
- Home
- Physical Activity and Health
- Medicine in Exercise and Sport
- Kinesiology/Exercise and Sport Science
- Health Care in Exercise and Sport
- Foundations of Physical Activity and Public Health

Foundations of Physical Activity and Public Health
by Harold W. Kohl, Tinker D. Murray and Deborah Salvo
320 Pages
Joining field leaders Harold (Bill) Kohl and Tinker Murray on this second edition is Deborah Salvo, an international expert with a special interest in the relationship between the built environment and health. Other updates to this edition include the following:
- New content on the use of electronic devices—such as pedometers and consumer-based wearable technology and apps—for measuring physical activity
- Urban design strategies for promoting physical activity at the community level
- An engaging, full-color visual presentation
- A new web resource that includes key term learning activities and links to the National Physical Activity Society (NPAS) core competencies for public health physical activity practitioners that relate to each chapter
To further tie theory to practice, case studies and callout boxes throughout the text provide practical examples, and each chapter ends with a review to solidify student understanding of the material. Leader Profile sidebars allow students to explore career options while learning more about individuals who have had a major impact on this growing field.
As the emphasis on physical activity as a tool for improving public health grows, professionals with combined knowledge and skills from both public health and exercise science fields will be highly sought. Foundations of Physical Activity and Public Health, Second Edition, will help students obtain an overview of kinesiology and public health areas, understand physical activity applications for public health, and learn about career options, and it will inspire them to choose a career and make a difference in the emerging field of physical activity and public health.
Chapter 1. Fundamentals of Public Health
Defining Moments in Public Health
Areas of Specialization in Public Health
Core Functions of Public Health
Public Health Law
Chapter 2. Fundamentals of Kinesiology
Kinesiology Subdisciplines and Exercise Training
Principles of Exercise Training, Prescription, and Planning
Applying Physical Activity and Exercise Training Principles
Health and Fitness Benefits of Physical Activity and Exercise
Chapter 3. Integrating Public Health and Physical Activity
History of Physical Activity and Public Health
Role of Physical Activity in Chronic Disease Development
From Science to Practice and Back
Promoting Physical Activity for Health
Practitioners of Physical Activity in Public Health
Chapter 4. Measuring Physical Activity
Evidence-Based Recommended Levels of Physical Activity for Health
Laboratory Measures of Energy Expenditure
Electronic Devices to Measure Physical Activity
Direct Observation Techniques
Self-Report Instruments
Surveillance in Populations
Combining Measurement Approaches
Part II. Health Effects of Exercise and Physical Activity
Chapter 5. Cardiorespiratory and Metabolic Health
Prevalence of Cardiovascular Disease
Risk Factors for Cardiovascular Disease
Kinesiology and Cardiorespiratory Health
Cardiorespiratory Fitness Assessments
General Recommendations for Cardiorespiratory Health
Prevalence and Economic Costs of Metabolic Disease
Metabolic Disease Risk Factors
Kinesiology and Metabolic Health
Common Tests of Metabolic Function
General Recommendations for Metabolic Health
Chapter 6. Overweight and Obesity
Caloric Balance
Prevalence of Obesity and Overweight and Associated Health Consequences
Obesity and Overweight Risk Factors
Obesity and Overweight Challenges
Kinesiology and Body Weight
Common Assessments of Obesity and Overweight
Physical Activity Guidelines for a Healthy Weight
Chapter 7. Musculoskeletal and Functional Health
Prevalence of Musculoskeletal Disorders and Related Health Challenges
Risk Factors Associated With Musculoskeletal Disorders and Associated Health Challenges
Kinesiology and Musculoskeletal Health
Common Tests of Musculoskeletal Fitness or Function
Physical Activity and Musculoskeletal Health
Functional Health
Risk Factors for Poor Functional Health
Common Tests of Functional Health
Fitness Recommendations for Functional Health
Chapter 8. Cancers
Prevalence of Cancers
Cancer Risk Factors
Kinesiology and Cancers
Physical Activity Among Cancer Survivors
Physical Activity Guidelines for Cancer Prevention
Chapter 9. Brain Health
Prevalence and Economic Costs of Brain Health Disorders
Common Brain Health Conditions
Risk Factors Associated With Brain Health Disorders
Physical Activity and Brain Health
Physical Activity and Brain Cognitive Function
Physical Activity Guidelines for Brain Health
Chapter 10. Health Risks of Exercise and Physical Activity
Musculoskeletal Injuries
Kinesiology and Musculoskeletal Injuries
Sudden Adverse Cardiac Events
Part III. Strategies for Effective Physical Activity Promotion
Chapter 11. Informational Approaches for Promoting Physical Activity
Understanding the Community Guide
Rationale for Informational Approaches
Chapter 12. School-Based Approaches to Promoting Physical Activity
Rationale for School-Based Physical Activity Programs
Kinesiology and Physical Activity Outcomes for Youth
School-Based Physical Activity and Physical Fitness Assessments of Youth
Physical Activity in Children and Adolescents
International and National Trends in Youth Physical Activity Levels
School-Based Physical Education
Developmental Considerations for Physical Activity in Youth
Chapter 13. Behavioral and Social Approaches to Understanding and Promoting Physical Activity
Behavioral Theories and Theoretical Models of Behavior Change
Social Support for Health Behavior Change
Individually Adapted Health Behavior Change Programs
Socio-Ecological Model of Behavior
Social Support Interventions in Community Settings
Chapter 14. Environmental and Policy Approaches to Promoting Physical Activity
Access
Urban Design
Measuring the Built Environment
Physical Activity Policy
Land Use Policy
Co-Benefits of Activity-Promoting Environments and Policies
Chapter 15. Program and Policy Evaluation for Physical Activity and Public Health
Ways to Measure Program and Policy Effectiveness
Logic Models for Physical Activity Promotion and Policies
Evaluation Designs
Data Collection and Analysis
Publishing and Communicating Results
Chapter 16. Partnership Development and Advocacy
Key Factors in Building Partnerships
Strategies for Physical Activity Advocacy
Harold W. (Bill) Kohl, III, PhD, was a professor of epidemiology and kinesiology at the University of Texas Health Science Center at Houston and the University of Texas at Austin. At the University of Texas Health Science Center, Dr. Kohl also served as the associate regional dean for academic affairs and international health affairs at the Austin regional campus.
His research concentrated on national and international physical activity surveillance and epidemiology issues, as well as program development and evaluation studies for the promotion of school-based physical activity for children and adolescents. He was a fellow of the American College of Sports Medicine (ACSM) and the National Academy of Kinesiology, and served as an elected trustee of ACSM. He was the founder and past president of the International Society for Physical Activity and Health and served as the elected chair of the U.S. National Physical Activity Plan Alliance. He also served in an editorial capacity for several scientific journals and is editor emeritus of the Journal of Physical Activity and Health. He published more than 200 papers, chapters, and monographs in the scientific literature. In 2018 he coauthored the textbook Foundations of Kinesiology.
Bill Kohl passed away in 2023.
Tinker D. Murray, PhD, is a professor emeritus and honorary professor of international studies in health and human performance at Texas State University in San Marcos. He earned his PhD in physical education from Texas A&M University in 1984. His research interests include school-based and clinical-based youth physical activity and interventions with public health linkages for the prevention of obesity and diabetes, continuing education opportunities for coaching education, and personal fitness and training applications related to exercise physiology.
From 1982 to 1984, Murray served as director of cardiac rehabilitation at Brooke Army Medical Center, where he was twice recognized for his exceptional performance. He began his career at Texas State University (formerly Southwest Texas State), where he served as the director of employee wellness from 1984 to 1988 and director of the exercise performance laboratory from 1984 to 2000. He was a volunteer assistant cross country and track coach at Southwest Texas State from 1985 to 1988 and helped win three Gulf Star Conference titles.
From 1985 to 1988, he was a subcommittee member for the Governor's Commission on Physical Fitness that developed the Fit Youth Today program. He served as lecturer and examiner for the USA Track and Field Level 2 coaching certification program from 1988 to 2008 and as the vice chair of the Governor's Commission on Physical Fitness in Texas from 1993 to 1994. He worked with the Texas High School Coaches Association (THSCA) from 2003 to 2013 as a facilitator with the Professional Development Cooperative, which promoted continuing education opportunities.
Murray is a fellow of the American College of Sports Medicine (ACSM) and is certified as an ACSM program director. He was a two-time president of the Texas regional chapter of ACSM (1987 and 1994). He served on the national ACSM board of trustees from 1998 to 2001. In the fall of 2003, he was a guest researcher at the Centers for Disease Control and Prevention (CDC) Division of Nutrition and Physical Activity. He has been actively involved with the International Society for Physical Activity and Health (ISPAH) and has attended several biannual meetings of the International Congress on Physical Activity and Public Health.
Murray retired from Texas State University in 2018 and was named a professor emeritus and honorary professor of international studies. He continues to remain physically active by cycling daily, jogging often, and lifting weights twice a week. He remains academically active by contributing to scholarly presentations and publications that promote physical active lifestyles.
Deborah Salvo, PhD, is an assistant professor of public health at the Brown School at Washington University in St. Louis, where she is a faculty scholar of the Prevention Research Center, the Center for Diabetes Translation Research, and the Institute for Public Health. Before this appointment, she held positions at the University of Texas School Health Science Center in Austin, Stanford University’s Prevention Research Center, and the National Institute of Public Health of Mexico.
Salvo is a native of Mexico City, Mexico, and earned her bachelor’s degree in nutrition and food sciences from Universidad Iberoamericana. She earned her doctorate in biological and biomedical sciences (nutrition and health sciences, public health and epidemiology track) from Emory University in 2013. Her interests lie in understanding the role of built environment on physical activity and health, and in using this evidence to resolve global health disparities. Her work ranges from local projects to multisite international consortia. She has expertise in using, improving, and developing novel methodological approaches that combine physical activity and spatial epidemiological tools to address complex questions on the effects of context on health. Throughout her career, she has facilitated and led international collaborations to support the growth of the field of physical activity and public health on a global scale, with special emphasis on low- and middle-income countries and populations.
Salvo is the current chair of the Council on Environment and Physical Activity within the International Society for Physical Activity and Health. She is also part of the steering committee of the Global Observatory for Physical Activity, and she is an active member of the Our Voice Global Network. Salvo serves as associate editor for Preventing Chronic Disease, an official scientific journal of the Centers for Disease Control and Prevention. Throughout her career, she has served as technical advisor on physical activity and the built environment for several agencies, including the Centers for Disease Control and Prevention, the Fogarty International Center within the National Institutes of Health, the National Institute of Public Health of Mexico, and the World Health Organization. Salvo was a contributing author to the second series on physical activity published by The Lancet in 2016, which convened global experts to present the latest evidence of the important role of physical activity for public health.
Community-scale or macro-environmental urban design
Community-scale or macro-environmental urban design strategies for promoting physical activity involve changes and enhancements to the built environment of urban areas of several square miles (or kilometers) or larger, which are usually defined as being an administrative unit (zip code, neighborhood, school district, city, or county). These kinds of approaches strive to make entire communities more amenable to physical activity, whether that activity is transportation-related or exercise performed in discretionary time. Strategies at this level of influence include connecting transportation arteries; creating landscaping and lighting to enhance the aesthetics and perceived safety of the entire community; building a large-scale and interconnected network of sidewalks, bicycle lanes, and trails; and designing new mixed-use residential areas so that destinations such as workplaces, schools, and areas for leisure and recreation are within safe walking or bicycling distances.
One important and unique macro-environmental urban design element is road connectivity. The concept of connectivity refers to the ease of getting from one place to another within a neighborhood using the city's road network to walk or bike. If city thoroughfares follow a grid pattern, it is easy to use the street network (assuming sidewalks or bicycle lanes are available) to move around on foot or on bicycle; however, if intersections are very far from each other or there are quite a few dead-end streets or culs-de-sac, connectivity is considered to be sub-optimal. Another related construct for the macro-environment that has emerged in the past couple of decades is walkability. Walkability refers to the conduciveness of walking for transportation based on features of the built environment of an urban area. Many researchers have proposed different definitions of walkability, using scores or indices. Some of these scores are even used by real-estate companies to provide their clients with information about potential neighborhoods. High walkability scores or indices could indicate the best mix of built environment elements, and if optimized, could point to a neighborhood that is very easy to navigate on foot. Likewise, neighborhoods with low walkability scores are those with suboptimal conditions for transport-based walking. Most available walkability scores or indices include measures of connectivity, land-use mix, and residential density, which are three critical components for optimal urban design that promote walking for transportation in an area. Although this definition for walkability is valid in many parts of the world, it is not applicable in others (e.g., Mexico or China) (Salvo et al. 2014; Lu et al. 2017). Therefore, it is always important to consider the local context, including the social environment (social norms and cultural values), when trying to promote walkable environments because these may look different in other parts of the world.
Studies examining community-scale changes for physical activity promotion have used a wide variety of outcome measures (Heath et al. 2006). Some have studied the absolute number of walking trips in a community over a given time period; others, the distance of those trips, minutes of walking per week, and number of pedestrians in a certain area. Although these outcomes are not entirely comparable, the general interpretation is that making the built environment more activity-friendly can improve levels of physical activity (regardless of how it is measured) by an average of more than 160%. Clearly, this is a major influence on physical activity habits in a community.
Development of health guidelines
The development of health guidelines is a third critical function of public health science. Public health guidelines are official policy statements, usually developed by a government body, agency, or other reputable organization, that are based on the best available science. Public health guidelines provide clear recommendations about a course of action to deal with a pressing public health issue. Recommendations for childhood immunization schedules (when and which vaccines and their timing), diabetes treatment (the frequency and method of glucose self-monitoring), nutrient intake (micronutrient daily recommended intakes for health), and annual influenza vaccinations (type and timing) are all examples of public health guidelines that, based on the best available science, give health professionals and the public clear guidance about the most appropriate courses of action for preventing and treating certain health problems.
In 2008, the U.S. Department of Health and Human Services published the first Physical Activity Guidelines for Americans (USDHHS 2008; see the highlight box2018 Physical Activity Guidelines for Americans). These guidelines, updated in 2018, are based on comprehensive scientific summaries to detail the best science-based recommendation for the weekly amount of physical activity necessary to prevent disease and promote positive health outcomes (USDHHS 2018). The physical activity guidelines were developed for children and adolescents, adults, and older adults. These guidelines should be used as targets for physical activity participation.
Several other countries, as well as the World Health Organization, have published guidelines similar to the Physical Activity Guidelines for Americans. Japan, Canada, Australia, and England have all taken leadership roles in establishing physical activity as a public health priority by setting physical activity guidelines and recommendations.
Promoting Physical Activity for Health
As the field of physical activity and public health has emerged, it has become clear that many factors at many levels influence physical activity behaviors. Many investigators have used the social ecological model as a guiding framework to explain these multiple levels. They are illustrated in figure 3.6 and form the basis for the third section of this textbook.
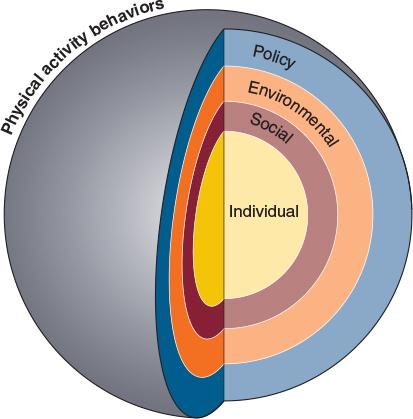
Figure 3.6 Multiple levels of influence on physical activity behaviors: The social ecological model.
At the center of the target in the social ecological model for physical activity behaviors are individual factors. These are the factors that are innate to each person and that differ among people. A person's genetic makeup, early life experiences (e.g., youth sport participation), self-efficacy, and other factors, such as sex, disability, growth and development, and socioeconomic status, may all be important determinants of health behaviors such as physical activity.
Moving out from the center, social influences on physical activity are important. Research has now shown that individual factors are not enough to explain physical activity behavior. Determinants at the social influences level aren't characteristics of the person per se, but are, rather, characteristics of how the person interacts with society or culture. Influences at this level can include peers, medical care organizations (doctors), family members, and organizations (schools, places of worship, worksites).
The third level in the social ecological model represents environmental influences. These influences may enhance or restrict physical activity behaviors, and are external to the person but common across societies and cultures. Research on the effects of physical environment on physical activity participation has exploded as the field of physical activity and public health has emerged. The ability to influence the physical activity of vast numbers of people (instead of one person at a time) by making a single change makes environmental influences on physical activity a particularly interesting area of research. The availability of places to be active, such as trails, sidewalks, fitness facilities, bicycle lanes, community and neighborhood design elements are examples of how the built environment can influence physical activity.
Finally, the outer level represents policy influences on physical activity. Influences in this sphere include written or unwritten rules, codes, and norms that influence environmental or social determinants of physical activity. As with the physical environment, determinants at this level are particularly attractive because of their potential to influence many people. Examples of policy influences on physical activity include policies allowing increased access to places to be physically active (making it easier to be physically active), educational policies (e.g., mandating high-quality daily physical education for schoolchildren), and transportation-related policies (e.g., making it easier to walk or bicycle for transportation).
By combining knowledge, skills, and abilities related to the basic exercise sciences and public health, you can better explain and discuss professionally the health benefits and risks of exercise and physical activity to your peers, colleagues, and the communities you serve (see part II, chapters 5 through 10). An understanding of the specific challenges that affect physical activity and exercise in professional exercise science jobs can clarify how the exercise sciences affect public health, and vice versa. The highlight box Careers Combining Exercise Science and Public Health lists careers in exercise physiology, biomechanics, and sport and exercise psychology that are commonly seen in the professional areas of health and fitness, preventive medicine, athletic performance, and rehabilitation.
Physical activity guidelines for a healthy weight
For many adults, obesity is associated with significant increases in abdominal fat that increase the risk for metabolic syndrome and type 2 diabetes (see chapter 5). Regular participation in aerobic physical activity and exercise can decrease total body fat and abdominal fat, and these changes are consistent with improved metabolic function. Generally, the greater the volume of physical activity or exercise acquired by individuals or populations, the greater the reductions in body and abdominal fat.
For children and adolescents, the prevention of excessive weight gain during maturation is critical to prevent obesity and overweight in adulthood. Unfortunately, recent public health surveys note that the parents of many at-risk children are not aware of the problem or do not recognize that their children are overweight. Recent U.S. national policy statements targeting pediatricians and other health care providers assert that children and adolescents who are overweight or obese in their early teens should be identified as early as possible and given some sort of weight management plan through the intervention of parents, teachers, coaches, and family physicians.
One of the most obvious influences on weight management is how people perceive their ideal weight or physique. Research findings indicate a great disparity between reasonable weight loss or weight gain goals and people's “dream weight.” Even though some people may not reach their goal weight, they will likely report positive physical, social, and psychological benefits from any weight loss. The following scientific evidence and guidelines can help individuals and populations establish realistic goals for weight management (e.g., achieving a healthy weight) and meet their specific needs (e.g., weight loss, weight stability, prevention of weight regain, or loss of excessive abdominal fat) through regular participation in physical activity and exercise.
Scientific Evidence
The 2008 PAGAC noted physical activity (150 minutes per week to ≥300 minutes per week) was associated with modest weight loss, prevention of weight gain following weight loss, and reductions in total and regional adiposity. Evidence that resistance training helped with weight maintenance was not as strong, given that resistance training increases lean muscle mass, and the volume of resistance training regimes was usually less than that for aerobic training.
The 2018 PAGAC expanded the review of the evidence available in 2008, and focused on weight maintenance and weight gain within normal BMI limits (18.5 to < 25 kg/m2) for adults in relation to participating in 150 minutes per week or more of physical activity. The 2018 report also reviewed the impact of sedentary behavior and sedentary activity in relationship to physical activity and weight status. The specific 2018 PAGAC findings regarding weight gain were:
- Strong evidence demonstrates that the significant relationship between greater time spent in physical activity (≥300 minutes per week) and attenuated weight gain in adults is observed with moderate-to-vigorous physical activity.
- Moderate evidence indicates that the relationship between greater amounts of physical activity and attenuated weight gain in adults does not appear to vary by sex.
- Limited evidence suggests a dose-response relationship between physical activity and the risk of weight gain in adults, with greater amounts of physical activity (150 minutes per week) associated with lower risk of weight gain.
- Limited evidence suggests that the relationship between greater amounts of physical activity and attenuated weight gain in adults varies by age, with the effect diminishing with increasing age. The evidence from studies of older adults, however, is inconsistent.
- Insufficient evidence is available to determine whether the relationship between greater amounts of physical activity and attenuated weight gain in adults varies by race and ethnicity.
- Insufficient evidence is available to determine whether the relationship between greater amounts of physical activity and attenuated weight gain in adults varies by socioeconomic status.
- Insufficient evidence is available to determine whether the relationship between greater amounts of physical activity and attenuated weight gain in adults varies by initial weight status.
- Insufficient evidence is available to determine an association between light-intensity activity and attenuated weight gain in adults.
The 2018 PAGAC concluded the following with regard to the impact of sedentary behavior and sedentary activity for adults in relationship to physical activity and weight status:
- Limited evidence suggests a positive relationship between greater time spent in sedentary behavior and higher levels of adiposity and indicators of weight status.
- Limited evidence suggests the existence of a direct, graded dose-response relationship between greater sedentary behavior and higher levels of adiposity and indicators of weight status.
- Insufficient evidence is available to determine whether the relationship between sedentary behavior and weight status varies by age, sex, ethnicity, socioeconomic status, or baseline weight status.
- Insufficient evidence is available to determine whether the relationship between sedentary behavior and weight status varies by amount of moderate-to-vigorous physical activity.
- Insufficient evidence is available to determine whether bouts or breaks in sedentary behavior are important factors in the relationship between sedentary behavior and weight status.
As mentioned earlier in the chapter, regular physical activity and exercise are also important to prevent and control obesity and overweight in children and adolescents. The 2008 PAGAC found strong evidence demonstrating that higher levels of physical activity were associated with multiple beneficial health outcomes, including cardiorespiratory and muscular fitness, bone health, and maintenance of healthy weight status in children and adolescents (ages 6-19). The 2018 PAGAC focused on expanding the review of literature since 2008 with the addition of studies on children 3-6 years of age. The additional scientific recommendations of the 2018 PAGAC for youth were as follows:
- Strong evidence demonstrates that higher amounts of physical activity are associated with a reduced risk of excessive increases in body weight and adiposity in children ages 3 to 6 years.
- Limited evidence suggests that greater time spent in sedentary behavior is related to higher weight status or adiposity in children and adolescents; the evidence is somewhat stronger for television viewing or screen time than for total sedentary time.
- Insufficient evidence is available to determine whether the relationship between physical activity and health effects in children younger than 6 years of age is moderated by age, sex, race, ethnicity, weight status, or socioeconomic status.
Community-scale or macro-environmental urban design
Community-scale or macro-environmental urban design strategies for promoting physical activity involve changes and enhancements to the built environment of urban areas of several square miles (or kilometers) or larger, which are usually defined as being an administrative unit (zip code, neighborhood, school district, city, or county). These kinds of approaches strive to make entire communities more amenable to physical activity, whether that activity is transportation-related or exercise performed in discretionary time. Strategies at this level of influence include connecting transportation arteries; creating landscaping and lighting to enhance the aesthetics and perceived safety of the entire community; building a large-scale and interconnected network of sidewalks, bicycle lanes, and trails; and designing new mixed-use residential areas so that destinations such as workplaces, schools, and areas for leisure and recreation are within safe walking or bicycling distances.
One important and unique macro-environmental urban design element is road connectivity. The concept of connectivity refers to the ease of getting from one place to another within a neighborhood using the city's road network to walk or bike. If city thoroughfares follow a grid pattern, it is easy to use the street network (assuming sidewalks or bicycle lanes are available) to move around on foot or on bicycle; however, if intersections are very far from each other or there are quite a few dead-end streets or culs-de-sac, connectivity is considered to be sub-optimal. Another related construct for the macro-environment that has emerged in the past couple of decades is walkability. Walkability refers to the conduciveness of walking for transportation based on features of the built environment of an urban area. Many researchers have proposed different definitions of walkability, using scores or indices. Some of these scores are even used by real-estate companies to provide their clients with information about potential neighborhoods. High walkability scores or indices could indicate the best mix of built environment elements, and if optimized, could point to a neighborhood that is very easy to navigate on foot. Likewise, neighborhoods with low walkability scores are those with suboptimal conditions for transport-based walking. Most available walkability scores or indices include measures of connectivity, land-use mix, and residential density, which are three critical components for optimal urban design that promote walking for transportation in an area. Although this definition for walkability is valid in many parts of the world, it is not applicable in others (e.g., Mexico or China) (Salvo et al. 2014; Lu et al. 2017). Therefore, it is always important to consider the local context, including the social environment (social norms and cultural values), when trying to promote walkable environments because these may look different in other parts of the world.
Studies examining community-scale changes for physical activity promotion have used a wide variety of outcome measures (Heath et al. 2006). Some have studied the absolute number of walking trips in a community over a given time period; others, the distance of those trips, minutes of walking per week, and number of pedestrians in a certain area. Although these outcomes are not entirely comparable, the general interpretation is that making the built environment more activity-friendly can improve levels of physical activity (regardless of how it is measured) by an average of more than 160%. Clearly, this is a major influence on physical activity habits in a community.
Development of health guidelines
The development of health guidelines is a third critical function of public health science. Public health guidelines are official policy statements, usually developed by a government body, agency, or other reputable organization, that are based on the best available science. Public health guidelines provide clear recommendations about a course of action to deal with a pressing public health issue. Recommendations for childhood immunization schedules (when and which vaccines and their timing), diabetes treatment (the frequency and method of glucose self-monitoring), nutrient intake (micronutrient daily recommended intakes for health), and annual influenza vaccinations (type and timing) are all examples of public health guidelines that, based on the best available science, give health professionals and the public clear guidance about the most appropriate courses of action for preventing and treating certain health problems.
In 2008, the U.S. Department of Health and Human Services published the first Physical Activity Guidelines for Americans (USDHHS 2008; see the highlight box2018 Physical Activity Guidelines for Americans). These guidelines, updated in 2018, are based on comprehensive scientific summaries to detail the best science-based recommendation for the weekly amount of physical activity necessary to prevent disease and promote positive health outcomes (USDHHS 2018). The physical activity guidelines were developed for children and adolescents, adults, and older adults. These guidelines should be used as targets for physical activity participation.
Several other countries, as well as the World Health Organization, have published guidelines similar to the Physical Activity Guidelines for Americans. Japan, Canada, Australia, and England have all taken leadership roles in establishing physical activity as a public health priority by setting physical activity guidelines and recommendations.
Promoting Physical Activity for Health
As the field of physical activity and public health has emerged, it has become clear that many factors at many levels influence physical activity behaviors. Many investigators have used the social ecological model as a guiding framework to explain these multiple levels. They are illustrated in figure 3.6 and form the basis for the third section of this textbook.
Figure 3.6 Multiple levels of influence on physical activity behaviors: The social ecological model.
At the center of the target in the social ecological model for physical activity behaviors are individual factors. These are the factors that are innate to each person and that differ among people. A person's genetic makeup, early life experiences (e.g., youth sport participation), self-efficacy, and other factors, such as sex, disability, growth and development, and socioeconomic status, may all be important determinants of health behaviors such as physical activity.
Moving out from the center, social influences on physical activity are important. Research has now shown that individual factors are not enough to explain physical activity behavior. Determinants at the social influences level aren't characteristics of the person per se, but are, rather, characteristics of how the person interacts with society or culture. Influences at this level can include peers, medical care organizations (doctors), family members, and organizations (schools, places of worship, worksites).
The third level in the social ecological model represents environmental influences. These influences may enhance or restrict physical activity behaviors, and are external to the person but common across societies and cultures. Research on the effects of physical environment on physical activity participation has exploded as the field of physical activity and public health has emerged. The ability to influence the physical activity of vast numbers of people (instead of one person at a time) by making a single change makes environmental influences on physical activity a particularly interesting area of research. The availability of places to be active, such as trails, sidewalks, fitness facilities, bicycle lanes, community and neighborhood design elements are examples of how the built environment can influence physical activity.
Finally, the outer level represents policy influences on physical activity. Influences in this sphere include written or unwritten rules, codes, and norms that influence environmental or social determinants of physical activity. As with the physical environment, determinants at this level are particularly attractive because of their potential to influence many people. Examples of policy influences on physical activity include policies allowing increased access to places to be physically active (making it easier to be physically active), educational policies (e.g., mandating high-quality daily physical education for schoolchildren), and transportation-related policies (e.g., making it easier to walk or bicycle for transportation).
By combining knowledge, skills, and abilities related to the basic exercise sciences and public health, you can better explain and discuss professionally the health benefits and risks of exercise and physical activity to your peers, colleagues, and the communities you serve (see part II, chapters 5 through 10). An understanding of the specific challenges that affect physical activity and exercise in professional exercise science jobs can clarify how the exercise sciences affect public health, and vice versa. The highlight box Careers Combining Exercise Science and Public Health lists careers in exercise physiology, biomechanics, and sport and exercise psychology that are commonly seen in the professional areas of health and fitness, preventive medicine, athletic performance, and rehabilitation.
Physical activity guidelines for a healthy weight
For many adults, obesity is associated with significant increases in abdominal fat that increase the risk for metabolic syndrome and type 2 diabetes (see chapter 5). Regular participation in aerobic physical activity and exercise can decrease total body fat and abdominal fat, and these changes are consistent with improved metabolic function. Generally, the greater the volume of physical activity or exercise acquired by individuals or populations, the greater the reductions in body and abdominal fat.
For children and adolescents, the prevention of excessive weight gain during maturation is critical to prevent obesity and overweight in adulthood. Unfortunately, recent public health surveys note that the parents of many at-risk children are not aware of the problem or do not recognize that their children are overweight. Recent U.S. national policy statements targeting pediatricians and other health care providers assert that children and adolescents who are overweight or obese in their early teens should be identified as early as possible and given some sort of weight management plan through the intervention of parents, teachers, coaches, and family physicians.
One of the most obvious influences on weight management is how people perceive their ideal weight or physique. Research findings indicate a great disparity between reasonable weight loss or weight gain goals and people's “dream weight.” Even though some people may not reach their goal weight, they will likely report positive physical, social, and psychological benefits from any weight loss. The following scientific evidence and guidelines can help individuals and populations establish realistic goals for weight management (e.g., achieving a healthy weight) and meet their specific needs (e.g., weight loss, weight stability, prevention of weight regain, or loss of excessive abdominal fat) through regular participation in physical activity and exercise.
Scientific Evidence
The 2008 PAGAC noted physical activity (150 minutes per week to ≥300 minutes per week) was associated with modest weight loss, prevention of weight gain following weight loss, and reductions in total and regional adiposity. Evidence that resistance training helped with weight maintenance was not as strong, given that resistance training increases lean muscle mass, and the volume of resistance training regimes was usually less than that for aerobic training.
The 2018 PAGAC expanded the review of the evidence available in 2008, and focused on weight maintenance and weight gain within normal BMI limits (18.5 to < 25 kg/m2) for adults in relation to participating in 150 minutes per week or more of physical activity. The 2018 report also reviewed the impact of sedentary behavior and sedentary activity in relationship to physical activity and weight status. The specific 2018 PAGAC findings regarding weight gain were:
- Strong evidence demonstrates that the significant relationship between greater time spent in physical activity (≥300 minutes per week) and attenuated weight gain in adults is observed with moderate-to-vigorous physical activity.
- Moderate evidence indicates that the relationship between greater amounts of physical activity and attenuated weight gain in adults does not appear to vary by sex.
- Limited evidence suggests a dose-response relationship between physical activity and the risk of weight gain in adults, with greater amounts of physical activity (150 minutes per week) associated with lower risk of weight gain.
- Limited evidence suggests that the relationship between greater amounts of physical activity and attenuated weight gain in adults varies by age, with the effect diminishing with increasing age. The evidence from studies of older adults, however, is inconsistent.
- Insufficient evidence is available to determine whether the relationship between greater amounts of physical activity and attenuated weight gain in adults varies by race and ethnicity.
- Insufficient evidence is available to determine whether the relationship between greater amounts of physical activity and attenuated weight gain in adults varies by socioeconomic status.
- Insufficient evidence is available to determine whether the relationship between greater amounts of physical activity and attenuated weight gain in adults varies by initial weight status.
- Insufficient evidence is available to determine an association between light-intensity activity and attenuated weight gain in adults.
The 2018 PAGAC concluded the following with regard to the impact of sedentary behavior and sedentary activity for adults in relationship to physical activity and weight status:
- Limited evidence suggests a positive relationship between greater time spent in sedentary behavior and higher levels of adiposity and indicators of weight status.
- Limited evidence suggests the existence of a direct, graded dose-response relationship between greater sedentary behavior and higher levels of adiposity and indicators of weight status.
- Insufficient evidence is available to determine whether the relationship between sedentary behavior and weight status varies by age, sex, ethnicity, socioeconomic status, or baseline weight status.
- Insufficient evidence is available to determine whether the relationship between sedentary behavior and weight status varies by amount of moderate-to-vigorous physical activity.
- Insufficient evidence is available to determine whether bouts or breaks in sedentary behavior are important factors in the relationship between sedentary behavior and weight status.
As mentioned earlier in the chapter, regular physical activity and exercise are also important to prevent and control obesity and overweight in children and adolescents. The 2008 PAGAC found strong evidence demonstrating that higher levels of physical activity were associated with multiple beneficial health outcomes, including cardiorespiratory and muscular fitness, bone health, and maintenance of healthy weight status in children and adolescents (ages 6-19). The 2018 PAGAC focused on expanding the review of literature since 2008 with the addition of studies on children 3-6 years of age. The additional scientific recommendations of the 2018 PAGAC for youth were as follows:
- Strong evidence demonstrates that higher amounts of physical activity are associated with a reduced risk of excessive increases in body weight and adiposity in children ages 3 to 6 years.
- Limited evidence suggests that greater time spent in sedentary behavior is related to higher weight status or adiposity in children and adolescents; the evidence is somewhat stronger for television viewing or screen time than for total sedentary time.
- Insufficient evidence is available to determine whether the relationship between physical activity and health effects in children younger than 6 years of age is moderated by age, sex, race, ethnicity, weight status, or socioeconomic status.
Community-scale or macro-environmental urban design
Community-scale or macro-environmental urban design strategies for promoting physical activity involve changes and enhancements to the built environment of urban areas of several square miles (or kilometers) or larger, which are usually defined as being an administrative unit (zip code, neighborhood, school district, city, or county). These kinds of approaches strive to make entire communities more amenable to physical activity, whether that activity is transportation-related or exercise performed in discretionary time. Strategies at this level of influence include connecting transportation arteries; creating landscaping and lighting to enhance the aesthetics and perceived safety of the entire community; building a large-scale and interconnected network of sidewalks, bicycle lanes, and trails; and designing new mixed-use residential areas so that destinations such as workplaces, schools, and areas for leisure and recreation are within safe walking or bicycling distances.
One important and unique macro-environmental urban design element is road connectivity. The concept of connectivity refers to the ease of getting from one place to another within a neighborhood using the city's road network to walk or bike. If city thoroughfares follow a grid pattern, it is easy to use the street network (assuming sidewalks or bicycle lanes are available) to move around on foot or on bicycle; however, if intersections are very far from each other or there are quite a few dead-end streets or culs-de-sac, connectivity is considered to be sub-optimal. Another related construct for the macro-environment that has emerged in the past couple of decades is walkability. Walkability refers to the conduciveness of walking for transportation based on features of the built environment of an urban area. Many researchers have proposed different definitions of walkability, using scores or indices. Some of these scores are even used by real-estate companies to provide their clients with information about potential neighborhoods. High walkability scores or indices could indicate the best mix of built environment elements, and if optimized, could point to a neighborhood that is very easy to navigate on foot. Likewise, neighborhoods with low walkability scores are those with suboptimal conditions for transport-based walking. Most available walkability scores or indices include measures of connectivity, land-use mix, and residential density, which are three critical components for optimal urban design that promote walking for transportation in an area. Although this definition for walkability is valid in many parts of the world, it is not applicable in others (e.g., Mexico or China) (Salvo et al. 2014; Lu et al. 2017). Therefore, it is always important to consider the local context, including the social environment (social norms and cultural values), when trying to promote walkable environments because these may look different in other parts of the world.
Studies examining community-scale changes for physical activity promotion have used a wide variety of outcome measures (Heath et al. 2006). Some have studied the absolute number of walking trips in a community over a given time period; others, the distance of those trips, minutes of walking per week, and number of pedestrians in a certain area. Although these outcomes are not entirely comparable, the general interpretation is that making the built environment more activity-friendly can improve levels of physical activity (regardless of how it is measured) by an average of more than 160%. Clearly, this is a major influence on physical activity habits in a community.
Development of health guidelines
The development of health guidelines is a third critical function of public health science. Public health guidelines are official policy statements, usually developed by a government body, agency, or other reputable organization, that are based on the best available science. Public health guidelines provide clear recommendations about a course of action to deal with a pressing public health issue. Recommendations for childhood immunization schedules (when and which vaccines and their timing), diabetes treatment (the frequency and method of glucose self-monitoring), nutrient intake (micronutrient daily recommended intakes for health), and annual influenza vaccinations (type and timing) are all examples of public health guidelines that, based on the best available science, give health professionals and the public clear guidance about the most appropriate courses of action for preventing and treating certain health problems.
In 2008, the U.S. Department of Health and Human Services published the first Physical Activity Guidelines for Americans (USDHHS 2008; see the highlight box2018 Physical Activity Guidelines for Americans). These guidelines, updated in 2018, are based on comprehensive scientific summaries to detail the best science-based recommendation for the weekly amount of physical activity necessary to prevent disease and promote positive health outcomes (USDHHS 2018). The physical activity guidelines were developed for children and adolescents, adults, and older adults. These guidelines should be used as targets for physical activity participation.
Several other countries, as well as the World Health Organization, have published guidelines similar to the Physical Activity Guidelines for Americans. Japan, Canada, Australia, and England have all taken leadership roles in establishing physical activity as a public health priority by setting physical activity guidelines and recommendations.
Promoting Physical Activity for Health
As the field of physical activity and public health has emerged, it has become clear that many factors at many levels influence physical activity behaviors. Many investigators have used the social ecological model as a guiding framework to explain these multiple levels. They are illustrated in figure 3.6 and form the basis for the third section of this textbook.
Figure 3.6 Multiple levels of influence on physical activity behaviors: The social ecological model.
At the center of the target in the social ecological model for physical activity behaviors are individual factors. These are the factors that are innate to each person and that differ among people. A person's genetic makeup, early life experiences (e.g., youth sport participation), self-efficacy, and other factors, such as sex, disability, growth and development, and socioeconomic status, may all be important determinants of health behaviors such as physical activity.
Moving out from the center, social influences on physical activity are important. Research has now shown that individual factors are not enough to explain physical activity behavior. Determinants at the social influences level aren't characteristics of the person per se, but are, rather, characteristics of how the person interacts with society or culture. Influences at this level can include peers, medical care organizations (doctors), family members, and organizations (schools, places of worship, worksites).
The third level in the social ecological model represents environmental influences. These influences may enhance or restrict physical activity behaviors, and are external to the person but common across societies and cultures. Research on the effects of physical environment on physical activity participation has exploded as the field of physical activity and public health has emerged. The ability to influence the physical activity of vast numbers of people (instead of one person at a time) by making a single change makes environmental influences on physical activity a particularly interesting area of research. The availability of places to be active, such as trails, sidewalks, fitness facilities, bicycle lanes, community and neighborhood design elements are examples of how the built environment can influence physical activity.
Finally, the outer level represents policy influences on physical activity. Influences in this sphere include written or unwritten rules, codes, and norms that influence environmental or social determinants of physical activity. As with the physical environment, determinants at this level are particularly attractive because of their potential to influence many people. Examples of policy influences on physical activity include policies allowing increased access to places to be physically active (making it easier to be physically active), educational policies (e.g., mandating high-quality daily physical education for schoolchildren), and transportation-related policies (e.g., making it easier to walk or bicycle for transportation).
By combining knowledge, skills, and abilities related to the basic exercise sciences and public health, you can better explain and discuss professionally the health benefits and risks of exercise and physical activity to your peers, colleagues, and the communities you serve (see part II, chapters 5 through 10). An understanding of the specific challenges that affect physical activity and exercise in professional exercise science jobs can clarify how the exercise sciences affect public health, and vice versa. The highlight box Careers Combining Exercise Science and Public Health lists careers in exercise physiology, biomechanics, and sport and exercise psychology that are commonly seen in the professional areas of health and fitness, preventive medicine, athletic performance, and rehabilitation.
Physical activity guidelines for a healthy weight
For many adults, obesity is associated with significant increases in abdominal fat that increase the risk for metabolic syndrome and type 2 diabetes (see chapter 5). Regular participation in aerobic physical activity and exercise can decrease total body fat and abdominal fat, and these changes are consistent with improved metabolic function. Generally, the greater the volume of physical activity or exercise acquired by individuals or populations, the greater the reductions in body and abdominal fat.
For children and adolescents, the prevention of excessive weight gain during maturation is critical to prevent obesity and overweight in adulthood. Unfortunately, recent public health surveys note that the parents of many at-risk children are not aware of the problem or do not recognize that their children are overweight. Recent U.S. national policy statements targeting pediatricians and other health care providers assert that children and adolescents who are overweight or obese in their early teens should be identified as early as possible and given some sort of weight management plan through the intervention of parents, teachers, coaches, and family physicians.
One of the most obvious influences on weight management is how people perceive their ideal weight or physique. Research findings indicate a great disparity between reasonable weight loss or weight gain goals and people's “dream weight.” Even though some people may not reach their goal weight, they will likely report positive physical, social, and psychological benefits from any weight loss. The following scientific evidence and guidelines can help individuals and populations establish realistic goals for weight management (e.g., achieving a healthy weight) and meet their specific needs (e.g., weight loss, weight stability, prevention of weight regain, or loss of excessive abdominal fat) through regular participation in physical activity and exercise.
Scientific Evidence
The 2008 PAGAC noted physical activity (150 minutes per week to ≥300 minutes per week) was associated with modest weight loss, prevention of weight gain following weight loss, and reductions in total and regional adiposity. Evidence that resistance training helped with weight maintenance was not as strong, given that resistance training increases lean muscle mass, and the volume of resistance training regimes was usually less than that for aerobic training.
The 2018 PAGAC expanded the review of the evidence available in 2008, and focused on weight maintenance and weight gain within normal BMI limits (18.5 to < 25 kg/m2) for adults in relation to participating in 150 minutes per week or more of physical activity. The 2018 report also reviewed the impact of sedentary behavior and sedentary activity in relationship to physical activity and weight status. The specific 2018 PAGAC findings regarding weight gain were:
- Strong evidence demonstrates that the significant relationship between greater time spent in physical activity (≥300 minutes per week) and attenuated weight gain in adults is observed with moderate-to-vigorous physical activity.
- Moderate evidence indicates that the relationship between greater amounts of physical activity and attenuated weight gain in adults does not appear to vary by sex.
- Limited evidence suggests a dose-response relationship between physical activity and the risk of weight gain in adults, with greater amounts of physical activity (150 minutes per week) associated with lower risk of weight gain.
- Limited evidence suggests that the relationship between greater amounts of physical activity and attenuated weight gain in adults varies by age, with the effect diminishing with increasing age. The evidence from studies of older adults, however, is inconsistent.
- Insufficient evidence is available to determine whether the relationship between greater amounts of physical activity and attenuated weight gain in adults varies by race and ethnicity.
- Insufficient evidence is available to determine whether the relationship between greater amounts of physical activity and attenuated weight gain in adults varies by socioeconomic status.
- Insufficient evidence is available to determine whether the relationship between greater amounts of physical activity and attenuated weight gain in adults varies by initial weight status.
- Insufficient evidence is available to determine an association between light-intensity activity and attenuated weight gain in adults.
The 2018 PAGAC concluded the following with regard to the impact of sedentary behavior and sedentary activity for adults in relationship to physical activity and weight status:
- Limited evidence suggests a positive relationship between greater time spent in sedentary behavior and higher levels of adiposity and indicators of weight status.
- Limited evidence suggests the existence of a direct, graded dose-response relationship between greater sedentary behavior and higher levels of adiposity and indicators of weight status.
- Insufficient evidence is available to determine whether the relationship between sedentary behavior and weight status varies by age, sex, ethnicity, socioeconomic status, or baseline weight status.
- Insufficient evidence is available to determine whether the relationship between sedentary behavior and weight status varies by amount of moderate-to-vigorous physical activity.
- Insufficient evidence is available to determine whether bouts or breaks in sedentary behavior are important factors in the relationship between sedentary behavior and weight status.
As mentioned earlier in the chapter, regular physical activity and exercise are also important to prevent and control obesity and overweight in children and adolescents. The 2008 PAGAC found strong evidence demonstrating that higher levels of physical activity were associated with multiple beneficial health outcomes, including cardiorespiratory and muscular fitness, bone health, and maintenance of healthy weight status in children and adolescents (ages 6-19). The 2018 PAGAC focused on expanding the review of literature since 2008 with the addition of studies on children 3-6 years of age. The additional scientific recommendations of the 2018 PAGAC for youth were as follows:
- Strong evidence demonstrates that higher amounts of physical activity are associated with a reduced risk of excessive increases in body weight and adiposity in children ages 3 to 6 years.
- Limited evidence suggests that greater time spent in sedentary behavior is related to higher weight status or adiposity in children and adolescents; the evidence is somewhat stronger for television viewing or screen time than for total sedentary time.
- Insufficient evidence is available to determine whether the relationship between physical activity and health effects in children younger than 6 years of age is moderated by age, sex, race, ethnicity, weight status, or socioeconomic status.
Community-scale or macro-environmental urban design
Community-scale or macro-environmental urban design strategies for promoting physical activity involve changes and enhancements to the built environment of urban areas of several square miles (or kilometers) or larger, which are usually defined as being an administrative unit (zip code, neighborhood, school district, city, or county). These kinds of approaches strive to make entire communities more amenable to physical activity, whether that activity is transportation-related or exercise performed in discretionary time. Strategies at this level of influence include connecting transportation arteries; creating landscaping and lighting to enhance the aesthetics and perceived safety of the entire community; building a large-scale and interconnected network of sidewalks, bicycle lanes, and trails; and designing new mixed-use residential areas so that destinations such as workplaces, schools, and areas for leisure and recreation are within safe walking or bicycling distances.
One important and unique macro-environmental urban design element is road connectivity. The concept of connectivity refers to the ease of getting from one place to another within a neighborhood using the city's road network to walk or bike. If city thoroughfares follow a grid pattern, it is easy to use the street network (assuming sidewalks or bicycle lanes are available) to move around on foot or on bicycle; however, if intersections are very far from each other or there are quite a few dead-end streets or culs-de-sac, connectivity is considered to be sub-optimal. Another related construct for the macro-environment that has emerged in the past couple of decades is walkability. Walkability refers to the conduciveness of walking for transportation based on features of the built environment of an urban area. Many researchers have proposed different definitions of walkability, using scores or indices. Some of these scores are even used by real-estate companies to provide their clients with information about potential neighborhoods. High walkability scores or indices could indicate the best mix of built environment elements, and if optimized, could point to a neighborhood that is very easy to navigate on foot. Likewise, neighborhoods with low walkability scores are those with suboptimal conditions for transport-based walking. Most available walkability scores or indices include measures of connectivity, land-use mix, and residential density, which are three critical components for optimal urban design that promote walking for transportation in an area. Although this definition for walkability is valid in many parts of the world, it is not applicable in others (e.g., Mexico or China) (Salvo et al. 2014; Lu et al. 2017). Therefore, it is always important to consider the local context, including the social environment (social norms and cultural values), when trying to promote walkable environments because these may look different in other parts of the world.
Studies examining community-scale changes for physical activity promotion have used a wide variety of outcome measures (Heath et al. 2006). Some have studied the absolute number of walking trips in a community over a given time period; others, the distance of those trips, minutes of walking per week, and number of pedestrians in a certain area. Although these outcomes are not entirely comparable, the general interpretation is that making the built environment more activity-friendly can improve levels of physical activity (regardless of how it is measured) by an average of more than 160%. Clearly, this is a major influence on physical activity habits in a community.
Development of health guidelines
The development of health guidelines is a third critical function of public health science. Public health guidelines are official policy statements, usually developed by a government body, agency, or other reputable organization, that are based on the best available science. Public health guidelines provide clear recommendations about a course of action to deal with a pressing public health issue. Recommendations for childhood immunization schedules (when and which vaccines and their timing), diabetes treatment (the frequency and method of glucose self-monitoring), nutrient intake (micronutrient daily recommended intakes for health), and annual influenza vaccinations (type and timing) are all examples of public health guidelines that, based on the best available science, give health professionals and the public clear guidance about the most appropriate courses of action for preventing and treating certain health problems.
In 2008, the U.S. Department of Health and Human Services published the first Physical Activity Guidelines for Americans (USDHHS 2008; see the highlight box2018 Physical Activity Guidelines for Americans). These guidelines, updated in 2018, are based on comprehensive scientific summaries to detail the best science-based recommendation for the weekly amount of physical activity necessary to prevent disease and promote positive health outcomes (USDHHS 2018). The physical activity guidelines were developed for children and adolescents, adults, and older adults. These guidelines should be used as targets for physical activity participation.
Several other countries, as well as the World Health Organization, have published guidelines similar to the Physical Activity Guidelines for Americans. Japan, Canada, Australia, and England have all taken leadership roles in establishing physical activity as a public health priority by setting physical activity guidelines and recommendations.
Promoting Physical Activity for Health
As the field of physical activity and public health has emerged, it has become clear that many factors at many levels influence physical activity behaviors. Many investigators have used the social ecological model as a guiding framework to explain these multiple levels. They are illustrated in figure 3.6 and form the basis for the third section of this textbook.
Figure 3.6 Multiple levels of influence on physical activity behaviors: The social ecological model.
At the center of the target in the social ecological model for physical activity behaviors are individual factors. These are the factors that are innate to each person and that differ among people. A person's genetic makeup, early life experiences (e.g., youth sport participation), self-efficacy, and other factors, such as sex, disability, growth and development, and socioeconomic status, may all be important determinants of health behaviors such as physical activity.
Moving out from the center, social influences on physical activity are important. Research has now shown that individual factors are not enough to explain physical activity behavior. Determinants at the social influences level aren't characteristics of the person per se, but are, rather, characteristics of how the person interacts with society or culture. Influences at this level can include peers, medical care organizations (doctors), family members, and organizations (schools, places of worship, worksites).
The third level in the social ecological model represents environmental influences. These influences may enhance or restrict physical activity behaviors, and are external to the person but common across societies and cultures. Research on the effects of physical environment on physical activity participation has exploded as the field of physical activity and public health has emerged. The ability to influence the physical activity of vast numbers of people (instead of one person at a time) by making a single change makes environmental influences on physical activity a particularly interesting area of research. The availability of places to be active, such as trails, sidewalks, fitness facilities, bicycle lanes, community and neighborhood design elements are examples of how the built environment can influence physical activity.
Finally, the outer level represents policy influences on physical activity. Influences in this sphere include written or unwritten rules, codes, and norms that influence environmental or social determinants of physical activity. As with the physical environment, determinants at this level are particularly attractive because of their potential to influence many people. Examples of policy influences on physical activity include policies allowing increased access to places to be physically active (making it easier to be physically active), educational policies (e.g., mandating high-quality daily physical education for schoolchildren), and transportation-related policies (e.g., making it easier to walk or bicycle for transportation).
By combining knowledge, skills, and abilities related to the basic exercise sciences and public health, you can better explain and discuss professionally the health benefits and risks of exercise and physical activity to your peers, colleagues, and the communities you serve (see part II, chapters 5 through 10). An understanding of the specific challenges that affect physical activity and exercise in professional exercise science jobs can clarify how the exercise sciences affect public health, and vice versa. The highlight box Careers Combining Exercise Science and Public Health lists careers in exercise physiology, biomechanics, and sport and exercise psychology that are commonly seen in the professional areas of health and fitness, preventive medicine, athletic performance, and rehabilitation.
Physical activity guidelines for a healthy weight
For many adults, obesity is associated with significant increases in abdominal fat that increase the risk for metabolic syndrome and type 2 diabetes (see chapter 5). Regular participation in aerobic physical activity and exercise can decrease total body fat and abdominal fat, and these changes are consistent with improved metabolic function. Generally, the greater the volume of physical activity or exercise acquired by individuals or populations, the greater the reductions in body and abdominal fat.
For children and adolescents, the prevention of excessive weight gain during maturation is critical to prevent obesity and overweight in adulthood. Unfortunately, recent public health surveys note that the parents of many at-risk children are not aware of the problem or do not recognize that their children are overweight. Recent U.S. national policy statements targeting pediatricians and other health care providers assert that children and adolescents who are overweight or obese in their early teens should be identified as early as possible and given some sort of weight management plan through the intervention of parents, teachers, coaches, and family physicians.
One of the most obvious influences on weight management is how people perceive their ideal weight or physique. Research findings indicate a great disparity between reasonable weight loss or weight gain goals and people's “dream weight.” Even though some people may not reach their goal weight, they will likely report positive physical, social, and psychological benefits from any weight loss. The following scientific evidence and guidelines can help individuals and populations establish realistic goals for weight management (e.g., achieving a healthy weight) and meet their specific needs (e.g., weight loss, weight stability, prevention of weight regain, or loss of excessive abdominal fat) through regular participation in physical activity and exercise.
Scientific Evidence
The 2008 PAGAC noted physical activity (150 minutes per week to ≥300 minutes per week) was associated with modest weight loss, prevention of weight gain following weight loss, and reductions in total and regional adiposity. Evidence that resistance training helped with weight maintenance was not as strong, given that resistance training increases lean muscle mass, and the volume of resistance training regimes was usually less than that for aerobic training.
The 2018 PAGAC expanded the review of the evidence available in 2008, and focused on weight maintenance and weight gain within normal BMI limits (18.5 to < 25 kg/m2) for adults in relation to participating in 150 minutes per week or more of physical activity. The 2018 report also reviewed the impact of sedentary behavior and sedentary activity in relationship to physical activity and weight status. The specific 2018 PAGAC findings regarding weight gain were:
- Strong evidence demonstrates that the significant relationship between greater time spent in physical activity (≥300 minutes per week) and attenuated weight gain in adults is observed with moderate-to-vigorous physical activity.
- Moderate evidence indicates that the relationship between greater amounts of physical activity and attenuated weight gain in adults does not appear to vary by sex.
- Limited evidence suggests a dose-response relationship between physical activity and the risk of weight gain in adults, with greater amounts of physical activity (150 minutes per week) associated with lower risk of weight gain.
- Limited evidence suggests that the relationship between greater amounts of physical activity and attenuated weight gain in adults varies by age, with the effect diminishing with increasing age. The evidence from studies of older adults, however, is inconsistent.
- Insufficient evidence is available to determine whether the relationship between greater amounts of physical activity and attenuated weight gain in adults varies by race and ethnicity.
- Insufficient evidence is available to determine whether the relationship between greater amounts of physical activity and attenuated weight gain in adults varies by socioeconomic status.
- Insufficient evidence is available to determine whether the relationship between greater amounts of physical activity and attenuated weight gain in adults varies by initial weight status.
- Insufficient evidence is available to determine an association between light-intensity activity and attenuated weight gain in adults.
The 2018 PAGAC concluded the following with regard to the impact of sedentary behavior and sedentary activity for adults in relationship to physical activity and weight status:
- Limited evidence suggests a positive relationship between greater time spent in sedentary behavior and higher levels of adiposity and indicators of weight status.
- Limited evidence suggests the existence of a direct, graded dose-response relationship between greater sedentary behavior and higher levels of adiposity and indicators of weight status.
- Insufficient evidence is available to determine whether the relationship between sedentary behavior and weight status varies by age, sex, ethnicity, socioeconomic status, or baseline weight status.
- Insufficient evidence is available to determine whether the relationship between sedentary behavior and weight status varies by amount of moderate-to-vigorous physical activity.
- Insufficient evidence is available to determine whether bouts or breaks in sedentary behavior are important factors in the relationship between sedentary behavior and weight status.
As mentioned earlier in the chapter, regular physical activity and exercise are also important to prevent and control obesity and overweight in children and adolescents. The 2008 PAGAC found strong evidence demonstrating that higher levels of physical activity were associated with multiple beneficial health outcomes, including cardiorespiratory and muscular fitness, bone health, and maintenance of healthy weight status in children and adolescents (ages 6-19). The 2018 PAGAC focused on expanding the review of literature since 2008 with the addition of studies on children 3-6 years of age. The additional scientific recommendations of the 2018 PAGAC for youth were as follows:
- Strong evidence demonstrates that higher amounts of physical activity are associated with a reduced risk of excessive increases in body weight and adiposity in children ages 3 to 6 years.
- Limited evidence suggests that greater time spent in sedentary behavior is related to higher weight status or adiposity in children and adolescents; the evidence is somewhat stronger for television viewing or screen time than for total sedentary time.
- Insufficient evidence is available to determine whether the relationship between physical activity and health effects in children younger than 6 years of age is moderated by age, sex, race, ethnicity, weight status, or socioeconomic status.
Community-scale or macro-environmental urban design
Community-scale or macro-environmental urban design strategies for promoting physical activity involve changes and enhancements to the built environment of urban areas of several square miles (or kilometers) or larger, which are usually defined as being an administrative unit (zip code, neighborhood, school district, city, or county). These kinds of approaches strive to make entire communities more amenable to physical activity, whether that activity is transportation-related or exercise performed in discretionary time. Strategies at this level of influence include connecting transportation arteries; creating landscaping and lighting to enhance the aesthetics and perceived safety of the entire community; building a large-scale and interconnected network of sidewalks, bicycle lanes, and trails; and designing new mixed-use residential areas so that destinations such as workplaces, schools, and areas for leisure and recreation are within safe walking or bicycling distances.
One important and unique macro-environmental urban design element is road connectivity. The concept of connectivity refers to the ease of getting from one place to another within a neighborhood using the city's road network to walk or bike. If city thoroughfares follow a grid pattern, it is easy to use the street network (assuming sidewalks or bicycle lanes are available) to move around on foot or on bicycle; however, if intersections are very far from each other or there are quite a few dead-end streets or culs-de-sac, connectivity is considered to be sub-optimal. Another related construct for the macro-environment that has emerged in the past couple of decades is walkability. Walkability refers to the conduciveness of walking for transportation based on features of the built environment of an urban area. Many researchers have proposed different definitions of walkability, using scores or indices. Some of these scores are even used by real-estate companies to provide their clients with information about potential neighborhoods. High walkability scores or indices could indicate the best mix of built environment elements, and if optimized, could point to a neighborhood that is very easy to navigate on foot. Likewise, neighborhoods with low walkability scores are those with suboptimal conditions for transport-based walking. Most available walkability scores or indices include measures of connectivity, land-use mix, and residential density, which are three critical components for optimal urban design that promote walking for transportation in an area. Although this definition for walkability is valid in many parts of the world, it is not applicable in others (e.g., Mexico or China) (Salvo et al. 2014; Lu et al. 2017). Therefore, it is always important to consider the local context, including the social environment (social norms and cultural values), when trying to promote walkable environments because these may look different in other parts of the world.
Studies examining community-scale changes for physical activity promotion have used a wide variety of outcome measures (Heath et al. 2006). Some have studied the absolute number of walking trips in a community over a given time period; others, the distance of those trips, minutes of walking per week, and number of pedestrians in a certain area. Although these outcomes are not entirely comparable, the general interpretation is that making the built environment more activity-friendly can improve levels of physical activity (regardless of how it is measured) by an average of more than 160%. Clearly, this is a major influence on physical activity habits in a community.
Development of health guidelines
The development of health guidelines is a third critical function of public health science. Public health guidelines are official policy statements, usually developed by a government body, agency, or other reputable organization, that are based on the best available science. Public health guidelines provide clear recommendations about a course of action to deal with a pressing public health issue. Recommendations for childhood immunization schedules (when and which vaccines and their timing), diabetes treatment (the frequency and method of glucose self-monitoring), nutrient intake (micronutrient daily recommended intakes for health), and annual influenza vaccinations (type and timing) are all examples of public health guidelines that, based on the best available science, give health professionals and the public clear guidance about the most appropriate courses of action for preventing and treating certain health problems.
In 2008, the U.S. Department of Health and Human Services published the first Physical Activity Guidelines for Americans (USDHHS 2008; see the highlight box2018 Physical Activity Guidelines for Americans). These guidelines, updated in 2018, are based on comprehensive scientific summaries to detail the best science-based recommendation for the weekly amount of physical activity necessary to prevent disease and promote positive health outcomes (USDHHS 2018). The physical activity guidelines were developed for children and adolescents, adults, and older adults. These guidelines should be used as targets for physical activity participation.
Several other countries, as well as the World Health Organization, have published guidelines similar to the Physical Activity Guidelines for Americans. Japan, Canada, Australia, and England have all taken leadership roles in establishing physical activity as a public health priority by setting physical activity guidelines and recommendations.
Promoting Physical Activity for Health
As the field of physical activity and public health has emerged, it has become clear that many factors at many levels influence physical activity behaviors. Many investigators have used the social ecological model as a guiding framework to explain these multiple levels. They are illustrated in figure 3.6 and form the basis for the third section of this textbook.
Figure 3.6 Multiple levels of influence on physical activity behaviors: The social ecological model.
At the center of the target in the social ecological model for physical activity behaviors are individual factors. These are the factors that are innate to each person and that differ among people. A person's genetic makeup, early life experiences (e.g., youth sport participation), self-efficacy, and other factors, such as sex, disability, growth and development, and socioeconomic status, may all be important determinants of health behaviors such as physical activity.
Moving out from the center, social influences on physical activity are important. Research has now shown that individual factors are not enough to explain physical activity behavior. Determinants at the social influences level aren't characteristics of the person per se, but are, rather, characteristics of how the person interacts with society or culture. Influences at this level can include peers, medical care organizations (doctors), family members, and organizations (schools, places of worship, worksites).
The third level in the social ecological model represents environmental influences. These influences may enhance or restrict physical activity behaviors, and are external to the person but common across societies and cultures. Research on the effects of physical environment on physical activity participation has exploded as the field of physical activity and public health has emerged. The ability to influence the physical activity of vast numbers of people (instead of one person at a time) by making a single change makes environmental influences on physical activity a particularly interesting area of research. The availability of places to be active, such as trails, sidewalks, fitness facilities, bicycle lanes, community and neighborhood design elements are examples of how the built environment can influence physical activity.
Finally, the outer level represents policy influences on physical activity. Influences in this sphere include written or unwritten rules, codes, and norms that influence environmental or social determinants of physical activity. As with the physical environment, determinants at this level are particularly attractive because of their potential to influence many people. Examples of policy influences on physical activity include policies allowing increased access to places to be physically active (making it easier to be physically active), educational policies (e.g., mandating high-quality daily physical education for schoolchildren), and transportation-related policies (e.g., making it easier to walk or bicycle for transportation).
By combining knowledge, skills, and abilities related to the basic exercise sciences and public health, you can better explain and discuss professionally the health benefits and risks of exercise and physical activity to your peers, colleagues, and the communities you serve (see part II, chapters 5 through 10). An understanding of the specific challenges that affect physical activity and exercise in professional exercise science jobs can clarify how the exercise sciences affect public health, and vice versa. The highlight box Careers Combining Exercise Science and Public Health lists careers in exercise physiology, biomechanics, and sport and exercise psychology that are commonly seen in the professional areas of health and fitness, preventive medicine, athletic performance, and rehabilitation.
Physical activity guidelines for a healthy weight
For many adults, obesity is associated with significant increases in abdominal fat that increase the risk for metabolic syndrome and type 2 diabetes (see chapter 5). Regular participation in aerobic physical activity and exercise can decrease total body fat and abdominal fat, and these changes are consistent with improved metabolic function. Generally, the greater the volume of physical activity or exercise acquired by individuals or populations, the greater the reductions in body and abdominal fat.
For children and adolescents, the prevention of excessive weight gain during maturation is critical to prevent obesity and overweight in adulthood. Unfortunately, recent public health surveys note that the parents of many at-risk children are not aware of the problem or do not recognize that their children are overweight. Recent U.S. national policy statements targeting pediatricians and other health care providers assert that children and adolescents who are overweight or obese in their early teens should be identified as early as possible and given some sort of weight management plan through the intervention of parents, teachers, coaches, and family physicians.
One of the most obvious influences on weight management is how people perceive their ideal weight or physique. Research findings indicate a great disparity between reasonable weight loss or weight gain goals and people's “dream weight.” Even though some people may not reach their goal weight, they will likely report positive physical, social, and psychological benefits from any weight loss. The following scientific evidence and guidelines can help individuals and populations establish realistic goals for weight management (e.g., achieving a healthy weight) and meet their specific needs (e.g., weight loss, weight stability, prevention of weight regain, or loss of excessive abdominal fat) through regular participation in physical activity and exercise.
Scientific Evidence
The 2008 PAGAC noted physical activity (150 minutes per week to ≥300 minutes per week) was associated with modest weight loss, prevention of weight gain following weight loss, and reductions in total and regional adiposity. Evidence that resistance training helped with weight maintenance was not as strong, given that resistance training increases lean muscle mass, and the volume of resistance training regimes was usually less than that for aerobic training.
The 2018 PAGAC expanded the review of the evidence available in 2008, and focused on weight maintenance and weight gain within normal BMI limits (18.5 to < 25 kg/m2) for adults in relation to participating in 150 minutes per week or more of physical activity. The 2018 report also reviewed the impact of sedentary behavior and sedentary activity in relationship to physical activity and weight status. The specific 2018 PAGAC findings regarding weight gain were:
- Strong evidence demonstrates that the significant relationship between greater time spent in physical activity (≥300 minutes per week) and attenuated weight gain in adults is observed with moderate-to-vigorous physical activity.
- Moderate evidence indicates that the relationship between greater amounts of physical activity and attenuated weight gain in adults does not appear to vary by sex.
- Limited evidence suggests a dose-response relationship between physical activity and the risk of weight gain in adults, with greater amounts of physical activity (150 minutes per week) associated with lower risk of weight gain.
- Limited evidence suggests that the relationship between greater amounts of physical activity and attenuated weight gain in adults varies by age, with the effect diminishing with increasing age. The evidence from studies of older adults, however, is inconsistent.
- Insufficient evidence is available to determine whether the relationship between greater amounts of physical activity and attenuated weight gain in adults varies by race and ethnicity.
- Insufficient evidence is available to determine whether the relationship between greater amounts of physical activity and attenuated weight gain in adults varies by socioeconomic status.
- Insufficient evidence is available to determine whether the relationship between greater amounts of physical activity and attenuated weight gain in adults varies by initial weight status.
- Insufficient evidence is available to determine an association between light-intensity activity and attenuated weight gain in adults.
The 2018 PAGAC concluded the following with regard to the impact of sedentary behavior and sedentary activity for adults in relationship to physical activity and weight status:
- Limited evidence suggests a positive relationship between greater time spent in sedentary behavior and higher levels of adiposity and indicators of weight status.
- Limited evidence suggests the existence of a direct, graded dose-response relationship between greater sedentary behavior and higher levels of adiposity and indicators of weight status.
- Insufficient evidence is available to determine whether the relationship between sedentary behavior and weight status varies by age, sex, ethnicity, socioeconomic status, or baseline weight status.
- Insufficient evidence is available to determine whether the relationship between sedentary behavior and weight status varies by amount of moderate-to-vigorous physical activity.
- Insufficient evidence is available to determine whether bouts or breaks in sedentary behavior are important factors in the relationship between sedentary behavior and weight status.
As mentioned earlier in the chapter, regular physical activity and exercise are also important to prevent and control obesity and overweight in children and adolescents. The 2008 PAGAC found strong evidence demonstrating that higher levels of physical activity were associated with multiple beneficial health outcomes, including cardiorespiratory and muscular fitness, bone health, and maintenance of healthy weight status in children and adolescents (ages 6-19). The 2018 PAGAC focused on expanding the review of literature since 2008 with the addition of studies on children 3-6 years of age. The additional scientific recommendations of the 2018 PAGAC for youth were as follows:
- Strong evidence demonstrates that higher amounts of physical activity are associated with a reduced risk of excessive increases in body weight and adiposity in children ages 3 to 6 years.
- Limited evidence suggests that greater time spent in sedentary behavior is related to higher weight status or adiposity in children and adolescents; the evidence is somewhat stronger for television viewing or screen time than for total sedentary time.
- Insufficient evidence is available to determine whether the relationship between physical activity and health effects in children younger than 6 years of age is moderated by age, sex, race, ethnicity, weight status, or socioeconomic status.
Community-scale or macro-environmental urban design
Community-scale or macro-environmental urban design strategies for promoting physical activity involve changes and enhancements to the built environment of urban areas of several square miles (or kilometers) or larger, which are usually defined as being an administrative unit (zip code, neighborhood, school district, city, or county). These kinds of approaches strive to make entire communities more amenable to physical activity, whether that activity is transportation-related or exercise performed in discretionary time. Strategies at this level of influence include connecting transportation arteries; creating landscaping and lighting to enhance the aesthetics and perceived safety of the entire community; building a large-scale and interconnected network of sidewalks, bicycle lanes, and trails; and designing new mixed-use residential areas so that destinations such as workplaces, schools, and areas for leisure and recreation are within safe walking or bicycling distances.
One important and unique macro-environmental urban design element is road connectivity. The concept of connectivity refers to the ease of getting from one place to another within a neighborhood using the city's road network to walk or bike. If city thoroughfares follow a grid pattern, it is easy to use the street network (assuming sidewalks or bicycle lanes are available) to move around on foot or on bicycle; however, if intersections are very far from each other or there are quite a few dead-end streets or culs-de-sac, connectivity is considered to be sub-optimal. Another related construct for the macro-environment that has emerged in the past couple of decades is walkability. Walkability refers to the conduciveness of walking for transportation based on features of the built environment of an urban area. Many researchers have proposed different definitions of walkability, using scores or indices. Some of these scores are even used by real-estate companies to provide their clients with information about potential neighborhoods. High walkability scores or indices could indicate the best mix of built environment elements, and if optimized, could point to a neighborhood that is very easy to navigate on foot. Likewise, neighborhoods with low walkability scores are those with suboptimal conditions for transport-based walking. Most available walkability scores or indices include measures of connectivity, land-use mix, and residential density, which are three critical components for optimal urban design that promote walking for transportation in an area. Although this definition for walkability is valid in many parts of the world, it is not applicable in others (e.g., Mexico or China) (Salvo et al. 2014; Lu et al. 2017). Therefore, it is always important to consider the local context, including the social environment (social norms and cultural values), when trying to promote walkable environments because these may look different in other parts of the world.
Studies examining community-scale changes for physical activity promotion have used a wide variety of outcome measures (Heath et al. 2006). Some have studied the absolute number of walking trips in a community over a given time period; others, the distance of those trips, minutes of walking per week, and number of pedestrians in a certain area. Although these outcomes are not entirely comparable, the general interpretation is that making the built environment more activity-friendly can improve levels of physical activity (regardless of how it is measured) by an average of more than 160%. Clearly, this is a major influence on physical activity habits in a community.
Development of health guidelines
The development of health guidelines is a third critical function of public health science. Public health guidelines are official policy statements, usually developed by a government body, agency, or other reputable organization, that are based on the best available science. Public health guidelines provide clear recommendations about a course of action to deal with a pressing public health issue. Recommendations for childhood immunization schedules (when and which vaccines and their timing), diabetes treatment (the frequency and method of glucose self-monitoring), nutrient intake (micronutrient daily recommended intakes for health), and annual influenza vaccinations (type and timing) are all examples of public health guidelines that, based on the best available science, give health professionals and the public clear guidance about the most appropriate courses of action for preventing and treating certain health problems.
In 2008, the U.S. Department of Health and Human Services published the first Physical Activity Guidelines for Americans (USDHHS 2008; see the highlight box2018 Physical Activity Guidelines for Americans). These guidelines, updated in 2018, are based on comprehensive scientific summaries to detail the best science-based recommendation for the weekly amount of physical activity necessary to prevent disease and promote positive health outcomes (USDHHS 2018). The physical activity guidelines were developed for children and adolescents, adults, and older adults. These guidelines should be used as targets for physical activity participation.
Several other countries, as well as the World Health Organization, have published guidelines similar to the Physical Activity Guidelines for Americans. Japan, Canada, Australia, and England have all taken leadership roles in establishing physical activity as a public health priority by setting physical activity guidelines and recommendations.
Promoting Physical Activity for Health
As the field of physical activity and public health has emerged, it has become clear that many factors at many levels influence physical activity behaviors. Many investigators have used the social ecological model as a guiding framework to explain these multiple levels. They are illustrated in figure 3.6 and form the basis for the third section of this textbook.
Figure 3.6 Multiple levels of influence on physical activity behaviors: The social ecological model.
At the center of the target in the social ecological model for physical activity behaviors are individual factors. These are the factors that are innate to each person and that differ among people. A person's genetic makeup, early life experiences (e.g., youth sport participation), self-efficacy, and other factors, such as sex, disability, growth and development, and socioeconomic status, may all be important determinants of health behaviors such as physical activity.
Moving out from the center, social influences on physical activity are important. Research has now shown that individual factors are not enough to explain physical activity behavior. Determinants at the social influences level aren't characteristics of the person per se, but are, rather, characteristics of how the person interacts with society or culture. Influences at this level can include peers, medical care organizations (doctors), family members, and organizations (schools, places of worship, worksites).
The third level in the social ecological model represents environmental influences. These influences may enhance or restrict physical activity behaviors, and are external to the person but common across societies and cultures. Research on the effects of physical environment on physical activity participation has exploded as the field of physical activity and public health has emerged. The ability to influence the physical activity of vast numbers of people (instead of one person at a time) by making a single change makes environmental influences on physical activity a particularly interesting area of research. The availability of places to be active, such as trails, sidewalks, fitness facilities, bicycle lanes, community and neighborhood design elements are examples of how the built environment can influence physical activity.
Finally, the outer level represents policy influences on physical activity. Influences in this sphere include written or unwritten rules, codes, and norms that influence environmental or social determinants of physical activity. As with the physical environment, determinants at this level are particularly attractive because of their potential to influence many people. Examples of policy influences on physical activity include policies allowing increased access to places to be physically active (making it easier to be physically active), educational policies (e.g., mandating high-quality daily physical education for schoolchildren), and transportation-related policies (e.g., making it easier to walk or bicycle for transportation).
By combining knowledge, skills, and abilities related to the basic exercise sciences and public health, you can better explain and discuss professionally the health benefits and risks of exercise and physical activity to your peers, colleagues, and the communities you serve (see part II, chapters 5 through 10). An understanding of the specific challenges that affect physical activity and exercise in professional exercise science jobs can clarify how the exercise sciences affect public health, and vice versa. The highlight box Careers Combining Exercise Science and Public Health lists careers in exercise physiology, biomechanics, and sport and exercise psychology that are commonly seen in the professional areas of health and fitness, preventive medicine, athletic performance, and rehabilitation.
Physical activity guidelines for a healthy weight
For many adults, obesity is associated with significant increases in abdominal fat that increase the risk for metabolic syndrome and type 2 diabetes (see chapter 5). Regular participation in aerobic physical activity and exercise can decrease total body fat and abdominal fat, and these changes are consistent with improved metabolic function. Generally, the greater the volume of physical activity or exercise acquired by individuals or populations, the greater the reductions in body and abdominal fat.
For children and adolescents, the prevention of excessive weight gain during maturation is critical to prevent obesity and overweight in adulthood. Unfortunately, recent public health surveys note that the parents of many at-risk children are not aware of the problem or do not recognize that their children are overweight. Recent U.S. national policy statements targeting pediatricians and other health care providers assert that children and adolescents who are overweight or obese in their early teens should be identified as early as possible and given some sort of weight management plan through the intervention of parents, teachers, coaches, and family physicians.
One of the most obvious influences on weight management is how people perceive their ideal weight or physique. Research findings indicate a great disparity between reasonable weight loss or weight gain goals and people's “dream weight.” Even though some people may not reach their goal weight, they will likely report positive physical, social, and psychological benefits from any weight loss. The following scientific evidence and guidelines can help individuals and populations establish realistic goals for weight management (e.g., achieving a healthy weight) and meet their specific needs (e.g., weight loss, weight stability, prevention of weight regain, or loss of excessive abdominal fat) through regular participation in physical activity and exercise.
Scientific Evidence
The 2008 PAGAC noted physical activity (150 minutes per week to ≥300 minutes per week) was associated with modest weight loss, prevention of weight gain following weight loss, and reductions in total and regional adiposity. Evidence that resistance training helped with weight maintenance was not as strong, given that resistance training increases lean muscle mass, and the volume of resistance training regimes was usually less than that for aerobic training.
The 2018 PAGAC expanded the review of the evidence available in 2008, and focused on weight maintenance and weight gain within normal BMI limits (18.5 to < 25 kg/m2) for adults in relation to participating in 150 minutes per week or more of physical activity. The 2018 report also reviewed the impact of sedentary behavior and sedentary activity in relationship to physical activity and weight status. The specific 2018 PAGAC findings regarding weight gain were:
- Strong evidence demonstrates that the significant relationship between greater time spent in physical activity (≥300 minutes per week) and attenuated weight gain in adults is observed with moderate-to-vigorous physical activity.
- Moderate evidence indicates that the relationship between greater amounts of physical activity and attenuated weight gain in adults does not appear to vary by sex.
- Limited evidence suggests a dose-response relationship between physical activity and the risk of weight gain in adults, with greater amounts of physical activity (150 minutes per week) associated with lower risk of weight gain.
- Limited evidence suggests that the relationship between greater amounts of physical activity and attenuated weight gain in adults varies by age, with the effect diminishing with increasing age. The evidence from studies of older adults, however, is inconsistent.
- Insufficient evidence is available to determine whether the relationship between greater amounts of physical activity and attenuated weight gain in adults varies by race and ethnicity.
- Insufficient evidence is available to determine whether the relationship between greater amounts of physical activity and attenuated weight gain in adults varies by socioeconomic status.
- Insufficient evidence is available to determine whether the relationship between greater amounts of physical activity and attenuated weight gain in adults varies by initial weight status.
- Insufficient evidence is available to determine an association between light-intensity activity and attenuated weight gain in adults.
The 2018 PAGAC concluded the following with regard to the impact of sedentary behavior and sedentary activity for adults in relationship to physical activity and weight status:
- Limited evidence suggests a positive relationship between greater time spent in sedentary behavior and higher levels of adiposity and indicators of weight status.
- Limited evidence suggests the existence of a direct, graded dose-response relationship between greater sedentary behavior and higher levels of adiposity and indicators of weight status.
- Insufficient evidence is available to determine whether the relationship between sedentary behavior and weight status varies by age, sex, ethnicity, socioeconomic status, or baseline weight status.
- Insufficient evidence is available to determine whether the relationship between sedentary behavior and weight status varies by amount of moderate-to-vigorous physical activity.
- Insufficient evidence is available to determine whether bouts or breaks in sedentary behavior are important factors in the relationship between sedentary behavior and weight status.
As mentioned earlier in the chapter, regular physical activity and exercise are also important to prevent and control obesity and overweight in children and adolescents. The 2008 PAGAC found strong evidence demonstrating that higher levels of physical activity were associated with multiple beneficial health outcomes, including cardiorespiratory and muscular fitness, bone health, and maintenance of healthy weight status in children and adolescents (ages 6-19). The 2018 PAGAC focused on expanding the review of literature since 2008 with the addition of studies on children 3-6 years of age. The additional scientific recommendations of the 2018 PAGAC for youth were as follows:
- Strong evidence demonstrates that higher amounts of physical activity are associated with a reduced risk of excessive increases in body weight and adiposity in children ages 3 to 6 years.
- Limited evidence suggests that greater time spent in sedentary behavior is related to higher weight status or adiposity in children and adolescents; the evidence is somewhat stronger for television viewing or screen time than for total sedentary time.
- Insufficient evidence is available to determine whether the relationship between physical activity and health effects in children younger than 6 years of age is moderated by age, sex, race, ethnicity, weight status, or socioeconomic status.
Community-scale or macro-environmental urban design
Community-scale or macro-environmental urban design strategies for promoting physical activity involve changes and enhancements to the built environment of urban areas of several square miles (or kilometers) or larger, which are usually defined as being an administrative unit (zip code, neighborhood, school district, city, or county). These kinds of approaches strive to make entire communities more amenable to physical activity, whether that activity is transportation-related or exercise performed in discretionary time. Strategies at this level of influence include connecting transportation arteries; creating landscaping and lighting to enhance the aesthetics and perceived safety of the entire community; building a large-scale and interconnected network of sidewalks, bicycle lanes, and trails; and designing new mixed-use residential areas so that destinations such as workplaces, schools, and areas for leisure and recreation are within safe walking or bicycling distances.
One important and unique macro-environmental urban design element is road connectivity. The concept of connectivity refers to the ease of getting from one place to another within a neighborhood using the city's road network to walk or bike. If city thoroughfares follow a grid pattern, it is easy to use the street network (assuming sidewalks or bicycle lanes are available) to move around on foot or on bicycle; however, if intersections are very far from each other or there are quite a few dead-end streets or culs-de-sac, connectivity is considered to be sub-optimal. Another related construct for the macro-environment that has emerged in the past couple of decades is walkability. Walkability refers to the conduciveness of walking for transportation based on features of the built environment of an urban area. Many researchers have proposed different definitions of walkability, using scores or indices. Some of these scores are even used by real-estate companies to provide their clients with information about potential neighborhoods. High walkability scores or indices could indicate the best mix of built environment elements, and if optimized, could point to a neighborhood that is very easy to navigate on foot. Likewise, neighborhoods with low walkability scores are those with suboptimal conditions for transport-based walking. Most available walkability scores or indices include measures of connectivity, land-use mix, and residential density, which are three critical components for optimal urban design that promote walking for transportation in an area. Although this definition for walkability is valid in many parts of the world, it is not applicable in others (e.g., Mexico or China) (Salvo et al. 2014; Lu et al. 2017). Therefore, it is always important to consider the local context, including the social environment (social norms and cultural values), when trying to promote walkable environments because these may look different in other parts of the world.
Studies examining community-scale changes for physical activity promotion have used a wide variety of outcome measures (Heath et al. 2006). Some have studied the absolute number of walking trips in a community over a given time period; others, the distance of those trips, minutes of walking per week, and number of pedestrians in a certain area. Although these outcomes are not entirely comparable, the general interpretation is that making the built environment more activity-friendly can improve levels of physical activity (regardless of how it is measured) by an average of more than 160%. Clearly, this is a major influence on physical activity habits in a community.
Development of health guidelines
The development of health guidelines is a third critical function of public health science. Public health guidelines are official policy statements, usually developed by a government body, agency, or other reputable organization, that are based on the best available science. Public health guidelines provide clear recommendations about a course of action to deal with a pressing public health issue. Recommendations for childhood immunization schedules (when and which vaccines and their timing), diabetes treatment (the frequency and method of glucose self-monitoring), nutrient intake (micronutrient daily recommended intakes for health), and annual influenza vaccinations (type and timing) are all examples of public health guidelines that, based on the best available science, give health professionals and the public clear guidance about the most appropriate courses of action for preventing and treating certain health problems.
In 2008, the U.S. Department of Health and Human Services published the first Physical Activity Guidelines for Americans (USDHHS 2008; see the highlight box2018 Physical Activity Guidelines for Americans). These guidelines, updated in 2018, are based on comprehensive scientific summaries to detail the best science-based recommendation for the weekly amount of physical activity necessary to prevent disease and promote positive health outcomes (USDHHS 2018). The physical activity guidelines were developed for children and adolescents, adults, and older adults. These guidelines should be used as targets for physical activity participation.
Several other countries, as well as the World Health Organization, have published guidelines similar to the Physical Activity Guidelines for Americans. Japan, Canada, Australia, and England have all taken leadership roles in establishing physical activity as a public health priority by setting physical activity guidelines and recommendations.
Promoting Physical Activity for Health
As the field of physical activity and public health has emerged, it has become clear that many factors at many levels influence physical activity behaviors. Many investigators have used the social ecological model as a guiding framework to explain these multiple levels. They are illustrated in figure 3.6 and form the basis for the third section of this textbook.
Figure 3.6 Multiple levels of influence on physical activity behaviors: The social ecological model.
At the center of the target in the social ecological model for physical activity behaviors are individual factors. These are the factors that are innate to each person and that differ among people. A person's genetic makeup, early life experiences (e.g., youth sport participation), self-efficacy, and other factors, such as sex, disability, growth and development, and socioeconomic status, may all be important determinants of health behaviors such as physical activity.
Moving out from the center, social influences on physical activity are important. Research has now shown that individual factors are not enough to explain physical activity behavior. Determinants at the social influences level aren't characteristics of the person per se, but are, rather, characteristics of how the person interacts with society or culture. Influences at this level can include peers, medical care organizations (doctors), family members, and organizations (schools, places of worship, worksites).
The third level in the social ecological model represents environmental influences. These influences may enhance or restrict physical activity behaviors, and are external to the person but common across societies and cultures. Research on the effects of physical environment on physical activity participation has exploded as the field of physical activity and public health has emerged. The ability to influence the physical activity of vast numbers of people (instead of one person at a time) by making a single change makes environmental influences on physical activity a particularly interesting area of research. The availability of places to be active, such as trails, sidewalks, fitness facilities, bicycle lanes, community and neighborhood design elements are examples of how the built environment can influence physical activity.
Finally, the outer level represents policy influences on physical activity. Influences in this sphere include written or unwritten rules, codes, and norms that influence environmental or social determinants of physical activity. As with the physical environment, determinants at this level are particularly attractive because of their potential to influence many people. Examples of policy influences on physical activity include policies allowing increased access to places to be physically active (making it easier to be physically active), educational policies (e.g., mandating high-quality daily physical education for schoolchildren), and transportation-related policies (e.g., making it easier to walk or bicycle for transportation).
By combining knowledge, skills, and abilities related to the basic exercise sciences and public health, you can better explain and discuss professionally the health benefits and risks of exercise and physical activity to your peers, colleagues, and the communities you serve (see part II, chapters 5 through 10). An understanding of the specific challenges that affect physical activity and exercise in professional exercise science jobs can clarify how the exercise sciences affect public health, and vice versa. The highlight box Careers Combining Exercise Science and Public Health lists careers in exercise physiology, biomechanics, and sport and exercise psychology that are commonly seen in the professional areas of health and fitness, preventive medicine, athletic performance, and rehabilitation.
Physical activity guidelines for a healthy weight
For many adults, obesity is associated with significant increases in abdominal fat that increase the risk for metabolic syndrome and type 2 diabetes (see chapter 5). Regular participation in aerobic physical activity and exercise can decrease total body fat and abdominal fat, and these changes are consistent with improved metabolic function. Generally, the greater the volume of physical activity or exercise acquired by individuals or populations, the greater the reductions in body and abdominal fat.
For children and adolescents, the prevention of excessive weight gain during maturation is critical to prevent obesity and overweight in adulthood. Unfortunately, recent public health surveys note that the parents of many at-risk children are not aware of the problem or do not recognize that their children are overweight. Recent U.S. national policy statements targeting pediatricians and other health care providers assert that children and adolescents who are overweight or obese in their early teens should be identified as early as possible and given some sort of weight management plan through the intervention of parents, teachers, coaches, and family physicians.
One of the most obvious influences on weight management is how people perceive their ideal weight or physique. Research findings indicate a great disparity between reasonable weight loss or weight gain goals and people's “dream weight.” Even though some people may not reach their goal weight, they will likely report positive physical, social, and psychological benefits from any weight loss. The following scientific evidence and guidelines can help individuals and populations establish realistic goals for weight management (e.g., achieving a healthy weight) and meet their specific needs (e.g., weight loss, weight stability, prevention of weight regain, or loss of excessive abdominal fat) through regular participation in physical activity and exercise.
Scientific Evidence
The 2008 PAGAC noted physical activity (150 minutes per week to ≥300 minutes per week) was associated with modest weight loss, prevention of weight gain following weight loss, and reductions in total and regional adiposity. Evidence that resistance training helped with weight maintenance was not as strong, given that resistance training increases lean muscle mass, and the volume of resistance training regimes was usually less than that for aerobic training.
The 2018 PAGAC expanded the review of the evidence available in 2008, and focused on weight maintenance and weight gain within normal BMI limits (18.5 to < 25 kg/m2) for adults in relation to participating in 150 minutes per week or more of physical activity. The 2018 report also reviewed the impact of sedentary behavior and sedentary activity in relationship to physical activity and weight status. The specific 2018 PAGAC findings regarding weight gain were:
- Strong evidence demonstrates that the significant relationship between greater time spent in physical activity (≥300 minutes per week) and attenuated weight gain in adults is observed with moderate-to-vigorous physical activity.
- Moderate evidence indicates that the relationship between greater amounts of physical activity and attenuated weight gain in adults does not appear to vary by sex.
- Limited evidence suggests a dose-response relationship between physical activity and the risk of weight gain in adults, with greater amounts of physical activity (150 minutes per week) associated with lower risk of weight gain.
- Limited evidence suggests that the relationship between greater amounts of physical activity and attenuated weight gain in adults varies by age, with the effect diminishing with increasing age. The evidence from studies of older adults, however, is inconsistent.
- Insufficient evidence is available to determine whether the relationship between greater amounts of physical activity and attenuated weight gain in adults varies by race and ethnicity.
- Insufficient evidence is available to determine whether the relationship between greater amounts of physical activity and attenuated weight gain in adults varies by socioeconomic status.
- Insufficient evidence is available to determine whether the relationship between greater amounts of physical activity and attenuated weight gain in adults varies by initial weight status.
- Insufficient evidence is available to determine an association between light-intensity activity and attenuated weight gain in adults.
The 2018 PAGAC concluded the following with regard to the impact of sedentary behavior and sedentary activity for adults in relationship to physical activity and weight status:
- Limited evidence suggests a positive relationship between greater time spent in sedentary behavior and higher levels of adiposity and indicators of weight status.
- Limited evidence suggests the existence of a direct, graded dose-response relationship between greater sedentary behavior and higher levels of adiposity and indicators of weight status.
- Insufficient evidence is available to determine whether the relationship between sedentary behavior and weight status varies by age, sex, ethnicity, socioeconomic status, or baseline weight status.
- Insufficient evidence is available to determine whether the relationship between sedentary behavior and weight status varies by amount of moderate-to-vigorous physical activity.
- Insufficient evidence is available to determine whether bouts or breaks in sedentary behavior are important factors in the relationship between sedentary behavior and weight status.
As mentioned earlier in the chapter, regular physical activity and exercise are also important to prevent and control obesity and overweight in children and adolescents. The 2008 PAGAC found strong evidence demonstrating that higher levels of physical activity were associated with multiple beneficial health outcomes, including cardiorespiratory and muscular fitness, bone health, and maintenance of healthy weight status in children and adolescents (ages 6-19). The 2018 PAGAC focused on expanding the review of literature since 2008 with the addition of studies on children 3-6 years of age. The additional scientific recommendations of the 2018 PAGAC for youth were as follows:
- Strong evidence demonstrates that higher amounts of physical activity are associated with a reduced risk of excessive increases in body weight and adiposity in children ages 3 to 6 years.
- Limited evidence suggests that greater time spent in sedentary behavior is related to higher weight status or adiposity in children and adolescents; the evidence is somewhat stronger for television viewing or screen time than for total sedentary time.
- Insufficient evidence is available to determine whether the relationship between physical activity and health effects in children younger than 6 years of age is moderated by age, sex, race, ethnicity, weight status, or socioeconomic status.
Community-scale or macro-environmental urban design
Community-scale or macro-environmental urban design strategies for promoting physical activity involve changes and enhancements to the built environment of urban areas of several square miles (or kilometers) or larger, which are usually defined as being an administrative unit (zip code, neighborhood, school district, city, or county). These kinds of approaches strive to make entire communities more amenable to physical activity, whether that activity is transportation-related or exercise performed in discretionary time. Strategies at this level of influence include connecting transportation arteries; creating landscaping and lighting to enhance the aesthetics and perceived safety of the entire community; building a large-scale and interconnected network of sidewalks, bicycle lanes, and trails; and designing new mixed-use residential areas so that destinations such as workplaces, schools, and areas for leisure and recreation are within safe walking or bicycling distances.
One important and unique macro-environmental urban design element is road connectivity. The concept of connectivity refers to the ease of getting from one place to another within a neighborhood using the city's road network to walk or bike. If city thoroughfares follow a grid pattern, it is easy to use the street network (assuming sidewalks or bicycle lanes are available) to move around on foot or on bicycle; however, if intersections are very far from each other or there are quite a few dead-end streets or culs-de-sac, connectivity is considered to be sub-optimal. Another related construct for the macro-environment that has emerged in the past couple of decades is walkability. Walkability refers to the conduciveness of walking for transportation based on features of the built environment of an urban area. Many researchers have proposed different definitions of walkability, using scores or indices. Some of these scores are even used by real-estate companies to provide their clients with information about potential neighborhoods. High walkability scores or indices could indicate the best mix of built environment elements, and if optimized, could point to a neighborhood that is very easy to navigate on foot. Likewise, neighborhoods with low walkability scores are those with suboptimal conditions for transport-based walking. Most available walkability scores or indices include measures of connectivity, land-use mix, and residential density, which are three critical components for optimal urban design that promote walking for transportation in an area. Although this definition for walkability is valid in many parts of the world, it is not applicable in others (e.g., Mexico or China) (Salvo et al. 2014; Lu et al. 2017). Therefore, it is always important to consider the local context, including the social environment (social norms and cultural values), when trying to promote walkable environments because these may look different in other parts of the world.
Studies examining community-scale changes for physical activity promotion have used a wide variety of outcome measures (Heath et al. 2006). Some have studied the absolute number of walking trips in a community over a given time period; others, the distance of those trips, minutes of walking per week, and number of pedestrians in a certain area. Although these outcomes are not entirely comparable, the general interpretation is that making the built environment more activity-friendly can improve levels of physical activity (regardless of how it is measured) by an average of more than 160%. Clearly, this is a major influence on physical activity habits in a community.
Development of health guidelines
The development of health guidelines is a third critical function of public health science. Public health guidelines are official policy statements, usually developed by a government body, agency, or other reputable organization, that are based on the best available science. Public health guidelines provide clear recommendations about a course of action to deal with a pressing public health issue. Recommendations for childhood immunization schedules (when and which vaccines and their timing), diabetes treatment (the frequency and method of glucose self-monitoring), nutrient intake (micronutrient daily recommended intakes for health), and annual influenza vaccinations (type and timing) are all examples of public health guidelines that, based on the best available science, give health professionals and the public clear guidance about the most appropriate courses of action for preventing and treating certain health problems.
In 2008, the U.S. Department of Health and Human Services published the first Physical Activity Guidelines for Americans (USDHHS 2008; see the highlight box2018 Physical Activity Guidelines for Americans). These guidelines, updated in 2018, are based on comprehensive scientific summaries to detail the best science-based recommendation for the weekly amount of physical activity necessary to prevent disease and promote positive health outcomes (USDHHS 2018). The physical activity guidelines were developed for children and adolescents, adults, and older adults. These guidelines should be used as targets for physical activity participation.
Several other countries, as well as the World Health Organization, have published guidelines similar to the Physical Activity Guidelines for Americans. Japan, Canada, Australia, and England have all taken leadership roles in establishing physical activity as a public health priority by setting physical activity guidelines and recommendations.
Promoting Physical Activity for Health
As the field of physical activity and public health has emerged, it has become clear that many factors at many levels influence physical activity behaviors. Many investigators have used the social ecological model as a guiding framework to explain these multiple levels. They are illustrated in figure 3.6 and form the basis for the third section of this textbook.
Figure 3.6 Multiple levels of influence on physical activity behaviors: The social ecological model.
At the center of the target in the social ecological model for physical activity behaviors are individual factors. These are the factors that are innate to each person and that differ among people. A person's genetic makeup, early life experiences (e.g., youth sport participation), self-efficacy, and other factors, such as sex, disability, growth and development, and socioeconomic status, may all be important determinants of health behaviors such as physical activity.
Moving out from the center, social influences on physical activity are important. Research has now shown that individual factors are not enough to explain physical activity behavior. Determinants at the social influences level aren't characteristics of the person per se, but are, rather, characteristics of how the person interacts with society or culture. Influences at this level can include peers, medical care organizations (doctors), family members, and organizations (schools, places of worship, worksites).
The third level in the social ecological model represents environmental influences. These influences may enhance or restrict physical activity behaviors, and are external to the person but common across societies and cultures. Research on the effects of physical environment on physical activity participation has exploded as the field of physical activity and public health has emerged. The ability to influence the physical activity of vast numbers of people (instead of one person at a time) by making a single change makes environmental influences on physical activity a particularly interesting area of research. The availability of places to be active, such as trails, sidewalks, fitness facilities, bicycle lanes, community and neighborhood design elements are examples of how the built environment can influence physical activity.
Finally, the outer level represents policy influences on physical activity. Influences in this sphere include written or unwritten rules, codes, and norms that influence environmental or social determinants of physical activity. As with the physical environment, determinants at this level are particularly attractive because of their potential to influence many people. Examples of policy influences on physical activity include policies allowing increased access to places to be physically active (making it easier to be physically active), educational policies (e.g., mandating high-quality daily physical education for schoolchildren), and transportation-related policies (e.g., making it easier to walk or bicycle for transportation).
By combining knowledge, skills, and abilities related to the basic exercise sciences and public health, you can better explain and discuss professionally the health benefits and risks of exercise and physical activity to your peers, colleagues, and the communities you serve (see part II, chapters 5 through 10). An understanding of the specific challenges that affect physical activity and exercise in professional exercise science jobs can clarify how the exercise sciences affect public health, and vice versa. The highlight box Careers Combining Exercise Science and Public Health lists careers in exercise physiology, biomechanics, and sport and exercise psychology that are commonly seen in the professional areas of health and fitness, preventive medicine, athletic performance, and rehabilitation.
Physical activity guidelines for a healthy weight
For many adults, obesity is associated with significant increases in abdominal fat that increase the risk for metabolic syndrome and type 2 diabetes (see chapter 5). Regular participation in aerobic physical activity and exercise can decrease total body fat and abdominal fat, and these changes are consistent with improved metabolic function. Generally, the greater the volume of physical activity or exercise acquired by individuals or populations, the greater the reductions in body and abdominal fat.
For children and adolescents, the prevention of excessive weight gain during maturation is critical to prevent obesity and overweight in adulthood. Unfortunately, recent public health surveys note that the parents of many at-risk children are not aware of the problem or do not recognize that their children are overweight. Recent U.S. national policy statements targeting pediatricians and other health care providers assert that children and adolescents who are overweight or obese in their early teens should be identified as early as possible and given some sort of weight management plan through the intervention of parents, teachers, coaches, and family physicians.
One of the most obvious influences on weight management is how people perceive their ideal weight or physique. Research findings indicate a great disparity between reasonable weight loss or weight gain goals and people's “dream weight.” Even though some people may not reach their goal weight, they will likely report positive physical, social, and psychological benefits from any weight loss. The following scientific evidence and guidelines can help individuals and populations establish realistic goals for weight management (e.g., achieving a healthy weight) and meet their specific needs (e.g., weight loss, weight stability, prevention of weight regain, or loss of excessive abdominal fat) through regular participation in physical activity and exercise.
Scientific Evidence
The 2008 PAGAC noted physical activity (150 minutes per week to ≥300 minutes per week) was associated with modest weight loss, prevention of weight gain following weight loss, and reductions in total and regional adiposity. Evidence that resistance training helped with weight maintenance was not as strong, given that resistance training increases lean muscle mass, and the volume of resistance training regimes was usually less than that for aerobic training.
The 2018 PAGAC expanded the review of the evidence available in 2008, and focused on weight maintenance and weight gain within normal BMI limits (18.5 to < 25 kg/m2) for adults in relation to participating in 150 minutes per week or more of physical activity. The 2018 report also reviewed the impact of sedentary behavior and sedentary activity in relationship to physical activity and weight status. The specific 2018 PAGAC findings regarding weight gain were:
- Strong evidence demonstrates that the significant relationship between greater time spent in physical activity (≥300 minutes per week) and attenuated weight gain in adults is observed with moderate-to-vigorous physical activity.
- Moderate evidence indicates that the relationship between greater amounts of physical activity and attenuated weight gain in adults does not appear to vary by sex.
- Limited evidence suggests a dose-response relationship between physical activity and the risk of weight gain in adults, with greater amounts of physical activity (150 minutes per week) associated with lower risk of weight gain.
- Limited evidence suggests that the relationship between greater amounts of physical activity and attenuated weight gain in adults varies by age, with the effect diminishing with increasing age. The evidence from studies of older adults, however, is inconsistent.
- Insufficient evidence is available to determine whether the relationship between greater amounts of physical activity and attenuated weight gain in adults varies by race and ethnicity.
- Insufficient evidence is available to determine whether the relationship between greater amounts of physical activity and attenuated weight gain in adults varies by socioeconomic status.
- Insufficient evidence is available to determine whether the relationship between greater amounts of physical activity and attenuated weight gain in adults varies by initial weight status.
- Insufficient evidence is available to determine an association between light-intensity activity and attenuated weight gain in adults.
The 2018 PAGAC concluded the following with regard to the impact of sedentary behavior and sedentary activity for adults in relationship to physical activity and weight status:
- Limited evidence suggests a positive relationship between greater time spent in sedentary behavior and higher levels of adiposity and indicators of weight status.
- Limited evidence suggests the existence of a direct, graded dose-response relationship between greater sedentary behavior and higher levels of adiposity and indicators of weight status.
- Insufficient evidence is available to determine whether the relationship between sedentary behavior and weight status varies by age, sex, ethnicity, socioeconomic status, or baseline weight status.
- Insufficient evidence is available to determine whether the relationship between sedentary behavior and weight status varies by amount of moderate-to-vigorous physical activity.
- Insufficient evidence is available to determine whether bouts or breaks in sedentary behavior are important factors in the relationship between sedentary behavior and weight status.
As mentioned earlier in the chapter, regular physical activity and exercise are also important to prevent and control obesity and overweight in children and adolescents. The 2008 PAGAC found strong evidence demonstrating that higher levels of physical activity were associated with multiple beneficial health outcomes, including cardiorespiratory and muscular fitness, bone health, and maintenance of healthy weight status in children and adolescents (ages 6-19). The 2018 PAGAC focused on expanding the review of literature since 2008 with the addition of studies on children 3-6 years of age. The additional scientific recommendations of the 2018 PAGAC for youth were as follows:
- Strong evidence demonstrates that higher amounts of physical activity are associated with a reduced risk of excessive increases in body weight and adiposity in children ages 3 to 6 years.
- Limited evidence suggests that greater time spent in sedentary behavior is related to higher weight status or adiposity in children and adolescents; the evidence is somewhat stronger for television viewing or screen time than for total sedentary time.
- Insufficient evidence is available to determine whether the relationship between physical activity and health effects in children younger than 6 years of age is moderated by age, sex, race, ethnicity, weight status, or socioeconomic status.
Community-scale or macro-environmental urban design
Community-scale or macro-environmental urban design strategies for promoting physical activity involve changes and enhancements to the built environment of urban areas of several square miles (or kilometers) or larger, which are usually defined as being an administrative unit (zip code, neighborhood, school district, city, or county). These kinds of approaches strive to make entire communities more amenable to physical activity, whether that activity is transportation-related or exercise performed in discretionary time. Strategies at this level of influence include connecting transportation arteries; creating landscaping and lighting to enhance the aesthetics and perceived safety of the entire community; building a large-scale and interconnected network of sidewalks, bicycle lanes, and trails; and designing new mixed-use residential areas so that destinations such as workplaces, schools, and areas for leisure and recreation are within safe walking or bicycling distances.
One important and unique macro-environmental urban design element is road connectivity. The concept of connectivity refers to the ease of getting from one place to another within a neighborhood using the city's road network to walk or bike. If city thoroughfares follow a grid pattern, it is easy to use the street network (assuming sidewalks or bicycle lanes are available) to move around on foot or on bicycle; however, if intersections are very far from each other or there are quite a few dead-end streets or culs-de-sac, connectivity is considered to be sub-optimal. Another related construct for the macro-environment that has emerged in the past couple of decades is walkability. Walkability refers to the conduciveness of walking for transportation based on features of the built environment of an urban area. Many researchers have proposed different definitions of walkability, using scores or indices. Some of these scores are even used by real-estate companies to provide their clients with information about potential neighborhoods. High walkability scores or indices could indicate the best mix of built environment elements, and if optimized, could point to a neighborhood that is very easy to navigate on foot. Likewise, neighborhoods with low walkability scores are those with suboptimal conditions for transport-based walking. Most available walkability scores or indices include measures of connectivity, land-use mix, and residential density, which are three critical components for optimal urban design that promote walking for transportation in an area. Although this definition for walkability is valid in many parts of the world, it is not applicable in others (e.g., Mexico or China) (Salvo et al. 2014; Lu et al. 2017). Therefore, it is always important to consider the local context, including the social environment (social norms and cultural values), when trying to promote walkable environments because these may look different in other parts of the world.
Studies examining community-scale changes for physical activity promotion have used a wide variety of outcome measures (Heath et al. 2006). Some have studied the absolute number of walking trips in a community over a given time period; others, the distance of those trips, minutes of walking per week, and number of pedestrians in a certain area. Although these outcomes are not entirely comparable, the general interpretation is that making the built environment more activity-friendly can improve levels of physical activity (regardless of how it is measured) by an average of more than 160%. Clearly, this is a major influence on physical activity habits in a community.
Development of health guidelines
The development of health guidelines is a third critical function of public health science. Public health guidelines are official policy statements, usually developed by a government body, agency, or other reputable organization, that are based on the best available science. Public health guidelines provide clear recommendations about a course of action to deal with a pressing public health issue. Recommendations for childhood immunization schedules (when and which vaccines and their timing), diabetes treatment (the frequency and method of glucose self-monitoring), nutrient intake (micronutrient daily recommended intakes for health), and annual influenza vaccinations (type and timing) are all examples of public health guidelines that, based on the best available science, give health professionals and the public clear guidance about the most appropriate courses of action for preventing and treating certain health problems.
In 2008, the U.S. Department of Health and Human Services published the first Physical Activity Guidelines for Americans (USDHHS 2008; see the highlight box2018 Physical Activity Guidelines for Americans). These guidelines, updated in 2018, are based on comprehensive scientific summaries to detail the best science-based recommendation for the weekly amount of physical activity necessary to prevent disease and promote positive health outcomes (USDHHS 2018). The physical activity guidelines were developed for children and adolescents, adults, and older adults. These guidelines should be used as targets for physical activity participation.
Several other countries, as well as the World Health Organization, have published guidelines similar to the Physical Activity Guidelines for Americans. Japan, Canada, Australia, and England have all taken leadership roles in establishing physical activity as a public health priority by setting physical activity guidelines and recommendations.
Promoting Physical Activity for Health
As the field of physical activity and public health has emerged, it has become clear that many factors at many levels influence physical activity behaviors. Many investigators have used the social ecological model as a guiding framework to explain these multiple levels. They are illustrated in figure 3.6 and form the basis for the third section of this textbook.
Figure 3.6 Multiple levels of influence on physical activity behaviors: The social ecological model.
At the center of the target in the social ecological model for physical activity behaviors are individual factors. These are the factors that are innate to each person and that differ among people. A person's genetic makeup, early life experiences (e.g., youth sport participation), self-efficacy, and other factors, such as sex, disability, growth and development, and socioeconomic status, may all be important determinants of health behaviors such as physical activity.
Moving out from the center, social influences on physical activity are important. Research has now shown that individual factors are not enough to explain physical activity behavior. Determinants at the social influences level aren't characteristics of the person per se, but are, rather, characteristics of how the person interacts with society or culture. Influences at this level can include peers, medical care organizations (doctors), family members, and organizations (schools, places of worship, worksites).
The third level in the social ecological model represents environmental influences. These influences may enhance or restrict physical activity behaviors, and are external to the person but common across societies and cultures. Research on the effects of physical environment on physical activity participation has exploded as the field of physical activity and public health has emerged. The ability to influence the physical activity of vast numbers of people (instead of one person at a time) by making a single change makes environmental influences on physical activity a particularly interesting area of research. The availability of places to be active, such as trails, sidewalks, fitness facilities, bicycle lanes, community and neighborhood design elements are examples of how the built environment can influence physical activity.
Finally, the outer level represents policy influences on physical activity. Influences in this sphere include written or unwritten rules, codes, and norms that influence environmental or social determinants of physical activity. As with the physical environment, determinants at this level are particularly attractive because of their potential to influence many people. Examples of policy influences on physical activity include policies allowing increased access to places to be physically active (making it easier to be physically active), educational policies (e.g., mandating high-quality daily physical education for schoolchildren), and transportation-related policies (e.g., making it easier to walk or bicycle for transportation).
By combining knowledge, skills, and abilities related to the basic exercise sciences and public health, you can better explain and discuss professionally the health benefits and risks of exercise and physical activity to your peers, colleagues, and the communities you serve (see part II, chapters 5 through 10). An understanding of the specific challenges that affect physical activity and exercise in professional exercise science jobs can clarify how the exercise sciences affect public health, and vice versa. The highlight box Careers Combining Exercise Science and Public Health lists careers in exercise physiology, biomechanics, and sport and exercise psychology that are commonly seen in the professional areas of health and fitness, preventive medicine, athletic performance, and rehabilitation.
Physical activity guidelines for a healthy weight
For many adults, obesity is associated with significant increases in abdominal fat that increase the risk for metabolic syndrome and type 2 diabetes (see chapter 5). Regular participation in aerobic physical activity and exercise can decrease total body fat and abdominal fat, and these changes are consistent with improved metabolic function. Generally, the greater the volume of physical activity or exercise acquired by individuals or populations, the greater the reductions in body and abdominal fat.
For children and adolescents, the prevention of excessive weight gain during maturation is critical to prevent obesity and overweight in adulthood. Unfortunately, recent public health surveys note that the parents of many at-risk children are not aware of the problem or do not recognize that their children are overweight. Recent U.S. national policy statements targeting pediatricians and other health care providers assert that children and adolescents who are overweight or obese in their early teens should be identified as early as possible and given some sort of weight management plan through the intervention of parents, teachers, coaches, and family physicians.
One of the most obvious influences on weight management is how people perceive their ideal weight or physique. Research findings indicate a great disparity between reasonable weight loss or weight gain goals and people's “dream weight.” Even though some people may not reach their goal weight, they will likely report positive physical, social, and psychological benefits from any weight loss. The following scientific evidence and guidelines can help individuals and populations establish realistic goals for weight management (e.g., achieving a healthy weight) and meet their specific needs (e.g., weight loss, weight stability, prevention of weight regain, or loss of excessive abdominal fat) through regular participation in physical activity and exercise.
Scientific Evidence
The 2008 PAGAC noted physical activity (150 minutes per week to ≥300 minutes per week) was associated with modest weight loss, prevention of weight gain following weight loss, and reductions in total and regional adiposity. Evidence that resistance training helped with weight maintenance was not as strong, given that resistance training increases lean muscle mass, and the volume of resistance training regimes was usually less than that for aerobic training.
The 2018 PAGAC expanded the review of the evidence available in 2008, and focused on weight maintenance and weight gain within normal BMI limits (18.5 to < 25 kg/m2) for adults in relation to participating in 150 minutes per week or more of physical activity. The 2018 report also reviewed the impact of sedentary behavior and sedentary activity in relationship to physical activity and weight status. The specific 2018 PAGAC findings regarding weight gain were:
- Strong evidence demonstrates that the significant relationship between greater time spent in physical activity (≥300 minutes per week) and attenuated weight gain in adults is observed with moderate-to-vigorous physical activity.
- Moderate evidence indicates that the relationship between greater amounts of physical activity and attenuated weight gain in adults does not appear to vary by sex.
- Limited evidence suggests a dose-response relationship between physical activity and the risk of weight gain in adults, with greater amounts of physical activity (150 minutes per week) associated with lower risk of weight gain.
- Limited evidence suggests that the relationship between greater amounts of physical activity and attenuated weight gain in adults varies by age, with the effect diminishing with increasing age. The evidence from studies of older adults, however, is inconsistent.
- Insufficient evidence is available to determine whether the relationship between greater amounts of physical activity and attenuated weight gain in adults varies by race and ethnicity.
- Insufficient evidence is available to determine whether the relationship between greater amounts of physical activity and attenuated weight gain in adults varies by socioeconomic status.
- Insufficient evidence is available to determine whether the relationship between greater amounts of physical activity and attenuated weight gain in adults varies by initial weight status.
- Insufficient evidence is available to determine an association between light-intensity activity and attenuated weight gain in adults.
The 2018 PAGAC concluded the following with regard to the impact of sedentary behavior and sedentary activity for adults in relationship to physical activity and weight status:
- Limited evidence suggests a positive relationship between greater time spent in sedentary behavior and higher levels of adiposity and indicators of weight status.
- Limited evidence suggests the existence of a direct, graded dose-response relationship between greater sedentary behavior and higher levels of adiposity and indicators of weight status.
- Insufficient evidence is available to determine whether the relationship between sedentary behavior and weight status varies by age, sex, ethnicity, socioeconomic status, or baseline weight status.
- Insufficient evidence is available to determine whether the relationship between sedentary behavior and weight status varies by amount of moderate-to-vigorous physical activity.
- Insufficient evidence is available to determine whether bouts or breaks in sedentary behavior are important factors in the relationship between sedentary behavior and weight status.
As mentioned earlier in the chapter, regular physical activity and exercise are also important to prevent and control obesity and overweight in children and adolescents. The 2008 PAGAC found strong evidence demonstrating that higher levels of physical activity were associated with multiple beneficial health outcomes, including cardiorespiratory and muscular fitness, bone health, and maintenance of healthy weight status in children and adolescents (ages 6-19). The 2018 PAGAC focused on expanding the review of literature since 2008 with the addition of studies on children 3-6 years of age. The additional scientific recommendations of the 2018 PAGAC for youth were as follows:
- Strong evidence demonstrates that higher amounts of physical activity are associated with a reduced risk of excessive increases in body weight and adiposity in children ages 3 to 6 years.
- Limited evidence suggests that greater time spent in sedentary behavior is related to higher weight status or adiposity in children and adolescents; the evidence is somewhat stronger for television viewing or screen time than for total sedentary time.
- Insufficient evidence is available to determine whether the relationship between physical activity and health effects in children younger than 6 years of age is moderated by age, sex, race, ethnicity, weight status, or socioeconomic status.
Related Books









