulating your body's storage of fuels (carbohydrate, fat, and protein) after you eat. It tells your insulin-sensitive cells (mainly your muscle and fat cells but also your liver) to take up glucose and fat to store them for later as muscle and liver glycogen (the storage form of glucose) as well as stored fat. During exercise, any insulin in your bloodstream can make your muscles take up extra blood glucose. In people who have a pancreas that functions normally, insulin levels typically decrease during exercise, and levels of a hormone called glucagon (released from the alpha cells of the pancreas) rise to stimulate glucose release.
Your blood glucose levels are managed by your liver, which would normally respond to the relative amounts of insulin and glucagon (table 2.1). Insulin and glucagon released from the pancreas go directly to the liver via the portal circulation. After a meal, high insulin and glucose levels tell the liver to store glucose for later use; fasting overnight or doing extended exercise leads to glucagon signaling the liver to release glucose. How people with type 1 diabetes respond hormonally to exercise is a major issue: the insulin and glucagon at the level of the liver are seldom perfectly normal because their insulin is injected or pumped under the skin rather than released directly from the pancreas.
People with type 1 diabetes have an altered hormonal response to exercise when their peripheral insulin is relatively high; lowering the circulating level of insulin helps normalize their hormone response.
All exercise causes the release of hormones that increase the production of glucose by your liver and lower your muscular use, based on how long and hard you exercise. Easy and moderate activities only release a small amount of glucose-raising hormones (unless you do them for a very long duration), but intense exercise such as heavy resistance training, sprinting, or high-intensity intervals causes an immediate rise in your blood glucose and leads to an exaggerated release of hormones. These hormones include adrenaline (formally known as epinephrine) and norepinephrine, which are released by the sympathetic nervous system (allowing your body to respond to physical or mental stressors with an increased heart rate), as well as glucagon, growth hormone, and cortisol (see table 2.1). The effects of these glucose-raising hormones can easily exceed your body's immediate need for glucose, especially because high-intensity exercise may not last long. As a result, your blood glucose often rises during and after short bouts of intense activity.
Intense exercise can cause a large increase in blood glucose because of your body's exaggerated release of glucose-raising hormones such as adrenaline and glucagon.
You may be more insulin resistant immediately after intense exercise and for a few hours due to these hormones. In one study, after near-maximal cycling to exhaustion, one group of people with type 1 diabetes on insulin pumps experienced elevated blood glucose levels for nearly 2 hours. Similarly, in exercisers with type 2 diabetes, blood glucose also rose for 1 hour in response to maximal cycling, as did their insulin levels (because their bodies still produced their own insulin). You may need some supplemental insulin to bring your blood glucose back down (albeit less than normal), or it may drop slowly over time on its own. After these hormones wane, your blood glucose may easily drop later when your body is working hard to restore the muscle glycogen you used during the activity. Be on the lookout for later-onset lows in these cases.
Getting the most from diabetes technologies
Technology and software related to diabetes and health management are advancing faster than most people can keep up with.
Technology and software related to diabetes and health management are advancing faster than most people can keep up with. Every day a new app seems to come out to keep track of something, be it your blood glucose levels, insulin on board, and carbohydrate counting or your calories, daily steps, and fitness goals. In the diabetes world, the latest management technologies guide people in making more informed and effective regimen change decisions—the most important of which are integrated systems that can take charge of the decision making by combining delivery of insulin via pumps, continuous glucose monitoring (CGM), and a control system with potential artificial intelligence(AI) capabilities. Next down the pike is integration of wearable technologies, which can add information related to heart rate and more. More improvements will make AI even more capable of “learning” and updating algorithms to match the changes and patterns in your metabolic state.
Given the challenges of exercising with diabetes, the latest technologies can be beneficial for managing your blood glucose and maximizing the benefits of physical activity. Insulin pumps (covered fully in chapter 3) offer a more fine-tuned ability to regulate basal insulin levels and bolus doses. Blood glucose meters give immediate feedback on where your glucose is starting and how you are responding to an activity. The CGM devices provide an added level of safety by offering the opportunity for improved decision making in real-time and retrospectively. Closed-loop systems that integrate a pump and CGM manage the decision making for you; they can potentially improve your blood glucose management before and during exercise and allow you to avoid any unwanted rises and falls in your blood glucose after workouts. All forms of technology have inherent drawbacks and limitations, but you can overcome most of their issues with planning and knowledge.
Blood Glucose Meters (and Their Precursors)
If you began your journey with diabetes after the advent of home blood glucose meters, consider yourself lucky. Back in 1968 when I began my life with diabetes, no one had blood glucose meters to use for self-monitoring, much less target blood glucose ranges for exercise. All we had were urine tests, which measured the excess glucose and ketones in urine. You would pee in a cup, then put 5 drops of urine with 10 drops of water into a test tube with a tablet. The test tube mixture changed color in a range from cool blue (no glucose) to flaming orange (4+glucose). It did not give you the foggiest idea of what your blood glucose was doing right then; it only told you whether you had been higher than optimal a few hours before. In other words, you could be shaking with the symptoms of a low while watching your urine turn bright orange, the indication of being very high. The ketone test strips merely confirmed what you already knew: you had some ketones in your urine (and therefore your blood) most of the time because the diabetes management tools were lacking.
The next generation of urine test strips eliminated the precise drops and test tubes, but they were not necessarily an improvement. After dipping the test strip in your urine, you had to match the color of the strip to a chart on the side of a bottle. Your six choices ranged from light blue to dark brown, corresponding to negative (0), 100, 250, 500, 1,000, and 2,000 mg/dL or more. This still did not give you a clue about the level of your blood glucose.
The blood glucose test strips of the early 1980s would only estimate your blood glucose within maybe 40 mg/dL (2.2 mmol/L), assuming your glucose was under 200 mg/dL (11.1 mmol/L). Over that range, from one color block to the next, the number jumped up by 100 to 200 mg/dL or more. In other words, blood glucose strips still were not remotely precise enough to allow anyone to safely make regimen changes.
Relatively small and affordable blood glucose meters did not become widely available to individuals until the mid-1980s. I got my first one in 1986 after I had already been living with type 1 diabetes for 18 years. My first meter still had significant potential for user error because you had to blot the blood off the strip halfway through the 2-minute testing period. Even with access to reasonably accurate blood glucose measurements for the first time, we all experienced a steep learning curve while figuring out what to do with our food or insulin in response to the readings.
The moral of this story is that we have come a long way with diabetes technology, even if all you use currently is a blood glucose meter that gives you feedback in only 5 seconds. Appreciate having the ability to check what your blood glucose is doing at any given moment and learn to use that vital information to expertly manipulate your medication doses and diet.
With access to a blood glucose meter, you have the primary tool you need to manage your diabetes effectively, especially with exercise as an added variable. Check as frequently as you need to, with the goal of avoiding both lows and highs.
Even if you do not normally get low during exercise, checking frequently is still advisable, especially before you start and after you finish working out. Once you learn your usual responses to activities, you can usually anticipate how to react to keep your blood glucose in an optimal range to perform well.
Continuous Glucose Monitors
In the past decade or so, a number of continuous glucose monitoring (CGM) devices have received approval from the U.S. Food and Drug Administration (FDA), the European Commission, and across the world. To date, all of them are still invasive: they require that you place and keep a probe of some sort under your skin to get readings. While many innovators are working on noninvasive CGM devices, none have been approved or are available yet for use. At least one company (Senseonics) has FDA approval for an implantable CGM device called Eversense, which lasts for 3 months at a time, and they are seeking approval for up to 180 days. (I have heard that their sensors go in easily during an office visit, but they are more difficult to remove after 90 or 180 days. That is not surprising: that time span is more than sufficient for your body to develop an inflammation and grow new tissue around a foreign object embedded in your skin.)
These monitors by themselves only give you information—much like a blood glucose meter does—but you still have to check the readings and make regimen adjustments yourself. However, getting feedback in real-time or at least every 1 to 5 minutes, 24 hours a day, can be extremely useful when you are trying to learn your patterns, see the trends, or keep your blood glucose in a tighter range with less hypoglycemia. The accuracy of these meters has been improving over time, but they are all still limited by their physiological methods: there is a lag of at least 6 to 20 minutes between the glucose they measure (in interstitialspaces between cells in the skin) and your actual blood glucose. This lag can be even greater during times when your blood glucose levels are often changing rapidly, such as after a meal or during exercise.
The CGM devices and models approved and available in the United States as of the publication of this book are shown in table 5.1. “Flash” glucose monitoring (as offered by the FreeStyle Libre device) is a recent innovation, possessing some but not all features of traditional CGM. Flash monitors can provide instantaneous glucose values and recent trends, but they lack the alerts for lows and highs.
Insurance reimbursement also has become more reasonable since CGM devices were first introduced over a decade ago. (I paid $35 out of pocket for each 3-day sensor for the first-generation Dexcom CGM I tried.) Currently, at least one model is covered by Medicare for anyone with type 1 diabetes age 65 and over. Studies have shown that people with type 2 diabetes—especially those using insulin—can also benefit from using CGM, but coverage for them has been an even harder sell to insurance companies so far. In any case, the number of model choices has declined recently, and their cost is still prohibitive for people who lack the insurance coverage.
What's more, CGM technology is not infallible. As I have noted, a major drawback of CGM devices used during exercise is that their glucose readings are not fully real-time because they measure glucose levels in your skin rather than in your blood, and it takes some time for glucose to move between these two parts of your body. Also, CGM users may have problems getting the device to stay put, similar to the issues experienced by pump users with their infusion sites. (Refer back to table 3.2 for solutions on resolving adhesion issues and to the list of strategies used by athletes in chapter 12; most of the tactics used to secure a pump infusion site will also work for CGM devices.) Other reported challenges include variable sensor accuracy, variable performance between sensors, breakage of sensor filaments, transportation of the sensor display, and inability to calibrate CGM during exercise. (If you have the option, you may want to use an integrated watch to display your values.) Although technical failures during exercise are possible even with the newer versions of these monitors, CGM is still the wave of the future when it comes to monitoring and managing blood glucose.
Exercisers have reported a compression effect when wearing the CGM sensor in areas underneath compression shorts, resulting in a greater lag time in readings due to reduced blood flow to areas with compressed skin. This can also happen when you lie directly on the sensors.
If you have access to CGM, you may be able to use either traditional CGM or Flash monitors to enhance your exercise experience in a variety of ways.
- Seeing your glucose values before exercise tells you whether you are likely to need extra carbohydrates, insulin reductions, or an insulin bolus.
- Knowing your glucose trends before you start to work out can also help you make more informed decisions about any necessary changes in your food or medications.
- High and low alerts during and after exercise can help you avoid dangerous glucose extremes, particularly if you set your alerts at preemptive or conservative levels.
- Reviewing your trend graph reports after working out can show you the patterns of your exercise highs and lows, particularly if you use event markers or workout logs.
Many exercisers swear by their CGM devices and do not want to have to live without them (and hopefully they will not ever have to). But if you do not have access to CGM due to lack of insurance coverage, availability in your country, or other reasons, do not despair—you can still learn your glucose patterns by using frequent checks with a blood glucose meter, as most of us have done. In general, most athletes using CGM have found that observing their glucose trends (shown by up, steady, or down arrows) can be helpful during exercise, even when the readings lag behind actual blood glucose or are sometimes inaccurate.
Troubleshooting your performance like an athlete
As you have come to realize in this chapter, being an athlete is mostly a state of mind. However, sometimes your performance when you are an athlete with diabetes also depends on overcoming some regimen obstacles and other physical issues.
As you have come to realize in this chapter, being an athlete is mostly a state of mind. However, sometimes your performance when you are an athlete with diabetes also depends on overcoming some regimen obstacles and other physical issues. In this final section, you will learn all you need to perform like a professional athlete.
As discussed back in chapter 2, many different factors can impact your blood glucose responses, and the more you know about them, the better equipped you are to figure out what works best for you in almost every situation. Regardless of how knowledgeable you are, this process always takes some trial and error. Consider using some of the following strategies if you are experiencing any of these issues with being active.
Managing Exercise-Associated Hypoglycemia
Having to slow down or stop during an activity due to low blood glucose is annoying even to recreational athletes. It can also compromise your ability to complete your event, competition, or just your daily workout. It is worth keeping this from happening if you can. If you have been having any exercise-related lows, consider taking some of these actions or precautions to avoid them, especially if you use insulin.
Lows During and After Exercise—Food Intake
- Treat lows with glucose or other rapidly absorbed carbohydrate first, and follow that up with other balanced foods and drinks if needed to keep from dropping later.
- Choose pre-exercise foods that require the smallest amount of (or no) insulin to cover them to keep your circulating insulin lower during activities.
- Take in extra carbohydrate before, during, and after activities (depending on your exercise intensity and duration, starting blood glucose, normal diet, and other factors).
- Consider using protein and/or fat intake during prolonged activities to help prevent lows, especially past the first hour of activity, because they take longer to digest.
- Consume some protein and/or fat shortly after exercise and possibly also at bedtime to counteract lows later on and overnight.
Lows During and After Exercise—Insulin Adjustments
- Exercise when your insulin levels are lower, such as before meals or first thing in the morning before taking any bolus insulin.
- Before doing longer duration exercise, lower your insulin levels in anticipation by cutting back on your dose(s) of bolus and/or basal insulin.
- Lower the dose of any rapid-acting insulin you take within 2 to 3 hours before doing an activity (or set a lower basal rate on your insulin pump, if you use one).
- If using an insulin pump, consider lowering your basal rate for up to 2 hours before the start of exercise as well as during (and likely after) the activity.
- If you are prone to lows after exercise, reduce your dose of rapid-acting insulin given after any activity, or set a temporary lower basal rate on your pump for 4 to 12 hours.
- If you inject your basal insulin (Lantus, Basaglar, Levemir, or Toujeo), consider splitting the dose (although not necessarily evenly) to give it twice daily to allow for easier dose reductions before and after activity.
- If you use an even longer-acting basal insulin like Tresiba, watch out for possible insulin “stacking” on subsequent days, particularly when you are more active than normal.
Training Effects and Other Considerations
- Check your blood glucose more often when doing a new activity or unaccustomed exercise because both are more likely to result in lows, both during and afterward.
- Check frequently if you have had a bad low or exercised hard in the 24 hours before your latest workout because both may blunt your release of glucose-raising hormones.
- Try doing an all-out sprint for 10 to 30 seconds to help counteract most lows during exercise, but only if your insulin levels are not too high.
- If you plan on doing both aerobic and resistance training during a workout, vary the order based on whether you want your glucose to stay more stable (during resistance work) or possibly decrease (during moderate aerobic work, although intense training may raise it).
- Keep in mind that the rate of insulin absorption from skin depots depends on the size of the dose: smaller doses (1 to 3 units) are absorbed more rapidly than larger ones (5 or more units), which linger longer while you are active.
- Do not forget that your overall insulin needs are lower when you are regularly active; you may need permanently lower basal (and mealtime bolus) insulin doses.
- Avoid massaging the area where you just gave some insulin—massaging it can speed up its absorption.
- Remember that getting in a hot tub or having other prolonged heat exposure can speed up the absorption of any insulin taken (causing lows first, then highs later).
Dealing With Exercise Hyperglycemia
If you have experienced high blood glucose related to being active, it can be hard to always pinpoint the source of the rise and take actions to prevent or manage it. Consider these possible scenarios and some solutions for troubleshooting.
Highs Before Exercise
- If your blood glucose is over 250 mg/dL (13.9 mmol/L) and has been elevated for a few hours, consider giving yourself some insulin and waiting for the level to decrease before starting to exercise (especially with moderate or higher blood and urine ketones).
- If you take a dose of insulin to lower your glucose with a plan to start exercising shortly thereafter, take less than you normally would (50 percent or less) to prevent your blood glucose from dropping too rapidly during the activity.
- If your blood glucose is over 300 mg/dL (16.7 mmol/L) with no ketones, exercise only if you feel well and use caution because you can dehydrate more easily.
Highs During or After Exercise
- Cut back on your carbohydrate intake during exercise, reduce your insulin less, or take extra insulin after exercise (albeit less than normal).
- Remember that eating a full meal within an hour of starting exercise can slow digestion and result in high blood glucose for 1 to 2 hours afterward, particularly when you have consumed lower glycemic index items (refer to chapter 4 for a discussion of the glycemic index).
- If you disconnect your pump during activities and your blood glucose starts to rise, reconnect at least once an hour and take at least a portion of your missed basal.
- Consider giving yourself some of your “missed” basal insulin in advance in some cases, such as when you have disconnected from your pump before a swim.
- Consider using an “untethered” pump regimen—that is, giving some of your insulin as an injection of long-acting insulin (e.g., Lantus, Levemir, Tresiba) and the rest via pump with a reduced basal rate; then if you disconnect, you still have some basal on board.
- For early morning exercise before eating, consider giving yourself a small dose of insulin (less than normal) and/or a small snack to break your fast to reduce cortisol levels that can lead to elevations at that time of day.
- If the stress or intensity of competitions affects you, keep your basal insulin higher and only give yourself 50 percent or less of your usual correction dose to lower glucose.
- Stay hydrated during activities because dehydration can make blood glucose seem higher (due to being more concentrated) and lead to excess correction dosing.
- Consider doing some easy aerobic exercise after more intense workouts to lower blood glucose naturally.
Training Effects and Other Considerations
- After you have trained for a few weeks doing an activity, you may need fewer carbohydrates or smaller insulin reductions than before training due to a greater use of fat.
- Both endurance training and fat adaptation (from a low-carbohydrate diet) increase your body's efficiency at using fat as a fuel during aerobic activities that are submaximal.
- When you get very sore from exercise (peaking 2 or 3 days afterward), you may be more insulin resistant because you cannot restore muscle glycogen until your muscle damage from the activity is repaired.
- If you load up on carbohydrates before events, you should take enough insulin to cover them; otherwise, loading can raise your blood glucose and limit glycogen storage (check out the discussion on carbohydrate loading in chapter 3).
- You should keep your insulin from getting too hot or too cold; otherwise, its action may diminish and cause your usual doses to inadequately cover your insulin needs.
- Injected or pumped bolus insulin is absorbed faster in smaller doses; after a larger dose, you may end up too high first and then too low later on.
- Smaller doses of injected basal insulin are also absorbed more rapidly than larger ones (think 5 units versus 20), and they often do not last as long as expected.
Understand hormonal responses to exercise
The human body only has insulin to lower blood glucose but has five hormones that raise it (with some overlap).
The human body only has insulin to lower blood glucose but has five hormones that raise it (with some overlap). This hormone redundancy tells you that, at least from a survival standpoint, your body is desperate to make sure you do not run out of blood glucose; it is not as concerned about you having too much. Insulin is an important hormone for regulating your body's storage of fuels (carbohydrate, fat, and protein) after you eat. It tells your insulin-sensitive cells (mainly your muscle and fat cells but also your liver) to take up glucose and fat to store them for later as muscle and liver glycogen (the storage form of glucose) as well as stored fat. During exercise, any insulin in your bloodstream can make your muscles take up extra blood glucose. In people who have a pancreas that functions normally, insulin levels typically decrease during exercise, and levels of a hormone called glucagon (released from the alpha cells of the pancreas) rise to stimulate glucose release.
Your blood glucose levels are managed by your liver, which would normally respond to the relative amounts of insulin and glucagon (table 2.1). Insulin and glucagon released from the pancreas go directly to the liver via the portal circulation. After a meal, high insulin and glucose levels tell the liver to store glucose for later use; fasting overnight or doing extended exercise leads to glucagon signaling the liver to release glucose. How people with type 1 diabetes respond hormonally to exercise is a major issue: the insulin and glucagon at the level of the liver are seldom perfectly normal because their insulin is injected or pumped under the skin rather than released directly from the pancreas.
People with type 1 diabetes have an altered hormonal response to exercise when their peripheral insulin is relatively high; lowering the circulating level of insulin helps normalize their hormone response.
All exercise causes the release of hormones that increase the production of glucose by your liver and lower your muscular use, based on how long and hard you exercise. Easy and moderate activities only release a small amount of glucose-raising hormones (unless you do them for a very long duration), but intense exercise such as heavy resistance training, sprinting, or high-intensity intervals causes an immediate rise in your blood glucose and leads to an exaggerated release of hormones. These hormones include adrenaline (formally known as epinephrine) and norepinephrine, which are released by the sympathetic nervous system (allowing your body to respond to physical or mental stressors with an increased heart rate), as well as glucagon, growth hormone, and cortisol (see table 2.1). The effects of these glucose-raising hormones can easily exceed your body's immediate need for glucose, especially because high-intensity exercise may not last long. As a result, your blood glucose often rises during and after short bouts of intense activity.
Intense exercise can cause a large increase in blood glucose because of your body's exaggerated release of glucose-raising hormones such as adrenaline and glucagon.
You may be more insulin resistant immediately after intense exercise and for a few hours due to these hormones. In one study, after near-maximal cycling to exhaustion, one group of people with type 1 diabetes on insulin pumps experienced elevated blood glucose levels for nearly 2 hours. Similarly, in exercisers with type 2 diabetes, blood glucose also rose for 1 hour in response to maximal cycling, as did their insulin levels (because their bodies still produced their own insulin). You may need some supplemental insulin to bring your blood glucose back down (albeit less than normal), or it may drop slowly over time on its own. After these hormones wane, your blood glucose may easily drop later when your body is working hard to restore the muscle glycogen you used during the activity. Be on the lookout for later-onset lows in these cases.
Getting the most from diabetes technologies
Technology and software related to diabetes and health management are advancing faster than most people can keep up with.
Technology and software related to diabetes and health management are advancing faster than most people can keep up with. Every day a new app seems to come out to keep track of something, be it your blood glucose levels, insulin on board, and carbohydrate counting or your calories, daily steps, and fitness goals. In the diabetes world, the latest management technologies guide people in making more informed and effective regimen change decisions—the most important of which are integrated systems that can take charge of the decision making by combining delivery of insulin via pumps, continuous glucose monitoring (CGM), and a control system with potential artificial intelligence(AI) capabilities. Next down the pike is integration of wearable technologies, which can add information related to heart rate and more. More improvements will make AI even more capable of “learning” and updating algorithms to match the changes and patterns in your metabolic state.
Given the challenges of exercising with diabetes, the latest technologies can be beneficial for managing your blood glucose and maximizing the benefits of physical activity. Insulin pumps (covered fully in chapter 3) offer a more fine-tuned ability to regulate basal insulin levels and bolus doses. Blood glucose meters give immediate feedback on where your glucose is starting and how you are responding to an activity. The CGM devices provide an added level of safety by offering the opportunity for improved decision making in real-time and retrospectively. Closed-loop systems that integrate a pump and CGM manage the decision making for you; they can potentially improve your blood glucose management before and during exercise and allow you to avoid any unwanted rises and falls in your blood glucose after workouts. All forms of technology have inherent drawbacks and limitations, but you can overcome most of their issues with planning and knowledge.
Blood Glucose Meters (and Their Precursors)
If you began your journey with diabetes after the advent of home blood glucose meters, consider yourself lucky. Back in 1968 when I began my life with diabetes, no one had blood glucose meters to use for self-monitoring, much less target blood glucose ranges for exercise. All we had were urine tests, which measured the excess glucose and ketones in urine. You would pee in a cup, then put 5 drops of urine with 10 drops of water into a test tube with a tablet. The test tube mixture changed color in a range from cool blue (no glucose) to flaming orange (4+glucose). It did not give you the foggiest idea of what your blood glucose was doing right then; it only told you whether you had been higher than optimal a few hours before. In other words, you could be shaking with the symptoms of a low while watching your urine turn bright orange, the indication of being very high. The ketone test strips merely confirmed what you already knew: you had some ketones in your urine (and therefore your blood) most of the time because the diabetes management tools were lacking.
The next generation of urine test strips eliminated the precise drops and test tubes, but they were not necessarily an improvement. After dipping the test strip in your urine, you had to match the color of the strip to a chart on the side of a bottle. Your six choices ranged from light blue to dark brown, corresponding to negative (0), 100, 250, 500, 1,000, and 2,000 mg/dL or more. This still did not give you a clue about the level of your blood glucose.
The blood glucose test strips of the early 1980s would only estimate your blood glucose within maybe 40 mg/dL (2.2 mmol/L), assuming your glucose was under 200 mg/dL (11.1 mmol/L). Over that range, from one color block to the next, the number jumped up by 100 to 200 mg/dL or more. In other words, blood glucose strips still were not remotely precise enough to allow anyone to safely make regimen changes.
Relatively small and affordable blood glucose meters did not become widely available to individuals until the mid-1980s. I got my first one in 1986 after I had already been living with type 1 diabetes for 18 years. My first meter still had significant potential for user error because you had to blot the blood off the strip halfway through the 2-minute testing period. Even with access to reasonably accurate blood glucose measurements for the first time, we all experienced a steep learning curve while figuring out what to do with our food or insulin in response to the readings.
The moral of this story is that we have come a long way with diabetes technology, even if all you use currently is a blood glucose meter that gives you feedback in only 5 seconds. Appreciate having the ability to check what your blood glucose is doing at any given moment and learn to use that vital information to expertly manipulate your medication doses and diet.
With access to a blood glucose meter, you have the primary tool you need to manage your diabetes effectively, especially with exercise as an added variable. Check as frequently as you need to, with the goal of avoiding both lows and highs.
Even if you do not normally get low during exercise, checking frequently is still advisable, especially before you start and after you finish working out. Once you learn your usual responses to activities, you can usually anticipate how to react to keep your blood glucose in an optimal range to perform well.
Continuous Glucose Monitors
In the past decade or so, a number of continuous glucose monitoring (CGM) devices have received approval from the U.S. Food and Drug Administration (FDA), the European Commission, and across the world. To date, all of them are still invasive: they require that you place and keep a probe of some sort under your skin to get readings. While many innovators are working on noninvasive CGM devices, none have been approved or are available yet for use. At least one company (Senseonics) has FDA approval for an implantable CGM device called Eversense, which lasts for 3 months at a time, and they are seeking approval for up to 180 days. (I have heard that their sensors go in easily during an office visit, but they are more difficult to remove after 90 or 180 days. That is not surprising: that time span is more than sufficient for your body to develop an inflammation and grow new tissue around a foreign object embedded in your skin.)
These monitors by themselves only give you information—much like a blood glucose meter does—but you still have to check the readings and make regimen adjustments yourself. However, getting feedback in real-time or at least every 1 to 5 minutes, 24 hours a day, can be extremely useful when you are trying to learn your patterns, see the trends, or keep your blood glucose in a tighter range with less hypoglycemia. The accuracy of these meters has been improving over time, but they are all still limited by their physiological methods: there is a lag of at least 6 to 20 minutes between the glucose they measure (in interstitialspaces between cells in the skin) and your actual blood glucose. This lag can be even greater during times when your blood glucose levels are often changing rapidly, such as after a meal or during exercise.
The CGM devices and models approved and available in the United States as of the publication of this book are shown in table 5.1. “Flash” glucose monitoring (as offered by the FreeStyle Libre device) is a recent innovation, possessing some but not all features of traditional CGM. Flash monitors can provide instantaneous glucose values and recent trends, but they lack the alerts for lows and highs.
Insurance reimbursement also has become more reasonable since CGM devices were first introduced over a decade ago. (I paid $35 out of pocket for each 3-day sensor for the first-generation Dexcom CGM I tried.) Currently, at least one model is covered by Medicare for anyone with type 1 diabetes age 65 and over. Studies have shown that people with type 2 diabetes—especially those using insulin—can also benefit from using CGM, but coverage for them has been an even harder sell to insurance companies so far. In any case, the number of model choices has declined recently, and their cost is still prohibitive for people who lack the insurance coverage.
What's more, CGM technology is not infallible. As I have noted, a major drawback of CGM devices used during exercise is that their glucose readings are not fully real-time because they measure glucose levels in your skin rather than in your blood, and it takes some time for glucose to move between these two parts of your body. Also, CGM users may have problems getting the device to stay put, similar to the issues experienced by pump users with their infusion sites. (Refer back to table 3.2 for solutions on resolving adhesion issues and to the list of strategies used by athletes in chapter 12; most of the tactics used to secure a pump infusion site will also work for CGM devices.) Other reported challenges include variable sensor accuracy, variable performance between sensors, breakage of sensor filaments, transportation of the sensor display, and inability to calibrate CGM during exercise. (If you have the option, you may want to use an integrated watch to display your values.) Although technical failures during exercise are possible even with the newer versions of these monitors, CGM is still the wave of the future when it comes to monitoring and managing blood glucose.
Exercisers have reported a compression effect when wearing the CGM sensor in areas underneath compression shorts, resulting in a greater lag time in readings due to reduced blood flow to areas with compressed skin. This can also happen when you lie directly on the sensors.
If you have access to CGM, you may be able to use either traditional CGM or Flash monitors to enhance your exercise experience in a variety of ways.
- Seeing your glucose values before exercise tells you whether you are likely to need extra carbohydrates, insulin reductions, or an insulin bolus.
- Knowing your glucose trends before you start to work out can also help you make more informed decisions about any necessary changes in your food or medications.
- High and low alerts during and after exercise can help you avoid dangerous glucose extremes, particularly if you set your alerts at preemptive or conservative levels.
- Reviewing your trend graph reports after working out can show you the patterns of your exercise highs and lows, particularly if you use event markers or workout logs.
Many exercisers swear by their CGM devices and do not want to have to live without them (and hopefully they will not ever have to). But if you do not have access to CGM due to lack of insurance coverage, availability in your country, or other reasons, do not despair—you can still learn your glucose patterns by using frequent checks with a blood glucose meter, as most of us have done. In general, most athletes using CGM have found that observing their glucose trends (shown by up, steady, or down arrows) can be helpful during exercise, even when the readings lag behind actual blood glucose or are sometimes inaccurate.
Troubleshooting your performance like an athlete
As you have come to realize in this chapter, being an athlete is mostly a state of mind. However, sometimes your performance when you are an athlete with diabetes also depends on overcoming some regimen obstacles and other physical issues.
As you have come to realize in this chapter, being an athlete is mostly a state of mind. However, sometimes your performance when you are an athlete with diabetes also depends on overcoming some regimen obstacles and other physical issues. In this final section, you will learn all you need to perform like a professional athlete.
As discussed back in chapter 2, many different factors can impact your blood glucose responses, and the more you know about them, the better equipped you are to figure out what works best for you in almost every situation. Regardless of how knowledgeable you are, this process always takes some trial and error. Consider using some of the following strategies if you are experiencing any of these issues with being active.
Managing Exercise-Associated Hypoglycemia
Having to slow down or stop during an activity due to low blood glucose is annoying even to recreational athletes. It can also compromise your ability to complete your event, competition, or just your daily workout. It is worth keeping this from happening if you can. If you have been having any exercise-related lows, consider taking some of these actions or precautions to avoid them, especially if you use insulin.
Lows During and After Exercise—Food Intake
- Treat lows with glucose or other rapidly absorbed carbohydrate first, and follow that up with other balanced foods and drinks if needed to keep from dropping later.
- Choose pre-exercise foods that require the smallest amount of (or no) insulin to cover them to keep your circulating insulin lower during activities.
- Take in extra carbohydrate before, during, and after activities (depending on your exercise intensity and duration, starting blood glucose, normal diet, and other factors).
- Consider using protein and/or fat intake during prolonged activities to help prevent lows, especially past the first hour of activity, because they take longer to digest.
- Consume some protein and/or fat shortly after exercise and possibly also at bedtime to counteract lows later on and overnight.
Lows During and After Exercise—Insulin Adjustments
- Exercise when your insulin levels are lower, such as before meals or first thing in the morning before taking any bolus insulin.
- Before doing longer duration exercise, lower your insulin levels in anticipation by cutting back on your dose(s) of bolus and/or basal insulin.
- Lower the dose of any rapid-acting insulin you take within 2 to 3 hours before doing an activity (or set a lower basal rate on your insulin pump, if you use one).
- If using an insulin pump, consider lowering your basal rate for up to 2 hours before the start of exercise as well as during (and likely after) the activity.
- If you are prone to lows after exercise, reduce your dose of rapid-acting insulin given after any activity, or set a temporary lower basal rate on your pump for 4 to 12 hours.
- If you inject your basal insulin (Lantus, Basaglar, Levemir, or Toujeo), consider splitting the dose (although not necessarily evenly) to give it twice daily to allow for easier dose reductions before and after activity.
- If you use an even longer-acting basal insulin like Tresiba, watch out for possible insulin “stacking” on subsequent days, particularly when you are more active than normal.
Training Effects and Other Considerations
- Check your blood glucose more often when doing a new activity or unaccustomed exercise because both are more likely to result in lows, both during and afterward.
- Check frequently if you have had a bad low or exercised hard in the 24 hours before your latest workout because both may blunt your release of glucose-raising hormones.
- Try doing an all-out sprint for 10 to 30 seconds to help counteract most lows during exercise, but only if your insulin levels are not too high.
- If you plan on doing both aerobic and resistance training during a workout, vary the order based on whether you want your glucose to stay more stable (during resistance work) or possibly decrease (during moderate aerobic work, although intense training may raise it).
- Keep in mind that the rate of insulin absorption from skin depots depends on the size of the dose: smaller doses (1 to 3 units) are absorbed more rapidly than larger ones (5 or more units), which linger longer while you are active.
- Do not forget that your overall insulin needs are lower when you are regularly active; you may need permanently lower basal (and mealtime bolus) insulin doses.
- Avoid massaging the area where you just gave some insulin—massaging it can speed up its absorption.
- Remember that getting in a hot tub or having other prolonged heat exposure can speed up the absorption of any insulin taken (causing lows first, then highs later).
Dealing With Exercise Hyperglycemia
If you have experienced high blood glucose related to being active, it can be hard to always pinpoint the source of the rise and take actions to prevent or manage it. Consider these possible scenarios and some solutions for troubleshooting.
Highs Before Exercise
- If your blood glucose is over 250 mg/dL (13.9 mmol/L) and has been elevated for a few hours, consider giving yourself some insulin and waiting for the level to decrease before starting to exercise (especially with moderate or higher blood and urine ketones).
- If you take a dose of insulin to lower your glucose with a plan to start exercising shortly thereafter, take less than you normally would (50 percent or less) to prevent your blood glucose from dropping too rapidly during the activity.
- If your blood glucose is over 300 mg/dL (16.7 mmol/L) with no ketones, exercise only if you feel well and use caution because you can dehydrate more easily.
Highs During or After Exercise
- Cut back on your carbohydrate intake during exercise, reduce your insulin less, or take extra insulin after exercise (albeit less than normal).
- Remember that eating a full meal within an hour of starting exercise can slow digestion and result in high blood glucose for 1 to 2 hours afterward, particularly when you have consumed lower glycemic index items (refer to chapter 4 for a discussion of the glycemic index).
- If you disconnect your pump during activities and your blood glucose starts to rise, reconnect at least once an hour and take at least a portion of your missed basal.
- Consider giving yourself some of your “missed” basal insulin in advance in some cases, such as when you have disconnected from your pump before a swim.
- Consider using an “untethered” pump regimen—that is, giving some of your insulin as an injection of long-acting insulin (e.g., Lantus, Levemir, Tresiba) and the rest via pump with a reduced basal rate; then if you disconnect, you still have some basal on board.
- For early morning exercise before eating, consider giving yourself a small dose of insulin (less than normal) and/or a small snack to break your fast to reduce cortisol levels that can lead to elevations at that time of day.
- If the stress or intensity of competitions affects you, keep your basal insulin higher and only give yourself 50 percent or less of your usual correction dose to lower glucose.
- Stay hydrated during activities because dehydration can make blood glucose seem higher (due to being more concentrated) and lead to excess correction dosing.
- Consider doing some easy aerobic exercise after more intense workouts to lower blood glucose naturally.
Training Effects and Other Considerations
- After you have trained for a few weeks doing an activity, you may need fewer carbohydrates or smaller insulin reductions than before training due to a greater use of fat.
- Both endurance training and fat adaptation (from a low-carbohydrate diet) increase your body's efficiency at using fat as a fuel during aerobic activities that are submaximal.
- When you get very sore from exercise (peaking 2 or 3 days afterward), you may be more insulin resistant because you cannot restore muscle glycogen until your muscle damage from the activity is repaired.
- If you load up on carbohydrates before events, you should take enough insulin to cover them; otherwise, loading can raise your blood glucose and limit glycogen storage (check out the discussion on carbohydrate loading in chapter 3).
- You should keep your insulin from getting too hot or too cold; otherwise, its action may diminish and cause your usual doses to inadequately cover your insulin needs.
- Injected or pumped bolus insulin is absorbed faster in smaller doses; after a larger dose, you may end up too high first and then too low later on.
- Smaller doses of injected basal insulin are also absorbed more rapidly than larger ones (think 5 units versus 20), and they often do not last as long as expected.
Understand hormonal responses to exercise
The human body only has insulin to lower blood glucose but has five hormones that raise it (with some overlap).
The human body only has insulin to lower blood glucose but has five hormones that raise it (with some overlap). This hormone redundancy tells you that, at least from a survival standpoint, your body is desperate to make sure you do not run out of blood glucose; it is not as concerned about you having too much. Insulin is an important hormone for regulating your body's storage of fuels (carbohydrate, fat, and protein) after you eat. It tells your insulin-sensitive cells (mainly your muscle and fat cells but also your liver) to take up glucose and fat to store them for later as muscle and liver glycogen (the storage form of glucose) as well as stored fat. During exercise, any insulin in your bloodstream can make your muscles take up extra blood glucose. In people who have a pancreas that functions normally, insulin levels typically decrease during exercise, and levels of a hormone called glucagon (released from the alpha cells of the pancreas) rise to stimulate glucose release.
Your blood glucose levels are managed by your liver, which would normally respond to the relative amounts of insulin and glucagon (table 2.1). Insulin and glucagon released from the pancreas go directly to the liver via the portal circulation. After a meal, high insulin and glucose levels tell the liver to store glucose for later use; fasting overnight or doing extended exercise leads to glucagon signaling the liver to release glucose. How people with type 1 diabetes respond hormonally to exercise is a major issue: the insulin and glucagon at the level of the liver are seldom perfectly normal because their insulin is injected or pumped under the skin rather than released directly from the pancreas.
People with type 1 diabetes have an altered hormonal response to exercise when their peripheral insulin is relatively high; lowering the circulating level of insulin helps normalize their hormone response.
All exercise causes the release of hormones that increase the production of glucose by your liver and lower your muscular use, based on how long and hard you exercise. Easy and moderate activities only release a small amount of glucose-raising hormones (unless you do them for a very long duration), but intense exercise such as heavy resistance training, sprinting, or high-intensity intervals causes an immediate rise in your blood glucose and leads to an exaggerated release of hormones. These hormones include adrenaline (formally known as epinephrine) and norepinephrine, which are released by the sympathetic nervous system (allowing your body to respond to physical or mental stressors with an increased heart rate), as well as glucagon, growth hormone, and cortisol (see table 2.1). The effects of these glucose-raising hormones can easily exceed your body's immediate need for glucose, especially because high-intensity exercise may not last long. As a result, your blood glucose often rises during and after short bouts of intense activity.
Intense exercise can cause a large increase in blood glucose because of your body's exaggerated release of glucose-raising hormones such as adrenaline and glucagon.
You may be more insulin resistant immediately after intense exercise and for a few hours due to these hormones. In one study, after near-maximal cycling to exhaustion, one group of people with type 1 diabetes on insulin pumps experienced elevated blood glucose levels for nearly 2 hours. Similarly, in exercisers with type 2 diabetes, blood glucose also rose for 1 hour in response to maximal cycling, as did their insulin levels (because their bodies still produced their own insulin). You may need some supplemental insulin to bring your blood glucose back down (albeit less than normal), or it may drop slowly over time on its own. After these hormones wane, your blood glucose may easily drop later when your body is working hard to restore the muscle glycogen you used during the activity. Be on the lookout for later-onset lows in these cases.
Getting the most from diabetes technologies
Technology and software related to diabetes and health management are advancing faster than most people can keep up with.
Technology and software related to diabetes and health management are advancing faster than most people can keep up with. Every day a new app seems to come out to keep track of something, be it your blood glucose levels, insulin on board, and carbohydrate counting or your calories, daily steps, and fitness goals. In the diabetes world, the latest management technologies guide people in making more informed and effective regimen change decisions—the most important of which are integrated systems that can take charge of the decision making by combining delivery of insulin via pumps, continuous glucose monitoring (CGM), and a control system with potential artificial intelligence(AI) capabilities. Next down the pike is integration of wearable technologies, which can add information related to heart rate and more. More improvements will make AI even more capable of “learning” and updating algorithms to match the changes and patterns in your metabolic state.
Given the challenges of exercising with diabetes, the latest technologies can be beneficial for managing your blood glucose and maximizing the benefits of physical activity. Insulin pumps (covered fully in chapter 3) offer a more fine-tuned ability to regulate basal insulin levels and bolus doses. Blood glucose meters give immediate feedback on where your glucose is starting and how you are responding to an activity. The CGM devices provide an added level of safety by offering the opportunity for improved decision making in real-time and retrospectively. Closed-loop systems that integrate a pump and CGM manage the decision making for you; they can potentially improve your blood glucose management before and during exercise and allow you to avoid any unwanted rises and falls in your blood glucose after workouts. All forms of technology have inherent drawbacks and limitations, but you can overcome most of their issues with planning and knowledge.
Blood Glucose Meters (and Their Precursors)
If you began your journey with diabetes after the advent of home blood glucose meters, consider yourself lucky. Back in 1968 when I began my life with diabetes, no one had blood glucose meters to use for self-monitoring, much less target blood glucose ranges for exercise. All we had were urine tests, which measured the excess glucose and ketones in urine. You would pee in a cup, then put 5 drops of urine with 10 drops of water into a test tube with a tablet. The test tube mixture changed color in a range from cool blue (no glucose) to flaming orange (4+glucose). It did not give you the foggiest idea of what your blood glucose was doing right then; it only told you whether you had been higher than optimal a few hours before. In other words, you could be shaking with the symptoms of a low while watching your urine turn bright orange, the indication of being very high. The ketone test strips merely confirmed what you already knew: you had some ketones in your urine (and therefore your blood) most of the time because the diabetes management tools were lacking.
The next generation of urine test strips eliminated the precise drops and test tubes, but they were not necessarily an improvement. After dipping the test strip in your urine, you had to match the color of the strip to a chart on the side of a bottle. Your six choices ranged from light blue to dark brown, corresponding to negative (0), 100, 250, 500, 1,000, and 2,000 mg/dL or more. This still did not give you a clue about the level of your blood glucose.
The blood glucose test strips of the early 1980s would only estimate your blood glucose within maybe 40 mg/dL (2.2 mmol/L), assuming your glucose was under 200 mg/dL (11.1 mmol/L). Over that range, from one color block to the next, the number jumped up by 100 to 200 mg/dL or more. In other words, blood glucose strips still were not remotely precise enough to allow anyone to safely make regimen changes.
Relatively small and affordable blood glucose meters did not become widely available to individuals until the mid-1980s. I got my first one in 1986 after I had already been living with type 1 diabetes for 18 years. My first meter still had significant potential for user error because you had to blot the blood off the strip halfway through the 2-minute testing period. Even with access to reasonably accurate blood glucose measurements for the first time, we all experienced a steep learning curve while figuring out what to do with our food or insulin in response to the readings.
The moral of this story is that we have come a long way with diabetes technology, even if all you use currently is a blood glucose meter that gives you feedback in only 5 seconds. Appreciate having the ability to check what your blood glucose is doing at any given moment and learn to use that vital information to expertly manipulate your medication doses and diet.
With access to a blood glucose meter, you have the primary tool you need to manage your diabetes effectively, especially with exercise as an added variable. Check as frequently as you need to, with the goal of avoiding both lows and highs.
Even if you do not normally get low during exercise, checking frequently is still advisable, especially before you start and after you finish working out. Once you learn your usual responses to activities, you can usually anticipate how to react to keep your blood glucose in an optimal range to perform well.
Continuous Glucose Monitors
In the past decade or so, a number of continuous glucose monitoring (CGM) devices have received approval from the U.S. Food and Drug Administration (FDA), the European Commission, and across the world. To date, all of them are still invasive: they require that you place and keep a probe of some sort under your skin to get readings. While many innovators are working on noninvasive CGM devices, none have been approved or are available yet for use. At least one company (Senseonics) has FDA approval for an implantable CGM device called Eversense, which lasts for 3 months at a time, and they are seeking approval for up to 180 days. (I have heard that their sensors go in easily during an office visit, but they are more difficult to remove after 90 or 180 days. That is not surprising: that time span is more than sufficient for your body to develop an inflammation and grow new tissue around a foreign object embedded in your skin.)
These monitors by themselves only give you information—much like a blood glucose meter does—but you still have to check the readings and make regimen adjustments yourself. However, getting feedback in real-time or at least every 1 to 5 minutes, 24 hours a day, can be extremely useful when you are trying to learn your patterns, see the trends, or keep your blood glucose in a tighter range with less hypoglycemia. The accuracy of these meters has been improving over time, but they are all still limited by their physiological methods: there is a lag of at least 6 to 20 minutes between the glucose they measure (in interstitialspaces between cells in the skin) and your actual blood glucose. This lag can be even greater during times when your blood glucose levels are often changing rapidly, such as after a meal or during exercise.
The CGM devices and models approved and available in the United States as of the publication of this book are shown in table 5.1. “Flash” glucose monitoring (as offered by the FreeStyle Libre device) is a recent innovation, possessing some but not all features of traditional CGM. Flash monitors can provide instantaneous glucose values and recent trends, but they lack the alerts for lows and highs.
Insurance reimbursement also has become more reasonable since CGM devices were first introduced over a decade ago. (I paid $35 out of pocket for each 3-day sensor for the first-generation Dexcom CGM I tried.) Currently, at least one model is covered by Medicare for anyone with type 1 diabetes age 65 and over. Studies have shown that people with type 2 diabetes—especially those using insulin—can also benefit from using CGM, but coverage for them has been an even harder sell to insurance companies so far. In any case, the number of model choices has declined recently, and their cost is still prohibitive for people who lack the insurance coverage.
What's more, CGM technology is not infallible. As I have noted, a major drawback of CGM devices used during exercise is that their glucose readings are not fully real-time because they measure glucose levels in your skin rather than in your blood, and it takes some time for glucose to move between these two parts of your body. Also, CGM users may have problems getting the device to stay put, similar to the issues experienced by pump users with their infusion sites. (Refer back to table 3.2 for solutions on resolving adhesion issues and to the list of strategies used by athletes in chapter 12; most of the tactics used to secure a pump infusion site will also work for CGM devices.) Other reported challenges include variable sensor accuracy, variable performance between sensors, breakage of sensor filaments, transportation of the sensor display, and inability to calibrate CGM during exercise. (If you have the option, you may want to use an integrated watch to display your values.) Although technical failures during exercise are possible even with the newer versions of these monitors, CGM is still the wave of the future when it comes to monitoring and managing blood glucose.
Exercisers have reported a compression effect when wearing the CGM sensor in areas underneath compression shorts, resulting in a greater lag time in readings due to reduced blood flow to areas with compressed skin. This can also happen when you lie directly on the sensors.
If you have access to CGM, you may be able to use either traditional CGM or Flash monitors to enhance your exercise experience in a variety of ways.
- Seeing your glucose values before exercise tells you whether you are likely to need extra carbohydrates, insulin reductions, or an insulin bolus.
- Knowing your glucose trends before you start to work out can also help you make more informed decisions about any necessary changes in your food or medications.
- High and low alerts during and after exercise can help you avoid dangerous glucose extremes, particularly if you set your alerts at preemptive or conservative levels.
- Reviewing your trend graph reports after working out can show you the patterns of your exercise highs and lows, particularly if you use event markers or workout logs.
Many exercisers swear by their CGM devices and do not want to have to live without them (and hopefully they will not ever have to). But if you do not have access to CGM due to lack of insurance coverage, availability in your country, or other reasons, do not despair—you can still learn your glucose patterns by using frequent checks with a blood glucose meter, as most of us have done. In general, most athletes using CGM have found that observing their glucose trends (shown by up, steady, or down arrows) can be helpful during exercise, even when the readings lag behind actual blood glucose or are sometimes inaccurate.
Troubleshooting your performance like an athlete
As you have come to realize in this chapter, being an athlete is mostly a state of mind. However, sometimes your performance when you are an athlete with diabetes also depends on overcoming some regimen obstacles and other physical issues.
As you have come to realize in this chapter, being an athlete is mostly a state of mind. However, sometimes your performance when you are an athlete with diabetes also depends on overcoming some regimen obstacles and other physical issues. In this final section, you will learn all you need to perform like a professional athlete.
As discussed back in chapter 2, many different factors can impact your blood glucose responses, and the more you know about them, the better equipped you are to figure out what works best for you in almost every situation. Regardless of how knowledgeable you are, this process always takes some trial and error. Consider using some of the following strategies if you are experiencing any of these issues with being active.
Managing Exercise-Associated Hypoglycemia
Having to slow down or stop during an activity due to low blood glucose is annoying even to recreational athletes. It can also compromise your ability to complete your event, competition, or just your daily workout. It is worth keeping this from happening if you can. If you have been having any exercise-related lows, consider taking some of these actions or precautions to avoid them, especially if you use insulin.
Lows During and After Exercise—Food Intake
- Treat lows with glucose or other rapidly absorbed carbohydrate first, and follow that up with other balanced foods and drinks if needed to keep from dropping later.
- Choose pre-exercise foods that require the smallest amount of (or no) insulin to cover them to keep your circulating insulin lower during activities.
- Take in extra carbohydrate before, during, and after activities (depending on your exercise intensity and duration, starting blood glucose, normal diet, and other factors).
- Consider using protein and/or fat intake during prolonged activities to help prevent lows, especially past the first hour of activity, because they take longer to digest.
- Consume some protein and/or fat shortly after exercise and possibly also at bedtime to counteract lows later on and overnight.
Lows During and After Exercise—Insulin Adjustments
- Exercise when your insulin levels are lower, such as before meals or first thing in the morning before taking any bolus insulin.
- Before doing longer duration exercise, lower your insulin levels in anticipation by cutting back on your dose(s) of bolus and/or basal insulin.
- Lower the dose of any rapid-acting insulin you take within 2 to 3 hours before doing an activity (or set a lower basal rate on your insulin pump, if you use one).
- If using an insulin pump, consider lowering your basal rate for up to 2 hours before the start of exercise as well as during (and likely after) the activity.
- If you are prone to lows after exercise, reduce your dose of rapid-acting insulin given after any activity, or set a temporary lower basal rate on your pump for 4 to 12 hours.
- If you inject your basal insulin (Lantus, Basaglar, Levemir, or Toujeo), consider splitting the dose (although not necessarily evenly) to give it twice daily to allow for easier dose reductions before and after activity.
- If you use an even longer-acting basal insulin like Tresiba, watch out for possible insulin “stacking” on subsequent days, particularly when you are more active than normal.
Training Effects and Other Considerations
- Check your blood glucose more often when doing a new activity or unaccustomed exercise because both are more likely to result in lows, both during and afterward.
- Check frequently if you have had a bad low or exercised hard in the 24 hours before your latest workout because both may blunt your release of glucose-raising hormones.
- Try doing an all-out sprint for 10 to 30 seconds to help counteract most lows during exercise, but only if your insulin levels are not too high.
- If you plan on doing both aerobic and resistance training during a workout, vary the order based on whether you want your glucose to stay more stable (during resistance work) or possibly decrease (during moderate aerobic work, although intense training may raise it).
- Keep in mind that the rate of insulin absorption from skin depots depends on the size of the dose: smaller doses (1 to 3 units) are absorbed more rapidly than larger ones (5 or more units), which linger longer while you are active.
- Do not forget that your overall insulin needs are lower when you are regularly active; you may need permanently lower basal (and mealtime bolus) insulin doses.
- Avoid massaging the area where you just gave some insulin—massaging it can speed up its absorption.
- Remember that getting in a hot tub or having other prolonged heat exposure can speed up the absorption of any insulin taken (causing lows first, then highs later).
Dealing With Exercise Hyperglycemia
If you have experienced high blood glucose related to being active, it can be hard to always pinpoint the source of the rise and take actions to prevent or manage it. Consider these possible scenarios and some solutions for troubleshooting.
Highs Before Exercise
- If your blood glucose is over 250 mg/dL (13.9 mmol/L) and has been elevated for a few hours, consider giving yourself some insulin and waiting for the level to decrease before starting to exercise (especially with moderate or higher blood and urine ketones).
- If you take a dose of insulin to lower your glucose with a plan to start exercising shortly thereafter, take less than you normally would (50 percent or less) to prevent your blood glucose from dropping too rapidly during the activity.
- If your blood glucose is over 300 mg/dL (16.7 mmol/L) with no ketones, exercise only if you feel well and use caution because you can dehydrate more easily.
Highs During or After Exercise
- Cut back on your carbohydrate intake during exercise, reduce your insulin less, or take extra insulin after exercise (albeit less than normal).
- Remember that eating a full meal within an hour of starting exercise can slow digestion and result in high blood glucose for 1 to 2 hours afterward, particularly when you have consumed lower glycemic index items (refer to chapter 4 for a discussion of the glycemic index).
- If you disconnect your pump during activities and your blood glucose starts to rise, reconnect at least once an hour and take at least a portion of your missed basal.
- Consider giving yourself some of your “missed” basal insulin in advance in some cases, such as when you have disconnected from your pump before a swim.
- Consider using an “untethered” pump regimen—that is, giving some of your insulin as an injection of long-acting insulin (e.g., Lantus, Levemir, Tresiba) and the rest via pump with a reduced basal rate; then if you disconnect, you still have some basal on board.
- For early morning exercise before eating, consider giving yourself a small dose of insulin (less than normal) and/or a small snack to break your fast to reduce cortisol levels that can lead to elevations at that time of day.
- If the stress or intensity of competitions affects you, keep your basal insulin higher and only give yourself 50 percent or less of your usual correction dose to lower glucose.
- Stay hydrated during activities because dehydration can make blood glucose seem higher (due to being more concentrated) and lead to excess correction dosing.
- Consider doing some easy aerobic exercise after more intense workouts to lower blood glucose naturally.
Training Effects and Other Considerations
- After you have trained for a few weeks doing an activity, you may need fewer carbohydrates or smaller insulin reductions than before training due to a greater use of fat.
- Both endurance training and fat adaptation (from a low-carbohydrate diet) increase your body's efficiency at using fat as a fuel during aerobic activities that are submaximal.
- When you get very sore from exercise (peaking 2 or 3 days afterward), you may be more insulin resistant because you cannot restore muscle glycogen until your muscle damage from the activity is repaired.
- If you load up on carbohydrates before events, you should take enough insulin to cover them; otherwise, loading can raise your blood glucose and limit glycogen storage (check out the discussion on carbohydrate loading in chapter 3).
- You should keep your insulin from getting too hot or too cold; otherwise, its action may diminish and cause your usual doses to inadequately cover your insulin needs.
- Injected or pumped bolus insulin is absorbed faster in smaller doses; after a larger dose, you may end up too high first and then too low later on.
- Smaller doses of injected basal insulin are also absorbed more rapidly than larger ones (think 5 units versus 20), and they often do not last as long as expected.
Understand hormonal responses to exercise
The human body only has insulin to lower blood glucose but has five hormones that raise it (with some overlap).
The human body only has insulin to lower blood glucose but has five hormones that raise it (with some overlap). This hormone redundancy tells you that, at least from a survival standpoint, your body is desperate to make sure you do not run out of blood glucose; it is not as concerned about you having too much. Insulin is an important hormone for regulating your body's storage of fuels (carbohydrate, fat, and protein) after you eat. It tells your insulin-sensitive cells (mainly your muscle and fat cells but also your liver) to take up glucose and fat to store them for later as muscle and liver glycogen (the storage form of glucose) as well as stored fat. During exercise, any insulin in your bloodstream can make your muscles take up extra blood glucose. In people who have a pancreas that functions normally, insulin levels typically decrease during exercise, and levels of a hormone called glucagon (released from the alpha cells of the pancreas) rise to stimulate glucose release.
Your blood glucose levels are managed by your liver, which would normally respond to the relative amounts of insulin and glucagon (table 2.1). Insulin and glucagon released from the pancreas go directly to the liver via the portal circulation. After a meal, high insulin and glucose levels tell the liver to store glucose for later use; fasting overnight or doing extended exercise leads to glucagon signaling the liver to release glucose. How people with type 1 diabetes respond hormonally to exercise is a major issue: the insulin and glucagon at the level of the liver are seldom perfectly normal because their insulin is injected or pumped under the skin rather than released directly from the pancreas.
People with type 1 diabetes have an altered hormonal response to exercise when their peripheral insulin is relatively high; lowering the circulating level of insulin helps normalize their hormone response.
All exercise causes the release of hormones that increase the production of glucose by your liver and lower your muscular use, based on how long and hard you exercise. Easy and moderate activities only release a small amount of glucose-raising hormones (unless you do them for a very long duration), but intense exercise such as heavy resistance training, sprinting, or high-intensity intervals causes an immediate rise in your blood glucose and leads to an exaggerated release of hormones. These hormones include adrenaline (formally known as epinephrine) and norepinephrine, which are released by the sympathetic nervous system (allowing your body to respond to physical or mental stressors with an increased heart rate), as well as glucagon, growth hormone, and cortisol (see table 2.1). The effects of these glucose-raising hormones can easily exceed your body's immediate need for glucose, especially because high-intensity exercise may not last long. As a result, your blood glucose often rises during and after short bouts of intense activity.
Intense exercise can cause a large increase in blood glucose because of your body's exaggerated release of glucose-raising hormones such as adrenaline and glucagon.
You may be more insulin resistant immediately after intense exercise and for a few hours due to these hormones. In one study, after near-maximal cycling to exhaustion, one group of people with type 1 diabetes on insulin pumps experienced elevated blood glucose levels for nearly 2 hours. Similarly, in exercisers with type 2 diabetes, blood glucose also rose for 1 hour in response to maximal cycling, as did their insulin levels (because their bodies still produced their own insulin). You may need some supplemental insulin to bring your blood glucose back down (albeit less than normal), or it may drop slowly over time on its own. After these hormones wane, your blood glucose may easily drop later when your body is working hard to restore the muscle glycogen you used during the activity. Be on the lookout for later-onset lows in these cases.
Getting the most from diabetes technologies
Technology and software related to diabetes and health management are advancing faster than most people can keep up with.
Technology and software related to diabetes and health management are advancing faster than most people can keep up with. Every day a new app seems to come out to keep track of something, be it your blood glucose levels, insulin on board, and carbohydrate counting or your calories, daily steps, and fitness goals. In the diabetes world, the latest management technologies guide people in making more informed and effective regimen change decisions—the most important of which are integrated systems that can take charge of the decision making by combining delivery of insulin via pumps, continuous glucose monitoring (CGM), and a control system with potential artificial intelligence(AI) capabilities. Next down the pike is integration of wearable technologies, which can add information related to heart rate and more. More improvements will make AI even more capable of “learning” and updating algorithms to match the changes and patterns in your metabolic state.
Given the challenges of exercising with diabetes, the latest technologies can be beneficial for managing your blood glucose and maximizing the benefits of physical activity. Insulin pumps (covered fully in chapter 3) offer a more fine-tuned ability to regulate basal insulin levels and bolus doses. Blood glucose meters give immediate feedback on where your glucose is starting and how you are responding to an activity. The CGM devices provide an added level of safety by offering the opportunity for improved decision making in real-time and retrospectively. Closed-loop systems that integrate a pump and CGM manage the decision making for you; they can potentially improve your blood glucose management before and during exercise and allow you to avoid any unwanted rises and falls in your blood glucose after workouts. All forms of technology have inherent drawbacks and limitations, but you can overcome most of their issues with planning and knowledge.
Blood Glucose Meters (and Their Precursors)
If you began your journey with diabetes after the advent of home blood glucose meters, consider yourself lucky. Back in 1968 when I began my life with diabetes, no one had blood glucose meters to use for self-monitoring, much less target blood glucose ranges for exercise. All we had were urine tests, which measured the excess glucose and ketones in urine. You would pee in a cup, then put 5 drops of urine with 10 drops of water into a test tube with a tablet. The test tube mixture changed color in a range from cool blue (no glucose) to flaming orange (4+glucose). It did not give you the foggiest idea of what your blood glucose was doing right then; it only told you whether you had been higher than optimal a few hours before. In other words, you could be shaking with the symptoms of a low while watching your urine turn bright orange, the indication of being very high. The ketone test strips merely confirmed what you already knew: you had some ketones in your urine (and therefore your blood) most of the time because the diabetes management tools were lacking.
The next generation of urine test strips eliminated the precise drops and test tubes, but they were not necessarily an improvement. After dipping the test strip in your urine, you had to match the color of the strip to a chart on the side of a bottle. Your six choices ranged from light blue to dark brown, corresponding to negative (0), 100, 250, 500, 1,000, and 2,000 mg/dL or more. This still did not give you a clue about the level of your blood glucose.
The blood glucose test strips of the early 1980s would only estimate your blood glucose within maybe 40 mg/dL (2.2 mmol/L), assuming your glucose was under 200 mg/dL (11.1 mmol/L). Over that range, from one color block to the next, the number jumped up by 100 to 200 mg/dL or more. In other words, blood glucose strips still were not remotely precise enough to allow anyone to safely make regimen changes.
Relatively small and affordable blood glucose meters did not become widely available to individuals until the mid-1980s. I got my first one in 1986 after I had already been living with type 1 diabetes for 18 years. My first meter still had significant potential for user error because you had to blot the blood off the strip halfway through the 2-minute testing period. Even with access to reasonably accurate blood glucose measurements for the first time, we all experienced a steep learning curve while figuring out what to do with our food or insulin in response to the readings.
The moral of this story is that we have come a long way with diabetes technology, even if all you use currently is a blood glucose meter that gives you feedback in only 5 seconds. Appreciate having the ability to check what your blood glucose is doing at any given moment and learn to use that vital information to expertly manipulate your medication doses and diet.
With access to a blood glucose meter, you have the primary tool you need to manage your diabetes effectively, especially with exercise as an added variable. Check as frequently as you need to, with the goal of avoiding both lows and highs.
Even if you do not normally get low during exercise, checking frequently is still advisable, especially before you start and after you finish working out. Once you learn your usual responses to activities, you can usually anticipate how to react to keep your blood glucose in an optimal range to perform well.
Continuous Glucose Monitors
In the past decade or so, a number of continuous glucose monitoring (CGM) devices have received approval from the U.S. Food and Drug Administration (FDA), the European Commission, and across the world. To date, all of them are still invasive: they require that you place and keep a probe of some sort under your skin to get readings. While many innovators are working on noninvasive CGM devices, none have been approved or are available yet for use. At least one company (Senseonics) has FDA approval for an implantable CGM device called Eversense, which lasts for 3 months at a time, and they are seeking approval for up to 180 days. (I have heard that their sensors go in easily during an office visit, but they are more difficult to remove after 90 or 180 days. That is not surprising: that time span is more than sufficient for your body to develop an inflammation and grow new tissue around a foreign object embedded in your skin.)
These monitors by themselves only give you information—much like a blood glucose meter does—but you still have to check the readings and make regimen adjustments yourself. However, getting feedback in real-time or at least every 1 to 5 minutes, 24 hours a day, can be extremely useful when you are trying to learn your patterns, see the trends, or keep your blood glucose in a tighter range with less hypoglycemia. The accuracy of these meters has been improving over time, but they are all still limited by their physiological methods: there is a lag of at least 6 to 20 minutes between the glucose they measure (in interstitialspaces between cells in the skin) and your actual blood glucose. This lag can be even greater during times when your blood glucose levels are often changing rapidly, such as after a meal or during exercise.
The CGM devices and models approved and available in the United States as of the publication of this book are shown in table 5.1. “Flash” glucose monitoring (as offered by the FreeStyle Libre device) is a recent innovation, possessing some but not all features of traditional CGM. Flash monitors can provide instantaneous glucose values and recent trends, but they lack the alerts for lows and highs.
Insurance reimbursement also has become more reasonable since CGM devices were first introduced over a decade ago. (I paid $35 out of pocket for each 3-day sensor for the first-generation Dexcom CGM I tried.) Currently, at least one model is covered by Medicare for anyone with type 1 diabetes age 65 and over. Studies have shown that people with type 2 diabetes—especially those using insulin—can also benefit from using CGM, but coverage for them has been an even harder sell to insurance companies so far. In any case, the number of model choices has declined recently, and their cost is still prohibitive for people who lack the insurance coverage.
What's more, CGM technology is not infallible. As I have noted, a major drawback of CGM devices used during exercise is that their glucose readings are not fully real-time because they measure glucose levels in your skin rather than in your blood, and it takes some time for glucose to move between these two parts of your body. Also, CGM users may have problems getting the device to stay put, similar to the issues experienced by pump users with their infusion sites. (Refer back to table 3.2 for solutions on resolving adhesion issues and to the list of strategies used by athletes in chapter 12; most of the tactics used to secure a pump infusion site will also work for CGM devices.) Other reported challenges include variable sensor accuracy, variable performance between sensors, breakage of sensor filaments, transportation of the sensor display, and inability to calibrate CGM during exercise. (If you have the option, you may want to use an integrated watch to display your values.) Although technical failures during exercise are possible even with the newer versions of these monitors, CGM is still the wave of the future when it comes to monitoring and managing blood glucose.
Exercisers have reported a compression effect when wearing the CGM sensor in areas underneath compression shorts, resulting in a greater lag time in readings due to reduced blood flow to areas with compressed skin. This can also happen when you lie directly on the sensors.
If you have access to CGM, you may be able to use either traditional CGM or Flash monitors to enhance your exercise experience in a variety of ways.
- Seeing your glucose values before exercise tells you whether you are likely to need extra carbohydrates, insulin reductions, or an insulin bolus.
- Knowing your glucose trends before you start to work out can also help you make more informed decisions about any necessary changes in your food or medications.
- High and low alerts during and after exercise can help you avoid dangerous glucose extremes, particularly if you set your alerts at preemptive or conservative levels.
- Reviewing your trend graph reports after working out can show you the patterns of your exercise highs and lows, particularly if you use event markers or workout logs.
Many exercisers swear by their CGM devices and do not want to have to live without them (and hopefully they will not ever have to). But if you do not have access to CGM due to lack of insurance coverage, availability in your country, or other reasons, do not despair—you can still learn your glucose patterns by using frequent checks with a blood glucose meter, as most of us have done. In general, most athletes using CGM have found that observing their glucose trends (shown by up, steady, or down arrows) can be helpful during exercise, even when the readings lag behind actual blood glucose or are sometimes inaccurate.
Troubleshooting your performance like an athlete
As you have come to realize in this chapter, being an athlete is mostly a state of mind. However, sometimes your performance when you are an athlete with diabetes also depends on overcoming some regimen obstacles and other physical issues.
As you have come to realize in this chapter, being an athlete is mostly a state of mind. However, sometimes your performance when you are an athlete with diabetes also depends on overcoming some regimen obstacles and other physical issues. In this final section, you will learn all you need to perform like a professional athlete.
As discussed back in chapter 2, many different factors can impact your blood glucose responses, and the more you know about them, the better equipped you are to figure out what works best for you in almost every situation. Regardless of how knowledgeable you are, this process always takes some trial and error. Consider using some of the following strategies if you are experiencing any of these issues with being active.
Managing Exercise-Associated Hypoglycemia
Having to slow down or stop during an activity due to low blood glucose is annoying even to recreational athletes. It can also compromise your ability to complete your event, competition, or just your daily workout. It is worth keeping this from happening if you can. If you have been having any exercise-related lows, consider taking some of these actions or precautions to avoid them, especially if you use insulin.
Lows During and After Exercise—Food Intake
- Treat lows with glucose or other rapidly absorbed carbohydrate first, and follow that up with other balanced foods and drinks if needed to keep from dropping later.
- Choose pre-exercise foods that require the smallest amount of (or no) insulin to cover them to keep your circulating insulin lower during activities.
- Take in extra carbohydrate before, during, and after activities (depending on your exercise intensity and duration, starting blood glucose, normal diet, and other factors).
- Consider using protein and/or fat intake during prolonged activities to help prevent lows, especially past the first hour of activity, because they take longer to digest.
- Consume some protein and/or fat shortly after exercise and possibly also at bedtime to counteract lows later on and overnight.
Lows During and After Exercise—Insulin Adjustments
- Exercise when your insulin levels are lower, such as before meals or first thing in the morning before taking any bolus insulin.
- Before doing longer duration exercise, lower your insulin levels in anticipation by cutting back on your dose(s) of bolus and/or basal insulin.
- Lower the dose of any rapid-acting insulin you take within 2 to 3 hours before doing an activity (or set a lower basal rate on your insulin pump, if you use one).
- If using an insulin pump, consider lowering your basal rate for up to 2 hours before the start of exercise as well as during (and likely after) the activity.
- If you are prone to lows after exercise, reduce your dose of rapid-acting insulin given after any activity, or set a temporary lower basal rate on your pump for 4 to 12 hours.
- If you inject your basal insulin (Lantus, Basaglar, Levemir, or Toujeo), consider splitting the dose (although not necessarily evenly) to give it twice daily to allow for easier dose reductions before and after activity.
- If you use an even longer-acting basal insulin like Tresiba, watch out for possible insulin “stacking” on subsequent days, particularly when you are more active than normal.
Training Effects and Other Considerations
- Check your blood glucose more often when doing a new activity or unaccustomed exercise because both are more likely to result in lows, both during and afterward.
- Check frequently if you have had a bad low or exercised hard in the 24 hours before your latest workout because both may blunt your release of glucose-raising hormones.
- Try doing an all-out sprint for 10 to 30 seconds to help counteract most lows during exercise, but only if your insulin levels are not too high.
- If you plan on doing both aerobic and resistance training during a workout, vary the order based on whether you want your glucose to stay more stable (during resistance work) or possibly decrease (during moderate aerobic work, although intense training may raise it).
- Keep in mind that the rate of insulin absorption from skin depots depends on the size of the dose: smaller doses (1 to 3 units) are absorbed more rapidly than larger ones (5 or more units), which linger longer while you are active.
- Do not forget that your overall insulin needs are lower when you are regularly active; you may need permanently lower basal (and mealtime bolus) insulin doses.
- Avoid massaging the area where you just gave some insulin—massaging it can speed up its absorption.
- Remember that getting in a hot tub or having other prolonged heat exposure can speed up the absorption of any insulin taken (causing lows first, then highs later).
Dealing With Exercise Hyperglycemia
If you have experienced high blood glucose related to being active, it can be hard to always pinpoint the source of the rise and take actions to prevent or manage it. Consider these possible scenarios and some solutions for troubleshooting.
Highs Before Exercise
- If your blood glucose is over 250 mg/dL (13.9 mmol/L) and has been elevated for a few hours, consider giving yourself some insulin and waiting for the level to decrease before starting to exercise (especially with moderate or higher blood and urine ketones).
- If you take a dose of insulin to lower your glucose with a plan to start exercising shortly thereafter, take less than you normally would (50 percent or less) to prevent your blood glucose from dropping too rapidly during the activity.
- If your blood glucose is over 300 mg/dL (16.7 mmol/L) with no ketones, exercise only if you feel well and use caution because you can dehydrate more easily.
Highs During or After Exercise
- Cut back on your carbohydrate intake during exercise, reduce your insulin less, or take extra insulin after exercise (albeit less than normal).
- Remember that eating a full meal within an hour of starting exercise can slow digestion and result in high blood glucose for 1 to 2 hours afterward, particularly when you have consumed lower glycemic index items (refer to chapter 4 for a discussion of the glycemic index).
- If you disconnect your pump during activities and your blood glucose starts to rise, reconnect at least once an hour and take at least a portion of your missed basal.
- Consider giving yourself some of your “missed” basal insulin in advance in some cases, such as when you have disconnected from your pump before a swim.
- Consider using an “untethered” pump regimen—that is, giving some of your insulin as an injection of long-acting insulin (e.g., Lantus, Levemir, Tresiba) and the rest via pump with a reduced basal rate; then if you disconnect, you still have some basal on board.
- For early morning exercise before eating, consider giving yourself a small dose of insulin (less than normal) and/or a small snack to break your fast to reduce cortisol levels that can lead to elevations at that time of day.
- If the stress or intensity of competitions affects you, keep your basal insulin higher and only give yourself 50 percent or less of your usual correction dose to lower glucose.
- Stay hydrated during activities because dehydration can make blood glucose seem higher (due to being more concentrated) and lead to excess correction dosing.
- Consider doing some easy aerobic exercise after more intense workouts to lower blood glucose naturally.
Training Effects and Other Considerations
- After you have trained for a few weeks doing an activity, you may need fewer carbohydrates or smaller insulin reductions than before training due to a greater use of fat.
- Both endurance training and fat adaptation (from a low-carbohydrate diet) increase your body's efficiency at using fat as a fuel during aerobic activities that are submaximal.
- When you get very sore from exercise (peaking 2 or 3 days afterward), you may be more insulin resistant because you cannot restore muscle glycogen until your muscle damage from the activity is repaired.
- If you load up on carbohydrates before events, you should take enough insulin to cover them; otherwise, loading can raise your blood glucose and limit glycogen storage (check out the discussion on carbohydrate loading in chapter 3).
- You should keep your insulin from getting too hot or too cold; otherwise, its action may diminish and cause your usual doses to inadequately cover your insulin needs.
- Injected or pumped bolus insulin is absorbed faster in smaller doses; after a larger dose, you may end up too high first and then too low later on.
- Smaller doses of injected basal insulin are also absorbed more rapidly than larger ones (think 5 units versus 20), and they often do not last as long as expected.
Understand hormonal responses to exercise
The human body only has insulin to lower blood glucose but has five hormones that raise it (with some overlap).
The human body only has insulin to lower blood glucose but has five hormones that raise it (with some overlap). This hormone redundancy tells you that, at least from a survival standpoint, your body is desperate to make sure you do not run out of blood glucose; it is not as concerned about you having too much. Insulin is an important hormone for regulating your body's storage of fuels (carbohydrate, fat, and protein) after you eat. It tells your insulin-sensitive cells (mainly your muscle and fat cells but also your liver) to take up glucose and fat to store them for later as muscle and liver glycogen (the storage form of glucose) as well as stored fat. During exercise, any insulin in your bloodstream can make your muscles take up extra blood glucose. In people who have a pancreas that functions normally, insulin levels typically decrease during exercise, and levels of a hormone called glucagon (released from the alpha cells of the pancreas) rise to stimulate glucose release.
Your blood glucose levels are managed by your liver, which would normally respond to the relative amounts of insulin and glucagon (table 2.1). Insulin and glucagon released from the pancreas go directly to the liver via the portal circulation. After a meal, high insulin and glucose levels tell the liver to store glucose for later use; fasting overnight or doing extended exercise leads to glucagon signaling the liver to release glucose. How people with type 1 diabetes respond hormonally to exercise is a major issue: the insulin and glucagon at the level of the liver are seldom perfectly normal because their insulin is injected or pumped under the skin rather than released directly from the pancreas.
People with type 1 diabetes have an altered hormonal response to exercise when their peripheral insulin is relatively high; lowering the circulating level of insulin helps normalize their hormone response.
All exercise causes the release of hormones that increase the production of glucose by your liver and lower your muscular use, based on how long and hard you exercise. Easy and moderate activities only release a small amount of glucose-raising hormones (unless you do them for a very long duration), but intense exercise such as heavy resistance training, sprinting, or high-intensity intervals causes an immediate rise in your blood glucose and leads to an exaggerated release of hormones. These hormones include adrenaline (formally known as epinephrine) and norepinephrine, which are released by the sympathetic nervous system (allowing your body to respond to physical or mental stressors with an increased heart rate), as well as glucagon, growth hormone, and cortisol (see table 2.1). The effects of these glucose-raising hormones can easily exceed your body's immediate need for glucose, especially because high-intensity exercise may not last long. As a result, your blood glucose often rises during and after short bouts of intense activity.
Intense exercise can cause a large increase in blood glucose because of your body's exaggerated release of glucose-raising hormones such as adrenaline and glucagon.
You may be more insulin resistant immediately after intense exercise and for a few hours due to these hormones. In one study, after near-maximal cycling to exhaustion, one group of people with type 1 diabetes on insulin pumps experienced elevated blood glucose levels for nearly 2 hours. Similarly, in exercisers with type 2 diabetes, blood glucose also rose for 1 hour in response to maximal cycling, as did their insulin levels (because their bodies still produced their own insulin). You may need some supplemental insulin to bring your blood glucose back down (albeit less than normal), or it may drop slowly over time on its own. After these hormones wane, your blood glucose may easily drop later when your body is working hard to restore the muscle glycogen you used during the activity. Be on the lookout for later-onset lows in these cases.
Related Books









