- Home
- Sociology of Sport
- Recreation and Leisure
- Health Care in Exercise and Sport
- Health Care for Special Conditions
- Recreational Therapy Assessment

Recreational Therapy Assessment provides direction on how to assess clients in order to determine their specific needs. The first book of its kind structured to facilitate program planning at an individualized level, readers will find assessment protocols for various consumer groups:
- Older adults
- Mental health consumers
- Individuals with intellectual and developmental disabilities
- People with physical disabilities
- Those from diverse cultural backgrounds
Conducting effective consumer assessments is a vital skill for both current and future professionals in the field of recreational therapy. Recreational Therapy Assessment will prepare readers to perform those assessments to help them plan and implement customized services for a range of clients.
Chapter 2. Principles of Assessment
Chapter 3. Understanding the International Classification for Functioning, Disability, and Health (ICF) and Consumer Assessment
Chapter 4. Documentation of Health Outcomes in Recreational Therapy
Chapter 5. Assessment and Aging: Considerations and Recommendations for Recreational Therapy
Chapter 6. Assessment and Behavioral Health
Chapter 7. Assessment of Outcomes in Physical Disability: Considerations and Recommendations for Recreational Therapy
Chapter 8. Recreational Therapy Assessment and Individuals With Intellectual Disabilities
Chapter 9. Assessing Clients With Diverse Cultural Backgrounds
Chapter 10. Final Reflections
Thomas Skalko, PhD, LRT/CTRS, FDRT, is a professor emeritus in the College of Health and Human Performance at East Carolina University. Skalko earned his bachelor’s and master’s degrees in education from the University of Georgia and his doctorate from the University of Maryland. Thomas’ background includes direct services in community mental health, inpatient behavioral health, inpatient pediatrics, and primitive therapeutic camping. Thomas is a past president of the American Therapeutic Recreation Association (ATRA) and of the Commission on Accreditation of Allied Health Education Programs (CAAHEP). Skalko is also a past chair of the Committee on Accreditation of Recreational Therapy Education (CARTE) and of the North Carolina Board of Recreational Therapy Licensure (NCBRTL).
Jerome Singleton, PhD, CTRS, retired in 2018 after 37 years as a professor of recreation and leisure studies in the School of Health and Human Performance at Dalhousie University. He was also cross-appointed to the Schools of Nursing, Sociology and Anthropology, and Business Administration at Dalhousie. He earned his bachelor’s degree in recreation from the University of Waterloo, his master’s degree in recreation from Pennsylvania State University, and his PhD in leisure studies from the University of Maryland. He also completed the academic requirements for a doctorate certificate in gerontology at the University of Maryland.
Singleton was made a fellow of the World Demographic Association in 2006 and was named Canadian Therapeutic Recreation Association Professional of the Year in 2007. He was recognized by the Recreation and Leisure Studies program at the University of Waterloo as a Distinguished Alumnus in 2008 and is also the founding member of the Leisure and Aging Research Group, which was established in 2008. Singleton received the Dr. Gonzaga da Gama Memorial Award from the Canadian Therapeutic Recreation Association in 2011 and was made a fellow of the Academy of Leisure Science by the Society of Park and Recreation Educators in 2011.
A snapshot of serving clients from diverse cultural backgrounds in a physical medicine setting
John is a 56-year-old male from Manila, Philippines. The primary language he speaks at home is Tagalog but he is also fluent in English.
By Marc Zaremski
Case Study
A Snapshot of Serving Clients From Diverse Cultural Backgrounds in a Physical Medicine Setting
Written by Marc Zaremski, MS, CTRS: Clemson University
John is a 56-year-old male from Manila, Philippines. The primary language he speaks at home is Tagalog but he is also fluent in English. John moved from Manila to Florida when he was 13 years old with his parents. John has remained in Florida and he currently lives with his wife and youngest daughter. John's wife speaks Tagalog and some English and his daughter is bilingual. John was working on his roof when he experienced a dizzy spell and fell backward off of the ladder, approximately 15 feet, landing on his driveway. John did not lose consciousness and an ambulance was called immediately once he expressed to his wife that he could not move his legs. John sustained fractures in several thoracic vertebrae from T8 to T12. At the T10 level, he sustained a complete spinal cord injury, resulting in paralysis below the T10 level. The ambulance took him to the local trauma center, where he underwent several procedures to stabilize the spinal cord and relieve pressure at the injury site. After John was deemed medically stable, he was transferred to ABC Rehabilitation to receive inpatient rehabilitation approximately seven days postoperative.
At ABC Rehabilitation, John's therapy and medical teams consist of only English-speaking therapists who are all non-Hispanic Caucasian. The facility offers a translation service, when available, which is a live video feed of a translator that can assist during therapy sessions, doctor's visits, and any other time a patient might need information translated to or from a provider. John initially feels comfortable but some aspects of the hospital begin to conflict with his culture. The constant cold temperature throughout the hospital is concerning to him because he believes warmth promotes good health. John's more traditional relatives have expressed concern over food, the treatment plan, and the temperature of the facility as well. A member of John's family is a babaylan, which is a form of healer that uses prayers, herbs, and massage or tissue manipulation as a healing method. John asked his physician and physical therapist if this family member could perform their healing rituals on him. They deemed it unwise because the family member is not a medical professional and John has many precautions. John was disappointed but eventually convinced the medical team to allow this healer to work with him. They agreed, as long as John informed the babaylan of his medical precautions to avoid further injury. The healer is not fluent in English and John had difficulties translating some of the medical terminology. The therapy team used the translation service to confirm that the healer and John understand the restrictions of the treatment. John and the healer articulated that they understood the precautions and John was able to participate in this healing session. John enjoyed the healing session and it put his more traditional family members at ease.
Throughout John's stay he experienced some frustrations and setbacks. Some frustrations were because of how his life had changed due to his injury and some were because of language barriers and a lack of specific cultural knowledge from health care providers. With the flexibility and extra effort of his health care professional, John overcame some of these issues to progress into being independent in his wheelchair and was deemed eligible to return home safely.
It is unrealistic to expect every health care provider to be knowledgeable on the cultural traditions and preferences of every client or patient. But it is important to utilize available resources to gain some insight into what our patients and clients prefer and to find compromise between those beliefs and the best possible medical care.
Applying ICF and Purnell's Stages of Cultural Competence
Based on Purnell's (2012) cultural competence milestones, the level of cultural competence of the physicians and physical therapist does not appear to reach to the cultural sensitivity stage, as evidenced by careless rejections of the healing rituals. They might have noticed that John's background is Filipino; however, they were not aware of how important it was to John and his family members for John to receive healing rituals. In order for physicians and physical therapists to reach a higher stage of cultural competence, the ICF framework is helpful. Personal factors of ICF allow them to look at the person's worldview and value system, beyond race and ethnicity. By understanding the client's values, professionals are more likely to seek ways to achieve things that are important to the person.
Implications for Recreational Therapy Practice
Working with patients or clients from different cultural backgrounds can provide some difficulties for professionals. But many of these difficulties can be resolved or mitigated with extra effort and preparation. Taking the time to look at the resources of your facility and how to access them is a great starting point for establishing a protocol for future clients. If there is admission data or another professional at the facility that may have seen this client first, talking to them can be useful for knowing what resources you may need to acquire. For example, if a patient is admitted who only speaks Spanish, that fact should appear in admission data or a member of the treatment team may inform you prior to you seeing them. This will enable you to schedule that patient when a translator, translation device, or family member that can translate is available. Scheduling appropriately, however, is not a static solution, so a backup plan should be established in case those resources are unavailable. Online translators can be useful for getting some basic translations to assist in your sessions. When all resources are unavailable, a list of key translated words to assist in administering the intervention for that day or for their length of stay may be required. It is difficult to coordinate translation services throughout an entire length of a patient's stay, so having these backup words can be vital for continuing quality service delivery.
Information on those you serve is vital for providing quality care. But it is also important to remember that something you may have found to be true for one patient may not be true for another, even if they have similar backgrounds. The Internet can be useful for finding information on cultures and their traditions, but it is safer to not to make assumptions. The best source of information on your client's beliefs, traditions, and background is typically from the client or their close family members and friends.
Being an active listener allows you to hear concerns that your client may have. This opens up an opportunity for recreational therapists to mitigate those concerns that could be making the client feel uncomfortable. For example, at some facilities, the recreational therapist may have the opportunity to do cooking or kitchen interventions. On occasion, a patient will have religious or cultural dietary restrictions and the food service department may not be meeting these needs. Members of the recreation department should perform functional cooking tasks with patients that meet their religious or cultural needs. This can make the patient or client feel more comfortable during their stay and assist other medical providers in meeting their goals for the client or patient.
When working with patients or clients from diverse cultural backgrounds, the best strategy for working with them can be broken down into four parts:
- Take extra time to gather and access resources.
- Utilize all available data and information.
- Listen to the patient and their caregiver(s) and family members.
- Work to minimize any of the client's concerns.
To help yourself, it can be beneficial to write down or keep stock of the resources and strategies that were most effective for a given scenario. Using these strategies, a solid foundation can be made to assist recreational therapists in better serving populations from diverse cultural backgrounds.
Questions for Consideration
- What strategies did the treatment team use in order to understand John?
- Based on the descriptions of John, to what extent was John culturally assimilated?
- Viewing this case study through an intersectionality lens, what sociodemographic variables might be helpful to understand John?
- If you were a member of John's therapy team, what would you do to implement cultural safety?
- In what way can practitioners move up the stages of cultural competence? How are ICF's personal factors helpful in the process?
Application of the assessment process with an individual with a physical disability
Bill is a 26-year-old with C6 quadriplegia. He completed three months of physical rehabilitation and has been living in the community with his wife for the past nine months.
By David P. Loy
Case Study
Application of the Assessment Process With an Individual With a Physical Disability
Bill is a 26-year-old with C6 quadriplegia. He completed three months of physical rehabilitation and has been living in the community with his wife for the past nine months. Bill heard about the recreational therapist working in his community and met with her to gain more independence and become more active since his discharge. Sarah Bellinger, a CTRS working in Bill's community, agreed to meet with Bill to conduct an assessment. She asked Bill if he could access his inpatient rehabilitation records or have them transferred to her in order to provide some preliminary information. During the initial meeting, Sarah performed a battery of assessments. She used a recreation interest survey to assess Bill's preferred recreation and leisure (d920) activities, a hand and finger dynamometer test for fine hand use (d440), the WST for mobility (d498), the CHART for community reintegration, and the modified functional reach test for vestibular balance (b240). The information indicates Bill has had limited recreation engagement (d920) since his SCI but expressed interest in sports and exercise (d9201) with a desire to get stronger so that he can progress from his power chair to a manual wheelchair. He has expressed a small fear of going in the community by himself because he doesn't have confidence in his skills. Hand and finger dynamometer readings indicate below average fine hand use (d440), but appropriate considering his spinal cord injury level. The WST test indicated a score of 19 (out of 66) for mobility (d498) and the CHART scores ranged from 18 to 32 in all five areas of CI. Answer the following questions based on this information.
- Discuss how the diagnosis of an SCI may have affected the CTRS's selection of assessment instruments.
- What are some appropriate treatment goals based on the interpretation of the assessment performance data provided?
- What are some preliminary interventions appropriate for Bill based on your interpretation of the assessment results?
Understanding the International Classification for Functioning, Disability and Health (ICF) model
To apply the coding of the ICF for effective service delivery, one needs to first understand how to utilize the ICF as a means to classify the full functioning of the individual, perhaps beginning with a diagnosis from the ICD-11.
By Thomas K. Skalko
Understanding the ICF Model
To apply the coding of the ICF for effective service delivery, one needs to first understand how to utilize the ICF as a means to classify the full functioning of the individual, perhaps beginning with a diagnosis from the ICD-11 (see www.who.int/classifications/icd/revision/icdprojectplan2015to2018.pdf?ua=1). The ICD-11 is a medical coding system for documenting diagnoses, signs of illness, symptoms of a condition, and social circumstances. Unlike the ICF, which focuses on functioning, the ICD offers some insights into the etiological classification by diagnosis of health condition, disorder, or disease. Coupled with the ICF, both classification schemes offer a relatively full picture of the medical and biopsychosocial aspects of the individual (Stucki, 2012).
Because this chapter focuses on understanding the ICF and demonstrating its connection to assessment, a full understanding of the ICF is of value to the reader. The ICF is a hierarchical structure consisting of two parts, each with two components. Part 1, functioning and disability, is broken into the components (1) body functions and structures, and (2) activities and participation. Part 2, contextual factors, is broken into (1) environmental factors and (2) personal factors. (Note: Types of personal factors are identified for clarity but are not classified, because every person has unique personal factors and the classification of every person's personal factors would be impossible.) In the ICF, “Each component (except personal factors) can be expressed in both positive and negative terms” (WHO, 2001, p. 10).
The ICF
domains are classified from body, individual and societal perspectives by means of two lists: a list of body functions and structure, and a list of domains of activity and participation. In the ICF, the term functioning refers to all body functions, activities and participation. The term disability is similarly an umbrella term for impairments, activity limitations and participation restrictions. The ICF also lists environmental factors that interact with all these components. (WHO, 2002, p. 2)
The ICF is
a classification of health and health-related domains—domains that help us to describe changes in body function and structure, what a person with a health condition can do in a standard environment (their level of capacity), as well as what they actually do in their usual environment (their level of performance). (WHO, 2002, p. 2)
Let's break down these concepts in order to better understand the ICF. The ICF model, as shown in figure 3.1, offers a coding system that begins with the recognition of a health condition. As delineated in the ICF, a health condition (disorder or disease) generally affects some physical (biological) or functional aspect of the individual's body structure or body function. Changes or impacts on body structure—for example, a spinal cord injury, limb amputation, or even pregnancy or aging—may affect an individual's functioning in multiple domains. The affected body structure or function affects the activities and participation of the individual in the life of the community. In addition, environmental factors contextually affect the individual in a positive (facilitator) or negative (barrier) manner. Remember, since every person is unique, the ICF does not include personal factors in the classification system but does provide examples of factors to consider.
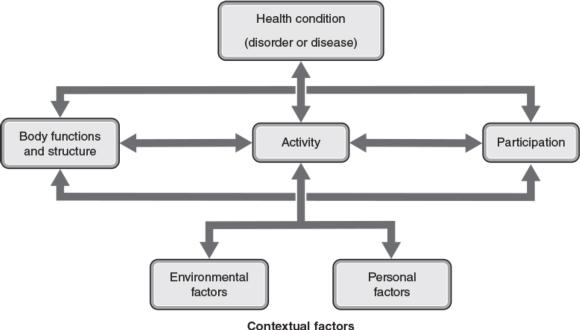
Figure 3.1 The ICF model.
Adapted by permission from International Classification of Functioning, Disability, and Health, pg. 18, copyright 2001 (Geneva, World Health Organization); Adapted from B. Prodinger et al., “Toward the ICF Rehabilitation Set: A Minimal Generic Set of Domains for Rehabilitation as a Health Strategy,” Archives of Physical Medicine and Rehabilitation 97, no. 6 (2016): 875-884.
The impact on body structure and body function has implications for the ability of the individual to engage in activities (execution of a task) and participation (engagement in the life of the community). It is important to note that the community may range from the broader environment (e.g., city or neighborhood) to home or residential facility.
Unlike what one may perceive from the term activities (e.g., a recreational event), activities under the ICF are more discrete. Activities within the ICF refer to the specific execution of a task like manipulating objects (i.e., holding a pencil), focusing attention, or walking on different surfaces. Participation, on the other hand, may include moving around within a facility or using transportation. Together, the concepts of activities and participation are a bit different within the ICF model than how they are often used within recreational therapy practice. In recreational therapy service delivery, we often think of an activity as a game or manual arts project or exercise in a group. In the ICF model, as noted, an activity may be grasping an object, balancing on a foot, or making a decision. If a consumer cannot grasp a paint brush, they will not be able to participate in a painting experience or event. Therefore, participation in a community art class may not be possible unless the therapist assists the consumer in acquiring the skill of grasping or making a modification. So, it is important to note that the ICF classifies the functional performance of the discrete tasks or actions needed to participate in life situations. As therapists, we want to be able to assess one's functioning in such discrete tasks so that we can improve the functioning, design adapted supplies, or modify the activity to enhance engagement (participation).
In addition to body structure, body function, and activities and participation, environmental and personal factors also affect the functioning of the individual. Environmental elements include products and technology, natural environment and human-made changes to the environment, support and relationships, attitudes of others, and services, systems, and policies. The qualities (or lack thereof) of the environment, including technology, affect the ability of an individual to address functioning (e.g., a prosthetic device) and, therefore, engagement in the life of the community (see figure 3.1). Remember that personal factors, such as gender, ethnicity, religious beliefs, cultural morays, and family upbringing, are not coded because every individual is unique.
To understand the model, a brief description of each element is of value. Table 3.1 offers an explanation/definition of each component of the ICF (Rauch, Luckenkemper, & Cieza, 2012; WHO, 2001). Unlike earlier linear models of disability, the ICF model is a dynamic and interactive model that reflects the functioning of the individual and recognizes the impacts of each element in an individual's life. Each component interacts with the other components depicting this dynamic relationship. For instance, when an individual's body structure is changed, there is a subsequent impact on body function, activities, and engagement in the life of the community. When an individual engages in an activity that improves body function or structure, there is a resulting impact on activities that may also affect participation in the community. The ICF is about classifying functioning and includes those environmental factors that can facilitate functioning and engagement or serve as barriers to one's functioning.
The following sections offer a brief explanation of each element of the ICF. It is important to recognize the dynamic relationship between each element and the resulting positive or negative impact on an individual. The health condition has an impact on body structure, body function, activities, participation, and environment functioning, each altering the functioning of the individual.
A snapshot of serving clients from diverse cultural backgrounds in a physical medicine setting
John is a 56-year-old male from Manila, Philippines. The primary language he speaks at home is Tagalog but he is also fluent in English.
By Marc Zaremski
Case Study
A Snapshot of Serving Clients From Diverse Cultural Backgrounds in a Physical Medicine Setting
Written by Marc Zaremski, MS, CTRS: Clemson University
John is a 56-year-old male from Manila, Philippines. The primary language he speaks at home is Tagalog but he is also fluent in English. John moved from Manila to Florida when he was 13 years old with his parents. John has remained in Florida and he currently lives with his wife and youngest daughter. John's wife speaks Tagalog and some English and his daughter is bilingual. John was working on his roof when he experienced a dizzy spell and fell backward off of the ladder, approximately 15 feet, landing on his driveway. John did not lose consciousness and an ambulance was called immediately once he expressed to his wife that he could not move his legs. John sustained fractures in several thoracic vertebrae from T8 to T12. At the T10 level, he sustained a complete spinal cord injury, resulting in paralysis below the T10 level. The ambulance took him to the local trauma center, where he underwent several procedures to stabilize the spinal cord and relieve pressure at the injury site. After John was deemed medically stable, he was transferred to ABC Rehabilitation to receive inpatient rehabilitation approximately seven days postoperative.
At ABC Rehabilitation, John's therapy and medical teams consist of only English-speaking therapists who are all non-Hispanic Caucasian. The facility offers a translation service, when available, which is a live video feed of a translator that can assist during therapy sessions, doctor's visits, and any other time a patient might need information translated to or from a provider. John initially feels comfortable but some aspects of the hospital begin to conflict with his culture. The constant cold temperature throughout the hospital is concerning to him because he believes warmth promotes good health. John's more traditional relatives have expressed concern over food, the treatment plan, and the temperature of the facility as well. A member of John's family is a babaylan, which is a form of healer that uses prayers, herbs, and massage or tissue manipulation as a healing method. John asked his physician and physical therapist if this family member could perform their healing rituals on him. They deemed it unwise because the family member is not a medical professional and John has many precautions. John was disappointed but eventually convinced the medical team to allow this healer to work with him. They agreed, as long as John informed the babaylan of his medical precautions to avoid further injury. The healer is not fluent in English and John had difficulties translating some of the medical terminology. The therapy team used the translation service to confirm that the healer and John understand the restrictions of the treatment. John and the healer articulated that they understood the precautions and John was able to participate in this healing session. John enjoyed the healing session and it put his more traditional family members at ease.
Throughout John's stay he experienced some frustrations and setbacks. Some frustrations were because of how his life had changed due to his injury and some were because of language barriers and a lack of specific cultural knowledge from health care providers. With the flexibility and extra effort of his health care professional, John overcame some of these issues to progress into being independent in his wheelchair and was deemed eligible to return home safely.
It is unrealistic to expect every health care provider to be knowledgeable on the cultural traditions and preferences of every client or patient. But it is important to utilize available resources to gain some insight into what our patients and clients prefer and to find compromise between those beliefs and the best possible medical care.
Applying ICF and Purnell's Stages of Cultural Competence
Based on Purnell's (2012) cultural competence milestones, the level of cultural competence of the physicians and physical therapist does not appear to reach to the cultural sensitivity stage, as evidenced by careless rejections of the healing rituals. They might have noticed that John's background is Filipino; however, they were not aware of how important it was to John and his family members for John to receive healing rituals. In order for physicians and physical therapists to reach a higher stage of cultural competence, the ICF framework is helpful. Personal factors of ICF allow them to look at the person's worldview and value system, beyond race and ethnicity. By understanding the client's values, professionals are more likely to seek ways to achieve things that are important to the person.
Implications for Recreational Therapy Practice
Working with patients or clients from different cultural backgrounds can provide some difficulties for professionals. But many of these difficulties can be resolved or mitigated with extra effort and preparation. Taking the time to look at the resources of your facility and how to access them is a great starting point for establishing a protocol for future clients. If there is admission data or another professional at the facility that may have seen this client first, talking to them can be useful for knowing what resources you may need to acquire. For example, if a patient is admitted who only speaks Spanish, that fact should appear in admission data or a member of the treatment team may inform you prior to you seeing them. This will enable you to schedule that patient when a translator, translation device, or family member that can translate is available. Scheduling appropriately, however, is not a static solution, so a backup plan should be established in case those resources are unavailable. Online translators can be useful for getting some basic translations to assist in your sessions. When all resources are unavailable, a list of key translated words to assist in administering the intervention for that day or for their length of stay may be required. It is difficult to coordinate translation services throughout an entire length of a patient's stay, so having these backup words can be vital for continuing quality service delivery.
Information on those you serve is vital for providing quality care. But it is also important to remember that something you may have found to be true for one patient may not be true for another, even if they have similar backgrounds. The Internet can be useful for finding information on cultures and their traditions, but it is safer to not to make assumptions. The best source of information on your client's beliefs, traditions, and background is typically from the client or their close family members and friends.
Being an active listener allows you to hear concerns that your client may have. This opens up an opportunity for recreational therapists to mitigate those concerns that could be making the client feel uncomfortable. For example, at some facilities, the recreational therapist may have the opportunity to do cooking or kitchen interventions. On occasion, a patient will have religious or cultural dietary restrictions and the food service department may not be meeting these needs. Members of the recreation department should perform functional cooking tasks with patients that meet their religious or cultural needs. This can make the patient or client feel more comfortable during their stay and assist other medical providers in meeting their goals for the client or patient.
When working with patients or clients from diverse cultural backgrounds, the best strategy for working with them can be broken down into four parts:
- Take extra time to gather and access resources.
- Utilize all available data and information.
- Listen to the patient and their caregiver(s) and family members.
- Work to minimize any of the client's concerns.
To help yourself, it can be beneficial to write down or keep stock of the resources and strategies that were most effective for a given scenario. Using these strategies, a solid foundation can be made to assist recreational therapists in better serving populations from diverse cultural backgrounds.
Questions for Consideration
- What strategies did the treatment team use in order to understand John?
- Based on the descriptions of John, to what extent was John culturally assimilated?
- Viewing this case study through an intersectionality lens, what sociodemographic variables might be helpful to understand John?
- If you were a member of John's therapy team, what would you do to implement cultural safety?
- In what way can practitioners move up the stages of cultural competence? How are ICF's personal factors helpful in the process?
Application of the assessment process with an individual with a physical disability
Bill is a 26-year-old with C6 quadriplegia. He completed three months of physical rehabilitation and has been living in the community with his wife for the past nine months.
By David P. Loy
Case Study
Application of the Assessment Process With an Individual With a Physical Disability
Bill is a 26-year-old with C6 quadriplegia. He completed three months of physical rehabilitation and has been living in the community with his wife for the past nine months. Bill heard about the recreational therapist working in his community and met with her to gain more independence and become more active since his discharge. Sarah Bellinger, a CTRS working in Bill's community, agreed to meet with Bill to conduct an assessment. She asked Bill if he could access his inpatient rehabilitation records or have them transferred to her in order to provide some preliminary information. During the initial meeting, Sarah performed a battery of assessments. She used a recreation interest survey to assess Bill's preferred recreation and leisure (d920) activities, a hand and finger dynamometer test for fine hand use (d440), the WST for mobility (d498), the CHART for community reintegration, and the modified functional reach test for vestibular balance (b240). The information indicates Bill has had limited recreation engagement (d920) since his SCI but expressed interest in sports and exercise (d9201) with a desire to get stronger so that he can progress from his power chair to a manual wheelchair. He has expressed a small fear of going in the community by himself because he doesn't have confidence in his skills. Hand and finger dynamometer readings indicate below average fine hand use (d440), but appropriate considering his spinal cord injury level. The WST test indicated a score of 19 (out of 66) for mobility (d498) and the CHART scores ranged from 18 to 32 in all five areas of CI. Answer the following questions based on this information.
- Discuss how the diagnosis of an SCI may have affected the CTRS's selection of assessment instruments.
- What are some appropriate treatment goals based on the interpretation of the assessment performance data provided?
- What are some preliminary interventions appropriate for Bill based on your interpretation of the assessment results?
Understanding the International Classification for Functioning, Disability and Health (ICF) model
To apply the coding of the ICF for effective service delivery, one needs to first understand how to utilize the ICF as a means to classify the full functioning of the individual, perhaps beginning with a diagnosis from the ICD-11.
By Thomas K. Skalko
Understanding the ICF Model
To apply the coding of the ICF for effective service delivery, one needs to first understand how to utilize the ICF as a means to classify the full functioning of the individual, perhaps beginning with a diagnosis from the ICD-11 (see www.who.int/classifications/icd/revision/icdprojectplan2015to2018.pdf?ua=1). The ICD-11 is a medical coding system for documenting diagnoses, signs of illness, symptoms of a condition, and social circumstances. Unlike the ICF, which focuses on functioning, the ICD offers some insights into the etiological classification by diagnosis of health condition, disorder, or disease. Coupled with the ICF, both classification schemes offer a relatively full picture of the medical and biopsychosocial aspects of the individual (Stucki, 2012).
Because this chapter focuses on understanding the ICF and demonstrating its connection to assessment, a full understanding of the ICF is of value to the reader. The ICF is a hierarchical structure consisting of two parts, each with two components. Part 1, functioning and disability, is broken into the components (1) body functions and structures, and (2) activities and participation. Part 2, contextual factors, is broken into (1) environmental factors and (2) personal factors. (Note: Types of personal factors are identified for clarity but are not classified, because every person has unique personal factors and the classification of every person's personal factors would be impossible.) In the ICF, “Each component (except personal factors) can be expressed in both positive and negative terms” (WHO, 2001, p. 10).
The ICF
domains are classified from body, individual and societal perspectives by means of two lists: a list of body functions and structure, and a list of domains of activity and participation. In the ICF, the term functioning refers to all body functions, activities and participation. The term disability is similarly an umbrella term for impairments, activity limitations and participation restrictions. The ICF also lists environmental factors that interact with all these components. (WHO, 2002, p. 2)
The ICF is
a classification of health and health-related domains—domains that help us to describe changes in body function and structure, what a person with a health condition can do in a standard environment (their level of capacity), as well as what they actually do in their usual environment (their level of performance). (WHO, 2002, p. 2)
Let's break down these concepts in order to better understand the ICF. The ICF model, as shown in figure 3.1, offers a coding system that begins with the recognition of a health condition. As delineated in the ICF, a health condition (disorder or disease) generally affects some physical (biological) or functional aspect of the individual's body structure or body function. Changes or impacts on body structure—for example, a spinal cord injury, limb amputation, or even pregnancy or aging—may affect an individual's functioning in multiple domains. The affected body structure or function affects the activities and participation of the individual in the life of the community. In addition, environmental factors contextually affect the individual in a positive (facilitator) or negative (barrier) manner. Remember, since every person is unique, the ICF does not include personal factors in the classification system but does provide examples of factors to consider.
Figure 3.1 The ICF model.
Adapted by permission from International Classification of Functioning, Disability, and Health, pg. 18, copyright 2001 (Geneva, World Health Organization); Adapted from B. Prodinger et al., “Toward the ICF Rehabilitation Set: A Minimal Generic Set of Domains for Rehabilitation as a Health Strategy,” Archives of Physical Medicine and Rehabilitation 97, no. 6 (2016): 875-884.
The impact on body structure and body function has implications for the ability of the individual to engage in activities (execution of a task) and participation (engagement in the life of the community). It is important to note that the community may range from the broader environment (e.g., city or neighborhood) to home or residential facility.
Unlike what one may perceive from the term activities (e.g., a recreational event), activities under the ICF are more discrete. Activities within the ICF refer to the specific execution of a task like manipulating objects (i.e., holding a pencil), focusing attention, or walking on different surfaces. Participation, on the other hand, may include moving around within a facility or using transportation. Together, the concepts of activities and participation are a bit different within the ICF model than how they are often used within recreational therapy practice. In recreational therapy service delivery, we often think of an activity as a game or manual arts project or exercise in a group. In the ICF model, as noted, an activity may be grasping an object, balancing on a foot, or making a decision. If a consumer cannot grasp a paint brush, they will not be able to participate in a painting experience or event. Therefore, participation in a community art class may not be possible unless the therapist assists the consumer in acquiring the skill of grasping or making a modification. So, it is important to note that the ICF classifies the functional performance of the discrete tasks or actions needed to participate in life situations. As therapists, we want to be able to assess one's functioning in such discrete tasks so that we can improve the functioning, design adapted supplies, or modify the activity to enhance engagement (participation).
In addition to body structure, body function, and activities and participation, environmental and personal factors also affect the functioning of the individual. Environmental elements include products and technology, natural environment and human-made changes to the environment, support and relationships, attitudes of others, and services, systems, and policies. The qualities (or lack thereof) of the environment, including technology, affect the ability of an individual to address functioning (e.g., a prosthetic device) and, therefore, engagement in the life of the community (see figure 3.1). Remember that personal factors, such as gender, ethnicity, religious beliefs, cultural morays, and family upbringing, are not coded because every individual is unique.
To understand the model, a brief description of each element is of value. Table 3.1 offers an explanation/definition of each component of the ICF (Rauch, Luckenkemper, & Cieza, 2012; WHO, 2001). Unlike earlier linear models of disability, the ICF model is a dynamic and interactive model that reflects the functioning of the individual and recognizes the impacts of each element in an individual's life. Each component interacts with the other components depicting this dynamic relationship. For instance, when an individual's body structure is changed, there is a subsequent impact on body function, activities, and engagement in the life of the community. When an individual engages in an activity that improves body function or structure, there is a resulting impact on activities that may also affect participation in the community. The ICF is about classifying functioning and includes those environmental factors that can facilitate functioning and engagement or serve as barriers to one's functioning.
The following sections offer a brief explanation of each element of the ICF. It is important to recognize the dynamic relationship between each element and the resulting positive or negative impact on an individual. The health condition has an impact on body structure, body function, activities, participation, and environment functioning, each altering the functioning of the individual.
A snapshot of serving clients from diverse cultural backgrounds in a physical medicine setting
John is a 56-year-old male from Manila, Philippines. The primary language he speaks at home is Tagalog but he is also fluent in English.
By Marc Zaremski
Case Study
A Snapshot of Serving Clients From Diverse Cultural Backgrounds in a Physical Medicine Setting
Written by Marc Zaremski, MS, CTRS: Clemson University
John is a 56-year-old male from Manila, Philippines. The primary language he speaks at home is Tagalog but he is also fluent in English. John moved from Manila to Florida when he was 13 years old with his parents. John has remained in Florida and he currently lives with his wife and youngest daughter. John's wife speaks Tagalog and some English and his daughter is bilingual. John was working on his roof when he experienced a dizzy spell and fell backward off of the ladder, approximately 15 feet, landing on his driveway. John did not lose consciousness and an ambulance was called immediately once he expressed to his wife that he could not move his legs. John sustained fractures in several thoracic vertebrae from T8 to T12. At the T10 level, he sustained a complete spinal cord injury, resulting in paralysis below the T10 level. The ambulance took him to the local trauma center, where he underwent several procedures to stabilize the spinal cord and relieve pressure at the injury site. After John was deemed medically stable, he was transferred to ABC Rehabilitation to receive inpatient rehabilitation approximately seven days postoperative.
At ABC Rehabilitation, John's therapy and medical teams consist of only English-speaking therapists who are all non-Hispanic Caucasian. The facility offers a translation service, when available, which is a live video feed of a translator that can assist during therapy sessions, doctor's visits, and any other time a patient might need information translated to or from a provider. John initially feels comfortable but some aspects of the hospital begin to conflict with his culture. The constant cold temperature throughout the hospital is concerning to him because he believes warmth promotes good health. John's more traditional relatives have expressed concern over food, the treatment plan, and the temperature of the facility as well. A member of John's family is a babaylan, which is a form of healer that uses prayers, herbs, and massage or tissue manipulation as a healing method. John asked his physician and physical therapist if this family member could perform their healing rituals on him. They deemed it unwise because the family member is not a medical professional and John has many precautions. John was disappointed but eventually convinced the medical team to allow this healer to work with him. They agreed, as long as John informed the babaylan of his medical precautions to avoid further injury. The healer is not fluent in English and John had difficulties translating some of the medical terminology. The therapy team used the translation service to confirm that the healer and John understand the restrictions of the treatment. John and the healer articulated that they understood the precautions and John was able to participate in this healing session. John enjoyed the healing session and it put his more traditional family members at ease.
Throughout John's stay he experienced some frustrations and setbacks. Some frustrations were because of how his life had changed due to his injury and some were because of language barriers and a lack of specific cultural knowledge from health care providers. With the flexibility and extra effort of his health care professional, John overcame some of these issues to progress into being independent in his wheelchair and was deemed eligible to return home safely.
It is unrealistic to expect every health care provider to be knowledgeable on the cultural traditions and preferences of every client or patient. But it is important to utilize available resources to gain some insight into what our patients and clients prefer and to find compromise between those beliefs and the best possible medical care.
Applying ICF and Purnell's Stages of Cultural Competence
Based on Purnell's (2012) cultural competence milestones, the level of cultural competence of the physicians and physical therapist does not appear to reach to the cultural sensitivity stage, as evidenced by careless rejections of the healing rituals. They might have noticed that John's background is Filipino; however, they were not aware of how important it was to John and his family members for John to receive healing rituals. In order for physicians and physical therapists to reach a higher stage of cultural competence, the ICF framework is helpful. Personal factors of ICF allow them to look at the person's worldview and value system, beyond race and ethnicity. By understanding the client's values, professionals are more likely to seek ways to achieve things that are important to the person.
Implications for Recreational Therapy Practice
Working with patients or clients from different cultural backgrounds can provide some difficulties for professionals. But many of these difficulties can be resolved or mitigated with extra effort and preparation. Taking the time to look at the resources of your facility and how to access them is a great starting point for establishing a protocol for future clients. If there is admission data or another professional at the facility that may have seen this client first, talking to them can be useful for knowing what resources you may need to acquire. For example, if a patient is admitted who only speaks Spanish, that fact should appear in admission data or a member of the treatment team may inform you prior to you seeing them. This will enable you to schedule that patient when a translator, translation device, or family member that can translate is available. Scheduling appropriately, however, is not a static solution, so a backup plan should be established in case those resources are unavailable. Online translators can be useful for getting some basic translations to assist in your sessions. When all resources are unavailable, a list of key translated words to assist in administering the intervention for that day or for their length of stay may be required. It is difficult to coordinate translation services throughout an entire length of a patient's stay, so having these backup words can be vital for continuing quality service delivery.
Information on those you serve is vital for providing quality care. But it is also important to remember that something you may have found to be true for one patient may not be true for another, even if they have similar backgrounds. The Internet can be useful for finding information on cultures and their traditions, but it is safer to not to make assumptions. The best source of information on your client's beliefs, traditions, and background is typically from the client or their close family members and friends.
Being an active listener allows you to hear concerns that your client may have. This opens up an opportunity for recreational therapists to mitigate those concerns that could be making the client feel uncomfortable. For example, at some facilities, the recreational therapist may have the opportunity to do cooking or kitchen interventions. On occasion, a patient will have religious or cultural dietary restrictions and the food service department may not be meeting these needs. Members of the recreation department should perform functional cooking tasks with patients that meet their religious or cultural needs. This can make the patient or client feel more comfortable during their stay and assist other medical providers in meeting their goals for the client or patient.
When working with patients or clients from diverse cultural backgrounds, the best strategy for working with them can be broken down into four parts:
- Take extra time to gather and access resources.
- Utilize all available data and information.
- Listen to the patient and their caregiver(s) and family members.
- Work to minimize any of the client's concerns.
To help yourself, it can be beneficial to write down or keep stock of the resources and strategies that were most effective for a given scenario. Using these strategies, a solid foundation can be made to assist recreational therapists in better serving populations from diverse cultural backgrounds.
Questions for Consideration
- What strategies did the treatment team use in order to understand John?
- Based on the descriptions of John, to what extent was John culturally assimilated?
- Viewing this case study through an intersectionality lens, what sociodemographic variables might be helpful to understand John?
- If you were a member of John's therapy team, what would you do to implement cultural safety?
- In what way can practitioners move up the stages of cultural competence? How are ICF's personal factors helpful in the process?
Application of the assessment process with an individual with a physical disability
Bill is a 26-year-old with C6 quadriplegia. He completed three months of physical rehabilitation and has been living in the community with his wife for the past nine months.
By David P. Loy
Case Study
Application of the Assessment Process With an Individual With a Physical Disability
Bill is a 26-year-old with C6 quadriplegia. He completed three months of physical rehabilitation and has been living in the community with his wife for the past nine months. Bill heard about the recreational therapist working in his community and met with her to gain more independence and become more active since his discharge. Sarah Bellinger, a CTRS working in Bill's community, agreed to meet with Bill to conduct an assessment. She asked Bill if he could access his inpatient rehabilitation records or have them transferred to her in order to provide some preliminary information. During the initial meeting, Sarah performed a battery of assessments. She used a recreation interest survey to assess Bill's preferred recreation and leisure (d920) activities, a hand and finger dynamometer test for fine hand use (d440), the WST for mobility (d498), the CHART for community reintegration, and the modified functional reach test for vestibular balance (b240). The information indicates Bill has had limited recreation engagement (d920) since his SCI but expressed interest in sports and exercise (d9201) with a desire to get stronger so that he can progress from his power chair to a manual wheelchair. He has expressed a small fear of going in the community by himself because he doesn't have confidence in his skills. Hand and finger dynamometer readings indicate below average fine hand use (d440), but appropriate considering his spinal cord injury level. The WST test indicated a score of 19 (out of 66) for mobility (d498) and the CHART scores ranged from 18 to 32 in all five areas of CI. Answer the following questions based on this information.
- Discuss how the diagnosis of an SCI may have affected the CTRS's selection of assessment instruments.
- What are some appropriate treatment goals based on the interpretation of the assessment performance data provided?
- What are some preliminary interventions appropriate for Bill based on your interpretation of the assessment results?
Understanding the International Classification for Functioning, Disability and Health (ICF) model
To apply the coding of the ICF for effective service delivery, one needs to first understand how to utilize the ICF as a means to classify the full functioning of the individual, perhaps beginning with a diagnosis from the ICD-11.
By Thomas K. Skalko
Understanding the ICF Model
To apply the coding of the ICF for effective service delivery, one needs to first understand how to utilize the ICF as a means to classify the full functioning of the individual, perhaps beginning with a diagnosis from the ICD-11 (see www.who.int/classifications/icd/revision/icdprojectplan2015to2018.pdf?ua=1). The ICD-11 is a medical coding system for documenting diagnoses, signs of illness, symptoms of a condition, and social circumstances. Unlike the ICF, which focuses on functioning, the ICD offers some insights into the etiological classification by diagnosis of health condition, disorder, or disease. Coupled with the ICF, both classification schemes offer a relatively full picture of the medical and biopsychosocial aspects of the individual (Stucki, 2012).
Because this chapter focuses on understanding the ICF and demonstrating its connection to assessment, a full understanding of the ICF is of value to the reader. The ICF is a hierarchical structure consisting of two parts, each with two components. Part 1, functioning and disability, is broken into the components (1) body functions and structures, and (2) activities and participation. Part 2, contextual factors, is broken into (1) environmental factors and (2) personal factors. (Note: Types of personal factors are identified for clarity but are not classified, because every person has unique personal factors and the classification of every person's personal factors would be impossible.) In the ICF, “Each component (except personal factors) can be expressed in both positive and negative terms” (WHO, 2001, p. 10).
The ICF
domains are classified from body, individual and societal perspectives by means of two lists: a list of body functions and structure, and a list of domains of activity and participation. In the ICF, the term functioning refers to all body functions, activities and participation. The term disability is similarly an umbrella term for impairments, activity limitations and participation restrictions. The ICF also lists environmental factors that interact with all these components. (WHO, 2002, p. 2)
The ICF is
a classification of health and health-related domains—domains that help us to describe changes in body function and structure, what a person with a health condition can do in a standard environment (their level of capacity), as well as what they actually do in their usual environment (their level of performance). (WHO, 2002, p. 2)
Let's break down these concepts in order to better understand the ICF. The ICF model, as shown in figure 3.1, offers a coding system that begins with the recognition of a health condition. As delineated in the ICF, a health condition (disorder or disease) generally affects some physical (biological) or functional aspect of the individual's body structure or body function. Changes or impacts on body structure—for example, a spinal cord injury, limb amputation, or even pregnancy or aging—may affect an individual's functioning in multiple domains. The affected body structure or function affects the activities and participation of the individual in the life of the community. In addition, environmental factors contextually affect the individual in a positive (facilitator) or negative (barrier) manner. Remember, since every person is unique, the ICF does not include personal factors in the classification system but does provide examples of factors to consider.
Figure 3.1 The ICF model.
Adapted by permission from International Classification of Functioning, Disability, and Health, pg. 18, copyright 2001 (Geneva, World Health Organization); Adapted from B. Prodinger et al., “Toward the ICF Rehabilitation Set: A Minimal Generic Set of Domains for Rehabilitation as a Health Strategy,” Archives of Physical Medicine and Rehabilitation 97, no. 6 (2016): 875-884.
The impact on body structure and body function has implications for the ability of the individual to engage in activities (execution of a task) and participation (engagement in the life of the community). It is important to note that the community may range from the broader environment (e.g., city or neighborhood) to home or residential facility.
Unlike what one may perceive from the term activities (e.g., a recreational event), activities under the ICF are more discrete. Activities within the ICF refer to the specific execution of a task like manipulating objects (i.e., holding a pencil), focusing attention, or walking on different surfaces. Participation, on the other hand, may include moving around within a facility or using transportation. Together, the concepts of activities and participation are a bit different within the ICF model than how they are often used within recreational therapy practice. In recreational therapy service delivery, we often think of an activity as a game or manual arts project or exercise in a group. In the ICF model, as noted, an activity may be grasping an object, balancing on a foot, or making a decision. If a consumer cannot grasp a paint brush, they will not be able to participate in a painting experience or event. Therefore, participation in a community art class may not be possible unless the therapist assists the consumer in acquiring the skill of grasping or making a modification. So, it is important to note that the ICF classifies the functional performance of the discrete tasks or actions needed to participate in life situations. As therapists, we want to be able to assess one's functioning in such discrete tasks so that we can improve the functioning, design adapted supplies, or modify the activity to enhance engagement (participation).
In addition to body structure, body function, and activities and participation, environmental and personal factors also affect the functioning of the individual. Environmental elements include products and technology, natural environment and human-made changes to the environment, support and relationships, attitudes of others, and services, systems, and policies. The qualities (or lack thereof) of the environment, including technology, affect the ability of an individual to address functioning (e.g., a prosthetic device) and, therefore, engagement in the life of the community (see figure 3.1). Remember that personal factors, such as gender, ethnicity, religious beliefs, cultural morays, and family upbringing, are not coded because every individual is unique.
To understand the model, a brief description of each element is of value. Table 3.1 offers an explanation/definition of each component of the ICF (Rauch, Luckenkemper, & Cieza, 2012; WHO, 2001). Unlike earlier linear models of disability, the ICF model is a dynamic and interactive model that reflects the functioning of the individual and recognizes the impacts of each element in an individual's life. Each component interacts with the other components depicting this dynamic relationship. For instance, when an individual's body structure is changed, there is a subsequent impact on body function, activities, and engagement in the life of the community. When an individual engages in an activity that improves body function or structure, there is a resulting impact on activities that may also affect participation in the community. The ICF is about classifying functioning and includes those environmental factors that can facilitate functioning and engagement or serve as barriers to one's functioning.
The following sections offer a brief explanation of each element of the ICF. It is important to recognize the dynamic relationship between each element and the resulting positive or negative impact on an individual. The health condition has an impact on body structure, body function, activities, participation, and environment functioning, each altering the functioning of the individual.
A snapshot of serving clients from diverse cultural backgrounds in a physical medicine setting
John is a 56-year-old male from Manila, Philippines. The primary language he speaks at home is Tagalog but he is also fluent in English.
By Marc Zaremski
Case Study
A Snapshot of Serving Clients From Diverse Cultural Backgrounds in a Physical Medicine Setting
Written by Marc Zaremski, MS, CTRS: Clemson University
John is a 56-year-old male from Manila, Philippines. The primary language he speaks at home is Tagalog but he is also fluent in English. John moved from Manila to Florida when he was 13 years old with his parents. John has remained in Florida and he currently lives with his wife and youngest daughter. John's wife speaks Tagalog and some English and his daughter is bilingual. John was working on his roof when he experienced a dizzy spell and fell backward off of the ladder, approximately 15 feet, landing on his driveway. John did not lose consciousness and an ambulance was called immediately once he expressed to his wife that he could not move his legs. John sustained fractures in several thoracic vertebrae from T8 to T12. At the T10 level, he sustained a complete spinal cord injury, resulting in paralysis below the T10 level. The ambulance took him to the local trauma center, where he underwent several procedures to stabilize the spinal cord and relieve pressure at the injury site. After John was deemed medically stable, he was transferred to ABC Rehabilitation to receive inpatient rehabilitation approximately seven days postoperative.
At ABC Rehabilitation, John's therapy and medical teams consist of only English-speaking therapists who are all non-Hispanic Caucasian. The facility offers a translation service, when available, which is a live video feed of a translator that can assist during therapy sessions, doctor's visits, and any other time a patient might need information translated to or from a provider. John initially feels comfortable but some aspects of the hospital begin to conflict with his culture. The constant cold temperature throughout the hospital is concerning to him because he believes warmth promotes good health. John's more traditional relatives have expressed concern over food, the treatment plan, and the temperature of the facility as well. A member of John's family is a babaylan, which is a form of healer that uses prayers, herbs, and massage or tissue manipulation as a healing method. John asked his physician and physical therapist if this family member could perform their healing rituals on him. They deemed it unwise because the family member is not a medical professional and John has many precautions. John was disappointed but eventually convinced the medical team to allow this healer to work with him. They agreed, as long as John informed the babaylan of his medical precautions to avoid further injury. The healer is not fluent in English and John had difficulties translating some of the medical terminology. The therapy team used the translation service to confirm that the healer and John understand the restrictions of the treatment. John and the healer articulated that they understood the precautions and John was able to participate in this healing session. John enjoyed the healing session and it put his more traditional family members at ease.
Throughout John's stay he experienced some frustrations and setbacks. Some frustrations were because of how his life had changed due to his injury and some were because of language barriers and a lack of specific cultural knowledge from health care providers. With the flexibility and extra effort of his health care professional, John overcame some of these issues to progress into being independent in his wheelchair and was deemed eligible to return home safely.
It is unrealistic to expect every health care provider to be knowledgeable on the cultural traditions and preferences of every client or patient. But it is important to utilize available resources to gain some insight into what our patients and clients prefer and to find compromise between those beliefs and the best possible medical care.
Applying ICF and Purnell's Stages of Cultural Competence
Based on Purnell's (2012) cultural competence milestones, the level of cultural competence of the physicians and physical therapist does not appear to reach to the cultural sensitivity stage, as evidenced by careless rejections of the healing rituals. They might have noticed that John's background is Filipino; however, they were not aware of how important it was to John and his family members for John to receive healing rituals. In order for physicians and physical therapists to reach a higher stage of cultural competence, the ICF framework is helpful. Personal factors of ICF allow them to look at the person's worldview and value system, beyond race and ethnicity. By understanding the client's values, professionals are more likely to seek ways to achieve things that are important to the person.
Implications for Recreational Therapy Practice
Working with patients or clients from different cultural backgrounds can provide some difficulties for professionals. But many of these difficulties can be resolved or mitigated with extra effort and preparation. Taking the time to look at the resources of your facility and how to access them is a great starting point for establishing a protocol for future clients. If there is admission data or another professional at the facility that may have seen this client first, talking to them can be useful for knowing what resources you may need to acquire. For example, if a patient is admitted who only speaks Spanish, that fact should appear in admission data or a member of the treatment team may inform you prior to you seeing them. This will enable you to schedule that patient when a translator, translation device, or family member that can translate is available. Scheduling appropriately, however, is not a static solution, so a backup plan should be established in case those resources are unavailable. Online translators can be useful for getting some basic translations to assist in your sessions. When all resources are unavailable, a list of key translated words to assist in administering the intervention for that day or for their length of stay may be required. It is difficult to coordinate translation services throughout an entire length of a patient's stay, so having these backup words can be vital for continuing quality service delivery.
Information on those you serve is vital for providing quality care. But it is also important to remember that something you may have found to be true for one patient may not be true for another, even if they have similar backgrounds. The Internet can be useful for finding information on cultures and their traditions, but it is safer to not to make assumptions. The best source of information on your client's beliefs, traditions, and background is typically from the client or their close family members and friends.
Being an active listener allows you to hear concerns that your client may have. This opens up an opportunity for recreational therapists to mitigate those concerns that could be making the client feel uncomfortable. For example, at some facilities, the recreational therapist may have the opportunity to do cooking or kitchen interventions. On occasion, a patient will have religious or cultural dietary restrictions and the food service department may not be meeting these needs. Members of the recreation department should perform functional cooking tasks with patients that meet their religious or cultural needs. This can make the patient or client feel more comfortable during their stay and assist other medical providers in meeting their goals for the client or patient.
When working with patients or clients from diverse cultural backgrounds, the best strategy for working with them can be broken down into four parts:
- Take extra time to gather and access resources.
- Utilize all available data and information.
- Listen to the patient and their caregiver(s) and family members.
- Work to minimize any of the client's concerns.
To help yourself, it can be beneficial to write down or keep stock of the resources and strategies that were most effective for a given scenario. Using these strategies, a solid foundation can be made to assist recreational therapists in better serving populations from diverse cultural backgrounds.
Questions for Consideration
- What strategies did the treatment team use in order to understand John?
- Based on the descriptions of John, to what extent was John culturally assimilated?
- Viewing this case study through an intersectionality lens, what sociodemographic variables might be helpful to understand John?
- If you were a member of John's therapy team, what would you do to implement cultural safety?
- In what way can practitioners move up the stages of cultural competence? How are ICF's personal factors helpful in the process?
Application of the assessment process with an individual with a physical disability
Bill is a 26-year-old with C6 quadriplegia. He completed three months of physical rehabilitation and has been living in the community with his wife for the past nine months.
By David P. Loy
Case Study
Application of the Assessment Process With an Individual With a Physical Disability
Bill is a 26-year-old with C6 quadriplegia. He completed three months of physical rehabilitation and has been living in the community with his wife for the past nine months. Bill heard about the recreational therapist working in his community and met with her to gain more independence and become more active since his discharge. Sarah Bellinger, a CTRS working in Bill's community, agreed to meet with Bill to conduct an assessment. She asked Bill if he could access his inpatient rehabilitation records or have them transferred to her in order to provide some preliminary information. During the initial meeting, Sarah performed a battery of assessments. She used a recreation interest survey to assess Bill's preferred recreation and leisure (d920) activities, a hand and finger dynamometer test for fine hand use (d440), the WST for mobility (d498), the CHART for community reintegration, and the modified functional reach test for vestibular balance (b240). The information indicates Bill has had limited recreation engagement (d920) since his SCI but expressed interest in sports and exercise (d9201) with a desire to get stronger so that he can progress from his power chair to a manual wheelchair. He has expressed a small fear of going in the community by himself because he doesn't have confidence in his skills. Hand and finger dynamometer readings indicate below average fine hand use (d440), but appropriate considering his spinal cord injury level. The WST test indicated a score of 19 (out of 66) for mobility (d498) and the CHART scores ranged from 18 to 32 in all five areas of CI. Answer the following questions based on this information.
- Discuss how the diagnosis of an SCI may have affected the CTRS's selection of assessment instruments.
- What are some appropriate treatment goals based on the interpretation of the assessment performance data provided?
- What are some preliminary interventions appropriate for Bill based on your interpretation of the assessment results?
Understanding the International Classification for Functioning, Disability and Health (ICF) model
To apply the coding of the ICF for effective service delivery, one needs to first understand how to utilize the ICF as a means to classify the full functioning of the individual, perhaps beginning with a diagnosis from the ICD-11.
By Thomas K. Skalko
Understanding the ICF Model
To apply the coding of the ICF for effective service delivery, one needs to first understand how to utilize the ICF as a means to classify the full functioning of the individual, perhaps beginning with a diagnosis from the ICD-11 (see www.who.int/classifications/icd/revision/icdprojectplan2015to2018.pdf?ua=1). The ICD-11 is a medical coding system for documenting diagnoses, signs of illness, symptoms of a condition, and social circumstances. Unlike the ICF, which focuses on functioning, the ICD offers some insights into the etiological classification by diagnosis of health condition, disorder, or disease. Coupled with the ICF, both classification schemes offer a relatively full picture of the medical and biopsychosocial aspects of the individual (Stucki, 2012).
Because this chapter focuses on understanding the ICF and demonstrating its connection to assessment, a full understanding of the ICF is of value to the reader. The ICF is a hierarchical structure consisting of two parts, each with two components. Part 1, functioning and disability, is broken into the components (1) body functions and structures, and (2) activities and participation. Part 2, contextual factors, is broken into (1) environmental factors and (2) personal factors. (Note: Types of personal factors are identified for clarity but are not classified, because every person has unique personal factors and the classification of every person's personal factors would be impossible.) In the ICF, “Each component (except personal factors) can be expressed in both positive and negative terms” (WHO, 2001, p. 10).
The ICF
domains are classified from body, individual and societal perspectives by means of two lists: a list of body functions and structure, and a list of domains of activity and participation. In the ICF, the term functioning refers to all body functions, activities and participation. The term disability is similarly an umbrella term for impairments, activity limitations and participation restrictions. The ICF also lists environmental factors that interact with all these components. (WHO, 2002, p. 2)
The ICF is
a classification of health and health-related domains—domains that help us to describe changes in body function and structure, what a person with a health condition can do in a standard environment (their level of capacity), as well as what they actually do in their usual environment (their level of performance). (WHO, 2002, p. 2)
Let's break down these concepts in order to better understand the ICF. The ICF model, as shown in figure 3.1, offers a coding system that begins with the recognition of a health condition. As delineated in the ICF, a health condition (disorder or disease) generally affects some physical (biological) or functional aspect of the individual's body structure or body function. Changes or impacts on body structure—for example, a spinal cord injury, limb amputation, or even pregnancy or aging—may affect an individual's functioning in multiple domains. The affected body structure or function affects the activities and participation of the individual in the life of the community. In addition, environmental factors contextually affect the individual in a positive (facilitator) or negative (barrier) manner. Remember, since every person is unique, the ICF does not include personal factors in the classification system but does provide examples of factors to consider.
Figure 3.1 The ICF model.
Adapted by permission from International Classification of Functioning, Disability, and Health, pg. 18, copyright 2001 (Geneva, World Health Organization); Adapted from B. Prodinger et al., “Toward the ICF Rehabilitation Set: A Minimal Generic Set of Domains for Rehabilitation as a Health Strategy,” Archives of Physical Medicine and Rehabilitation 97, no. 6 (2016): 875-884.
The impact on body structure and body function has implications for the ability of the individual to engage in activities (execution of a task) and participation (engagement in the life of the community). It is important to note that the community may range from the broader environment (e.g., city or neighborhood) to home or residential facility.
Unlike what one may perceive from the term activities (e.g., a recreational event), activities under the ICF are more discrete. Activities within the ICF refer to the specific execution of a task like manipulating objects (i.e., holding a pencil), focusing attention, or walking on different surfaces. Participation, on the other hand, may include moving around within a facility or using transportation. Together, the concepts of activities and participation are a bit different within the ICF model than how they are often used within recreational therapy practice. In recreational therapy service delivery, we often think of an activity as a game or manual arts project or exercise in a group. In the ICF model, as noted, an activity may be grasping an object, balancing on a foot, or making a decision. If a consumer cannot grasp a paint brush, they will not be able to participate in a painting experience or event. Therefore, participation in a community art class may not be possible unless the therapist assists the consumer in acquiring the skill of grasping or making a modification. So, it is important to note that the ICF classifies the functional performance of the discrete tasks or actions needed to participate in life situations. As therapists, we want to be able to assess one's functioning in such discrete tasks so that we can improve the functioning, design adapted supplies, or modify the activity to enhance engagement (participation).
In addition to body structure, body function, and activities and participation, environmental and personal factors also affect the functioning of the individual. Environmental elements include products and technology, natural environment and human-made changes to the environment, support and relationships, attitudes of others, and services, systems, and policies. The qualities (or lack thereof) of the environment, including technology, affect the ability of an individual to address functioning (e.g., a prosthetic device) and, therefore, engagement in the life of the community (see figure 3.1). Remember that personal factors, such as gender, ethnicity, religious beliefs, cultural morays, and family upbringing, are not coded because every individual is unique.
To understand the model, a brief description of each element is of value. Table 3.1 offers an explanation/definition of each component of the ICF (Rauch, Luckenkemper, & Cieza, 2012; WHO, 2001). Unlike earlier linear models of disability, the ICF model is a dynamic and interactive model that reflects the functioning of the individual and recognizes the impacts of each element in an individual's life. Each component interacts with the other components depicting this dynamic relationship. For instance, when an individual's body structure is changed, there is a subsequent impact on body function, activities, and engagement in the life of the community. When an individual engages in an activity that improves body function or structure, there is a resulting impact on activities that may also affect participation in the community. The ICF is about classifying functioning and includes those environmental factors that can facilitate functioning and engagement or serve as barriers to one's functioning.
The following sections offer a brief explanation of each element of the ICF. It is important to recognize the dynamic relationship between each element and the resulting positive or negative impact on an individual. The health condition has an impact on body structure, body function, activities, participation, and environment functioning, each altering the functioning of the individual.
A snapshot of serving clients from diverse cultural backgrounds in a physical medicine setting
John is a 56-year-old male from Manila, Philippines. The primary language he speaks at home is Tagalog but he is also fluent in English.
By Marc Zaremski
Case Study
A Snapshot of Serving Clients From Diverse Cultural Backgrounds in a Physical Medicine Setting
Written by Marc Zaremski, MS, CTRS: Clemson University
John is a 56-year-old male from Manila, Philippines. The primary language he speaks at home is Tagalog but he is also fluent in English. John moved from Manila to Florida when he was 13 years old with his parents. John has remained in Florida and he currently lives with his wife and youngest daughter. John's wife speaks Tagalog and some English and his daughter is bilingual. John was working on his roof when he experienced a dizzy spell and fell backward off of the ladder, approximately 15 feet, landing on his driveway. John did not lose consciousness and an ambulance was called immediately once he expressed to his wife that he could not move his legs. John sustained fractures in several thoracic vertebrae from T8 to T12. At the T10 level, he sustained a complete spinal cord injury, resulting in paralysis below the T10 level. The ambulance took him to the local trauma center, where he underwent several procedures to stabilize the spinal cord and relieve pressure at the injury site. After John was deemed medically stable, he was transferred to ABC Rehabilitation to receive inpatient rehabilitation approximately seven days postoperative.
At ABC Rehabilitation, John's therapy and medical teams consist of only English-speaking therapists who are all non-Hispanic Caucasian. The facility offers a translation service, when available, which is a live video feed of a translator that can assist during therapy sessions, doctor's visits, and any other time a patient might need information translated to or from a provider. John initially feels comfortable but some aspects of the hospital begin to conflict with his culture. The constant cold temperature throughout the hospital is concerning to him because he believes warmth promotes good health. John's more traditional relatives have expressed concern over food, the treatment plan, and the temperature of the facility as well. A member of John's family is a babaylan, which is a form of healer that uses prayers, herbs, and massage or tissue manipulation as a healing method. John asked his physician and physical therapist if this family member could perform their healing rituals on him. They deemed it unwise because the family member is not a medical professional and John has many precautions. John was disappointed but eventually convinced the medical team to allow this healer to work with him. They agreed, as long as John informed the babaylan of his medical precautions to avoid further injury. The healer is not fluent in English and John had difficulties translating some of the medical terminology. The therapy team used the translation service to confirm that the healer and John understand the restrictions of the treatment. John and the healer articulated that they understood the precautions and John was able to participate in this healing session. John enjoyed the healing session and it put his more traditional family members at ease.
Throughout John's stay he experienced some frustrations and setbacks. Some frustrations were because of how his life had changed due to his injury and some were because of language barriers and a lack of specific cultural knowledge from health care providers. With the flexibility and extra effort of his health care professional, John overcame some of these issues to progress into being independent in his wheelchair and was deemed eligible to return home safely.
It is unrealistic to expect every health care provider to be knowledgeable on the cultural traditions and preferences of every client or patient. But it is important to utilize available resources to gain some insight into what our patients and clients prefer and to find compromise between those beliefs and the best possible medical care.
Applying ICF and Purnell's Stages of Cultural Competence
Based on Purnell's (2012) cultural competence milestones, the level of cultural competence of the physicians and physical therapist does not appear to reach to the cultural sensitivity stage, as evidenced by careless rejections of the healing rituals. They might have noticed that John's background is Filipino; however, they were not aware of how important it was to John and his family members for John to receive healing rituals. In order for physicians and physical therapists to reach a higher stage of cultural competence, the ICF framework is helpful. Personal factors of ICF allow them to look at the person's worldview and value system, beyond race and ethnicity. By understanding the client's values, professionals are more likely to seek ways to achieve things that are important to the person.
Implications for Recreational Therapy Practice
Working with patients or clients from different cultural backgrounds can provide some difficulties for professionals. But many of these difficulties can be resolved or mitigated with extra effort and preparation. Taking the time to look at the resources of your facility and how to access them is a great starting point for establishing a protocol for future clients. If there is admission data or another professional at the facility that may have seen this client first, talking to them can be useful for knowing what resources you may need to acquire. For example, if a patient is admitted who only speaks Spanish, that fact should appear in admission data or a member of the treatment team may inform you prior to you seeing them. This will enable you to schedule that patient when a translator, translation device, or family member that can translate is available. Scheduling appropriately, however, is not a static solution, so a backup plan should be established in case those resources are unavailable. Online translators can be useful for getting some basic translations to assist in your sessions. When all resources are unavailable, a list of key translated words to assist in administering the intervention for that day or for their length of stay may be required. It is difficult to coordinate translation services throughout an entire length of a patient's stay, so having these backup words can be vital for continuing quality service delivery.
Information on those you serve is vital for providing quality care. But it is also important to remember that something you may have found to be true for one patient may not be true for another, even if they have similar backgrounds. The Internet can be useful for finding information on cultures and their traditions, but it is safer to not to make assumptions. The best source of information on your client's beliefs, traditions, and background is typically from the client or their close family members and friends.
Being an active listener allows you to hear concerns that your client may have. This opens up an opportunity for recreational therapists to mitigate those concerns that could be making the client feel uncomfortable. For example, at some facilities, the recreational therapist may have the opportunity to do cooking or kitchen interventions. On occasion, a patient will have religious or cultural dietary restrictions and the food service department may not be meeting these needs. Members of the recreation department should perform functional cooking tasks with patients that meet their religious or cultural needs. This can make the patient or client feel more comfortable during their stay and assist other medical providers in meeting their goals for the client or patient.
When working with patients or clients from diverse cultural backgrounds, the best strategy for working with them can be broken down into four parts:
- Take extra time to gather and access resources.
- Utilize all available data and information.
- Listen to the patient and their caregiver(s) and family members.
- Work to minimize any of the client's concerns.
To help yourself, it can be beneficial to write down or keep stock of the resources and strategies that were most effective for a given scenario. Using these strategies, a solid foundation can be made to assist recreational therapists in better serving populations from diverse cultural backgrounds.
Questions for Consideration
- What strategies did the treatment team use in order to understand John?
- Based on the descriptions of John, to what extent was John culturally assimilated?
- Viewing this case study through an intersectionality lens, what sociodemographic variables might be helpful to understand John?
- If you were a member of John's therapy team, what would you do to implement cultural safety?
- In what way can practitioners move up the stages of cultural competence? How are ICF's personal factors helpful in the process?
Application of the assessment process with an individual with a physical disability
Bill is a 26-year-old with C6 quadriplegia. He completed three months of physical rehabilitation and has been living in the community with his wife for the past nine months.
By David P. Loy
Case Study
Application of the Assessment Process With an Individual With a Physical Disability
Bill is a 26-year-old with C6 quadriplegia. He completed three months of physical rehabilitation and has been living in the community with his wife for the past nine months. Bill heard about the recreational therapist working in his community and met with her to gain more independence and become more active since his discharge. Sarah Bellinger, a CTRS working in Bill's community, agreed to meet with Bill to conduct an assessment. She asked Bill if he could access his inpatient rehabilitation records or have them transferred to her in order to provide some preliminary information. During the initial meeting, Sarah performed a battery of assessments. She used a recreation interest survey to assess Bill's preferred recreation and leisure (d920) activities, a hand and finger dynamometer test for fine hand use (d440), the WST for mobility (d498), the CHART for community reintegration, and the modified functional reach test for vestibular balance (b240). The information indicates Bill has had limited recreation engagement (d920) since his SCI but expressed interest in sports and exercise (d9201) with a desire to get stronger so that he can progress from his power chair to a manual wheelchair. He has expressed a small fear of going in the community by himself because he doesn't have confidence in his skills. Hand and finger dynamometer readings indicate below average fine hand use (d440), but appropriate considering his spinal cord injury level. The WST test indicated a score of 19 (out of 66) for mobility (d498) and the CHART scores ranged from 18 to 32 in all five areas of CI. Answer the following questions based on this information.
- Discuss how the diagnosis of an SCI may have affected the CTRS's selection of assessment instruments.
- What are some appropriate treatment goals based on the interpretation of the assessment performance data provided?
- What are some preliminary interventions appropriate for Bill based on your interpretation of the assessment results?
Understanding the International Classification for Functioning, Disability and Health (ICF) model
To apply the coding of the ICF for effective service delivery, one needs to first understand how to utilize the ICF as a means to classify the full functioning of the individual, perhaps beginning with a diagnosis from the ICD-11.
By Thomas K. Skalko
Understanding the ICF Model
To apply the coding of the ICF for effective service delivery, one needs to first understand how to utilize the ICF as a means to classify the full functioning of the individual, perhaps beginning with a diagnosis from the ICD-11 (see www.who.int/classifications/icd/revision/icdprojectplan2015to2018.pdf?ua=1). The ICD-11 is a medical coding system for documenting diagnoses, signs of illness, symptoms of a condition, and social circumstances. Unlike the ICF, which focuses on functioning, the ICD offers some insights into the etiological classification by diagnosis of health condition, disorder, or disease. Coupled with the ICF, both classification schemes offer a relatively full picture of the medical and biopsychosocial aspects of the individual (Stucki, 2012).
Because this chapter focuses on understanding the ICF and demonstrating its connection to assessment, a full understanding of the ICF is of value to the reader. The ICF is a hierarchical structure consisting of two parts, each with two components. Part 1, functioning and disability, is broken into the components (1) body functions and structures, and (2) activities and participation. Part 2, contextual factors, is broken into (1) environmental factors and (2) personal factors. (Note: Types of personal factors are identified for clarity but are not classified, because every person has unique personal factors and the classification of every person's personal factors would be impossible.) In the ICF, “Each component (except personal factors) can be expressed in both positive and negative terms” (WHO, 2001, p. 10).
The ICF
domains are classified from body, individual and societal perspectives by means of two lists: a list of body functions and structure, and a list of domains of activity and participation. In the ICF, the term functioning refers to all body functions, activities and participation. The term disability is similarly an umbrella term for impairments, activity limitations and participation restrictions. The ICF also lists environmental factors that interact with all these components. (WHO, 2002, p. 2)
The ICF is
a classification of health and health-related domains—domains that help us to describe changes in body function and structure, what a person with a health condition can do in a standard environment (their level of capacity), as well as what they actually do in their usual environment (their level of performance). (WHO, 2002, p. 2)
Let's break down these concepts in order to better understand the ICF. The ICF model, as shown in figure 3.1, offers a coding system that begins with the recognition of a health condition. As delineated in the ICF, a health condition (disorder or disease) generally affects some physical (biological) or functional aspect of the individual's body structure or body function. Changes or impacts on body structure—for example, a spinal cord injury, limb amputation, or even pregnancy or aging—may affect an individual's functioning in multiple domains. The affected body structure or function affects the activities and participation of the individual in the life of the community. In addition, environmental factors contextually affect the individual in a positive (facilitator) or negative (barrier) manner. Remember, since every person is unique, the ICF does not include personal factors in the classification system but does provide examples of factors to consider.
Figure 3.1 The ICF model.
Adapted by permission from International Classification of Functioning, Disability, and Health, pg. 18, copyright 2001 (Geneva, World Health Organization); Adapted from B. Prodinger et al., “Toward the ICF Rehabilitation Set: A Minimal Generic Set of Domains for Rehabilitation as a Health Strategy,” Archives of Physical Medicine and Rehabilitation 97, no. 6 (2016): 875-884.
The impact on body structure and body function has implications for the ability of the individual to engage in activities (execution of a task) and participation (engagement in the life of the community). It is important to note that the community may range from the broader environment (e.g., city or neighborhood) to home or residential facility.
Unlike what one may perceive from the term activities (e.g., a recreational event), activities under the ICF are more discrete. Activities within the ICF refer to the specific execution of a task like manipulating objects (i.e., holding a pencil), focusing attention, or walking on different surfaces. Participation, on the other hand, may include moving around within a facility or using transportation. Together, the concepts of activities and participation are a bit different within the ICF model than how they are often used within recreational therapy practice. In recreational therapy service delivery, we often think of an activity as a game or manual arts project or exercise in a group. In the ICF model, as noted, an activity may be grasping an object, balancing on a foot, or making a decision. If a consumer cannot grasp a paint brush, they will not be able to participate in a painting experience or event. Therefore, participation in a community art class may not be possible unless the therapist assists the consumer in acquiring the skill of grasping or making a modification. So, it is important to note that the ICF classifies the functional performance of the discrete tasks or actions needed to participate in life situations. As therapists, we want to be able to assess one's functioning in such discrete tasks so that we can improve the functioning, design adapted supplies, or modify the activity to enhance engagement (participation).
In addition to body structure, body function, and activities and participation, environmental and personal factors also affect the functioning of the individual. Environmental elements include products and technology, natural environment and human-made changes to the environment, support and relationships, attitudes of others, and services, systems, and policies. The qualities (or lack thereof) of the environment, including technology, affect the ability of an individual to address functioning (e.g., a prosthetic device) and, therefore, engagement in the life of the community (see figure 3.1). Remember that personal factors, such as gender, ethnicity, religious beliefs, cultural morays, and family upbringing, are not coded because every individual is unique.
To understand the model, a brief description of each element is of value. Table 3.1 offers an explanation/definition of each component of the ICF (Rauch, Luckenkemper, & Cieza, 2012; WHO, 2001). Unlike earlier linear models of disability, the ICF model is a dynamic and interactive model that reflects the functioning of the individual and recognizes the impacts of each element in an individual's life. Each component interacts with the other components depicting this dynamic relationship. For instance, when an individual's body structure is changed, there is a subsequent impact on body function, activities, and engagement in the life of the community. When an individual engages in an activity that improves body function or structure, there is a resulting impact on activities that may also affect participation in the community. The ICF is about classifying functioning and includes those environmental factors that can facilitate functioning and engagement or serve as barriers to one's functioning.
The following sections offer a brief explanation of each element of the ICF. It is important to recognize the dynamic relationship between each element and the resulting positive or negative impact on an individual. The health condition has an impact on body structure, body function, activities, participation, and environment functioning, each altering the functioning of the individual.
A snapshot of serving clients from diverse cultural backgrounds in a physical medicine setting
John is a 56-year-old male from Manila, Philippines. The primary language he speaks at home is Tagalog but he is also fluent in English.
By Marc Zaremski
Case Study
A Snapshot of Serving Clients From Diverse Cultural Backgrounds in a Physical Medicine Setting
Written by Marc Zaremski, MS, CTRS: Clemson University
John is a 56-year-old male from Manila, Philippines. The primary language he speaks at home is Tagalog but he is also fluent in English. John moved from Manila to Florida when he was 13 years old with his parents. John has remained in Florida and he currently lives with his wife and youngest daughter. John's wife speaks Tagalog and some English and his daughter is bilingual. John was working on his roof when he experienced a dizzy spell and fell backward off of the ladder, approximately 15 feet, landing on his driveway. John did not lose consciousness and an ambulance was called immediately once he expressed to his wife that he could not move his legs. John sustained fractures in several thoracic vertebrae from T8 to T12. At the T10 level, he sustained a complete spinal cord injury, resulting in paralysis below the T10 level. The ambulance took him to the local trauma center, where he underwent several procedures to stabilize the spinal cord and relieve pressure at the injury site. After John was deemed medically stable, he was transferred to ABC Rehabilitation to receive inpatient rehabilitation approximately seven days postoperative.
At ABC Rehabilitation, John's therapy and medical teams consist of only English-speaking therapists who are all non-Hispanic Caucasian. The facility offers a translation service, when available, which is a live video feed of a translator that can assist during therapy sessions, doctor's visits, and any other time a patient might need information translated to or from a provider. John initially feels comfortable but some aspects of the hospital begin to conflict with his culture. The constant cold temperature throughout the hospital is concerning to him because he believes warmth promotes good health. John's more traditional relatives have expressed concern over food, the treatment plan, and the temperature of the facility as well. A member of John's family is a babaylan, which is a form of healer that uses prayers, herbs, and massage or tissue manipulation as a healing method. John asked his physician and physical therapist if this family member could perform their healing rituals on him. They deemed it unwise because the family member is not a medical professional and John has many precautions. John was disappointed but eventually convinced the medical team to allow this healer to work with him. They agreed, as long as John informed the babaylan of his medical precautions to avoid further injury. The healer is not fluent in English and John had difficulties translating some of the medical terminology. The therapy team used the translation service to confirm that the healer and John understand the restrictions of the treatment. John and the healer articulated that they understood the precautions and John was able to participate in this healing session. John enjoyed the healing session and it put his more traditional family members at ease.
Throughout John's stay he experienced some frustrations and setbacks. Some frustrations were because of how his life had changed due to his injury and some were because of language barriers and a lack of specific cultural knowledge from health care providers. With the flexibility and extra effort of his health care professional, John overcame some of these issues to progress into being independent in his wheelchair and was deemed eligible to return home safely.
It is unrealistic to expect every health care provider to be knowledgeable on the cultural traditions and preferences of every client or patient. But it is important to utilize available resources to gain some insight into what our patients and clients prefer and to find compromise between those beliefs and the best possible medical care.
Applying ICF and Purnell's Stages of Cultural Competence
Based on Purnell's (2012) cultural competence milestones, the level of cultural competence of the physicians and physical therapist does not appear to reach to the cultural sensitivity stage, as evidenced by careless rejections of the healing rituals. They might have noticed that John's background is Filipino; however, they were not aware of how important it was to John and his family members for John to receive healing rituals. In order for physicians and physical therapists to reach a higher stage of cultural competence, the ICF framework is helpful. Personal factors of ICF allow them to look at the person's worldview and value system, beyond race and ethnicity. By understanding the client's values, professionals are more likely to seek ways to achieve things that are important to the person.
Implications for Recreational Therapy Practice
Working with patients or clients from different cultural backgrounds can provide some difficulties for professionals. But many of these difficulties can be resolved or mitigated with extra effort and preparation. Taking the time to look at the resources of your facility and how to access them is a great starting point for establishing a protocol for future clients. If there is admission data or another professional at the facility that may have seen this client first, talking to them can be useful for knowing what resources you may need to acquire. For example, if a patient is admitted who only speaks Spanish, that fact should appear in admission data or a member of the treatment team may inform you prior to you seeing them. This will enable you to schedule that patient when a translator, translation device, or family member that can translate is available. Scheduling appropriately, however, is not a static solution, so a backup plan should be established in case those resources are unavailable. Online translators can be useful for getting some basic translations to assist in your sessions. When all resources are unavailable, a list of key translated words to assist in administering the intervention for that day or for their length of stay may be required. It is difficult to coordinate translation services throughout an entire length of a patient's stay, so having these backup words can be vital for continuing quality service delivery.
Information on those you serve is vital for providing quality care. But it is also important to remember that something you may have found to be true for one patient may not be true for another, even if they have similar backgrounds. The Internet can be useful for finding information on cultures and their traditions, but it is safer to not to make assumptions. The best source of information on your client's beliefs, traditions, and background is typically from the client or their close family members and friends.
Being an active listener allows you to hear concerns that your client may have. This opens up an opportunity for recreational therapists to mitigate those concerns that could be making the client feel uncomfortable. For example, at some facilities, the recreational therapist may have the opportunity to do cooking or kitchen interventions. On occasion, a patient will have religious or cultural dietary restrictions and the food service department may not be meeting these needs. Members of the recreation department should perform functional cooking tasks with patients that meet their religious or cultural needs. This can make the patient or client feel more comfortable during their stay and assist other medical providers in meeting their goals for the client or patient.
When working with patients or clients from diverse cultural backgrounds, the best strategy for working with them can be broken down into four parts:
- Take extra time to gather and access resources.
- Utilize all available data and information.
- Listen to the patient and their caregiver(s) and family members.
- Work to minimize any of the client's concerns.
To help yourself, it can be beneficial to write down or keep stock of the resources and strategies that were most effective for a given scenario. Using these strategies, a solid foundation can be made to assist recreational therapists in better serving populations from diverse cultural backgrounds.
Questions for Consideration
- What strategies did the treatment team use in order to understand John?
- Based on the descriptions of John, to what extent was John culturally assimilated?
- Viewing this case study through an intersectionality lens, what sociodemographic variables might be helpful to understand John?
- If you were a member of John's therapy team, what would you do to implement cultural safety?
- In what way can practitioners move up the stages of cultural competence? How are ICF's personal factors helpful in the process?
Application of the assessment process with an individual with a physical disability
Bill is a 26-year-old with C6 quadriplegia. He completed three months of physical rehabilitation and has been living in the community with his wife for the past nine months.
By David P. Loy
Case Study
Application of the Assessment Process With an Individual With a Physical Disability
Bill is a 26-year-old with C6 quadriplegia. He completed three months of physical rehabilitation and has been living in the community with his wife for the past nine months. Bill heard about the recreational therapist working in his community and met with her to gain more independence and become more active since his discharge. Sarah Bellinger, a CTRS working in Bill's community, agreed to meet with Bill to conduct an assessment. She asked Bill if he could access his inpatient rehabilitation records or have them transferred to her in order to provide some preliminary information. During the initial meeting, Sarah performed a battery of assessments. She used a recreation interest survey to assess Bill's preferred recreation and leisure (d920) activities, a hand and finger dynamometer test for fine hand use (d440), the WST for mobility (d498), the CHART for community reintegration, and the modified functional reach test for vestibular balance (b240). The information indicates Bill has had limited recreation engagement (d920) since his SCI but expressed interest in sports and exercise (d9201) with a desire to get stronger so that he can progress from his power chair to a manual wheelchair. He has expressed a small fear of going in the community by himself because he doesn't have confidence in his skills. Hand and finger dynamometer readings indicate below average fine hand use (d440), but appropriate considering his spinal cord injury level. The WST test indicated a score of 19 (out of 66) for mobility (d498) and the CHART scores ranged from 18 to 32 in all five areas of CI. Answer the following questions based on this information.
- Discuss how the diagnosis of an SCI may have affected the CTRS's selection of assessment instruments.
- What are some appropriate treatment goals based on the interpretation of the assessment performance data provided?
- What are some preliminary interventions appropriate for Bill based on your interpretation of the assessment results?
Understanding the International Classification for Functioning, Disability and Health (ICF) model
To apply the coding of the ICF for effective service delivery, one needs to first understand how to utilize the ICF as a means to classify the full functioning of the individual, perhaps beginning with a diagnosis from the ICD-11.
By Thomas K. Skalko
Understanding the ICF Model
To apply the coding of the ICF for effective service delivery, one needs to first understand how to utilize the ICF as a means to classify the full functioning of the individual, perhaps beginning with a diagnosis from the ICD-11 (see www.who.int/classifications/icd/revision/icdprojectplan2015to2018.pdf?ua=1). The ICD-11 is a medical coding system for documenting diagnoses, signs of illness, symptoms of a condition, and social circumstances. Unlike the ICF, which focuses on functioning, the ICD offers some insights into the etiological classification by diagnosis of health condition, disorder, or disease. Coupled with the ICF, both classification schemes offer a relatively full picture of the medical and biopsychosocial aspects of the individual (Stucki, 2012).
Because this chapter focuses on understanding the ICF and demonstrating its connection to assessment, a full understanding of the ICF is of value to the reader. The ICF is a hierarchical structure consisting of two parts, each with two components. Part 1, functioning and disability, is broken into the components (1) body functions and structures, and (2) activities and participation. Part 2, contextual factors, is broken into (1) environmental factors and (2) personal factors. (Note: Types of personal factors are identified for clarity but are not classified, because every person has unique personal factors and the classification of every person's personal factors would be impossible.) In the ICF, “Each component (except personal factors) can be expressed in both positive and negative terms” (WHO, 2001, p. 10).
The ICF
domains are classified from body, individual and societal perspectives by means of two lists: a list of body functions and structure, and a list of domains of activity and participation. In the ICF, the term functioning refers to all body functions, activities and participation. The term disability is similarly an umbrella term for impairments, activity limitations and participation restrictions. The ICF also lists environmental factors that interact with all these components. (WHO, 2002, p. 2)
The ICF is
a classification of health and health-related domains—domains that help us to describe changes in body function and structure, what a person with a health condition can do in a standard environment (their level of capacity), as well as what they actually do in their usual environment (their level of performance). (WHO, 2002, p. 2)
Let's break down these concepts in order to better understand the ICF. The ICF model, as shown in figure 3.1, offers a coding system that begins with the recognition of a health condition. As delineated in the ICF, a health condition (disorder or disease) generally affects some physical (biological) or functional aspect of the individual's body structure or body function. Changes or impacts on body structure—for example, a spinal cord injury, limb amputation, or even pregnancy or aging—may affect an individual's functioning in multiple domains. The affected body structure or function affects the activities and participation of the individual in the life of the community. In addition, environmental factors contextually affect the individual in a positive (facilitator) or negative (barrier) manner. Remember, since every person is unique, the ICF does not include personal factors in the classification system but does provide examples of factors to consider.
Figure 3.1 The ICF model.
Adapted by permission from International Classification of Functioning, Disability, and Health, pg. 18, copyright 2001 (Geneva, World Health Organization); Adapted from B. Prodinger et al., “Toward the ICF Rehabilitation Set: A Minimal Generic Set of Domains for Rehabilitation as a Health Strategy,” Archives of Physical Medicine and Rehabilitation 97, no. 6 (2016): 875-884.
The impact on body structure and body function has implications for the ability of the individual to engage in activities (execution of a task) and participation (engagement in the life of the community). It is important to note that the community may range from the broader environment (e.g., city or neighborhood) to home or residential facility.
Unlike what one may perceive from the term activities (e.g., a recreational event), activities under the ICF are more discrete. Activities within the ICF refer to the specific execution of a task like manipulating objects (i.e., holding a pencil), focusing attention, or walking on different surfaces. Participation, on the other hand, may include moving around within a facility or using transportation. Together, the concepts of activities and participation are a bit different within the ICF model than how they are often used within recreational therapy practice. In recreational therapy service delivery, we often think of an activity as a game or manual arts project or exercise in a group. In the ICF model, as noted, an activity may be grasping an object, balancing on a foot, or making a decision. If a consumer cannot grasp a paint brush, they will not be able to participate in a painting experience or event. Therefore, participation in a community art class may not be possible unless the therapist assists the consumer in acquiring the skill of grasping or making a modification. So, it is important to note that the ICF classifies the functional performance of the discrete tasks or actions needed to participate in life situations. As therapists, we want to be able to assess one's functioning in such discrete tasks so that we can improve the functioning, design adapted supplies, or modify the activity to enhance engagement (participation).
In addition to body structure, body function, and activities and participation, environmental and personal factors also affect the functioning of the individual. Environmental elements include products and technology, natural environment and human-made changes to the environment, support and relationships, attitudes of others, and services, systems, and policies. The qualities (or lack thereof) of the environment, including technology, affect the ability of an individual to address functioning (e.g., a prosthetic device) and, therefore, engagement in the life of the community (see figure 3.1). Remember that personal factors, such as gender, ethnicity, religious beliefs, cultural morays, and family upbringing, are not coded because every individual is unique.
To understand the model, a brief description of each element is of value. Table 3.1 offers an explanation/definition of each component of the ICF (Rauch, Luckenkemper, & Cieza, 2012; WHO, 2001). Unlike earlier linear models of disability, the ICF model is a dynamic and interactive model that reflects the functioning of the individual and recognizes the impacts of each element in an individual's life. Each component interacts with the other components depicting this dynamic relationship. For instance, when an individual's body structure is changed, there is a subsequent impact on body function, activities, and engagement in the life of the community. When an individual engages in an activity that improves body function or structure, there is a resulting impact on activities that may also affect participation in the community. The ICF is about classifying functioning and includes those environmental factors that can facilitate functioning and engagement or serve as barriers to one's functioning.
The following sections offer a brief explanation of each element of the ICF. It is important to recognize the dynamic relationship between each element and the resulting positive or negative impact on an individual. The health condition has an impact on body structure, body function, activities, participation, and environment functioning, each altering the functioning of the individual.
A snapshot of serving clients from diverse cultural backgrounds in a physical medicine setting
John is a 56-year-old male from Manila, Philippines. The primary language he speaks at home is Tagalog but he is also fluent in English.
By Marc Zaremski
Case Study
A Snapshot of Serving Clients From Diverse Cultural Backgrounds in a Physical Medicine Setting
Written by Marc Zaremski, MS, CTRS: Clemson University
John is a 56-year-old male from Manila, Philippines. The primary language he speaks at home is Tagalog but he is also fluent in English. John moved from Manila to Florida when he was 13 years old with his parents. John has remained in Florida and he currently lives with his wife and youngest daughter. John's wife speaks Tagalog and some English and his daughter is bilingual. John was working on his roof when he experienced a dizzy spell and fell backward off of the ladder, approximately 15 feet, landing on his driveway. John did not lose consciousness and an ambulance was called immediately once he expressed to his wife that he could not move his legs. John sustained fractures in several thoracic vertebrae from T8 to T12. At the T10 level, he sustained a complete spinal cord injury, resulting in paralysis below the T10 level. The ambulance took him to the local trauma center, where he underwent several procedures to stabilize the spinal cord and relieve pressure at the injury site. After John was deemed medically stable, he was transferred to ABC Rehabilitation to receive inpatient rehabilitation approximately seven days postoperative.
At ABC Rehabilitation, John's therapy and medical teams consist of only English-speaking therapists who are all non-Hispanic Caucasian. The facility offers a translation service, when available, which is a live video feed of a translator that can assist during therapy sessions, doctor's visits, and any other time a patient might need information translated to or from a provider. John initially feels comfortable but some aspects of the hospital begin to conflict with his culture. The constant cold temperature throughout the hospital is concerning to him because he believes warmth promotes good health. John's more traditional relatives have expressed concern over food, the treatment plan, and the temperature of the facility as well. A member of John's family is a babaylan, which is a form of healer that uses prayers, herbs, and massage or tissue manipulation as a healing method. John asked his physician and physical therapist if this family member could perform their healing rituals on him. They deemed it unwise because the family member is not a medical professional and John has many precautions. John was disappointed but eventually convinced the medical team to allow this healer to work with him. They agreed, as long as John informed the babaylan of his medical precautions to avoid further injury. The healer is not fluent in English and John had difficulties translating some of the medical terminology. The therapy team used the translation service to confirm that the healer and John understand the restrictions of the treatment. John and the healer articulated that they understood the precautions and John was able to participate in this healing session. John enjoyed the healing session and it put his more traditional family members at ease.
Throughout John's stay he experienced some frustrations and setbacks. Some frustrations were because of how his life had changed due to his injury and some were because of language barriers and a lack of specific cultural knowledge from health care providers. With the flexibility and extra effort of his health care professional, John overcame some of these issues to progress into being independent in his wheelchair and was deemed eligible to return home safely.
It is unrealistic to expect every health care provider to be knowledgeable on the cultural traditions and preferences of every client or patient. But it is important to utilize available resources to gain some insight into what our patients and clients prefer and to find compromise between those beliefs and the best possible medical care.
Applying ICF and Purnell's Stages of Cultural Competence
Based on Purnell's (2012) cultural competence milestones, the level of cultural competence of the physicians and physical therapist does not appear to reach to the cultural sensitivity stage, as evidenced by careless rejections of the healing rituals. They might have noticed that John's background is Filipino; however, they were not aware of how important it was to John and his family members for John to receive healing rituals. In order for physicians and physical therapists to reach a higher stage of cultural competence, the ICF framework is helpful. Personal factors of ICF allow them to look at the person's worldview and value system, beyond race and ethnicity. By understanding the client's values, professionals are more likely to seek ways to achieve things that are important to the person.
Implications for Recreational Therapy Practice
Working with patients or clients from different cultural backgrounds can provide some difficulties for professionals. But many of these difficulties can be resolved or mitigated with extra effort and preparation. Taking the time to look at the resources of your facility and how to access them is a great starting point for establishing a protocol for future clients. If there is admission data or another professional at the facility that may have seen this client first, talking to them can be useful for knowing what resources you may need to acquire. For example, if a patient is admitted who only speaks Spanish, that fact should appear in admission data or a member of the treatment team may inform you prior to you seeing them. This will enable you to schedule that patient when a translator, translation device, or family member that can translate is available. Scheduling appropriately, however, is not a static solution, so a backup plan should be established in case those resources are unavailable. Online translators can be useful for getting some basic translations to assist in your sessions. When all resources are unavailable, a list of key translated words to assist in administering the intervention for that day or for their length of stay may be required. It is difficult to coordinate translation services throughout an entire length of a patient's stay, so having these backup words can be vital for continuing quality service delivery.
Information on those you serve is vital for providing quality care. But it is also important to remember that something you may have found to be true for one patient may not be true for another, even if they have similar backgrounds. The Internet can be useful for finding information on cultures and their traditions, but it is safer to not to make assumptions. The best source of information on your client's beliefs, traditions, and background is typically from the client or their close family members and friends.
Being an active listener allows you to hear concerns that your client may have. This opens up an opportunity for recreational therapists to mitigate those concerns that could be making the client feel uncomfortable. For example, at some facilities, the recreational therapist may have the opportunity to do cooking or kitchen interventions. On occasion, a patient will have religious or cultural dietary restrictions and the food service department may not be meeting these needs. Members of the recreation department should perform functional cooking tasks with patients that meet their religious or cultural needs. This can make the patient or client feel more comfortable during their stay and assist other medical providers in meeting their goals for the client or patient.
When working with patients or clients from diverse cultural backgrounds, the best strategy for working with them can be broken down into four parts:
- Take extra time to gather and access resources.
- Utilize all available data and information.
- Listen to the patient and their caregiver(s) and family members.
- Work to minimize any of the client's concerns.
To help yourself, it can be beneficial to write down or keep stock of the resources and strategies that were most effective for a given scenario. Using these strategies, a solid foundation can be made to assist recreational therapists in better serving populations from diverse cultural backgrounds.
Questions for Consideration
- What strategies did the treatment team use in order to understand John?
- Based on the descriptions of John, to what extent was John culturally assimilated?
- Viewing this case study through an intersectionality lens, what sociodemographic variables might be helpful to understand John?
- If you were a member of John's therapy team, what would you do to implement cultural safety?
- In what way can practitioners move up the stages of cultural competence? How are ICF's personal factors helpful in the process?
Application of the assessment process with an individual with a physical disability
Bill is a 26-year-old with C6 quadriplegia. He completed three months of physical rehabilitation and has been living in the community with his wife for the past nine months.
By David P. Loy
Case Study
Application of the Assessment Process With an Individual With a Physical Disability
Bill is a 26-year-old with C6 quadriplegia. He completed three months of physical rehabilitation and has been living in the community with his wife for the past nine months. Bill heard about the recreational therapist working in his community and met with her to gain more independence and become more active since his discharge. Sarah Bellinger, a CTRS working in Bill's community, agreed to meet with Bill to conduct an assessment. She asked Bill if he could access his inpatient rehabilitation records or have them transferred to her in order to provide some preliminary information. During the initial meeting, Sarah performed a battery of assessments. She used a recreation interest survey to assess Bill's preferred recreation and leisure (d920) activities, a hand and finger dynamometer test for fine hand use (d440), the WST for mobility (d498), the CHART for community reintegration, and the modified functional reach test for vestibular balance (b240). The information indicates Bill has had limited recreation engagement (d920) since his SCI but expressed interest in sports and exercise (d9201) with a desire to get stronger so that he can progress from his power chair to a manual wheelchair. He has expressed a small fear of going in the community by himself because he doesn't have confidence in his skills. Hand and finger dynamometer readings indicate below average fine hand use (d440), but appropriate considering his spinal cord injury level. The WST test indicated a score of 19 (out of 66) for mobility (d498) and the CHART scores ranged from 18 to 32 in all five areas of CI. Answer the following questions based on this information.
- Discuss how the diagnosis of an SCI may have affected the CTRS's selection of assessment instruments.
- What are some appropriate treatment goals based on the interpretation of the assessment performance data provided?
- What are some preliminary interventions appropriate for Bill based on your interpretation of the assessment results?
Understanding the International Classification for Functioning, Disability and Health (ICF) model
To apply the coding of the ICF for effective service delivery, one needs to first understand how to utilize the ICF as a means to classify the full functioning of the individual, perhaps beginning with a diagnosis from the ICD-11.
By Thomas K. Skalko
Understanding the ICF Model
To apply the coding of the ICF for effective service delivery, one needs to first understand how to utilize the ICF as a means to classify the full functioning of the individual, perhaps beginning with a diagnosis from the ICD-11 (see www.who.int/classifications/icd/revision/icdprojectplan2015to2018.pdf?ua=1). The ICD-11 is a medical coding system for documenting diagnoses, signs of illness, symptoms of a condition, and social circumstances. Unlike the ICF, which focuses on functioning, the ICD offers some insights into the etiological classification by diagnosis of health condition, disorder, or disease. Coupled with the ICF, both classification schemes offer a relatively full picture of the medical and biopsychosocial aspects of the individual (Stucki, 2012).
Because this chapter focuses on understanding the ICF and demonstrating its connection to assessment, a full understanding of the ICF is of value to the reader. The ICF is a hierarchical structure consisting of two parts, each with two components. Part 1, functioning and disability, is broken into the components (1) body functions and structures, and (2) activities and participation. Part 2, contextual factors, is broken into (1) environmental factors and (2) personal factors. (Note: Types of personal factors are identified for clarity but are not classified, because every person has unique personal factors and the classification of every person's personal factors would be impossible.) In the ICF, “Each component (except personal factors) can be expressed in both positive and negative terms” (WHO, 2001, p. 10).
The ICF
domains are classified from body, individual and societal perspectives by means of two lists: a list of body functions and structure, and a list of domains of activity and participation. In the ICF, the term functioning refers to all body functions, activities and participation. The term disability is similarly an umbrella term for impairments, activity limitations and participation restrictions. The ICF also lists environmental factors that interact with all these components. (WHO, 2002, p. 2)
The ICF is
a classification of health and health-related domains—domains that help us to describe changes in body function and structure, what a person with a health condition can do in a standard environment (their level of capacity), as well as what they actually do in their usual environment (their level of performance). (WHO, 2002, p. 2)
Let's break down these concepts in order to better understand the ICF. The ICF model, as shown in figure 3.1, offers a coding system that begins with the recognition of a health condition. As delineated in the ICF, a health condition (disorder or disease) generally affects some physical (biological) or functional aspect of the individual's body structure or body function. Changes or impacts on body structure—for example, a spinal cord injury, limb amputation, or even pregnancy or aging—may affect an individual's functioning in multiple domains. The affected body structure or function affects the activities and participation of the individual in the life of the community. In addition, environmental factors contextually affect the individual in a positive (facilitator) or negative (barrier) manner. Remember, since every person is unique, the ICF does not include personal factors in the classification system but does provide examples of factors to consider.
Figure 3.1 The ICF model.
Adapted by permission from International Classification of Functioning, Disability, and Health, pg. 18, copyright 2001 (Geneva, World Health Organization); Adapted from B. Prodinger et al., “Toward the ICF Rehabilitation Set: A Minimal Generic Set of Domains for Rehabilitation as a Health Strategy,” Archives of Physical Medicine and Rehabilitation 97, no. 6 (2016): 875-884.
The impact on body structure and body function has implications for the ability of the individual to engage in activities (execution of a task) and participation (engagement in the life of the community). It is important to note that the community may range from the broader environment (e.g., city or neighborhood) to home or residential facility.
Unlike what one may perceive from the term activities (e.g., a recreational event), activities under the ICF are more discrete. Activities within the ICF refer to the specific execution of a task like manipulating objects (i.e., holding a pencil), focusing attention, or walking on different surfaces. Participation, on the other hand, may include moving around within a facility or using transportation. Together, the concepts of activities and participation are a bit different within the ICF model than how they are often used within recreational therapy practice. In recreational therapy service delivery, we often think of an activity as a game or manual arts project or exercise in a group. In the ICF model, as noted, an activity may be grasping an object, balancing on a foot, or making a decision. If a consumer cannot grasp a paint brush, they will not be able to participate in a painting experience or event. Therefore, participation in a community art class may not be possible unless the therapist assists the consumer in acquiring the skill of grasping or making a modification. So, it is important to note that the ICF classifies the functional performance of the discrete tasks or actions needed to participate in life situations. As therapists, we want to be able to assess one's functioning in such discrete tasks so that we can improve the functioning, design adapted supplies, or modify the activity to enhance engagement (participation).
In addition to body structure, body function, and activities and participation, environmental and personal factors also affect the functioning of the individual. Environmental elements include products and technology, natural environment and human-made changes to the environment, support and relationships, attitudes of others, and services, systems, and policies. The qualities (or lack thereof) of the environment, including technology, affect the ability of an individual to address functioning (e.g., a prosthetic device) and, therefore, engagement in the life of the community (see figure 3.1). Remember that personal factors, such as gender, ethnicity, religious beliefs, cultural morays, and family upbringing, are not coded because every individual is unique.
To understand the model, a brief description of each element is of value. Table 3.1 offers an explanation/definition of each component of the ICF (Rauch, Luckenkemper, & Cieza, 2012; WHO, 2001). Unlike earlier linear models of disability, the ICF model is a dynamic and interactive model that reflects the functioning of the individual and recognizes the impacts of each element in an individual's life. Each component interacts with the other components depicting this dynamic relationship. For instance, when an individual's body structure is changed, there is a subsequent impact on body function, activities, and engagement in the life of the community. When an individual engages in an activity that improves body function or structure, there is a resulting impact on activities that may also affect participation in the community. The ICF is about classifying functioning and includes those environmental factors that can facilitate functioning and engagement or serve as barriers to one's functioning.
The following sections offer a brief explanation of each element of the ICF. It is important to recognize the dynamic relationship between each element and the resulting positive or negative impact on an individual. The health condition has an impact on body structure, body function, activities, participation, and environment functioning, each altering the functioning of the individual.
A snapshot of serving clients from diverse cultural backgrounds in a physical medicine setting
John is a 56-year-old male from Manila, Philippines. The primary language he speaks at home is Tagalog but he is also fluent in English.
By Marc Zaremski
Case Study
A Snapshot of Serving Clients From Diverse Cultural Backgrounds in a Physical Medicine Setting
Written by Marc Zaremski, MS, CTRS: Clemson University
John is a 56-year-old male from Manila, Philippines. The primary language he speaks at home is Tagalog but he is also fluent in English. John moved from Manila to Florida when he was 13 years old with his parents. John has remained in Florida and he currently lives with his wife and youngest daughter. John's wife speaks Tagalog and some English and his daughter is bilingual. John was working on his roof when he experienced a dizzy spell and fell backward off of the ladder, approximately 15 feet, landing on his driveway. John did not lose consciousness and an ambulance was called immediately once he expressed to his wife that he could not move his legs. John sustained fractures in several thoracic vertebrae from T8 to T12. At the T10 level, he sustained a complete spinal cord injury, resulting in paralysis below the T10 level. The ambulance took him to the local trauma center, where he underwent several procedures to stabilize the spinal cord and relieve pressure at the injury site. After John was deemed medically stable, he was transferred to ABC Rehabilitation to receive inpatient rehabilitation approximately seven days postoperative.
At ABC Rehabilitation, John's therapy and medical teams consist of only English-speaking therapists who are all non-Hispanic Caucasian. The facility offers a translation service, when available, which is a live video feed of a translator that can assist during therapy sessions, doctor's visits, and any other time a patient might need information translated to or from a provider. John initially feels comfortable but some aspects of the hospital begin to conflict with his culture. The constant cold temperature throughout the hospital is concerning to him because he believes warmth promotes good health. John's more traditional relatives have expressed concern over food, the treatment plan, and the temperature of the facility as well. A member of John's family is a babaylan, which is a form of healer that uses prayers, herbs, and massage or tissue manipulation as a healing method. John asked his physician and physical therapist if this family member could perform their healing rituals on him. They deemed it unwise because the family member is not a medical professional and John has many precautions. John was disappointed but eventually convinced the medical team to allow this healer to work with him. They agreed, as long as John informed the babaylan of his medical precautions to avoid further injury. The healer is not fluent in English and John had difficulties translating some of the medical terminology. The therapy team used the translation service to confirm that the healer and John understand the restrictions of the treatment. John and the healer articulated that they understood the precautions and John was able to participate in this healing session. John enjoyed the healing session and it put his more traditional family members at ease.
Throughout John's stay he experienced some frustrations and setbacks. Some frustrations were because of how his life had changed due to his injury and some were because of language barriers and a lack of specific cultural knowledge from health care providers. With the flexibility and extra effort of his health care professional, John overcame some of these issues to progress into being independent in his wheelchair and was deemed eligible to return home safely.
It is unrealistic to expect every health care provider to be knowledgeable on the cultural traditions and preferences of every client or patient. But it is important to utilize available resources to gain some insight into what our patients and clients prefer and to find compromise between those beliefs and the best possible medical care.
Applying ICF and Purnell's Stages of Cultural Competence
Based on Purnell's (2012) cultural competence milestones, the level of cultural competence of the physicians and physical therapist does not appear to reach to the cultural sensitivity stage, as evidenced by careless rejections of the healing rituals. They might have noticed that John's background is Filipino; however, they were not aware of how important it was to John and his family members for John to receive healing rituals. In order for physicians and physical therapists to reach a higher stage of cultural competence, the ICF framework is helpful. Personal factors of ICF allow them to look at the person's worldview and value system, beyond race and ethnicity. By understanding the client's values, professionals are more likely to seek ways to achieve things that are important to the person.
Implications for Recreational Therapy Practice
Working with patients or clients from different cultural backgrounds can provide some difficulties for professionals. But many of these difficulties can be resolved or mitigated with extra effort and preparation. Taking the time to look at the resources of your facility and how to access them is a great starting point for establishing a protocol for future clients. If there is admission data or another professional at the facility that may have seen this client first, talking to them can be useful for knowing what resources you may need to acquire. For example, if a patient is admitted who only speaks Spanish, that fact should appear in admission data or a member of the treatment team may inform you prior to you seeing them. This will enable you to schedule that patient when a translator, translation device, or family member that can translate is available. Scheduling appropriately, however, is not a static solution, so a backup plan should be established in case those resources are unavailable. Online translators can be useful for getting some basic translations to assist in your sessions. When all resources are unavailable, a list of key translated words to assist in administering the intervention for that day or for their length of stay may be required. It is difficult to coordinate translation services throughout an entire length of a patient's stay, so having these backup words can be vital for continuing quality service delivery.
Information on those you serve is vital for providing quality care. But it is also important to remember that something you may have found to be true for one patient may not be true for another, even if they have similar backgrounds. The Internet can be useful for finding information on cultures and their traditions, but it is safer to not to make assumptions. The best source of information on your client's beliefs, traditions, and background is typically from the client or their close family members and friends.
Being an active listener allows you to hear concerns that your client may have. This opens up an opportunity for recreational therapists to mitigate those concerns that could be making the client feel uncomfortable. For example, at some facilities, the recreational therapist may have the opportunity to do cooking or kitchen interventions. On occasion, a patient will have religious or cultural dietary restrictions and the food service department may not be meeting these needs. Members of the recreation department should perform functional cooking tasks with patients that meet their religious or cultural needs. This can make the patient or client feel more comfortable during their stay and assist other medical providers in meeting their goals for the client or patient.
When working with patients or clients from diverse cultural backgrounds, the best strategy for working with them can be broken down into four parts:
- Take extra time to gather and access resources.
- Utilize all available data and information.
- Listen to the patient and their caregiver(s) and family members.
- Work to minimize any of the client's concerns.
To help yourself, it can be beneficial to write down or keep stock of the resources and strategies that were most effective for a given scenario. Using these strategies, a solid foundation can be made to assist recreational therapists in better serving populations from diverse cultural backgrounds.
Questions for Consideration
- What strategies did the treatment team use in order to understand John?
- Based on the descriptions of John, to what extent was John culturally assimilated?
- Viewing this case study through an intersectionality lens, what sociodemographic variables might be helpful to understand John?
- If you were a member of John's therapy team, what would you do to implement cultural safety?
- In what way can practitioners move up the stages of cultural competence? How are ICF's personal factors helpful in the process?
Application of the assessment process with an individual with a physical disability
Bill is a 26-year-old with C6 quadriplegia. He completed three months of physical rehabilitation and has been living in the community with his wife for the past nine months.
By David P. Loy
Case Study
Application of the Assessment Process With an Individual With a Physical Disability
Bill is a 26-year-old with C6 quadriplegia. He completed three months of physical rehabilitation and has been living in the community with his wife for the past nine months. Bill heard about the recreational therapist working in his community and met with her to gain more independence and become more active since his discharge. Sarah Bellinger, a CTRS working in Bill's community, agreed to meet with Bill to conduct an assessment. She asked Bill if he could access his inpatient rehabilitation records or have them transferred to her in order to provide some preliminary information. During the initial meeting, Sarah performed a battery of assessments. She used a recreation interest survey to assess Bill's preferred recreation and leisure (d920) activities, a hand and finger dynamometer test for fine hand use (d440), the WST for mobility (d498), the CHART for community reintegration, and the modified functional reach test for vestibular balance (b240). The information indicates Bill has had limited recreation engagement (d920) since his SCI but expressed interest in sports and exercise (d9201) with a desire to get stronger so that he can progress from his power chair to a manual wheelchair. He has expressed a small fear of going in the community by himself because he doesn't have confidence in his skills. Hand and finger dynamometer readings indicate below average fine hand use (d440), but appropriate considering his spinal cord injury level. The WST test indicated a score of 19 (out of 66) for mobility (d498) and the CHART scores ranged from 18 to 32 in all five areas of CI. Answer the following questions based on this information.
- Discuss how the diagnosis of an SCI may have affected the CTRS's selection of assessment instruments.
- What are some appropriate treatment goals based on the interpretation of the assessment performance data provided?
- What are some preliminary interventions appropriate for Bill based on your interpretation of the assessment results?
Understanding the International Classification for Functioning, Disability and Health (ICF) model
To apply the coding of the ICF for effective service delivery, one needs to first understand how to utilize the ICF as a means to classify the full functioning of the individual, perhaps beginning with a diagnosis from the ICD-11.
By Thomas K. Skalko
Understanding the ICF Model
To apply the coding of the ICF for effective service delivery, one needs to first understand how to utilize the ICF as a means to classify the full functioning of the individual, perhaps beginning with a diagnosis from the ICD-11 (see www.who.int/classifications/icd/revision/icdprojectplan2015to2018.pdf?ua=1). The ICD-11 is a medical coding system for documenting diagnoses, signs of illness, symptoms of a condition, and social circumstances. Unlike the ICF, which focuses on functioning, the ICD offers some insights into the etiological classification by diagnosis of health condition, disorder, or disease. Coupled with the ICF, both classification schemes offer a relatively full picture of the medical and biopsychosocial aspects of the individual (Stucki, 2012).
Because this chapter focuses on understanding the ICF and demonstrating its connection to assessment, a full understanding of the ICF is of value to the reader. The ICF is a hierarchical structure consisting of two parts, each with two components. Part 1, functioning and disability, is broken into the components (1) body functions and structures, and (2) activities and participation. Part 2, contextual factors, is broken into (1) environmental factors and (2) personal factors. (Note: Types of personal factors are identified for clarity but are not classified, because every person has unique personal factors and the classification of every person's personal factors would be impossible.) In the ICF, “Each component (except personal factors) can be expressed in both positive and negative terms” (WHO, 2001, p. 10).
The ICF
domains are classified from body, individual and societal perspectives by means of two lists: a list of body functions and structure, and a list of domains of activity and participation. In the ICF, the term functioning refers to all body functions, activities and participation. The term disability is similarly an umbrella term for impairments, activity limitations and participation restrictions. The ICF also lists environmental factors that interact with all these components. (WHO, 2002, p. 2)
The ICF is
a classification of health and health-related domains—domains that help us to describe changes in body function and structure, what a person with a health condition can do in a standard environment (their level of capacity), as well as what they actually do in their usual environment (their level of performance). (WHO, 2002, p. 2)
Let's break down these concepts in order to better understand the ICF. The ICF model, as shown in figure 3.1, offers a coding system that begins with the recognition of a health condition. As delineated in the ICF, a health condition (disorder or disease) generally affects some physical (biological) or functional aspect of the individual's body structure or body function. Changes or impacts on body structure—for example, a spinal cord injury, limb amputation, or even pregnancy or aging—may affect an individual's functioning in multiple domains. The affected body structure or function affects the activities and participation of the individual in the life of the community. In addition, environmental factors contextually affect the individual in a positive (facilitator) or negative (barrier) manner. Remember, since every person is unique, the ICF does not include personal factors in the classification system but does provide examples of factors to consider.
Figure 3.1 The ICF model.
Adapted by permission from International Classification of Functioning, Disability, and Health, pg. 18, copyright 2001 (Geneva, World Health Organization); Adapted from B. Prodinger et al., “Toward the ICF Rehabilitation Set: A Minimal Generic Set of Domains for Rehabilitation as a Health Strategy,” Archives of Physical Medicine and Rehabilitation 97, no. 6 (2016): 875-884.
The impact on body structure and body function has implications for the ability of the individual to engage in activities (execution of a task) and participation (engagement in the life of the community). It is important to note that the community may range from the broader environment (e.g., city or neighborhood) to home or residential facility.
Unlike what one may perceive from the term activities (e.g., a recreational event), activities under the ICF are more discrete. Activities within the ICF refer to the specific execution of a task like manipulating objects (i.e., holding a pencil), focusing attention, or walking on different surfaces. Participation, on the other hand, may include moving around within a facility or using transportation. Together, the concepts of activities and participation are a bit different within the ICF model than how they are often used within recreational therapy practice. In recreational therapy service delivery, we often think of an activity as a game or manual arts project or exercise in a group. In the ICF model, as noted, an activity may be grasping an object, balancing on a foot, or making a decision. If a consumer cannot grasp a paint brush, they will not be able to participate in a painting experience or event. Therefore, participation in a community art class may not be possible unless the therapist assists the consumer in acquiring the skill of grasping or making a modification. So, it is important to note that the ICF classifies the functional performance of the discrete tasks or actions needed to participate in life situations. As therapists, we want to be able to assess one's functioning in such discrete tasks so that we can improve the functioning, design adapted supplies, or modify the activity to enhance engagement (participation).
In addition to body structure, body function, and activities and participation, environmental and personal factors also affect the functioning of the individual. Environmental elements include products and technology, natural environment and human-made changes to the environment, support and relationships, attitudes of others, and services, systems, and policies. The qualities (or lack thereof) of the environment, including technology, affect the ability of an individual to address functioning (e.g., a prosthetic device) and, therefore, engagement in the life of the community (see figure 3.1). Remember that personal factors, such as gender, ethnicity, religious beliefs, cultural morays, and family upbringing, are not coded because every individual is unique.
To understand the model, a brief description of each element is of value. Table 3.1 offers an explanation/definition of each component of the ICF (Rauch, Luckenkemper, & Cieza, 2012; WHO, 2001). Unlike earlier linear models of disability, the ICF model is a dynamic and interactive model that reflects the functioning of the individual and recognizes the impacts of each element in an individual's life. Each component interacts with the other components depicting this dynamic relationship. For instance, when an individual's body structure is changed, there is a subsequent impact on body function, activities, and engagement in the life of the community. When an individual engages in an activity that improves body function or structure, there is a resulting impact on activities that may also affect participation in the community. The ICF is about classifying functioning and includes those environmental factors that can facilitate functioning and engagement or serve as barriers to one's functioning.
The following sections offer a brief explanation of each element of the ICF. It is important to recognize the dynamic relationship between each element and the resulting positive or negative impact on an individual. The health condition has an impact on body structure, body function, activities, participation, and environment functioning, each altering the functioning of the individual.
A snapshot of serving clients from diverse cultural backgrounds in a physical medicine setting
John is a 56-year-old male from Manila, Philippines. The primary language he speaks at home is Tagalog but he is also fluent in English.
By Marc Zaremski
Case Study
A Snapshot of Serving Clients From Diverse Cultural Backgrounds in a Physical Medicine Setting
Written by Marc Zaremski, MS, CTRS: Clemson University
John is a 56-year-old male from Manila, Philippines. The primary language he speaks at home is Tagalog but he is also fluent in English. John moved from Manila to Florida when he was 13 years old with his parents. John has remained in Florida and he currently lives with his wife and youngest daughter. John's wife speaks Tagalog and some English and his daughter is bilingual. John was working on his roof when he experienced a dizzy spell and fell backward off of the ladder, approximately 15 feet, landing on his driveway. John did not lose consciousness and an ambulance was called immediately once he expressed to his wife that he could not move his legs. John sustained fractures in several thoracic vertebrae from T8 to T12. At the T10 level, he sustained a complete spinal cord injury, resulting in paralysis below the T10 level. The ambulance took him to the local trauma center, where he underwent several procedures to stabilize the spinal cord and relieve pressure at the injury site. After John was deemed medically stable, he was transferred to ABC Rehabilitation to receive inpatient rehabilitation approximately seven days postoperative.
At ABC Rehabilitation, John's therapy and medical teams consist of only English-speaking therapists who are all non-Hispanic Caucasian. The facility offers a translation service, when available, which is a live video feed of a translator that can assist during therapy sessions, doctor's visits, and any other time a patient might need information translated to or from a provider. John initially feels comfortable but some aspects of the hospital begin to conflict with his culture. The constant cold temperature throughout the hospital is concerning to him because he believes warmth promotes good health. John's more traditional relatives have expressed concern over food, the treatment plan, and the temperature of the facility as well. A member of John's family is a babaylan, which is a form of healer that uses prayers, herbs, and massage or tissue manipulation as a healing method. John asked his physician and physical therapist if this family member could perform their healing rituals on him. They deemed it unwise because the family member is not a medical professional and John has many precautions. John was disappointed but eventually convinced the medical team to allow this healer to work with him. They agreed, as long as John informed the babaylan of his medical precautions to avoid further injury. The healer is not fluent in English and John had difficulties translating some of the medical terminology. The therapy team used the translation service to confirm that the healer and John understand the restrictions of the treatment. John and the healer articulated that they understood the precautions and John was able to participate in this healing session. John enjoyed the healing session and it put his more traditional family members at ease.
Throughout John's stay he experienced some frustrations and setbacks. Some frustrations were because of how his life had changed due to his injury and some were because of language barriers and a lack of specific cultural knowledge from health care providers. With the flexibility and extra effort of his health care professional, John overcame some of these issues to progress into being independent in his wheelchair and was deemed eligible to return home safely.
It is unrealistic to expect every health care provider to be knowledgeable on the cultural traditions and preferences of every client or patient. But it is important to utilize available resources to gain some insight into what our patients and clients prefer and to find compromise between those beliefs and the best possible medical care.
Applying ICF and Purnell's Stages of Cultural Competence
Based on Purnell's (2012) cultural competence milestones, the level of cultural competence of the physicians and physical therapist does not appear to reach to the cultural sensitivity stage, as evidenced by careless rejections of the healing rituals. They might have noticed that John's background is Filipino; however, they were not aware of how important it was to John and his family members for John to receive healing rituals. In order for physicians and physical therapists to reach a higher stage of cultural competence, the ICF framework is helpful. Personal factors of ICF allow them to look at the person's worldview and value system, beyond race and ethnicity. By understanding the client's values, professionals are more likely to seek ways to achieve things that are important to the person.
Implications for Recreational Therapy Practice
Working with patients or clients from different cultural backgrounds can provide some difficulties for professionals. But many of these difficulties can be resolved or mitigated with extra effort and preparation. Taking the time to look at the resources of your facility and how to access them is a great starting point for establishing a protocol for future clients. If there is admission data or another professional at the facility that may have seen this client first, talking to them can be useful for knowing what resources you may need to acquire. For example, if a patient is admitted who only speaks Spanish, that fact should appear in admission data or a member of the treatment team may inform you prior to you seeing them. This will enable you to schedule that patient when a translator, translation device, or family member that can translate is available. Scheduling appropriately, however, is not a static solution, so a backup plan should be established in case those resources are unavailable. Online translators can be useful for getting some basic translations to assist in your sessions. When all resources are unavailable, a list of key translated words to assist in administering the intervention for that day or for their length of stay may be required. It is difficult to coordinate translation services throughout an entire length of a patient's stay, so having these backup words can be vital for continuing quality service delivery.
Information on those you serve is vital for providing quality care. But it is also important to remember that something you may have found to be true for one patient may not be true for another, even if they have similar backgrounds. The Internet can be useful for finding information on cultures and their traditions, but it is safer to not to make assumptions. The best source of information on your client's beliefs, traditions, and background is typically from the client or their close family members and friends.
Being an active listener allows you to hear concerns that your client may have. This opens up an opportunity for recreational therapists to mitigate those concerns that could be making the client feel uncomfortable. For example, at some facilities, the recreational therapist may have the opportunity to do cooking or kitchen interventions. On occasion, a patient will have religious or cultural dietary restrictions and the food service department may not be meeting these needs. Members of the recreation department should perform functional cooking tasks with patients that meet their religious or cultural needs. This can make the patient or client feel more comfortable during their stay and assist other medical providers in meeting their goals for the client or patient.
When working with patients or clients from diverse cultural backgrounds, the best strategy for working with them can be broken down into four parts:
- Take extra time to gather and access resources.
- Utilize all available data and information.
- Listen to the patient and their caregiver(s) and family members.
- Work to minimize any of the client's concerns.
To help yourself, it can be beneficial to write down or keep stock of the resources and strategies that were most effective for a given scenario. Using these strategies, a solid foundation can be made to assist recreational therapists in better serving populations from diverse cultural backgrounds.
Questions for Consideration
- What strategies did the treatment team use in order to understand John?
- Based on the descriptions of John, to what extent was John culturally assimilated?
- Viewing this case study through an intersectionality lens, what sociodemographic variables might be helpful to understand John?
- If you were a member of John's therapy team, what would you do to implement cultural safety?
- In what way can practitioners move up the stages of cultural competence? How are ICF's personal factors helpful in the process?
Application of the assessment process with an individual with a physical disability
Bill is a 26-year-old with C6 quadriplegia. He completed three months of physical rehabilitation and has been living in the community with his wife for the past nine months.
By David P. Loy
Case Study
Application of the Assessment Process With an Individual With a Physical Disability
Bill is a 26-year-old with C6 quadriplegia. He completed three months of physical rehabilitation and has been living in the community with his wife for the past nine months. Bill heard about the recreational therapist working in his community and met with her to gain more independence and become more active since his discharge. Sarah Bellinger, a CTRS working in Bill's community, agreed to meet with Bill to conduct an assessment. She asked Bill if he could access his inpatient rehabilitation records or have them transferred to her in order to provide some preliminary information. During the initial meeting, Sarah performed a battery of assessments. She used a recreation interest survey to assess Bill's preferred recreation and leisure (d920) activities, a hand and finger dynamometer test for fine hand use (d440), the WST for mobility (d498), the CHART for community reintegration, and the modified functional reach test for vestibular balance (b240). The information indicates Bill has had limited recreation engagement (d920) since his SCI but expressed interest in sports and exercise (d9201) with a desire to get stronger so that he can progress from his power chair to a manual wheelchair. He has expressed a small fear of going in the community by himself because he doesn't have confidence in his skills. Hand and finger dynamometer readings indicate below average fine hand use (d440), but appropriate considering his spinal cord injury level. The WST test indicated a score of 19 (out of 66) for mobility (d498) and the CHART scores ranged from 18 to 32 in all five areas of CI. Answer the following questions based on this information.
- Discuss how the diagnosis of an SCI may have affected the CTRS's selection of assessment instruments.
- What are some appropriate treatment goals based on the interpretation of the assessment performance data provided?
- What are some preliminary interventions appropriate for Bill based on your interpretation of the assessment results?
Understanding the International Classification for Functioning, Disability and Health (ICF) model
To apply the coding of the ICF for effective service delivery, one needs to first understand how to utilize the ICF as a means to classify the full functioning of the individual, perhaps beginning with a diagnosis from the ICD-11.
By Thomas K. Skalko
Understanding the ICF Model
To apply the coding of the ICF for effective service delivery, one needs to first understand how to utilize the ICF as a means to classify the full functioning of the individual, perhaps beginning with a diagnosis from the ICD-11 (see www.who.int/classifications/icd/revision/icdprojectplan2015to2018.pdf?ua=1). The ICD-11 is a medical coding system for documenting diagnoses, signs of illness, symptoms of a condition, and social circumstances. Unlike the ICF, which focuses on functioning, the ICD offers some insights into the etiological classification by diagnosis of health condition, disorder, or disease. Coupled with the ICF, both classification schemes offer a relatively full picture of the medical and biopsychosocial aspects of the individual (Stucki, 2012).
Because this chapter focuses on understanding the ICF and demonstrating its connection to assessment, a full understanding of the ICF is of value to the reader. The ICF is a hierarchical structure consisting of two parts, each with two components. Part 1, functioning and disability, is broken into the components (1) body functions and structures, and (2) activities and participation. Part 2, contextual factors, is broken into (1) environmental factors and (2) personal factors. (Note: Types of personal factors are identified for clarity but are not classified, because every person has unique personal factors and the classification of every person's personal factors would be impossible.) In the ICF, “Each component (except personal factors) can be expressed in both positive and negative terms” (WHO, 2001, p. 10).
The ICF
domains are classified from body, individual and societal perspectives by means of two lists: a list of body functions and structure, and a list of domains of activity and participation. In the ICF, the term functioning refers to all body functions, activities and participation. The term disability is similarly an umbrella term for impairments, activity limitations and participation restrictions. The ICF also lists environmental factors that interact with all these components. (WHO, 2002, p. 2)
The ICF is
a classification of health and health-related domains—domains that help us to describe changes in body function and structure, what a person with a health condition can do in a standard environment (their level of capacity), as well as what they actually do in their usual environment (their level of performance). (WHO, 2002, p. 2)
Let's break down these concepts in order to better understand the ICF. The ICF model, as shown in figure 3.1, offers a coding system that begins with the recognition of a health condition. As delineated in the ICF, a health condition (disorder or disease) generally affects some physical (biological) or functional aspect of the individual's body structure or body function. Changes or impacts on body structure—for example, a spinal cord injury, limb amputation, or even pregnancy or aging—may affect an individual's functioning in multiple domains. The affected body structure or function affects the activities and participation of the individual in the life of the community. In addition, environmental factors contextually affect the individual in a positive (facilitator) or negative (barrier) manner. Remember, since every person is unique, the ICF does not include personal factors in the classification system but does provide examples of factors to consider.
Figure 3.1 The ICF model.
Adapted by permission from International Classification of Functioning, Disability, and Health, pg. 18, copyright 2001 (Geneva, World Health Organization); Adapted from B. Prodinger et al., “Toward the ICF Rehabilitation Set: A Minimal Generic Set of Domains for Rehabilitation as a Health Strategy,” Archives of Physical Medicine and Rehabilitation 97, no. 6 (2016): 875-884.
The impact on body structure and body function has implications for the ability of the individual to engage in activities (execution of a task) and participation (engagement in the life of the community). It is important to note that the community may range from the broader environment (e.g., city or neighborhood) to home or residential facility.
Unlike what one may perceive from the term activities (e.g., a recreational event), activities under the ICF are more discrete. Activities within the ICF refer to the specific execution of a task like manipulating objects (i.e., holding a pencil), focusing attention, or walking on different surfaces. Participation, on the other hand, may include moving around within a facility or using transportation. Together, the concepts of activities and participation are a bit different within the ICF model than how they are often used within recreational therapy practice. In recreational therapy service delivery, we often think of an activity as a game or manual arts project or exercise in a group. In the ICF model, as noted, an activity may be grasping an object, balancing on a foot, or making a decision. If a consumer cannot grasp a paint brush, they will not be able to participate in a painting experience or event. Therefore, participation in a community art class may not be possible unless the therapist assists the consumer in acquiring the skill of grasping or making a modification. So, it is important to note that the ICF classifies the functional performance of the discrete tasks or actions needed to participate in life situations. As therapists, we want to be able to assess one's functioning in such discrete tasks so that we can improve the functioning, design adapted supplies, or modify the activity to enhance engagement (participation).
In addition to body structure, body function, and activities and participation, environmental and personal factors also affect the functioning of the individual. Environmental elements include products and technology, natural environment and human-made changes to the environment, support and relationships, attitudes of others, and services, systems, and policies. The qualities (or lack thereof) of the environment, including technology, affect the ability of an individual to address functioning (e.g., a prosthetic device) and, therefore, engagement in the life of the community (see figure 3.1). Remember that personal factors, such as gender, ethnicity, religious beliefs, cultural morays, and family upbringing, are not coded because every individual is unique.
To understand the model, a brief description of each element is of value. Table 3.1 offers an explanation/definition of each component of the ICF (Rauch, Luckenkemper, & Cieza, 2012; WHO, 2001). Unlike earlier linear models of disability, the ICF model is a dynamic and interactive model that reflects the functioning of the individual and recognizes the impacts of each element in an individual's life. Each component interacts with the other components depicting this dynamic relationship. For instance, when an individual's body structure is changed, there is a subsequent impact on body function, activities, and engagement in the life of the community. When an individual engages in an activity that improves body function or structure, there is a resulting impact on activities that may also affect participation in the community. The ICF is about classifying functioning and includes those environmental factors that can facilitate functioning and engagement or serve as barriers to one's functioning.
The following sections offer a brief explanation of each element of the ICF. It is important to recognize the dynamic relationship between each element and the resulting positive or negative impact on an individual. The health condition has an impact on body structure, body function, activities, participation, and environment functioning, each altering the functioning of the individual.
Related Books