- Home
- Research Methods, Measurements, and Evaluation
- Kinesiology/Exercise and Sport Science
- Evidence-Based Practice in Exercise Science

Evidence-Based Practice in Exercise Science
The Six-Step Approach
by William E. Amonette, Kirk L. English and William J. Kraemer
344 Pages
Exercise science practitioners have access to mountains of research findings, expert opinions, novel techniques, and program plans via blogs, fitness magazines, conference presentations, and peer-reviewed journals. To facilitate effective practice, practitioners must sift through this information and retain only the best evidence to form a sound base of knowledge. Evidence-Based Practice in Exercise Science: The Six-Step Approach equips readers with the basic skills and competencies for discerning the value of scientific research. Using a methodical approach, students and professionals will learn to identify appropriate evidence to support novel interventions and avoid counterproductive or dangerous information to eliminate ineffective exercise options.
The authors, well-known advocates in the study and application of evidence-based practice in the field of exercise science, take the five-step method of evidence-based practice that has been established in medicine, adapt it specifically for exercise science, and expand it to embrace individuality in exercise training. The content is accessible for students in a variety of courses in exercise science curricula; those seeking certification through professional organizations; and practitioners in the fields of exercise, nutrition, sports medicine, and sport science.
This text is an instruction manual in understanding and applying evidence-based practice. The process is divided into six steps that begin with asking a question and then finding, evaluating, implementing, confirming, and re-evaluating the evidence. Readers of Evidence-Based Practice in Exercise Science will explore these aspects:
• The philosophy of science and design of scientific studies
• The use of search tools like PubMed and Google Scholar and how to rank or define the strength of the evidence
• Practical suggestions for implementing evidence-based practice in the field to better advise and serve athletes, clients, and patients
• Case studies that demonstrate realistic scenarios of how the evidence-based process may be used in a variety of sport and exercise settings
Each chapter opens with chapter objectives that provide a road map for learning, and a chapter conclusion summarizes main points and ensures understanding. The case studies cover topics including exercise prescription; exercise for special populations; nutrition and supplementation; and exercise devices, equipment, and apparel. Each case presents a realistic scenario that an exercise practitioner may experience, presents background information, formulates a question for investigation, describes a search of the literature, discusses the findings, and provides a recommendation for practice based on the best current evidence.
Evidence-Based Practice in Exercise Science is grouped into four sections that assist readers in gaining a better understanding of the evidence-based practice paradigm, learning the step-by-step method, and acquiring experience in the evidence-based approach by working through practical examples using real-world scenarios. Part I offers foundational knowledge of evidence-based practice in exercise sciences. Part II introduces the six-step method of evidence-based practice with chapters that explore each step of the process in depth. Part III presents 16 case studies grouped into chapters by generaal topics. Part IV concludes the text with chapters on disseminating and sharing knowledge and the future of evidence-based practice in exercise science.
By understanding the concepts and process of evidence-based practice, current and future sport, exercise, and health professionals will prescribe individualized programs and treatments that improve athletic performance and lead individuals toward better health. Embracing evidence-based practice will ultimately advance the field and produce optimal outcomes for clients, patients, and athletes.
Part I: Overview and Historical Background of Evidence-Based Practice
Chapter 1. The Need for Evidence-Based Practice in Exercise Science
Evidence-Based Practice in Action
Defining Evidence-Based Practice
Applying Evidence-Based Practice in Exercise Science
Team Approach to Evidence-Based Practice
Becoming an Evidence-Based Practitioner
Conclusion
Chapter 2. The Process of Evidence-Based Practice
The Importance of Evidence in Exercise Science
Applying the Five Steps of Evidence-Based Practice
The Case for Evidence-Based Practice
Criticisms of Evidence-Based Practice
Conclusion
Chapter 3. Philosophy, Science, and Evidence-Based Practice
Epistemology
Epistemology of Modern Science
The Paradigm of Evidence-Based Practice
Conclusions
Chapter 4. Sources of Evidence
Sources of Knowledge
Types of Evidence
Conclusion
Chapter 5. Reading and Interpreting Research Evidence
Consumers of Research
What is Research?
Components of a Research Paper
Steps to Critically Reading Research
Conclusion
Part II: The Six Steps of Evidence-Based Practice
Chapter 6. Developing a Question
Question Development Areas
Types of Questions
Components of a Foreground Question
Conclusion
Chapter 7. Searching for Evidence
Searching for Preliminary Information
Finding Peer-Reviewed Sources
Searching a Research Database
Conducting a Secondary Search From Reference Lists
Conclusion
Chapter 8. Evaluating the Evidence
Why is it Important to Rank the Evidence?
Critically Appraising the Literature
Levels of Evidence
Conclusion
Chapter 9. Incorporating Evidence into Practice
Translating Research Into Practice
Deciding When to Act on Evidence
The Influence of Evidence
Implementing Research-Based Evidence
Conclusion
Chapter 10. Confirming the Evidence in the Individual
Generalizability of Research
n-of-1 as a Model for Confirming the Evidence
Confirming the Evidence in the Individual in Exercise Science
Basic Principles in Testing and Measurement
Deciding to Continue or Discontinue an Intervention
Collaboration in Evidence-Based Practice
Conclusion
Chapter 11. Reevaluating the Evidence
Prompts to Reevaluate
Techniques to Stay Current
Conclusion
Part III: Case Studies in Evidence-Based Practice
Chapter 12. Exercise Prescription
Case Study 1: Strength Training and Cycling
Case Study 2: Static Stretching and Soccer
Case Study 3: ACL Injury Prevention in Female Athletes
Case Study 4: Single Versus Multiple Sets for Strength Improvement
Case Study 5: Models of Periodization
Conclusion
Chapter 13. Exercise for Special Populations
Case Study 1: Resistance Exercise and Functional Outcomes in Those Who Are Elderly
Case Study 2: Exercise and Cancer Cachexia
Case Study 3: Exercise and Traumatic Brain Injury
Conclusion
Chapter 14. Nutrition and Supplementation
Case Study 1: Creatine Monohydrate and Cycling
Case Study 2: Caffeine, Coffee, and Performance Enhancement
Case Study 3: Protein Intake for Endurance Athletes
Case Study 4: HMB and Strength–Power Athletes
Conclusion
Chapter 15. Exercise Devices, Equipment, and Apparel
Case Study 1: Chains
Case Study 2: Vibration and Muscle Strength and Power
Case Study 3: Instability Training and Muscle Strength
Case Study 4: Minimalist or Barefoot Running and Running Economy
Conclusion
Part IV: Integrating Evidence-Based Practice into Exercise Science
Chapter 16. Disseminating and Sharing Knowledge
Local Discussion and Networking
Conferences
Formal and Informal Publications
Conclusion
Chapter 17. The Future of Evidence-based Practice in Exercise Science
Ability, Judgment, and Evidence
Review of the Rationale for Evidence-Based Practice
The Future of Exercise and Science
Spreading the Evidence-Based Practice Philosophy
Working With Scientists
Becoming an Evidence-Based Practitioner
Conclusion
William E. Amonette, PhD, is an assistant professor and director of the exercise and health sciences program in the Department of Clinical Health and Applied Sciences at the University of Houston – Clear Lake. Prior to becoming an academician, Amonette served as an assistant strength and conditioning coach for the Chinese national basketball team at the Beijing Olympic Training Center. He was also previously the assistant strength and conditioning coach and rehabilitation coordinator for the NBA’s Houston Rockets, an astronaut strength, conditioning, and rehabilitation specialist, an exercise physiologist, and an integrated testing specialist for the Countermeasures Evaluation and Validation Project for Wyle Laboratories at NASA–Johnson Space Center.
Amonette earned his PhD at the University of Texas Medical Branch in rehabilitation sciences, with a research emphasis in clinical exercise physiology. He is a certified strength and conditioning specialist (CSCS) though the National Strength and Conditioning Association, an Associate Editor for the Journal of Strength and Conditioning Research, and ad hoc peer-reviewer for many scientific journals related to exercise and sport science.
Amonette’s research interests include physiological and mechanical predictors of sports performance and injury. He also has clinical research interest in neuroendocrine and metabolic responses to exercise in patients with traumatic brain injuries and the effect of novel exercise interventions on rehabilitation outcomes in people with disabilities. He has published numerous scientific and academic peer-reviewed journal articles, reports, and book chapters and has presented his work nationally and internationally.
Kirk L. English, PhD, is a senior scientist with JES Tech LLC, a NASA contractor, and works in the Exercise Physiology and Countermeasures Laboratory at NASA – Johnson Space Center. He is also a research scientist in the Department of Nutrition and Metabolism at the University of Texas Medical Branch (UTMB) and an adjunct professor at the University of Houston – Clear Lake, where he teaches a graduate course.
English, who is a member of the National Strength and Conditioning Association, American College of Sports Medicine, and American Physiological Society, received his PhD in rehabilitation sciences from UTMB. During his graduate studies, he was awarded a competitive three-year NASA/Texas Space Grant Consortium Graduate Fellowship. English has published numerous peer-reviewed articles, technical reports, conference abstracts, and book chapters on exercise, nutrition, aging, spaceflight, and evidence-based practice in the field of exercise science.
In his work with NASA, English’s research focuses on the prevention of spaceflight-induced decreases in skeletal muscle mass, strength, and performance. His work includes the development and validation of novel exercise protocols and hardware that are used both on the ground and during spaceflight. He also conducts all pre- and post-flight strength testing of American, European, Canadian, and Japanese International Space Station crewmembers and serves as the liaison and subject matter expert on this topic to NASA’s international partners.
William J. Kraemer, PhD, is a full professor in the Department of Human Sciences at The Ohio State University. He has also held fuull professorships at the University of Connecticut, Ball State University, and The Pennsylvania State University, including each medical school. Dr. Kraemer is a fellow of the American College of Sports Medicine, the National Strength and Conditioning Association (NSCA), and the American College of Nutrition. Among many of his professional achievements, he is a recipient of the NSCA’s Lifetime Achievement Award. He is editor in chief of the NSCA’s Journal of Strength and Conditioning Research, an editor of the European Journal of Applied Physiology, and an associate editor of the Journal of the American College of Nutrition. He holds many other editorial board positions in the field. Kraemer has published more than 450 peer-reviewed papers in scientific literature and has published 12 books. He received the 2014 Expertscape Award, which named him the nation’s top expert in resistance training research over the past ten years. With almost 40,000 citations on Harzing’s Publish or Perish lists, his scholarly impact is impressive.
Translating Research Into Practice
As discussed earlier in this book, research design is a critical element to answering questions relevant to mechanistic, practical, and clinical science. One of the key aspects of research design is control of all potential confounding factors to eliminate the possibility that the outcomes arising from the intervention (independent variable) were influenced by an external factor.
As discussed earlier in this book, research design is a critical element to answering questions relevant to mechanistic, practical, and clinical science. One of the key aspects of research design is control of all potential confounding factors to eliminate the possibility that the outcomes arising from the intervention (independent variable) were influenced by an external factor. Although experimental control is a strength of research, and in particular of randomized control trials, it can also create problems when one is implementing research evidence in client, athlete, or patient populations. Suppose a clinical scientist is interested in studying the effect of interval exercise compared to steady-state exercise on hypercholesterolemia in adults who are obese. A logical study design to address such a question would be a randomized controlled trial. Consider the following hypothetical study:
One hundred participants who were obese were selected at random and then randomly assigned to one of four groups: interval exercise, short-duration steady-state exercise, long-duration steady-state exercise, and control with no exercise. In order to eliminate potential confounding factors, the participants were free from comorbidities including hypertension, insulin resistance, diabetes, overt cardiovascular disease, and recent orthopedic injuries. Before the intervention, all groups completed a treadmill
O2 maximum test and a test of blood cholesterol; the individuals conducting both of these tests were blinded to subjects' group assignment. The interval exercise group completed a protocol consisting of 1 min of exercise at a velocity equal to 90%
On the surface, this appears to be a sound single-blind randomized controlled trial. It is in fact well-designed and controlled, but there are some potential problems when a practitioner considers implementation. Because the scientists were interested in studying training responses to an intervention in obesity alone, they eliminated subjects with diabetes, hypertension, and other common comorbidities. This was a good decision for internal validity, but not for external validity; practitioners rarely treat individuals who are obese without any of these companion conditions (Castro, Kolka, Kim, & Bergman, 2014; Despres et al., 2008). Thus, practitioners are left to wonder whether the evidence is truly applicable to their patients or clients.
A second possible problem with the evidence is the elimination of secondary interventions. Strengths of a scientific experiment may actually be perceived as weaknesses with regard to practical implementation. In practice, multiple interventions are often implemented in concert with one another. This hypothetical experiment evaluated the effectiveness of interval versus steady-state treadmill exercise alone. An exercise practitioner is unlikely to implement the interval training protocol in isolation; instead, the protocol may be combined with resistance training, a healthy diet, and other behavioral modifications. Implementation of such multifaceted protocols may enhance the effectiveness of either of the interventions. Conversely, the addition of such interventions may also reduce the effectiveness of the protocol. Obviously, it is not scientifically plausible that resistance exercise would cause an increase in cholesterol or biologically negate the effects of the interval training protocol. However, it is possible that implementation of the secondary intervention will lead to overtraining, injury, soreness, and perhaps poor adherence to the protocol due to each of these secondary results of the combined protocol. Again, this is not likely, but it is certainly something the practitioner must consider.
Another potential problem with the implementation of scientific evidence is the possibility that a client may not be able to tolerate the protocol. For example, the initial fitness level of the client may not be sufficient to enable him to tolerate its rigors. The practitioner is then left to decide whether a modified version of the research protocol will be effective in improving blood cholesterol profiles. It is also possible that the protocol used in the scientific experiment will result in undertraining in some individuals; that is, in contrast to the previous scenario, the intensity of the stimulus may be insufficient to induce a training response. The exercise practitioner must then decide how to effectively alter the training loads in order to induce a similar response in a client or patient with a greater initial fitness level. In situations like these, it is often helpful to consult the discussion section of the research paper. Often the authors discuss in great detail the programmatic elements that they believe are responsible for the particular adaptations they observed; for instance, they may note that their subjects completed 10 intervals (with positive outcomes) in contrast to a previous study in the same population that used four intervals with negative findings. Mechanistic evidence, from either the same study or another, would further elucidate the cause(s) for the positive adaptations from a higher volume of exercise.
In medicine, one of the often cited criticisms of the evidence-based philosophy is that it leads to a cookbook approach to practice (Sackett, Rosenberg, Gray, Haynes, & Richardson, 1996). Opponents assert that evidence-based practitioners read scientific papers and then implement the protocols directly from the papers. The example we have presented illustrates that there really is no "recipe" for prescription; that is not the purpose of science. Because people are different, protocols may need to be altered to fit individual patient or client needs. Science influences the "ingredients" of the prescription. This hypothetical experiment demonstrates that interval exercise might be more effective than steady-state treadmill exercise in improving blood cholesterol of patients who are obese. It also provides some basic parameters for intensity, volume, mode, and so on for the implementation of a protocol. Practitioners must then decide whether to implement the protocol. They must also decide how they should implement interval exercise in a manner that is best suited to their client's, patient's, or athlete's individual needs and experience level.
Learn more about Evidence-Based Practice in Exercise Science.
Case Study 2: Vibration and Muscle Strength and Power
Charity is a university strength and conditioning coach. Recently, a professor in the school’s exercise physiology program acquired several vibration plates for a planned research study. The vibration plates are housed in the athletic training facility and are available to the athletes.
Charity is a university strength and conditioning coach. Recently, a professor in the school's exercise physiology program acquired several vibration plates for a planned research study. The vibration plates are housed in the athletic training facility and are available to the athletes. Charity heard about training with vibration plates at a national conference she attended recently; the presenter described a variety of upper and lower body exercises that could be performed on the plate and anecdotally claimed that such training results in noticeable performance improvements in athletes participating in a variety of sports. As an evidence-based practitioner, Charity realizes that although the vibration plate presentation was compelling, she needs to search the literature to determine what kind of scientific support exists for using vibration plate training as a modality to improve physiological and athletic performance.
Background
Vibration is thought to enhance acute neuromuscular performance via the stimulation of Ia afferent nerves, which effects a myotatic reflex contraction (Abercromby et al., 2007). Acutely, vibration improves maximal force and power output during concentric contractions; this facilitative effect is greater in elite athletes than in amateurs (Issurin & Tenenbaum, 1999; Liebermann & Issurin, 1997). However, vibration is ineffective when applied acutely to promote recovery or improve subsequent running performance after a strenuous exercise bout in highly fit runners (Edge, Mundel, Weir, & Cochrane, 2009). In competitive athletes, routine vibration training can increase strength, jump performance, and flexibility (Fagnani, Giombini, Di Cesare, Pigozzi, & Di Salvo, 2006), as well as improve proprioception and balance after anterior cruciate ligament reconstruction in comparison to a conventional rehabilitation program (Moezy, Olyaei, Hadian, Razi, & Faghihzadeh, 2008).
Charity currently employs evidence-based strength and conditioning programs with her athletes; these programs consist largely of resistance exercise - both traditional strength and explosive Olympic weightlifting exercises. Thus, to make a valid comparison in her athletic population, Charity should compare the effectiveness of vibration training to that of traditional resistance exercise. Given the limitations of vibration training (cost, availability, spatial restrictions), only if vibration training (either alone or in combination with traditional training) proves superior to traditional training would it be prudent to incorporate it on a large scale. Thus the evidence-based question is as follows.
In trained athletes, does vibration training, either alone or as an adjunct to resistance exercise, elicit improvements in muscle strength or power that are superior to those realized with traditional resistance training?
Search Strategy
Typing "vibration" into PubMed yields a list of MeSH subheadings; we select "vibration training." This returns 1141 studies. Activating the Age filter (Adult: 19-44 years) and Language filter (English) reduces this number to 377. Next, we add "AND athletes" to the search string ("vibration training AND athletes"), which returns 20 articles. Scanning these abstracts reveals 3 papers directly related to the chronic effects of vibration training (Delecluse et al., 2005; Issurin, Liebermann, & Tenenbaum, 1994; Preatoni et al., 2012). Of the 17 articles not included, most are acute studies and several others examine the effects of vibration on postworkout recovery and postsurgical rehabilitation outcomes; another study was excluded because it is not clear what exercise the control group performed.
Discussion of Results
The three articles reviewed are summarized in table 15.2. Preatoni and colleagues (2012) evaluated the effects of vibration training alone and in combination with traditional resistance training in 18 national-level female athletes (12 soccer and 6 softball athletes, with equal proportions in all groups). Subjects were randomized to one of three groups: (1) whole-body vibration training group, (2) traditional strength training group, and (3) combined whole-body vibration and strength training group. All training was performed during the winter preparatory period and in combination with other sport-specific field training such as speed drills, aerobic work, and technical and tactical skill practice. The periodized resistance training program was performed 2 days per week for 8 weeks; for the first week it consisted of six sets × six repetitions of squats performed at body weight with vibration (vibration group), at 60% 1RM (strength training group), or 30% 1RM with vibration (combined whole-body vibration and strength training group). Every 2 weeks, the external load was increased 6% (for the strength training group) and 3% (for the combined whole-body vibration and strength training group); greater intensity for the vibration group was achieved by increasing vibration frequency 5 Hz every 2 weeks (frequency was also increased for the combined group). Outcome measures included isometric strength (leg press); dynamic force, velocity, and power (explosive leg press with loads of 100% to 200% body weight in 20% increments); and power and power endurance (vertical jump and continuous 15-s vertical jumps, respectively). Training increased isometric strength (main effect, P = 0.02) with no differences between groups. No changes were observed for any parameter of the explosive leg press test. Performance on both vertical jump tests increased with training (main effect, P < 0.002), but there were no differences between groups. Maximum jump height (vertical jump test) and mean jump height and power (continuous 15-s vertical jump test) were increased only in the strength-trained group. The investigators also evaluated the characteristics of the vibration device (i.e., frequency, amplitude, and acceleration) and found variations up to 20% from the selected value; this was particularly true at higher frequencies. On the basis of other published data (Blottner et al., 2006; Mulder et al., 2008, 2007; Rittweger et al., 2006), the authors conclude that vibration exercise can elicit similar or improved outcomes compared to traditional strength training only when similar external loads are used; that is, they attribute the lack of an effect in their study to the lower external loads lifted by the combined vibration + strength training group (Preatoni et al., 2012).

Delecluse and colleagues (2005) examined the additive effect of a whole-body vibration training program over 5 weeks in 20 sprinters. Male and female sprinters (mean 100 m times: female = 12.46 ± 0.59 s, male = 11.45 ± 0.42 s) were randomly assigned to either a vibration or a control group. Both groups maintained their conventional training program, which consisted of intervals (10-60 s), speed training (two or three sessions per week with efforts near race pace), speed drills (two sessions per week), plyometric drills (one session per week), and explosive resistance training (three sessions per week) at 75% to 95% 1RM (three to five sets × two to five repetitions). In addition to their typical training, the vibration group completed three sessions per week of unloaded static and dynamic leg exercise on a vibration platform. The exercises employed were high squat, deep squat, wide stance squat, single-leg squat, lunge, and heel raise. The vibration program was implemented progressively through increases in the duration of vibration time and concomitant decreases in the rest periods; vibration amplitude (displacement) and frequency were also increased over the 5-week program. The study was conducted during the precompetitive phase of training. Outcome measures included strength (isometric and isokinetic knee extensor-flexor), maximal knee extension velocity (at 1%, 20%, 40%, and 60% of maximum isometric force), vertical jump, starting parameters (start time, horizontal start velocity, and horizontal start acceleration), and maximum velocity in a 30 m sprint. There were no changes in either group after the 5-week training program, nor were there any interaction effects or differences between groups posttraining.
Issurin, Liebermann, and Tenenbaum (1994) examined the effects of vibration training in 28 young male athletes who regularly participated in a wide cross section of club or varsity sports such as judo, swimming, volleyball, tennis, soccer, track and field, and cycling. Subjects were randomized to one of three groups: (1) upper body strength training with vibration and lower body flexibility training, (2) upper body strength training and lower body flexibility training with vibration, and (3) a calisthenics - basketball game control. The training program, which was conducted three times per week for 3 weeks, consisted of a ~10-min warm-up, a single upper body strength exercise (seated bench pull: six sets × six repetitions at 80% to 100% 1RM performed to failure), and ~20 min of specific static and ballistic stretching of the upper leg musculature. The program was performed by both experimental groups; vibration was added to either the upper or lower body activity according to group assignment. Outcome measures included strength (bench pull 1RM) and flexibility (two-leg split distance and sit and reach distance). Collectively, 1RM strength and both flexibility measures increased with training (main effects); there were also differences between groups for each outcome (group × time interaction effect). Unfortunately, the authors did not provide statistical contrasts between groups (e.g., strength training vs. strength training with vibration) to elucidate the between-group differences; because of the influence of the control group (which changed very little for any measure) on both main and interaction effects, it is difficult to interpret the study findings.
Luo, NcNamara, and Moran (2005) published a review evaluating the effects of vibration training on muscle strength and power, examining the effects of both chronic and acute vibration training. In 2005, only three papers had been published on the chronic adaptations to vibration training; of these, only one study employed trained athletes as subjects and has already been discussed (Issurin et al., 1994).
Conclusion and Strength of Evidence
There has been an explosion of literature regarding whole-body vibration in recent years. Some studies have been well conducted; others are poorly designed or uncontrolled, leading to erroneous or equivocal conclusions. There is still minimal understanding of the appropriate frequency, amplitude, direction, and length and mode of exercise needed for positive adaptations to vibration training. Despite the widespread use of vibration in athletic and private training settings, the evidence at the current time does not suggest that it is a strong tool to improve strength in athletically trained populations, although there is evidence for use in other populations.
There is level B evidence to refute the use of vibration training as a stand-alone or adjunct training method to increase muscle strength or power in athletes, as it is not demonstrably superior to traditional resistance exercise.
Program Recommendations
Although evidence supports vibration as a tool to improve strength and power in untrained populations, the data do not support its use to improve performance in athletes versus traditional strength methods. There is some evidence to support its use as a tool to acutely potentiate a power response; thus if Charity chooses to implement vibration, based on the literature it should be used as a postexcitatory potentiation tool. In general, Charity should continue training her athletes using traditional strength and conditioning programs but continue to watch the literature for emergent studies and protocols.
Save
Learn more about Evidence-Based Practice in Exercise Science.
Evidence-Based Practice in Action
On September 9, 2007, the second week of the 2007-2008 National Football League (NFL) season, the Buffalo Bills were at home for a game with the Denver Broncos. On a routine kickoff, third-year tight end Kevin Everett sprinted down the field and approached the kick returner, Domenik Hixon (Carchidi, 2008).
On September 9, 2007, the second week of the 2007-2008 National Football League (NFL) season, the Buffalo Bills were at home for a game with the Denver Broncos. On a routine kickoff, third-year tight end Kevin Everett sprinted down the field and approached the kick returner, Domenik Hixon (Carchidi, 2008). Everett dropped his center of gravity and extended into Hixon for the tackle - a motor skill that he had presumably performed thousands of times previously. Everett led with the crown of his helmet, contacting the helmet of Hixon at a high velocity, inadvertently violating a common but too often disregarded fundamental of tackling. The consequences of the collision were devastating and nearly fatal for Everett.
Immediately upon impact, Everett fell to the ground and lay face down, motionless. The collision resulted in a fracture dislocation of his third and fourth cervical vertebrae, injuring the spinal cord and instantly paralyzing Everett (Cappuccino et al., 2010; Carchidi, 2008). The sports medicine staff reacted quickly to the injury, clearing the scene to ensure that Everett was not injured further. With an injury such as Everett's, the standard-of-care protocol provides that the helmet remain on, the player be placed on a board, the face mask removed, and the player carefully moved to a stretcher and then transported by ambulance directly to the hospital. The sports medicine staff appeared to perfectly execute the protocol, and Everett was carefully transported to Millard Fillmore Gates Hospital (Carchidi, 2008).
In the ambulance ride en route to the hospital, the neurosurgery team used an experimental therapy that they hoped would improve Everett's prognosis. Infusing a cold saline solution into Everett's veins, the medical team induced a mild hypothermic state (Cappuccino et al., 2010). The use of ice to treat an injury is not novel - ice is used acutely for virtually every orthopedic injury. The principle of inducing systemic hypothermia is similar. The cold saline solution acutely controls systemic inflammation, and the medical team apparently believed that the therapy would reduce inflammation surrounding the spinal cord injury, preventing further damage (Cappuccino et al., 2010; Mummaneni, 2010). After evaluation by the medical staff, the neurosurgeon performed an emergency surgery in an attempt to save Everett's life (Cappuccino et al., 2010). After the surgery, Everett was placed on a respirator; it was believed that if he lived, he was unlikely to ever walk again (Carchidi, 2008).
Two days after the injury, Everett was removed from the respirator; he was reported to have minimal voluntary movements in his lower extremities, suggesting a theoretical possibility that he could regain the ability to walk (Cappuccino et al., 2010). On the basis on previous cases, the medical team believed that Everett had a small chance of regaining full control of his extremities (Carchidi, 2008). In the weeks and months that followed, Everett made remarkable progress, recovering at a rate far greater than expected. He was transferred to a top rehabilitation center for neurologic injuries in Houston, Texas, that implemented a comprehensive rehabilitation program. On December 23, 2007, Kevin Everett walked onto the field of Ralph Wilson Stadium - a remarkable feat that a few short months earlier had seemed impossible.
Kevin Everett's recovery was remarkable and a testament to the professional competence and readiness of the integrated sports medicine team, who made numerous decisions improving the chances that he might walk. Everett's story is also a demonstration of personal determination and perseverance that has inspired hope. For patients suffering severe spinal cord injuries, the story validates that dramatic recovery is possible. Medical personnel are encouraged in that Everett's case shows that diligent medical and rehabilitative therapy facilitates recovery. However, there is one overriding question that surrounds Kevin Everett's case: Why did he recover and why so fast? There are a number of possible explanations:
- Everett's recovery was simply a statistical improbability - he was an outlier and his recovery a chance occurrence.
- It was the result of sheer human determination and will in an athlete who simply would not accept his prognosis and would give everything to ensure he had the best chance to walk.
- It was the result of the sports medicine team's careful execution of the standard-of-care practice to prevent further injury immediately post-accident.
- Everett's recovery was the result of the precise execution of the neurosurgery team.
- The recovery was a result of the rehabilitation protocol implemented by a leading neurorehabilitation center.
- The rapid recovery was the result of cryotherapy, an experimental method that dramatically improved his prognosis.
The case of Kevin Everett highlights an important concept, that knowledge is a dynamic phenomenon (Amonette et al., 2010). The team of doctors, physical therapists, athletic trainers, and exercise specialists involved in the acute and postacute treatment of Everett's injury made numerous decisions that positively or negatively affected his outcome. The athletic trainers and sports medicine staff identified a possible injury to the spine and ensured that the athlete was quickly transported to the hospital. A careful procedure was used to move him to avoid further injury. The physicians made a decision to use the hypothermic technique to reduce spinal swelling. The neurosurgeon decided to perform surgery, and at some point, a physician determined that it was safe to remove Everett from the ventilator. In the rehabilitative process, physical therapists along with the medical team decided which therapeutic interventions were best suited to the stage of injury and made daily decisions on when to increase, decrease, or hold parameters like the intensity, volume, and duration of the rehabilitation program.
How did the sports medicine team determine the appropriate treatment?
Learn more about Evidence-Based Practice in Exercise Science.
Steps to Reading Research Critically
Reading and interpreting research may be one of the most important tasks of an evidence-based practitioner. It is important to develop the skills necessary to identify the key findings and to disregard the superfluous information.
Reading and interpreting research may be one of the most important tasks of an evidence-based practitioner. It is important to develop the skills necessary to identify the key findings and to disregard the superfluous information. Although critical appraisal is a topic left to a later chapter, next we present some practical guidelines for reading research evidence.
1-2. Read the Title and Abstract
The title of a research article can provide an important clue to the most important findings in the manuscript. But you should never read only the title and abstract. Some journal titles explicitly state the major finding of the paper. In a 1989 publication in Archives of Neurology, an article titled "Focused Stroke Rehabilitation Programs Improve Outcome" appears on pages 700-701 (Reding & McDowell, 1989) (figure 5.7). From the title alone, without reading the paper or the abstract, the reader learns that the investigators determined that a stroke rehabilitation program was effective in improving clinical outcomes. However, the very next article in the same volume of Archives of Neurology is titled "Focused Stroke Rehabilitation Programs Do Not Improve Outcome" (Dobkin, 1989) (figure 5.7). Which article is correct?
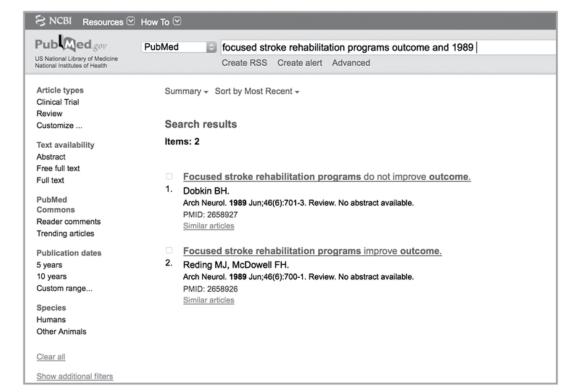
Two studies with directly contradictory titles that appeared consecutively in 1989 in Archives of Neurology.
Reprinted from PubMed.gov.
When the evidence-based practitioner relies on the title or abstract alone, he can make significant mistakes in the interpretation of research evidence. Also, examples such as the one just presented clearly show that research can be contradictory. The practitioner should read the title and abstract to determine whether the paper is relevant to the evidence-based question. If it is, he should proceed to a more careful reading and analysis to determine if the study methods and results support the findings stated in the abstract and title.
3. Read the Purpose, Construct, Theory, or Hypothesis Statement
After reading the title and abstract to determine the relevance of the study to the evidence-based question, the practitioner can skip to the final statement in the introduction that presents the study purpose, construct, theory, or hypothesis statement. This should provide the information needed to determine how the study should be designed to best answer the research question.
4. Read the Methods and Look for Flaws
The methods section is the most important part of a paper to read carefully and critically. It is from the methods section that an evidence-based practitioner can determine many of the potential biases and confounding factors associated with the study. This is also the section of the paper that determines the level or strength of evidence (chapter 8) provided by the research. As authors critically appraise their own research, they should carefully consider the study design, testing protocols, devices used, training and intervention protocols, statistical analyses, and study group allocations. If the authors are unclear in their presentation of any component of the methods, this should be a "red flag" to the reader and could potentially be a fatal flaw in the design.
Additional steps found inside Evidence-Based Practice in Exercise Science.
Translating Research Into Practice
As discussed earlier in this book, research design is a critical element to answering questions relevant to mechanistic, practical, and clinical science. One of the key aspects of research design is control of all potential confounding factors to eliminate the possibility that the outcomes arising from the intervention (independent variable) were influenced by an external factor.
As discussed earlier in this book, research design is a critical element to answering questions relevant to mechanistic, practical, and clinical science. One of the key aspects of research design is control of all potential confounding factors to eliminate the possibility that the outcomes arising from the intervention (independent variable) were influenced by an external factor. Although experimental control is a strength of research, and in particular of randomized control trials, it can also create problems when one is implementing research evidence in client, athlete, or patient populations. Suppose a clinical scientist is interested in studying the effect of interval exercise compared to steady-state exercise on hypercholesterolemia in adults who are obese. A logical study design to address such a question would be a randomized controlled trial. Consider the following hypothetical study:
One hundred participants who were obese were selected at random and then randomly assigned to one of four groups: interval exercise, short-duration steady-state exercise, long-duration steady-state exercise, and control with no exercise. In order to eliminate potential confounding factors, the participants were free from comorbidities including hypertension, insulin resistance, diabetes, overt cardiovascular disease, and recent orthopedic injuries. Before the intervention, all groups completed a treadmill
On the surface, this appears to be a sound single-blind randomized controlled trial. It is in fact well-designed and controlled, but there are some potential problems when a practitioner considers implementation. Because the scientists were interested in studying training responses to an intervention in obesity alone, they eliminated subjects with diabetes, hypertension, and other common comorbidities. This was a good decision for internal validity, but not for external validity; practitioners rarely treat individuals who are obese without any of these companion conditions (Castro, Kolka, Kim, & Bergman, 2014; Despres et al., 2008). Thus, practitioners are left to wonder whether the evidence is truly applicable to their patients or clients.
A second possible problem with the evidence is the elimination of secondary interventions. Strengths of a scientific experiment may actually be perceived as weaknesses with regard to practical implementation. In practice, multiple interventions are often implemented in concert with one another. This hypothetical experiment evaluated the effectiveness of interval versus steady-state treadmill exercise alone. An exercise practitioner is unlikely to implement the interval training protocol in isolation; instead, the protocol may be combined with resistance training, a healthy diet, and other behavioral modifications. Implementation of such multifaceted protocols may enhance the effectiveness of either of the interventions. Conversely, the addition of such interventions may also reduce the effectiveness of the protocol. Obviously, it is not scientifically plausible that resistance exercise would cause an increase in cholesterol or biologically negate the effects of the interval training protocol. However, it is possible that implementation of the secondary intervention will lead to overtraining, injury, soreness, and perhaps poor adherence to the protocol due to each of these secondary results of the combined protocol. Again, this is not likely, but it is certainly something the practitioner must consider.
Another potential problem with the implementation of scientific evidence is the possibility that a client may not be able to tolerate the protocol. For example, the initial fitness level of the client may not be sufficient to enable him to tolerate its rigors. The practitioner is then left to decide whether a modified version of the research protocol will be effective in improving blood cholesterol profiles. It is also possible that the protocol used in the scientific experiment will result in undertraining in some individuals; that is, in contrast to the previous scenario, the intensity of the stimulus may be insufficient to induce a training response. The exercise practitioner must then decide how to effectively alter the training loads in order to induce a similar response in a client or patient with a greater initial fitness level. In situations like these, it is often helpful to consult the discussion section of the research paper. Often the authors discuss in great detail the programmatic elements that they believe are responsible for the particular adaptations they observed; for instance, they may note that their subjects completed 10 intervals (with positive outcomes) in contrast to a previous study in the same population that used four intervals with negative findings. Mechanistic evidence, from either the same study or another, would further elucidate the cause(s) for the positive adaptations from a higher volume of exercise.
In medicine, one of the often cited criticisms of the evidence-based philosophy is that it leads to a cookbook approach to practice (Sackett, Rosenberg, Gray, Haynes, & Richardson, 1996). Opponents assert that evidence-based practitioners read scientific papers and then implement the protocols directly from the papers. The example we have presented illustrates that there really is no "recipe" for prescription; that is not the purpose of science. Because people are different, protocols may need to be altered to fit individual patient or client needs. Science influences the "ingredients" of the prescription. This hypothetical experiment demonstrates that interval exercise might be more effective than steady-state treadmill exercise in improving blood cholesterol of patients who are obese. It also provides some basic parameters for intensity, volume, mode, and so on for the implementation of a protocol. Practitioners must then decide whether to implement the protocol. They must also decide how they should implement interval exercise in a manner that is best suited to their client's, patient's, or athlete's individual needs and experience level.
Learn more about Evidence-Based Practice in Exercise Science.
Case Study 2: Vibration and Muscle Strength and Power
Charity is a university strength and conditioning coach. Recently, a professor in the school’s exercise physiology program acquired several vibration plates for a planned research study. The vibration plates are housed in the athletic training facility and are available to the athletes.
Charity is a university strength and conditioning coach. Recently, a professor in the school's exercise physiology program acquired several vibration plates for a planned research study. The vibration plates are housed in the athletic training facility and are available to the athletes. Charity heard about training with vibration plates at a national conference she attended recently; the presenter described a variety of upper and lower body exercises that could be performed on the plate and anecdotally claimed that such training results in noticeable performance improvements in athletes participating in a variety of sports. As an evidence-based practitioner, Charity realizes that although the vibration plate presentation was compelling, she needs to search the literature to determine what kind of scientific support exists for using vibration plate training as a modality to improve physiological and athletic performance.
Background
Vibration is thought to enhance acute neuromuscular performance via the stimulation of Ia afferent nerves, which effects a myotatic reflex contraction (Abercromby et al., 2007). Acutely, vibration improves maximal force and power output during concentric contractions; this facilitative effect is greater in elite athletes than in amateurs (Issurin & Tenenbaum, 1999; Liebermann & Issurin, 1997). However, vibration is ineffective when applied acutely to promote recovery or improve subsequent running performance after a strenuous exercise bout in highly fit runners (Edge, Mundel, Weir, & Cochrane, 2009). In competitive athletes, routine vibration training can increase strength, jump performance, and flexibility (Fagnani, Giombini, Di Cesare, Pigozzi, & Di Salvo, 2006), as well as improve proprioception and balance after anterior cruciate ligament reconstruction in comparison to a conventional rehabilitation program (Moezy, Olyaei, Hadian, Razi, & Faghihzadeh, 2008).
Charity currently employs evidence-based strength and conditioning programs with her athletes; these programs consist largely of resistance exercise - both traditional strength and explosive Olympic weightlifting exercises. Thus, to make a valid comparison in her athletic population, Charity should compare the effectiveness of vibration training to that of traditional resistance exercise. Given the limitations of vibration training (cost, availability, spatial restrictions), only if vibration training (either alone or in combination with traditional training) proves superior to traditional training would it be prudent to incorporate it on a large scale. Thus the evidence-based question is as follows.
In trained athletes, does vibration training, either alone or as an adjunct to resistance exercise, elicit improvements in muscle strength or power that are superior to those realized with traditional resistance training?
Search Strategy
Typing "vibration" into PubMed yields a list of MeSH subheadings; we select "vibration training." This returns 1141 studies. Activating the Age filter (Adult: 19-44 years) and Language filter (English) reduces this number to 377. Next, we add "AND athletes" to the search string ("vibration training AND athletes"), which returns 20 articles. Scanning these abstracts reveals 3 papers directly related to the chronic effects of vibration training (Delecluse et al., 2005; Issurin, Liebermann, & Tenenbaum, 1994; Preatoni et al., 2012). Of the 17 articles not included, most are acute studies and several others examine the effects of vibration on postworkout recovery and postsurgical rehabilitation outcomes; another study was excluded because it is not clear what exercise the control group performed.
Discussion of Results
The three articles reviewed are summarized in table 15.2. Preatoni and colleagues (2012) evaluated the effects of vibration training alone and in combination with traditional resistance training in 18 national-level female athletes (12 soccer and 6 softball athletes, with equal proportions in all groups). Subjects were randomized to one of three groups: (1) whole-body vibration training group, (2) traditional strength training group, and (3) combined whole-body vibration and strength training group. All training was performed during the winter preparatory period and in combination with other sport-specific field training such as speed drills, aerobic work, and technical and tactical skill practice. The periodized resistance training program was performed 2 days per week for 8 weeks; for the first week it consisted of six sets × six repetitions of squats performed at body weight with vibration (vibration group), at 60% 1RM (strength training group), or 30% 1RM with vibration (combined whole-body vibration and strength training group). Every 2 weeks, the external load was increased 6% (for the strength training group) and 3% (for the combined whole-body vibration and strength training group); greater intensity for the vibration group was achieved by increasing vibration frequency 5 Hz every 2 weeks (frequency was also increased for the combined group). Outcome measures included isometric strength (leg press); dynamic force, velocity, and power (explosive leg press with loads of 100% to 200% body weight in 20% increments); and power and power endurance (vertical jump and continuous 15-s vertical jumps, respectively). Training increased isometric strength (main effect, P = 0.02) with no differences between groups. No changes were observed for any parameter of the explosive leg press test. Performance on both vertical jump tests increased with training (main effect, P < 0.002), but there were no differences between groups. Maximum jump height (vertical jump test) and mean jump height and power (continuous 15-s vertical jump test) were increased only in the strength-trained group. The investigators also evaluated the characteristics of the vibration device (i.e., frequency, amplitude, and acceleration) and found variations up to 20% from the selected value; this was particularly true at higher frequencies. On the basis of other published data (Blottner et al., 2006; Mulder et al., 2008, 2007; Rittweger et al., 2006), the authors conclude that vibration exercise can elicit similar or improved outcomes compared to traditional strength training only when similar external loads are used; that is, they attribute the lack of an effect in their study to the lower external loads lifted by the combined vibration + strength training group (Preatoni et al., 2012).
Delecluse and colleagues (2005) examined the additive effect of a whole-body vibration training program over 5 weeks in 20 sprinters. Male and female sprinters (mean 100 m times: female = 12.46 ± 0.59 s, male = 11.45 ± 0.42 s) were randomly assigned to either a vibration or a control group. Both groups maintained their conventional training program, which consisted of intervals (10-60 s), speed training (two or three sessions per week with efforts near race pace), speed drills (two sessions per week), plyometric drills (one session per week), and explosive resistance training (three sessions per week) at 75% to 95% 1RM (three to five sets × two to five repetitions). In addition to their typical training, the vibration group completed three sessions per week of unloaded static and dynamic leg exercise on a vibration platform. The exercises employed were high squat, deep squat, wide stance squat, single-leg squat, lunge, and heel raise. The vibration program was implemented progressively through increases in the duration of vibration time and concomitant decreases in the rest periods; vibration amplitude (displacement) and frequency were also increased over the 5-week program. The study was conducted during the precompetitive phase of training. Outcome measures included strength (isometric and isokinetic knee extensor-flexor), maximal knee extension velocity (at 1%, 20%, 40%, and 60% of maximum isometric force), vertical jump, starting parameters (start time, horizontal start velocity, and horizontal start acceleration), and maximum velocity in a 30 m sprint. There were no changes in either group after the 5-week training program, nor were there any interaction effects or differences between groups posttraining.
Issurin, Liebermann, and Tenenbaum (1994) examined the effects of vibration training in 28 young male athletes who regularly participated in a wide cross section of club or varsity sports such as judo, swimming, volleyball, tennis, soccer, track and field, and cycling. Subjects were randomized to one of three groups: (1) upper body strength training with vibration and lower body flexibility training, (2) upper body strength training and lower body flexibility training with vibration, and (3) a calisthenics - basketball game control. The training program, which was conducted three times per week for 3 weeks, consisted of a ~10-min warm-up, a single upper body strength exercise (seated bench pull: six sets × six repetitions at 80% to 100% 1RM performed to failure), and ~20 min of specific static and ballistic stretching of the upper leg musculature. The program was performed by both experimental groups; vibration was added to either the upper or lower body activity according to group assignment. Outcome measures included strength (bench pull 1RM) and flexibility (two-leg split distance and sit and reach distance). Collectively, 1RM strength and both flexibility measures increased with training (main effects); there were also differences between groups for each outcome (group × time interaction effect). Unfortunately, the authors did not provide statistical contrasts between groups (e.g., strength training vs. strength training with vibration) to elucidate the between-group differences; because of the influence of the control group (which changed very little for any measure) on both main and interaction effects, it is difficult to interpret the study findings.
Luo, NcNamara, and Moran (2005) published a review evaluating the effects of vibration training on muscle strength and power, examining the effects of both chronic and acute vibration training. In 2005, only three papers had been published on the chronic adaptations to vibration training; of these, only one study employed trained athletes as subjects and has already been discussed (Issurin et al., 1994).
Conclusion and Strength of Evidence
There has been an explosion of literature regarding whole-body vibration in recent years. Some studies have been well conducted; others are poorly designed or uncontrolled, leading to erroneous or equivocal conclusions. There is still minimal understanding of the appropriate frequency, amplitude, direction, and length and mode of exercise needed for positive adaptations to vibration training. Despite the widespread use of vibration in athletic and private training settings, the evidence at the current time does not suggest that it is a strong tool to improve strength in athletically trained populations, although there is evidence for use in other populations.
There is level B evidence to refute the use of vibration training as a stand-alone or adjunct training method to increase muscle strength or power in athletes, as it is not demonstrably superior to traditional resistance exercise.
Program Recommendations
Although evidence supports vibration as a tool to improve strength and power in untrained populations, the data do not support its use to improve performance in athletes versus traditional strength methods. There is some evidence to support its use as a tool to acutely potentiate a power response; thus if Charity chooses to implement vibration, based on the literature it should be used as a postexcitatory potentiation tool. In general, Charity should continue training her athletes using traditional strength and conditioning programs but continue to watch the literature for emergent studies and protocols.
Save
Learn more about Evidence-Based Practice in Exercise Science.
Evidence-Based Practice in Action
On September 9, 2007, the second week of the 2007-2008 National Football League (NFL) season, the Buffalo Bills were at home for a game with the Denver Broncos. On a routine kickoff, third-year tight end Kevin Everett sprinted down the field and approached the kick returner, Domenik Hixon (Carchidi, 2008).
On September 9, 2007, the second week of the 2007-2008 National Football League (NFL) season, the Buffalo Bills were at home for a game with the Denver Broncos. On a routine kickoff, third-year tight end Kevin Everett sprinted down the field and approached the kick returner, Domenik Hixon (Carchidi, 2008). Everett dropped his center of gravity and extended into Hixon for the tackle - a motor skill that he had presumably performed thousands of times previously. Everett led with the crown of his helmet, contacting the helmet of Hixon at a high velocity, inadvertently violating a common but too often disregarded fundamental of tackling. The consequences of the collision were devastating and nearly fatal for Everett.
Immediately upon impact, Everett fell to the ground and lay face down, motionless. The collision resulted in a fracture dislocation of his third and fourth cervical vertebrae, injuring the spinal cord and instantly paralyzing Everett (Cappuccino et al., 2010; Carchidi, 2008). The sports medicine staff reacted quickly to the injury, clearing the scene to ensure that Everett was not injured further. With an injury such as Everett's, the standard-of-care protocol provides that the helmet remain on, the player be placed on a board, the face mask removed, and the player carefully moved to a stretcher and then transported by ambulance directly to the hospital. The sports medicine staff appeared to perfectly execute the protocol, and Everett was carefully transported to Millard Fillmore Gates Hospital (Carchidi, 2008).
In the ambulance ride en route to the hospital, the neurosurgery team used an experimental therapy that they hoped would improve Everett's prognosis. Infusing a cold saline solution into Everett's veins, the medical team induced a mild hypothermic state (Cappuccino et al., 2010). The use of ice to treat an injury is not novel - ice is used acutely for virtually every orthopedic injury. The principle of inducing systemic hypothermia is similar. The cold saline solution acutely controls systemic inflammation, and the medical team apparently believed that the therapy would reduce inflammation surrounding the spinal cord injury, preventing further damage (Cappuccino et al., 2010; Mummaneni, 2010). After evaluation by the medical staff, the neurosurgeon performed an emergency surgery in an attempt to save Everett's life (Cappuccino et al., 2010). After the surgery, Everett was placed on a respirator; it was believed that if he lived, he was unlikely to ever walk again (Carchidi, 2008).
Two days after the injury, Everett was removed from the respirator; he was reported to have minimal voluntary movements in his lower extremities, suggesting a theoretical possibility that he could regain the ability to walk (Cappuccino et al., 2010). On the basis on previous cases, the medical team believed that Everett had a small chance of regaining full control of his extremities (Carchidi, 2008). In the weeks and months that followed, Everett made remarkable progress, recovering at a rate far greater than expected. He was transferred to a top rehabilitation center for neurologic injuries in Houston, Texas, that implemented a comprehensive rehabilitation program. On December 23, 2007, Kevin Everett walked onto the field of Ralph Wilson Stadium - a remarkable feat that a few short months earlier had seemed impossible.
Kevin Everett's recovery was remarkable and a testament to the professional competence and readiness of the integrated sports medicine team, who made numerous decisions improving the chances that he might walk. Everett's story is also a demonstration of personal determination and perseverance that has inspired hope. For patients suffering severe spinal cord injuries, the story validates that dramatic recovery is possible. Medical personnel are encouraged in that Everett's case shows that diligent medical and rehabilitative therapy facilitates recovery. However, there is one overriding question that surrounds Kevin Everett's case: Why did he recover and why so fast? There are a number of possible explanations:
- Everett's recovery was simply a statistical improbability - he was an outlier and his recovery a chance occurrence.
- It was the result of sheer human determination and will in an athlete who simply would not accept his prognosis and would give everything to ensure he had the best chance to walk.
- It was the result of the sports medicine team's careful execution of the standard-of-care practice to prevent further injury immediately post-accident.
- Everett's recovery was the result of the precise execution of the neurosurgery team.
- The recovery was a result of the rehabilitation protocol implemented by a leading neurorehabilitation center.
- The rapid recovery was the result of cryotherapy, an experimental method that dramatically improved his prognosis.
The case of Kevin Everett highlights an important concept, that knowledge is a dynamic phenomenon (Amonette et al., 2010). The team of doctors, physical therapists, athletic trainers, and exercise specialists involved in the acute and postacute treatment of Everett's injury made numerous decisions that positively or negatively affected his outcome. The athletic trainers and sports medicine staff identified a possible injury to the spine and ensured that the athlete was quickly transported to the hospital. A careful procedure was used to move him to avoid further injury. The physicians made a decision to use the hypothermic technique to reduce spinal swelling. The neurosurgeon decided to perform surgery, and at some point, a physician determined that it was safe to remove Everett from the ventilator. In the rehabilitative process, physical therapists along with the medical team decided which therapeutic interventions were best suited to the stage of injury and made daily decisions on when to increase, decrease, or hold parameters like the intensity, volume, and duration of the rehabilitation program.
How did the sports medicine team determine the appropriate treatment?
Learn more about Evidence-Based Practice in Exercise Science.
Steps to Reading Research Critically
Reading and interpreting research may be one of the most important tasks of an evidence-based practitioner. It is important to develop the skills necessary to identify the key findings and to disregard the superfluous information.
Reading and interpreting research may be one of the most important tasks of an evidence-based practitioner. It is important to develop the skills necessary to identify the key findings and to disregard the superfluous information. Although critical appraisal is a topic left to a later chapter, next we present some practical guidelines for reading research evidence.
1-2. Read the Title and Abstract
The title of a research article can provide an important clue to the most important findings in the manuscript. But you should never read only the title and abstract. Some journal titles explicitly state the major finding of the paper. In a 1989 publication in Archives of Neurology, an article titled "Focused Stroke Rehabilitation Programs Improve Outcome" appears on pages 700-701 (Reding & McDowell, 1989) (figure 5.7). From the title alone, without reading the paper or the abstract, the reader learns that the investigators determined that a stroke rehabilitation program was effective in improving clinical outcomes. However, the very next article in the same volume of Archives of Neurology is titled "Focused Stroke Rehabilitation Programs Do Not Improve Outcome" (Dobkin, 1989) (figure 5.7). Which article is correct?
Two studies with directly contradictory titles that appeared consecutively in 1989 in Archives of Neurology.
Reprinted from PubMed.gov.
When the evidence-based practitioner relies on the title or abstract alone, he can make significant mistakes in the interpretation of research evidence. Also, examples such as the one just presented clearly show that research can be contradictory. The practitioner should read the title and abstract to determine whether the paper is relevant to the evidence-based question. If it is, he should proceed to a more careful reading and analysis to determine if the study methods and results support the findings stated in the abstract and title.
3. Read the Purpose, Construct, Theory, or Hypothesis Statement
After reading the title and abstract to determine the relevance of the study to the evidence-based question, the practitioner can skip to the final statement in the introduction that presents the study purpose, construct, theory, or hypothesis statement. This should provide the information needed to determine how the study should be designed to best answer the research question.
4. Read the Methods and Look for Flaws
The methods section is the most important part of a paper to read carefully and critically. It is from the methods section that an evidence-based practitioner can determine many of the potential biases and confounding factors associated with the study. This is also the section of the paper that determines the level or strength of evidence (chapter 8) provided by the research. As authors critically appraise their own research, they should carefully consider the study design, testing protocols, devices used, training and intervention protocols, statistical analyses, and study group allocations. If the authors are unclear in their presentation of any component of the methods, this should be a "red flag" to the reader and could potentially be a fatal flaw in the design.
Additional steps found inside Evidence-Based Practice in Exercise Science.
Translating Research Into Practice
As discussed earlier in this book, research design is a critical element to answering questions relevant to mechanistic, practical, and clinical science. One of the key aspects of research design is control of all potential confounding factors to eliminate the possibility that the outcomes arising from the intervention (independent variable) were influenced by an external factor.
As discussed earlier in this book, research design is a critical element to answering questions relevant to mechanistic, practical, and clinical science. One of the key aspects of research design is control of all potential confounding factors to eliminate the possibility that the outcomes arising from the intervention (independent variable) were influenced by an external factor. Although experimental control is a strength of research, and in particular of randomized control trials, it can also create problems when one is implementing research evidence in client, athlete, or patient populations. Suppose a clinical scientist is interested in studying the effect of interval exercise compared to steady-state exercise on hypercholesterolemia in adults who are obese. A logical study design to address such a question would be a randomized controlled trial. Consider the following hypothetical study:
One hundred participants who were obese were selected at random and then randomly assigned to one of four groups: interval exercise, short-duration steady-state exercise, long-duration steady-state exercise, and control with no exercise. In order to eliminate potential confounding factors, the participants were free from comorbidities including hypertension, insulin resistance, diabetes, overt cardiovascular disease, and recent orthopedic injuries. Before the intervention, all groups completed a treadmill
On the surface, this appears to be a sound single-blind randomized controlled trial. It is in fact well-designed and controlled, but there are some potential problems when a practitioner considers implementation. Because the scientists were interested in studying training responses to an intervention in obesity alone, they eliminated subjects with diabetes, hypertension, and other common comorbidities. This was a good decision for internal validity, but not for external validity; practitioners rarely treat individuals who are obese without any of these companion conditions (Castro, Kolka, Kim, & Bergman, 2014; Despres et al., 2008). Thus, practitioners are left to wonder whether the evidence is truly applicable to their patients or clients.
A second possible problem with the evidence is the elimination of secondary interventions. Strengths of a scientific experiment may actually be perceived as weaknesses with regard to practical implementation. In practice, multiple interventions are often implemented in concert with one another. This hypothetical experiment evaluated the effectiveness of interval versus steady-state treadmill exercise alone. An exercise practitioner is unlikely to implement the interval training protocol in isolation; instead, the protocol may be combined with resistance training, a healthy diet, and other behavioral modifications. Implementation of such multifaceted protocols may enhance the effectiveness of either of the interventions. Conversely, the addition of such interventions may also reduce the effectiveness of the protocol. Obviously, it is not scientifically plausible that resistance exercise would cause an increase in cholesterol or biologically negate the effects of the interval training protocol. However, it is possible that implementation of the secondary intervention will lead to overtraining, injury, soreness, and perhaps poor adherence to the protocol due to each of these secondary results of the combined protocol. Again, this is not likely, but it is certainly something the practitioner must consider.
Another potential problem with the implementation of scientific evidence is the possibility that a client may not be able to tolerate the protocol. For example, the initial fitness level of the client may not be sufficient to enable him to tolerate its rigors. The practitioner is then left to decide whether a modified version of the research protocol will be effective in improving blood cholesterol profiles. It is also possible that the protocol used in the scientific experiment will result in undertraining in some individuals; that is, in contrast to the previous scenario, the intensity of the stimulus may be insufficient to induce a training response. The exercise practitioner must then decide how to effectively alter the training loads in order to induce a similar response in a client or patient with a greater initial fitness level. In situations like these, it is often helpful to consult the discussion section of the research paper. Often the authors discuss in great detail the programmatic elements that they believe are responsible for the particular adaptations they observed; for instance, they may note that their subjects completed 10 intervals (with positive outcomes) in contrast to a previous study in the same population that used four intervals with negative findings. Mechanistic evidence, from either the same study or another, would further elucidate the cause(s) for the positive adaptations from a higher volume of exercise.
In medicine, one of the often cited criticisms of the evidence-based philosophy is that it leads to a cookbook approach to practice (Sackett, Rosenberg, Gray, Haynes, & Richardson, 1996). Opponents assert that evidence-based practitioners read scientific papers and then implement the protocols directly from the papers. The example we have presented illustrates that there really is no "recipe" for prescription; that is not the purpose of science. Because people are different, protocols may need to be altered to fit individual patient or client needs. Science influences the "ingredients" of the prescription. This hypothetical experiment demonstrates that interval exercise might be more effective than steady-state treadmill exercise in improving blood cholesterol of patients who are obese. It also provides some basic parameters for intensity, volume, mode, and so on for the implementation of a protocol. Practitioners must then decide whether to implement the protocol. They must also decide how they should implement interval exercise in a manner that is best suited to their client's, patient's, or athlete's individual needs and experience level.
Learn more about Evidence-Based Practice in Exercise Science.
Case Study 2: Vibration and Muscle Strength and Power
Charity is a university strength and conditioning coach. Recently, a professor in the school’s exercise physiology program acquired several vibration plates for a planned research study. The vibration plates are housed in the athletic training facility and are available to the athletes.
Charity is a university strength and conditioning coach. Recently, a professor in the school's exercise physiology program acquired several vibration plates for a planned research study. The vibration plates are housed in the athletic training facility and are available to the athletes. Charity heard about training with vibration plates at a national conference she attended recently; the presenter described a variety of upper and lower body exercises that could be performed on the plate and anecdotally claimed that such training results in noticeable performance improvements in athletes participating in a variety of sports. As an evidence-based practitioner, Charity realizes that although the vibration plate presentation was compelling, she needs to search the literature to determine what kind of scientific support exists for using vibration plate training as a modality to improve physiological and athletic performance.
Background
Vibration is thought to enhance acute neuromuscular performance via the stimulation of Ia afferent nerves, which effects a myotatic reflex contraction (Abercromby et al., 2007). Acutely, vibration improves maximal force and power output during concentric contractions; this facilitative effect is greater in elite athletes than in amateurs (Issurin & Tenenbaum, 1999; Liebermann & Issurin, 1997). However, vibration is ineffective when applied acutely to promote recovery or improve subsequent running performance after a strenuous exercise bout in highly fit runners (Edge, Mundel, Weir, & Cochrane, 2009). In competitive athletes, routine vibration training can increase strength, jump performance, and flexibility (Fagnani, Giombini, Di Cesare, Pigozzi, & Di Salvo, 2006), as well as improve proprioception and balance after anterior cruciate ligament reconstruction in comparison to a conventional rehabilitation program (Moezy, Olyaei, Hadian, Razi, & Faghihzadeh, 2008).
Charity currently employs evidence-based strength and conditioning programs with her athletes; these programs consist largely of resistance exercise - both traditional strength and explosive Olympic weightlifting exercises. Thus, to make a valid comparison in her athletic population, Charity should compare the effectiveness of vibration training to that of traditional resistance exercise. Given the limitations of vibration training (cost, availability, spatial restrictions), only if vibration training (either alone or in combination with traditional training) proves superior to traditional training would it be prudent to incorporate it on a large scale. Thus the evidence-based question is as follows.
In trained athletes, does vibration training, either alone or as an adjunct to resistance exercise, elicit improvements in muscle strength or power that are superior to those realized with traditional resistance training?
Search Strategy
Typing "vibration" into PubMed yields a list of MeSH subheadings; we select "vibration training." This returns 1141 studies. Activating the Age filter (Adult: 19-44 years) and Language filter (English) reduces this number to 377. Next, we add "AND athletes" to the search string ("vibration training AND athletes"), which returns 20 articles. Scanning these abstracts reveals 3 papers directly related to the chronic effects of vibration training (Delecluse et al., 2005; Issurin, Liebermann, & Tenenbaum, 1994; Preatoni et al., 2012). Of the 17 articles not included, most are acute studies and several others examine the effects of vibration on postworkout recovery and postsurgical rehabilitation outcomes; another study was excluded because it is not clear what exercise the control group performed.
Discussion of Results
The three articles reviewed are summarized in table 15.2. Preatoni and colleagues (2012) evaluated the effects of vibration training alone and in combination with traditional resistance training in 18 national-level female athletes (12 soccer and 6 softball athletes, with equal proportions in all groups). Subjects were randomized to one of three groups: (1) whole-body vibration training group, (2) traditional strength training group, and (3) combined whole-body vibration and strength training group. All training was performed during the winter preparatory period and in combination with other sport-specific field training such as speed drills, aerobic work, and technical and tactical skill practice. The periodized resistance training program was performed 2 days per week for 8 weeks; for the first week it consisted of six sets × six repetitions of squats performed at body weight with vibration (vibration group), at 60% 1RM (strength training group), or 30% 1RM with vibration (combined whole-body vibration and strength training group). Every 2 weeks, the external load was increased 6% (for the strength training group) and 3% (for the combined whole-body vibration and strength training group); greater intensity for the vibration group was achieved by increasing vibration frequency 5 Hz every 2 weeks (frequency was also increased for the combined group). Outcome measures included isometric strength (leg press); dynamic force, velocity, and power (explosive leg press with loads of 100% to 200% body weight in 20% increments); and power and power endurance (vertical jump and continuous 15-s vertical jumps, respectively). Training increased isometric strength (main effect, P = 0.02) with no differences between groups. No changes were observed for any parameter of the explosive leg press test. Performance on both vertical jump tests increased with training (main effect, P < 0.002), but there were no differences between groups. Maximum jump height (vertical jump test) and mean jump height and power (continuous 15-s vertical jump test) were increased only in the strength-trained group. The investigators also evaluated the characteristics of the vibration device (i.e., frequency, amplitude, and acceleration) and found variations up to 20% from the selected value; this was particularly true at higher frequencies. On the basis of other published data (Blottner et al., 2006; Mulder et al., 2008, 2007; Rittweger et al., 2006), the authors conclude that vibration exercise can elicit similar or improved outcomes compared to traditional strength training only when similar external loads are used; that is, they attribute the lack of an effect in their study to the lower external loads lifted by the combined vibration + strength training group (Preatoni et al., 2012).
Delecluse and colleagues (2005) examined the additive effect of a whole-body vibration training program over 5 weeks in 20 sprinters. Male and female sprinters (mean 100 m times: female = 12.46 ± 0.59 s, male = 11.45 ± 0.42 s) were randomly assigned to either a vibration or a control group. Both groups maintained their conventional training program, which consisted of intervals (10-60 s), speed training (two or three sessions per week with efforts near race pace), speed drills (two sessions per week), plyometric drills (one session per week), and explosive resistance training (three sessions per week) at 75% to 95% 1RM (three to five sets × two to five repetitions). In addition to their typical training, the vibration group completed three sessions per week of unloaded static and dynamic leg exercise on a vibration platform. The exercises employed were high squat, deep squat, wide stance squat, single-leg squat, lunge, and heel raise. The vibration program was implemented progressively through increases in the duration of vibration time and concomitant decreases in the rest periods; vibration amplitude (displacement) and frequency were also increased over the 5-week program. The study was conducted during the precompetitive phase of training. Outcome measures included strength (isometric and isokinetic knee extensor-flexor), maximal knee extension velocity (at 1%, 20%, 40%, and 60% of maximum isometric force), vertical jump, starting parameters (start time, horizontal start velocity, and horizontal start acceleration), and maximum velocity in a 30 m sprint. There were no changes in either group after the 5-week training program, nor were there any interaction effects or differences between groups posttraining.
Issurin, Liebermann, and Tenenbaum (1994) examined the effects of vibration training in 28 young male athletes who regularly participated in a wide cross section of club or varsity sports such as judo, swimming, volleyball, tennis, soccer, track and field, and cycling. Subjects were randomized to one of three groups: (1) upper body strength training with vibration and lower body flexibility training, (2) upper body strength training and lower body flexibility training with vibration, and (3) a calisthenics - basketball game control. The training program, which was conducted three times per week for 3 weeks, consisted of a ~10-min warm-up, a single upper body strength exercise (seated bench pull: six sets × six repetitions at 80% to 100% 1RM performed to failure), and ~20 min of specific static and ballistic stretching of the upper leg musculature. The program was performed by both experimental groups; vibration was added to either the upper or lower body activity according to group assignment. Outcome measures included strength (bench pull 1RM) and flexibility (two-leg split distance and sit and reach distance). Collectively, 1RM strength and both flexibility measures increased with training (main effects); there were also differences between groups for each outcome (group × time interaction effect). Unfortunately, the authors did not provide statistical contrasts between groups (e.g., strength training vs. strength training with vibration) to elucidate the between-group differences; because of the influence of the control group (which changed very little for any measure) on both main and interaction effects, it is difficult to interpret the study findings.
Luo, NcNamara, and Moran (2005) published a review evaluating the effects of vibration training on muscle strength and power, examining the effects of both chronic and acute vibration training. In 2005, only three papers had been published on the chronic adaptations to vibration training; of these, only one study employed trained athletes as subjects and has already been discussed (Issurin et al., 1994).
Conclusion and Strength of Evidence
There has been an explosion of literature regarding whole-body vibration in recent years. Some studies have been well conducted; others are poorly designed or uncontrolled, leading to erroneous or equivocal conclusions. There is still minimal understanding of the appropriate frequency, amplitude, direction, and length and mode of exercise needed for positive adaptations to vibration training. Despite the widespread use of vibration in athletic and private training settings, the evidence at the current time does not suggest that it is a strong tool to improve strength in athletically trained populations, although there is evidence for use in other populations.
There is level B evidence to refute the use of vibration training as a stand-alone or adjunct training method to increase muscle strength or power in athletes, as it is not demonstrably superior to traditional resistance exercise.
Program Recommendations
Although evidence supports vibration as a tool to improve strength and power in untrained populations, the data do not support its use to improve performance in athletes versus traditional strength methods. There is some evidence to support its use as a tool to acutely potentiate a power response; thus if Charity chooses to implement vibration, based on the literature it should be used as a postexcitatory potentiation tool. In general, Charity should continue training her athletes using traditional strength and conditioning programs but continue to watch the literature for emergent studies and protocols.
Save
Learn more about Evidence-Based Practice in Exercise Science.
Evidence-Based Practice in Action
On September 9, 2007, the second week of the 2007-2008 National Football League (NFL) season, the Buffalo Bills were at home for a game with the Denver Broncos. On a routine kickoff, third-year tight end Kevin Everett sprinted down the field and approached the kick returner, Domenik Hixon (Carchidi, 2008).
On September 9, 2007, the second week of the 2007-2008 National Football League (NFL) season, the Buffalo Bills were at home for a game with the Denver Broncos. On a routine kickoff, third-year tight end Kevin Everett sprinted down the field and approached the kick returner, Domenik Hixon (Carchidi, 2008). Everett dropped his center of gravity and extended into Hixon for the tackle - a motor skill that he had presumably performed thousands of times previously. Everett led with the crown of his helmet, contacting the helmet of Hixon at a high velocity, inadvertently violating a common but too often disregarded fundamental of tackling. The consequences of the collision were devastating and nearly fatal for Everett.
Immediately upon impact, Everett fell to the ground and lay face down, motionless. The collision resulted in a fracture dislocation of his third and fourth cervical vertebrae, injuring the spinal cord and instantly paralyzing Everett (Cappuccino et al., 2010; Carchidi, 2008). The sports medicine staff reacted quickly to the injury, clearing the scene to ensure that Everett was not injured further. With an injury such as Everett's, the standard-of-care protocol provides that the helmet remain on, the player be placed on a board, the face mask removed, and the player carefully moved to a stretcher and then transported by ambulance directly to the hospital. The sports medicine staff appeared to perfectly execute the protocol, and Everett was carefully transported to Millard Fillmore Gates Hospital (Carchidi, 2008).
In the ambulance ride en route to the hospital, the neurosurgery team used an experimental therapy that they hoped would improve Everett's prognosis. Infusing a cold saline solution into Everett's veins, the medical team induced a mild hypothermic state (Cappuccino et al., 2010). The use of ice to treat an injury is not novel - ice is used acutely for virtually every orthopedic injury. The principle of inducing systemic hypothermia is similar. The cold saline solution acutely controls systemic inflammation, and the medical team apparently believed that the therapy would reduce inflammation surrounding the spinal cord injury, preventing further damage (Cappuccino et al., 2010; Mummaneni, 2010). After evaluation by the medical staff, the neurosurgeon performed an emergency surgery in an attempt to save Everett's life (Cappuccino et al., 2010). After the surgery, Everett was placed on a respirator; it was believed that if he lived, he was unlikely to ever walk again (Carchidi, 2008).
Two days after the injury, Everett was removed from the respirator; he was reported to have minimal voluntary movements in his lower extremities, suggesting a theoretical possibility that he could regain the ability to walk (Cappuccino et al., 2010). On the basis on previous cases, the medical team believed that Everett had a small chance of regaining full control of his extremities (Carchidi, 2008). In the weeks and months that followed, Everett made remarkable progress, recovering at a rate far greater than expected. He was transferred to a top rehabilitation center for neurologic injuries in Houston, Texas, that implemented a comprehensive rehabilitation program. On December 23, 2007, Kevin Everett walked onto the field of Ralph Wilson Stadium - a remarkable feat that a few short months earlier had seemed impossible.
Kevin Everett's recovery was remarkable and a testament to the professional competence and readiness of the integrated sports medicine team, who made numerous decisions improving the chances that he might walk. Everett's story is also a demonstration of personal determination and perseverance that has inspired hope. For patients suffering severe spinal cord injuries, the story validates that dramatic recovery is possible. Medical personnel are encouraged in that Everett's case shows that diligent medical and rehabilitative therapy facilitates recovery. However, there is one overriding question that surrounds Kevin Everett's case: Why did he recover and why so fast? There are a number of possible explanations:
- Everett's recovery was simply a statistical improbability - he was an outlier and his recovery a chance occurrence.
- It was the result of sheer human determination and will in an athlete who simply would not accept his prognosis and would give everything to ensure he had the best chance to walk.
- It was the result of the sports medicine team's careful execution of the standard-of-care practice to prevent further injury immediately post-accident.
- Everett's recovery was the result of the precise execution of the neurosurgery team.
- The recovery was a result of the rehabilitation protocol implemented by a leading neurorehabilitation center.
- The rapid recovery was the result of cryotherapy, an experimental method that dramatically improved his prognosis.
The case of Kevin Everett highlights an important concept, that knowledge is a dynamic phenomenon (Amonette et al., 2010). The team of doctors, physical therapists, athletic trainers, and exercise specialists involved in the acute and postacute treatment of Everett's injury made numerous decisions that positively or negatively affected his outcome. The athletic trainers and sports medicine staff identified a possible injury to the spine and ensured that the athlete was quickly transported to the hospital. A careful procedure was used to move him to avoid further injury. The physicians made a decision to use the hypothermic technique to reduce spinal swelling. The neurosurgeon decided to perform surgery, and at some point, a physician determined that it was safe to remove Everett from the ventilator. In the rehabilitative process, physical therapists along with the medical team decided which therapeutic interventions were best suited to the stage of injury and made daily decisions on when to increase, decrease, or hold parameters like the intensity, volume, and duration of the rehabilitation program.
How did the sports medicine team determine the appropriate treatment?
Learn more about Evidence-Based Practice in Exercise Science.
Steps to Reading Research Critically
Reading and interpreting research may be one of the most important tasks of an evidence-based practitioner. It is important to develop the skills necessary to identify the key findings and to disregard the superfluous information.
Reading and interpreting research may be one of the most important tasks of an evidence-based practitioner. It is important to develop the skills necessary to identify the key findings and to disregard the superfluous information. Although critical appraisal is a topic left to a later chapter, next we present some practical guidelines for reading research evidence.
1-2. Read the Title and Abstract
The title of a research article can provide an important clue to the most important findings in the manuscript. But you should never read only the title and abstract. Some journal titles explicitly state the major finding of the paper. In a 1989 publication in Archives of Neurology, an article titled "Focused Stroke Rehabilitation Programs Improve Outcome" appears on pages 700-701 (Reding & McDowell, 1989) (figure 5.7). From the title alone, without reading the paper or the abstract, the reader learns that the investigators determined that a stroke rehabilitation program was effective in improving clinical outcomes. However, the very next article in the same volume of Archives of Neurology is titled "Focused Stroke Rehabilitation Programs Do Not Improve Outcome" (Dobkin, 1989) (figure 5.7). Which article is correct?
Two studies with directly contradictory titles that appeared consecutively in 1989 in Archives of Neurology.
Reprinted from PubMed.gov.
When the evidence-based practitioner relies on the title or abstract alone, he can make significant mistakes in the interpretation of research evidence. Also, examples such as the one just presented clearly show that research can be contradictory. The practitioner should read the title and abstract to determine whether the paper is relevant to the evidence-based question. If it is, he should proceed to a more careful reading and analysis to determine if the study methods and results support the findings stated in the abstract and title.
3. Read the Purpose, Construct, Theory, or Hypothesis Statement
After reading the title and abstract to determine the relevance of the study to the evidence-based question, the practitioner can skip to the final statement in the introduction that presents the study purpose, construct, theory, or hypothesis statement. This should provide the information needed to determine how the study should be designed to best answer the research question.
4. Read the Methods and Look for Flaws
The methods section is the most important part of a paper to read carefully and critically. It is from the methods section that an evidence-based practitioner can determine many of the potential biases and confounding factors associated with the study. This is also the section of the paper that determines the level or strength of evidence (chapter 8) provided by the research. As authors critically appraise their own research, they should carefully consider the study design, testing protocols, devices used, training and intervention protocols, statistical analyses, and study group allocations. If the authors are unclear in their presentation of any component of the methods, this should be a "red flag" to the reader and could potentially be a fatal flaw in the design.
Additional steps found inside Evidence-Based Practice in Exercise Science.
Translating Research Into Practice
As discussed earlier in this book, research design is a critical element to answering questions relevant to mechanistic, practical, and clinical science. One of the key aspects of research design is control of all potential confounding factors to eliminate the possibility that the outcomes arising from the intervention (independent variable) were influenced by an external factor.
As discussed earlier in this book, research design is a critical element to answering questions relevant to mechanistic, practical, and clinical science. One of the key aspects of research design is control of all potential confounding factors to eliminate the possibility that the outcomes arising from the intervention (independent variable) were influenced by an external factor. Although experimental control is a strength of research, and in particular of randomized control trials, it can also create problems when one is implementing research evidence in client, athlete, or patient populations. Suppose a clinical scientist is interested in studying the effect of interval exercise compared to steady-state exercise on hypercholesterolemia in adults who are obese. A logical study design to address such a question would be a randomized controlled trial. Consider the following hypothetical study:
One hundred participants who were obese were selected at random and then randomly assigned to one of four groups: interval exercise, short-duration steady-state exercise, long-duration steady-state exercise, and control with no exercise. In order to eliminate potential confounding factors, the participants were free from comorbidities including hypertension, insulin resistance, diabetes, overt cardiovascular disease, and recent orthopedic injuries. Before the intervention, all groups completed a treadmill
On the surface, this appears to be a sound single-blind randomized controlled trial. It is in fact well-designed and controlled, but there are some potential problems when a practitioner considers implementation. Because the scientists were interested in studying training responses to an intervention in obesity alone, they eliminated subjects with diabetes, hypertension, and other common comorbidities. This was a good decision for internal validity, but not for external validity; practitioners rarely treat individuals who are obese without any of these companion conditions (Castro, Kolka, Kim, & Bergman, 2014; Despres et al., 2008). Thus, practitioners are left to wonder whether the evidence is truly applicable to their patients or clients.
A second possible problem with the evidence is the elimination of secondary interventions. Strengths of a scientific experiment may actually be perceived as weaknesses with regard to practical implementation. In practice, multiple interventions are often implemented in concert with one another. This hypothetical experiment evaluated the effectiveness of interval versus steady-state treadmill exercise alone. An exercise practitioner is unlikely to implement the interval training protocol in isolation; instead, the protocol may be combined with resistance training, a healthy diet, and other behavioral modifications. Implementation of such multifaceted protocols may enhance the effectiveness of either of the interventions. Conversely, the addition of such interventions may also reduce the effectiveness of the protocol. Obviously, it is not scientifically plausible that resistance exercise would cause an increase in cholesterol or biologically negate the effects of the interval training protocol. However, it is possible that implementation of the secondary intervention will lead to overtraining, injury, soreness, and perhaps poor adherence to the protocol due to each of these secondary results of the combined protocol. Again, this is not likely, but it is certainly something the practitioner must consider.
Another potential problem with the implementation of scientific evidence is the possibility that a client may not be able to tolerate the protocol. For example, the initial fitness level of the client may not be sufficient to enable him to tolerate its rigors. The practitioner is then left to decide whether a modified version of the research protocol will be effective in improving blood cholesterol profiles. It is also possible that the protocol used in the scientific experiment will result in undertraining in some individuals; that is, in contrast to the previous scenario, the intensity of the stimulus may be insufficient to induce a training response. The exercise practitioner must then decide how to effectively alter the training loads in order to induce a similar response in a client or patient with a greater initial fitness level. In situations like these, it is often helpful to consult the discussion section of the research paper. Often the authors discuss in great detail the programmatic elements that they believe are responsible for the particular adaptations they observed; for instance, they may note that their subjects completed 10 intervals (with positive outcomes) in contrast to a previous study in the same population that used four intervals with negative findings. Mechanistic evidence, from either the same study or another, would further elucidate the cause(s) for the positive adaptations from a higher volume of exercise.
In medicine, one of the often cited criticisms of the evidence-based philosophy is that it leads to a cookbook approach to practice (Sackett, Rosenberg, Gray, Haynes, & Richardson, 1996). Opponents assert that evidence-based practitioners read scientific papers and then implement the protocols directly from the papers. The example we have presented illustrates that there really is no "recipe" for prescription; that is not the purpose of science. Because people are different, protocols may need to be altered to fit individual patient or client needs. Science influences the "ingredients" of the prescription. This hypothetical experiment demonstrates that interval exercise might be more effective than steady-state treadmill exercise in improving blood cholesterol of patients who are obese. It also provides some basic parameters for intensity, volume, mode, and so on for the implementation of a protocol. Practitioners must then decide whether to implement the protocol. They must also decide how they should implement interval exercise in a manner that is best suited to their client's, patient's, or athlete's individual needs and experience level.
Learn more about Evidence-Based Practice in Exercise Science.
Case Study 2: Vibration and Muscle Strength and Power
Charity is a university strength and conditioning coach. Recently, a professor in the school’s exercise physiology program acquired several vibration plates for a planned research study. The vibration plates are housed in the athletic training facility and are available to the athletes.
Charity is a university strength and conditioning coach. Recently, a professor in the school's exercise physiology program acquired several vibration plates for a planned research study. The vibration plates are housed in the athletic training facility and are available to the athletes. Charity heard about training with vibration plates at a national conference she attended recently; the presenter described a variety of upper and lower body exercises that could be performed on the plate and anecdotally claimed that such training results in noticeable performance improvements in athletes participating in a variety of sports. As an evidence-based practitioner, Charity realizes that although the vibration plate presentation was compelling, she needs to search the literature to determine what kind of scientific support exists for using vibration plate training as a modality to improve physiological and athletic performance.
Background
Vibration is thought to enhance acute neuromuscular performance via the stimulation of Ia afferent nerves, which effects a myotatic reflex contraction (Abercromby et al., 2007). Acutely, vibration improves maximal force and power output during concentric contractions; this facilitative effect is greater in elite athletes than in amateurs (Issurin & Tenenbaum, 1999; Liebermann & Issurin, 1997). However, vibration is ineffective when applied acutely to promote recovery or improve subsequent running performance after a strenuous exercise bout in highly fit runners (Edge, Mundel, Weir, & Cochrane, 2009). In competitive athletes, routine vibration training can increase strength, jump performance, and flexibility (Fagnani, Giombini, Di Cesare, Pigozzi, & Di Salvo, 2006), as well as improve proprioception and balance after anterior cruciate ligament reconstruction in comparison to a conventional rehabilitation program (Moezy, Olyaei, Hadian, Razi, & Faghihzadeh, 2008).
Charity currently employs evidence-based strength and conditioning programs with her athletes; these programs consist largely of resistance exercise - both traditional strength and explosive Olympic weightlifting exercises. Thus, to make a valid comparison in her athletic population, Charity should compare the effectiveness of vibration training to that of traditional resistance exercise. Given the limitations of vibration training (cost, availability, spatial restrictions), only if vibration training (either alone or in combination with traditional training) proves superior to traditional training would it be prudent to incorporate it on a large scale. Thus the evidence-based question is as follows.
In trained athletes, does vibration training, either alone or as an adjunct to resistance exercise, elicit improvements in muscle strength or power that are superior to those realized with traditional resistance training?
Search Strategy
Typing "vibration" into PubMed yields a list of MeSH subheadings; we select "vibration training." This returns 1141 studies. Activating the Age filter (Adult: 19-44 years) and Language filter (English) reduces this number to 377. Next, we add "AND athletes" to the search string ("vibration training AND athletes"), which returns 20 articles. Scanning these abstracts reveals 3 papers directly related to the chronic effects of vibration training (Delecluse et al., 2005; Issurin, Liebermann, & Tenenbaum, 1994; Preatoni et al., 2012). Of the 17 articles not included, most are acute studies and several others examine the effects of vibration on postworkout recovery and postsurgical rehabilitation outcomes; another study was excluded because it is not clear what exercise the control group performed.
Discussion of Results
The three articles reviewed are summarized in table 15.2. Preatoni and colleagues (2012) evaluated the effects of vibration training alone and in combination with traditional resistance training in 18 national-level female athletes (12 soccer and 6 softball athletes, with equal proportions in all groups). Subjects were randomized to one of three groups: (1) whole-body vibration training group, (2) traditional strength training group, and (3) combined whole-body vibration and strength training group. All training was performed during the winter preparatory period and in combination with other sport-specific field training such as speed drills, aerobic work, and technical and tactical skill practice. The periodized resistance training program was performed 2 days per week for 8 weeks; for the first week it consisted of six sets × six repetitions of squats performed at body weight with vibration (vibration group), at 60% 1RM (strength training group), or 30% 1RM with vibration (combined whole-body vibration and strength training group). Every 2 weeks, the external load was increased 6% (for the strength training group) and 3% (for the combined whole-body vibration and strength training group); greater intensity for the vibration group was achieved by increasing vibration frequency 5 Hz every 2 weeks (frequency was also increased for the combined group). Outcome measures included isometric strength (leg press); dynamic force, velocity, and power (explosive leg press with loads of 100% to 200% body weight in 20% increments); and power and power endurance (vertical jump and continuous 15-s vertical jumps, respectively). Training increased isometric strength (main effect, P = 0.02) with no differences between groups. No changes were observed for any parameter of the explosive leg press test. Performance on both vertical jump tests increased with training (main effect, P < 0.002), but there were no differences between groups. Maximum jump height (vertical jump test) and mean jump height and power (continuous 15-s vertical jump test) were increased only in the strength-trained group. The investigators also evaluated the characteristics of the vibration device (i.e., frequency, amplitude, and acceleration) and found variations up to 20% from the selected value; this was particularly true at higher frequencies. On the basis of other published data (Blottner et al., 2006; Mulder et al., 2008, 2007; Rittweger et al., 2006), the authors conclude that vibration exercise can elicit similar or improved outcomes compared to traditional strength training only when similar external loads are used; that is, they attribute the lack of an effect in their study to the lower external loads lifted by the combined vibration + strength training group (Preatoni et al., 2012).
Delecluse and colleagues (2005) examined the additive effect of a whole-body vibration training program over 5 weeks in 20 sprinters. Male and female sprinters (mean 100 m times: female = 12.46 ± 0.59 s, male = 11.45 ± 0.42 s) were randomly assigned to either a vibration or a control group. Both groups maintained their conventional training program, which consisted of intervals (10-60 s), speed training (two or three sessions per week with efforts near race pace), speed drills (two sessions per week), plyometric drills (one session per week), and explosive resistance training (three sessions per week) at 75% to 95% 1RM (three to five sets × two to five repetitions). In addition to their typical training, the vibration group completed three sessions per week of unloaded static and dynamic leg exercise on a vibration platform. The exercises employed were high squat, deep squat, wide stance squat, single-leg squat, lunge, and heel raise. The vibration program was implemented progressively through increases in the duration of vibration time and concomitant decreases in the rest periods; vibration amplitude (displacement) and frequency were also increased over the 5-week program. The study was conducted during the precompetitive phase of training. Outcome measures included strength (isometric and isokinetic knee extensor-flexor), maximal knee extension velocity (at 1%, 20%, 40%, and 60% of maximum isometric force), vertical jump, starting parameters (start time, horizontal start velocity, and horizontal start acceleration), and maximum velocity in a 30 m sprint. There were no changes in either group after the 5-week training program, nor were there any interaction effects or differences between groups posttraining.
Issurin, Liebermann, and Tenenbaum (1994) examined the effects of vibration training in 28 young male athletes who regularly participated in a wide cross section of club or varsity sports such as judo, swimming, volleyball, tennis, soccer, track and field, and cycling. Subjects were randomized to one of three groups: (1) upper body strength training with vibration and lower body flexibility training, (2) upper body strength training and lower body flexibility training with vibration, and (3) a calisthenics - basketball game control. The training program, which was conducted three times per week for 3 weeks, consisted of a ~10-min warm-up, a single upper body strength exercise (seated bench pull: six sets × six repetitions at 80% to 100% 1RM performed to failure), and ~20 min of specific static and ballistic stretching of the upper leg musculature. The program was performed by both experimental groups; vibration was added to either the upper or lower body activity according to group assignment. Outcome measures included strength (bench pull 1RM) and flexibility (two-leg split distance and sit and reach distance). Collectively, 1RM strength and both flexibility measures increased with training (main effects); there were also differences between groups for each outcome (group × time interaction effect). Unfortunately, the authors did not provide statistical contrasts between groups (e.g., strength training vs. strength training with vibration) to elucidate the between-group differences; because of the influence of the control group (which changed very little for any measure) on both main and interaction effects, it is difficult to interpret the study findings.
Luo, NcNamara, and Moran (2005) published a review evaluating the effects of vibration training on muscle strength and power, examining the effects of both chronic and acute vibration training. In 2005, only three papers had been published on the chronic adaptations to vibration training; of these, only one study employed trained athletes as subjects and has already been discussed (Issurin et al., 1994).
Conclusion and Strength of Evidence
There has been an explosion of literature regarding whole-body vibration in recent years. Some studies have been well conducted; others are poorly designed or uncontrolled, leading to erroneous or equivocal conclusions. There is still minimal understanding of the appropriate frequency, amplitude, direction, and length and mode of exercise needed for positive adaptations to vibration training. Despite the widespread use of vibration in athletic and private training settings, the evidence at the current time does not suggest that it is a strong tool to improve strength in athletically trained populations, although there is evidence for use in other populations.
There is level B evidence to refute the use of vibration training as a stand-alone or adjunct training method to increase muscle strength or power in athletes, as it is not demonstrably superior to traditional resistance exercise.
Program Recommendations
Although evidence supports vibration as a tool to improve strength and power in untrained populations, the data do not support its use to improve performance in athletes versus traditional strength methods. There is some evidence to support its use as a tool to acutely potentiate a power response; thus if Charity chooses to implement vibration, based on the literature it should be used as a postexcitatory potentiation tool. In general, Charity should continue training her athletes using traditional strength and conditioning programs but continue to watch the literature for emergent studies and protocols.
Save
Learn more about Evidence-Based Practice in Exercise Science.
Evidence-Based Practice in Action
On September 9, 2007, the second week of the 2007-2008 National Football League (NFL) season, the Buffalo Bills were at home for a game with the Denver Broncos. On a routine kickoff, third-year tight end Kevin Everett sprinted down the field and approached the kick returner, Domenik Hixon (Carchidi, 2008).
On September 9, 2007, the second week of the 2007-2008 National Football League (NFL) season, the Buffalo Bills were at home for a game with the Denver Broncos. On a routine kickoff, third-year tight end Kevin Everett sprinted down the field and approached the kick returner, Domenik Hixon (Carchidi, 2008). Everett dropped his center of gravity and extended into Hixon for the tackle - a motor skill that he had presumably performed thousands of times previously. Everett led with the crown of his helmet, contacting the helmet of Hixon at a high velocity, inadvertently violating a common but too often disregarded fundamental of tackling. The consequences of the collision were devastating and nearly fatal for Everett.
Immediately upon impact, Everett fell to the ground and lay face down, motionless. The collision resulted in a fracture dislocation of his third and fourth cervical vertebrae, injuring the spinal cord and instantly paralyzing Everett (Cappuccino et al., 2010; Carchidi, 2008). The sports medicine staff reacted quickly to the injury, clearing the scene to ensure that Everett was not injured further. With an injury such as Everett's, the standard-of-care protocol provides that the helmet remain on, the player be placed on a board, the face mask removed, and the player carefully moved to a stretcher and then transported by ambulance directly to the hospital. The sports medicine staff appeared to perfectly execute the protocol, and Everett was carefully transported to Millard Fillmore Gates Hospital (Carchidi, 2008).
In the ambulance ride en route to the hospital, the neurosurgery team used an experimental therapy that they hoped would improve Everett's prognosis. Infusing a cold saline solution into Everett's veins, the medical team induced a mild hypothermic state (Cappuccino et al., 2010). The use of ice to treat an injury is not novel - ice is used acutely for virtually every orthopedic injury. The principle of inducing systemic hypothermia is similar. The cold saline solution acutely controls systemic inflammation, and the medical team apparently believed that the therapy would reduce inflammation surrounding the spinal cord injury, preventing further damage (Cappuccino et al., 2010; Mummaneni, 2010). After evaluation by the medical staff, the neurosurgeon performed an emergency surgery in an attempt to save Everett's life (Cappuccino et al., 2010). After the surgery, Everett was placed on a respirator; it was believed that if he lived, he was unlikely to ever walk again (Carchidi, 2008).
Two days after the injury, Everett was removed from the respirator; he was reported to have minimal voluntary movements in his lower extremities, suggesting a theoretical possibility that he could regain the ability to walk (Cappuccino et al., 2010). On the basis on previous cases, the medical team believed that Everett had a small chance of regaining full control of his extremities (Carchidi, 2008). In the weeks and months that followed, Everett made remarkable progress, recovering at a rate far greater than expected. He was transferred to a top rehabilitation center for neurologic injuries in Houston, Texas, that implemented a comprehensive rehabilitation program. On December 23, 2007, Kevin Everett walked onto the field of Ralph Wilson Stadium - a remarkable feat that a few short months earlier had seemed impossible.
Kevin Everett's recovery was remarkable and a testament to the professional competence and readiness of the integrated sports medicine team, who made numerous decisions improving the chances that he might walk. Everett's story is also a demonstration of personal determination and perseverance that has inspired hope. For patients suffering severe spinal cord injuries, the story validates that dramatic recovery is possible. Medical personnel are encouraged in that Everett's case shows that diligent medical and rehabilitative therapy facilitates recovery. However, there is one overriding question that surrounds Kevin Everett's case: Why did he recover and why so fast? There are a number of possible explanations:
- Everett's recovery was simply a statistical improbability - he was an outlier and his recovery a chance occurrence.
- It was the result of sheer human determination and will in an athlete who simply would not accept his prognosis and would give everything to ensure he had the best chance to walk.
- It was the result of the sports medicine team's careful execution of the standard-of-care practice to prevent further injury immediately post-accident.
- Everett's recovery was the result of the precise execution of the neurosurgery team.
- The recovery was a result of the rehabilitation protocol implemented by a leading neurorehabilitation center.
- The rapid recovery was the result of cryotherapy, an experimental method that dramatically improved his prognosis.
The case of Kevin Everett highlights an important concept, that knowledge is a dynamic phenomenon (Amonette et al., 2010). The team of doctors, physical therapists, athletic trainers, and exercise specialists involved in the acute and postacute treatment of Everett's injury made numerous decisions that positively or negatively affected his outcome. The athletic trainers and sports medicine staff identified a possible injury to the spine and ensured that the athlete was quickly transported to the hospital. A careful procedure was used to move him to avoid further injury. The physicians made a decision to use the hypothermic technique to reduce spinal swelling. The neurosurgeon decided to perform surgery, and at some point, a physician determined that it was safe to remove Everett from the ventilator. In the rehabilitative process, physical therapists along with the medical team decided which therapeutic interventions were best suited to the stage of injury and made daily decisions on when to increase, decrease, or hold parameters like the intensity, volume, and duration of the rehabilitation program.
How did the sports medicine team determine the appropriate treatment?
Learn more about Evidence-Based Practice in Exercise Science.
Steps to Reading Research Critically
Reading and interpreting research may be one of the most important tasks of an evidence-based practitioner. It is important to develop the skills necessary to identify the key findings and to disregard the superfluous information.
Reading and interpreting research may be one of the most important tasks of an evidence-based practitioner. It is important to develop the skills necessary to identify the key findings and to disregard the superfluous information. Although critical appraisal is a topic left to a later chapter, next we present some practical guidelines for reading research evidence.
1-2. Read the Title and Abstract
The title of a research article can provide an important clue to the most important findings in the manuscript. But you should never read only the title and abstract. Some journal titles explicitly state the major finding of the paper. In a 1989 publication in Archives of Neurology, an article titled "Focused Stroke Rehabilitation Programs Improve Outcome" appears on pages 700-701 (Reding & McDowell, 1989) (figure 5.7). From the title alone, without reading the paper or the abstract, the reader learns that the investigators determined that a stroke rehabilitation program was effective in improving clinical outcomes. However, the very next article in the same volume of Archives of Neurology is titled "Focused Stroke Rehabilitation Programs Do Not Improve Outcome" (Dobkin, 1989) (figure 5.7). Which article is correct?
Two studies with directly contradictory titles that appeared consecutively in 1989 in Archives of Neurology.
Reprinted from PubMed.gov.
When the evidence-based practitioner relies on the title or abstract alone, he can make significant mistakes in the interpretation of research evidence. Also, examples such as the one just presented clearly show that research can be contradictory. The practitioner should read the title and abstract to determine whether the paper is relevant to the evidence-based question. If it is, he should proceed to a more careful reading and analysis to determine if the study methods and results support the findings stated in the abstract and title.
3. Read the Purpose, Construct, Theory, or Hypothesis Statement
After reading the title and abstract to determine the relevance of the study to the evidence-based question, the practitioner can skip to the final statement in the introduction that presents the study purpose, construct, theory, or hypothesis statement. This should provide the information needed to determine how the study should be designed to best answer the research question.
4. Read the Methods and Look for Flaws
The methods section is the most important part of a paper to read carefully and critically. It is from the methods section that an evidence-based practitioner can determine many of the potential biases and confounding factors associated with the study. This is also the section of the paper that determines the level or strength of evidence (chapter 8) provided by the research. As authors critically appraise their own research, they should carefully consider the study design, testing protocols, devices used, training and intervention protocols, statistical analyses, and study group allocations. If the authors are unclear in their presentation of any component of the methods, this should be a "red flag" to the reader and could potentially be a fatal flaw in the design.
Additional steps found inside Evidence-Based Practice in Exercise Science.
Translating Research Into Practice
As discussed earlier in this book, research design is a critical element to answering questions relevant to mechanistic, practical, and clinical science. One of the key aspects of research design is control of all potential confounding factors to eliminate the possibility that the outcomes arising from the intervention (independent variable) were influenced by an external factor.
As discussed earlier in this book, research design is a critical element to answering questions relevant to mechanistic, practical, and clinical science. One of the key aspects of research design is control of all potential confounding factors to eliminate the possibility that the outcomes arising from the intervention (independent variable) were influenced by an external factor. Although experimental control is a strength of research, and in particular of randomized control trials, it can also create problems when one is implementing research evidence in client, athlete, or patient populations. Suppose a clinical scientist is interested in studying the effect of interval exercise compared to steady-state exercise on hypercholesterolemia in adults who are obese. A logical study design to address such a question would be a randomized controlled trial. Consider the following hypothetical study:
One hundred participants who were obese were selected at random and then randomly assigned to one of four groups: interval exercise, short-duration steady-state exercise, long-duration steady-state exercise, and control with no exercise. In order to eliminate potential confounding factors, the participants were free from comorbidities including hypertension, insulin resistance, diabetes, overt cardiovascular disease, and recent orthopedic injuries. Before the intervention, all groups completed a treadmill
On the surface, this appears to be a sound single-blind randomized controlled trial. It is in fact well-designed and controlled, but there are some potential problems when a practitioner considers implementation. Because the scientists were interested in studying training responses to an intervention in obesity alone, they eliminated subjects with diabetes, hypertension, and other common comorbidities. This was a good decision for internal validity, but not for external validity; practitioners rarely treat individuals who are obese without any of these companion conditions (Castro, Kolka, Kim, & Bergman, 2014; Despres et al., 2008). Thus, practitioners are left to wonder whether the evidence is truly applicable to their patients or clients.
A second possible problem with the evidence is the elimination of secondary interventions. Strengths of a scientific experiment may actually be perceived as weaknesses with regard to practical implementation. In practice, multiple interventions are often implemented in concert with one another. This hypothetical experiment evaluated the effectiveness of interval versus steady-state treadmill exercise alone. An exercise practitioner is unlikely to implement the interval training protocol in isolation; instead, the protocol may be combined with resistance training, a healthy diet, and other behavioral modifications. Implementation of such multifaceted protocols may enhance the effectiveness of either of the interventions. Conversely, the addition of such interventions may also reduce the effectiveness of the protocol. Obviously, it is not scientifically plausible that resistance exercise would cause an increase in cholesterol or biologically negate the effects of the interval training protocol. However, it is possible that implementation of the secondary intervention will lead to overtraining, injury, soreness, and perhaps poor adherence to the protocol due to each of these secondary results of the combined protocol. Again, this is not likely, but it is certainly something the practitioner must consider.
Another potential problem with the implementation of scientific evidence is the possibility that a client may not be able to tolerate the protocol. For example, the initial fitness level of the client may not be sufficient to enable him to tolerate its rigors. The practitioner is then left to decide whether a modified version of the research protocol will be effective in improving blood cholesterol profiles. It is also possible that the protocol used in the scientific experiment will result in undertraining in some individuals; that is, in contrast to the previous scenario, the intensity of the stimulus may be insufficient to induce a training response. The exercise practitioner must then decide how to effectively alter the training loads in order to induce a similar response in a client or patient with a greater initial fitness level. In situations like these, it is often helpful to consult the discussion section of the research paper. Often the authors discuss in great detail the programmatic elements that they believe are responsible for the particular adaptations they observed; for instance, they may note that their subjects completed 10 intervals (with positive outcomes) in contrast to a previous study in the same population that used four intervals with negative findings. Mechanistic evidence, from either the same study or another, would further elucidate the cause(s) for the positive adaptations from a higher volume of exercise.
In medicine, one of the often cited criticisms of the evidence-based philosophy is that it leads to a cookbook approach to practice (Sackett, Rosenberg, Gray, Haynes, & Richardson, 1996). Opponents assert that evidence-based practitioners read scientific papers and then implement the protocols directly from the papers. The example we have presented illustrates that there really is no "recipe" for prescription; that is not the purpose of science. Because people are different, protocols may need to be altered to fit individual patient or client needs. Science influences the "ingredients" of the prescription. This hypothetical experiment demonstrates that interval exercise might be more effective than steady-state treadmill exercise in improving blood cholesterol of patients who are obese. It also provides some basic parameters for intensity, volume, mode, and so on for the implementation of a protocol. Practitioners must then decide whether to implement the protocol. They must also decide how they should implement interval exercise in a manner that is best suited to their client's, patient's, or athlete's individual needs and experience level.
Learn more about Evidence-Based Practice in Exercise Science.
Case Study 2: Vibration and Muscle Strength and Power
Charity is a university strength and conditioning coach. Recently, a professor in the school’s exercise physiology program acquired several vibration plates for a planned research study. The vibration plates are housed in the athletic training facility and are available to the athletes.
Charity is a university strength and conditioning coach. Recently, a professor in the school's exercise physiology program acquired several vibration plates for a planned research study. The vibration plates are housed in the athletic training facility and are available to the athletes. Charity heard about training with vibration plates at a national conference she attended recently; the presenter described a variety of upper and lower body exercises that could be performed on the plate and anecdotally claimed that such training results in noticeable performance improvements in athletes participating in a variety of sports. As an evidence-based practitioner, Charity realizes that although the vibration plate presentation was compelling, she needs to search the literature to determine what kind of scientific support exists for using vibration plate training as a modality to improve physiological and athletic performance.
Background
Vibration is thought to enhance acute neuromuscular performance via the stimulation of Ia afferent nerves, which effects a myotatic reflex contraction (Abercromby et al., 2007). Acutely, vibration improves maximal force and power output during concentric contractions; this facilitative effect is greater in elite athletes than in amateurs (Issurin & Tenenbaum, 1999; Liebermann & Issurin, 1997). However, vibration is ineffective when applied acutely to promote recovery or improve subsequent running performance after a strenuous exercise bout in highly fit runners (Edge, Mundel, Weir, & Cochrane, 2009). In competitive athletes, routine vibration training can increase strength, jump performance, and flexibility (Fagnani, Giombini, Di Cesare, Pigozzi, & Di Salvo, 2006), as well as improve proprioception and balance after anterior cruciate ligament reconstruction in comparison to a conventional rehabilitation program (Moezy, Olyaei, Hadian, Razi, & Faghihzadeh, 2008).
Charity currently employs evidence-based strength and conditioning programs with her athletes; these programs consist largely of resistance exercise - both traditional strength and explosive Olympic weightlifting exercises. Thus, to make a valid comparison in her athletic population, Charity should compare the effectiveness of vibration training to that of traditional resistance exercise. Given the limitations of vibration training (cost, availability, spatial restrictions), only if vibration training (either alone or in combination with traditional training) proves superior to traditional training would it be prudent to incorporate it on a large scale. Thus the evidence-based question is as follows.
In trained athletes, does vibration training, either alone or as an adjunct to resistance exercise, elicit improvements in muscle strength or power that are superior to those realized with traditional resistance training?
Search Strategy
Typing "vibration" into PubMed yields a list of MeSH subheadings; we select "vibration training." This returns 1141 studies. Activating the Age filter (Adult: 19-44 years) and Language filter (English) reduces this number to 377. Next, we add "AND athletes" to the search string ("vibration training AND athletes"), which returns 20 articles. Scanning these abstracts reveals 3 papers directly related to the chronic effects of vibration training (Delecluse et al., 2005; Issurin, Liebermann, & Tenenbaum, 1994; Preatoni et al., 2012). Of the 17 articles not included, most are acute studies and several others examine the effects of vibration on postworkout recovery and postsurgical rehabilitation outcomes; another study was excluded because it is not clear what exercise the control group performed.
Discussion of Results
The three articles reviewed are summarized in table 15.2. Preatoni and colleagues (2012) evaluated the effects of vibration training alone and in combination with traditional resistance training in 18 national-level female athletes (12 soccer and 6 softball athletes, with equal proportions in all groups). Subjects were randomized to one of three groups: (1) whole-body vibration training group, (2) traditional strength training group, and (3) combined whole-body vibration and strength training group. All training was performed during the winter preparatory period and in combination with other sport-specific field training such as speed drills, aerobic work, and technical and tactical skill practice. The periodized resistance training program was performed 2 days per week for 8 weeks; for the first week it consisted of six sets × six repetitions of squats performed at body weight with vibration (vibration group), at 60% 1RM (strength training group), or 30% 1RM with vibration (combined whole-body vibration and strength training group). Every 2 weeks, the external load was increased 6% (for the strength training group) and 3% (for the combined whole-body vibration and strength training group); greater intensity for the vibration group was achieved by increasing vibration frequency 5 Hz every 2 weeks (frequency was also increased for the combined group). Outcome measures included isometric strength (leg press); dynamic force, velocity, and power (explosive leg press with loads of 100% to 200% body weight in 20% increments); and power and power endurance (vertical jump and continuous 15-s vertical jumps, respectively). Training increased isometric strength (main effect, P = 0.02) with no differences between groups. No changes were observed for any parameter of the explosive leg press test. Performance on both vertical jump tests increased with training (main effect, P < 0.002), but there were no differences between groups. Maximum jump height (vertical jump test) and mean jump height and power (continuous 15-s vertical jump test) were increased only in the strength-trained group. The investigators also evaluated the characteristics of the vibration device (i.e., frequency, amplitude, and acceleration) and found variations up to 20% from the selected value; this was particularly true at higher frequencies. On the basis of other published data (Blottner et al., 2006; Mulder et al., 2008, 2007; Rittweger et al., 2006), the authors conclude that vibration exercise can elicit similar or improved outcomes compared to traditional strength training only when similar external loads are used; that is, they attribute the lack of an effect in their study to the lower external loads lifted by the combined vibration + strength training group (Preatoni et al., 2012).
Delecluse and colleagues (2005) examined the additive effect of a whole-body vibration training program over 5 weeks in 20 sprinters. Male and female sprinters (mean 100 m times: female = 12.46 ± 0.59 s, male = 11.45 ± 0.42 s) were randomly assigned to either a vibration or a control group. Both groups maintained their conventional training program, which consisted of intervals (10-60 s), speed training (two or three sessions per week with efforts near race pace), speed drills (two sessions per week), plyometric drills (one session per week), and explosive resistance training (three sessions per week) at 75% to 95% 1RM (three to five sets × two to five repetitions). In addition to their typical training, the vibration group completed three sessions per week of unloaded static and dynamic leg exercise on a vibration platform. The exercises employed were high squat, deep squat, wide stance squat, single-leg squat, lunge, and heel raise. The vibration program was implemented progressively through increases in the duration of vibration time and concomitant decreases in the rest periods; vibration amplitude (displacement) and frequency were also increased over the 5-week program. The study was conducted during the precompetitive phase of training. Outcome measures included strength (isometric and isokinetic knee extensor-flexor), maximal knee extension velocity (at 1%, 20%, 40%, and 60% of maximum isometric force), vertical jump, starting parameters (start time, horizontal start velocity, and horizontal start acceleration), and maximum velocity in a 30 m sprint. There were no changes in either group after the 5-week training program, nor were there any interaction effects or differences between groups posttraining.
Issurin, Liebermann, and Tenenbaum (1994) examined the effects of vibration training in 28 young male athletes who regularly participated in a wide cross section of club or varsity sports such as judo, swimming, volleyball, tennis, soccer, track and field, and cycling. Subjects were randomized to one of three groups: (1) upper body strength training with vibration and lower body flexibility training, (2) upper body strength training and lower body flexibility training with vibration, and (3) a calisthenics - basketball game control. The training program, which was conducted three times per week for 3 weeks, consisted of a ~10-min warm-up, a single upper body strength exercise (seated bench pull: six sets × six repetitions at 80% to 100% 1RM performed to failure), and ~20 min of specific static and ballistic stretching of the upper leg musculature. The program was performed by both experimental groups; vibration was added to either the upper or lower body activity according to group assignment. Outcome measures included strength (bench pull 1RM) and flexibility (two-leg split distance and sit and reach distance). Collectively, 1RM strength and both flexibility measures increased with training (main effects); there were also differences between groups for each outcome (group × time interaction effect). Unfortunately, the authors did not provide statistical contrasts between groups (e.g., strength training vs. strength training with vibration) to elucidate the between-group differences; because of the influence of the control group (which changed very little for any measure) on both main and interaction effects, it is difficult to interpret the study findings.
Luo, NcNamara, and Moran (2005) published a review evaluating the effects of vibration training on muscle strength and power, examining the effects of both chronic and acute vibration training. In 2005, only three papers had been published on the chronic adaptations to vibration training; of these, only one study employed trained athletes as subjects and has already been discussed (Issurin et al., 1994).
Conclusion and Strength of Evidence
There has been an explosion of literature regarding whole-body vibration in recent years. Some studies have been well conducted; others are poorly designed or uncontrolled, leading to erroneous or equivocal conclusions. There is still minimal understanding of the appropriate frequency, amplitude, direction, and length and mode of exercise needed for positive adaptations to vibration training. Despite the widespread use of vibration in athletic and private training settings, the evidence at the current time does not suggest that it is a strong tool to improve strength in athletically trained populations, although there is evidence for use in other populations.
There is level B evidence to refute the use of vibration training as a stand-alone or adjunct training method to increase muscle strength or power in athletes, as it is not demonstrably superior to traditional resistance exercise.
Program Recommendations
Although evidence supports vibration as a tool to improve strength and power in untrained populations, the data do not support its use to improve performance in athletes versus traditional strength methods. There is some evidence to support its use as a tool to acutely potentiate a power response; thus if Charity chooses to implement vibration, based on the literature it should be used as a postexcitatory potentiation tool. In general, Charity should continue training her athletes using traditional strength and conditioning programs but continue to watch the literature for emergent studies and protocols.
Save
Learn more about Evidence-Based Practice in Exercise Science.
Evidence-Based Practice in Action
On September 9, 2007, the second week of the 2007-2008 National Football League (NFL) season, the Buffalo Bills were at home for a game with the Denver Broncos. On a routine kickoff, third-year tight end Kevin Everett sprinted down the field and approached the kick returner, Domenik Hixon (Carchidi, 2008).
On September 9, 2007, the second week of the 2007-2008 National Football League (NFL) season, the Buffalo Bills were at home for a game with the Denver Broncos. On a routine kickoff, third-year tight end Kevin Everett sprinted down the field and approached the kick returner, Domenik Hixon (Carchidi, 2008). Everett dropped his center of gravity and extended into Hixon for the tackle - a motor skill that he had presumably performed thousands of times previously. Everett led with the crown of his helmet, contacting the helmet of Hixon at a high velocity, inadvertently violating a common but too often disregarded fundamental of tackling. The consequences of the collision were devastating and nearly fatal for Everett.
Immediately upon impact, Everett fell to the ground and lay face down, motionless. The collision resulted in a fracture dislocation of his third and fourth cervical vertebrae, injuring the spinal cord and instantly paralyzing Everett (Cappuccino et al., 2010; Carchidi, 2008). The sports medicine staff reacted quickly to the injury, clearing the scene to ensure that Everett was not injured further. With an injury such as Everett's, the standard-of-care protocol provides that the helmet remain on, the player be placed on a board, the face mask removed, and the player carefully moved to a stretcher and then transported by ambulance directly to the hospital. The sports medicine staff appeared to perfectly execute the protocol, and Everett was carefully transported to Millard Fillmore Gates Hospital (Carchidi, 2008).
In the ambulance ride en route to the hospital, the neurosurgery team used an experimental therapy that they hoped would improve Everett's prognosis. Infusing a cold saline solution into Everett's veins, the medical team induced a mild hypothermic state (Cappuccino et al., 2010). The use of ice to treat an injury is not novel - ice is used acutely for virtually every orthopedic injury. The principle of inducing systemic hypothermia is similar. The cold saline solution acutely controls systemic inflammation, and the medical team apparently believed that the therapy would reduce inflammation surrounding the spinal cord injury, preventing further damage (Cappuccino et al., 2010; Mummaneni, 2010). After evaluation by the medical staff, the neurosurgeon performed an emergency surgery in an attempt to save Everett's life (Cappuccino et al., 2010). After the surgery, Everett was placed on a respirator; it was believed that if he lived, he was unlikely to ever walk again (Carchidi, 2008).
Two days after the injury, Everett was removed from the respirator; he was reported to have minimal voluntary movements in his lower extremities, suggesting a theoretical possibility that he could regain the ability to walk (Cappuccino et al., 2010). On the basis on previous cases, the medical team believed that Everett had a small chance of regaining full control of his extremities (Carchidi, 2008). In the weeks and months that followed, Everett made remarkable progress, recovering at a rate far greater than expected. He was transferred to a top rehabilitation center for neurologic injuries in Houston, Texas, that implemented a comprehensive rehabilitation program. On December 23, 2007, Kevin Everett walked onto the field of Ralph Wilson Stadium - a remarkable feat that a few short months earlier had seemed impossible.
Kevin Everett's recovery was remarkable and a testament to the professional competence and readiness of the integrated sports medicine team, who made numerous decisions improving the chances that he might walk. Everett's story is also a demonstration of personal determination and perseverance that has inspired hope. For patients suffering severe spinal cord injuries, the story validates that dramatic recovery is possible. Medical personnel are encouraged in that Everett's case shows that diligent medical and rehabilitative therapy facilitates recovery. However, there is one overriding question that surrounds Kevin Everett's case: Why did he recover and why so fast? There are a number of possible explanations:
- Everett's recovery was simply a statistical improbability - he was an outlier and his recovery a chance occurrence.
- It was the result of sheer human determination and will in an athlete who simply would not accept his prognosis and would give everything to ensure he had the best chance to walk.
- It was the result of the sports medicine team's careful execution of the standard-of-care practice to prevent further injury immediately post-accident.
- Everett's recovery was the result of the precise execution of the neurosurgery team.
- The recovery was a result of the rehabilitation protocol implemented by a leading neurorehabilitation center.
- The rapid recovery was the result of cryotherapy, an experimental method that dramatically improved his prognosis.
The case of Kevin Everett highlights an important concept, that knowledge is a dynamic phenomenon (Amonette et al., 2010). The team of doctors, physical therapists, athletic trainers, and exercise specialists involved in the acute and postacute treatment of Everett's injury made numerous decisions that positively or negatively affected his outcome. The athletic trainers and sports medicine staff identified a possible injury to the spine and ensured that the athlete was quickly transported to the hospital. A careful procedure was used to move him to avoid further injury. The physicians made a decision to use the hypothermic technique to reduce spinal swelling. The neurosurgeon decided to perform surgery, and at some point, a physician determined that it was safe to remove Everett from the ventilator. In the rehabilitative process, physical therapists along with the medical team decided which therapeutic interventions were best suited to the stage of injury and made daily decisions on when to increase, decrease, or hold parameters like the intensity, volume, and duration of the rehabilitation program.
How did the sports medicine team determine the appropriate treatment?
Learn more about Evidence-Based Practice in Exercise Science.
Steps to Reading Research Critically
Reading and interpreting research may be one of the most important tasks of an evidence-based practitioner. It is important to develop the skills necessary to identify the key findings and to disregard the superfluous information.
Reading and interpreting research may be one of the most important tasks of an evidence-based practitioner. It is important to develop the skills necessary to identify the key findings and to disregard the superfluous information. Although critical appraisal is a topic left to a later chapter, next we present some practical guidelines for reading research evidence.
1-2. Read the Title and Abstract
The title of a research article can provide an important clue to the most important findings in the manuscript. But you should never read only the title and abstract. Some journal titles explicitly state the major finding of the paper. In a 1989 publication in Archives of Neurology, an article titled "Focused Stroke Rehabilitation Programs Improve Outcome" appears on pages 700-701 (Reding & McDowell, 1989) (figure 5.7). From the title alone, without reading the paper or the abstract, the reader learns that the investigators determined that a stroke rehabilitation program was effective in improving clinical outcomes. However, the very next article in the same volume of Archives of Neurology is titled "Focused Stroke Rehabilitation Programs Do Not Improve Outcome" (Dobkin, 1989) (figure 5.7). Which article is correct?
Two studies with directly contradictory titles that appeared consecutively in 1989 in Archives of Neurology.
Reprinted from PubMed.gov.
When the evidence-based practitioner relies on the title or abstract alone, he can make significant mistakes in the interpretation of research evidence. Also, examples such as the one just presented clearly show that research can be contradictory. The practitioner should read the title and abstract to determine whether the paper is relevant to the evidence-based question. If it is, he should proceed to a more careful reading and analysis to determine if the study methods and results support the findings stated in the abstract and title.
3. Read the Purpose, Construct, Theory, or Hypothesis Statement
After reading the title and abstract to determine the relevance of the study to the evidence-based question, the practitioner can skip to the final statement in the introduction that presents the study purpose, construct, theory, or hypothesis statement. This should provide the information needed to determine how the study should be designed to best answer the research question.
4. Read the Methods and Look for Flaws
The methods section is the most important part of a paper to read carefully and critically. It is from the methods section that an evidence-based practitioner can determine many of the potential biases and confounding factors associated with the study. This is also the section of the paper that determines the level or strength of evidence (chapter 8) provided by the research. As authors critically appraise their own research, they should carefully consider the study design, testing protocols, devices used, training and intervention protocols, statistical analyses, and study group allocations. If the authors are unclear in their presentation of any component of the methods, this should be a "red flag" to the reader and could potentially be a fatal flaw in the design.
Additional steps found inside Evidence-Based Practice in Exercise Science.
Translating Research Into Practice
As discussed earlier in this book, research design is a critical element to answering questions relevant to mechanistic, practical, and clinical science. One of the key aspects of research design is control of all potential confounding factors to eliminate the possibility that the outcomes arising from the intervention (independent variable) were influenced by an external factor.
As discussed earlier in this book, research design is a critical element to answering questions relevant to mechanistic, practical, and clinical science. One of the key aspects of research design is control of all potential confounding factors to eliminate the possibility that the outcomes arising from the intervention (independent variable) were influenced by an external factor. Although experimental control is a strength of research, and in particular of randomized control trials, it can also create problems when one is implementing research evidence in client, athlete, or patient populations. Suppose a clinical scientist is interested in studying the effect of interval exercise compared to steady-state exercise on hypercholesterolemia in adults who are obese. A logical study design to address such a question would be a randomized controlled trial. Consider the following hypothetical study:
One hundred participants who were obese were selected at random and then randomly assigned to one of four groups: interval exercise, short-duration steady-state exercise, long-duration steady-state exercise, and control with no exercise. In order to eliminate potential confounding factors, the participants were free from comorbidities including hypertension, insulin resistance, diabetes, overt cardiovascular disease, and recent orthopedic injuries. Before the intervention, all groups completed a treadmill
On the surface, this appears to be a sound single-blind randomized controlled trial. It is in fact well-designed and controlled, but there are some potential problems when a practitioner considers implementation. Because the scientists were interested in studying training responses to an intervention in obesity alone, they eliminated subjects with diabetes, hypertension, and other common comorbidities. This was a good decision for internal validity, but not for external validity; practitioners rarely treat individuals who are obese without any of these companion conditions (Castro, Kolka, Kim, & Bergman, 2014; Despres et al., 2008). Thus, practitioners are left to wonder whether the evidence is truly applicable to their patients or clients.
A second possible problem with the evidence is the elimination of secondary interventions. Strengths of a scientific experiment may actually be perceived as weaknesses with regard to practical implementation. In practice, multiple interventions are often implemented in concert with one another. This hypothetical experiment evaluated the effectiveness of interval versus steady-state treadmill exercise alone. An exercise practitioner is unlikely to implement the interval training protocol in isolation; instead, the protocol may be combined with resistance training, a healthy diet, and other behavioral modifications. Implementation of such multifaceted protocols may enhance the effectiveness of either of the interventions. Conversely, the addition of such interventions may also reduce the effectiveness of the protocol. Obviously, it is not scientifically plausible that resistance exercise would cause an increase in cholesterol or biologically negate the effects of the interval training protocol. However, it is possible that implementation of the secondary intervention will lead to overtraining, injury, soreness, and perhaps poor adherence to the protocol due to each of these secondary results of the combined protocol. Again, this is not likely, but it is certainly something the practitioner must consider.
Another potential problem with the implementation of scientific evidence is the possibility that a client may not be able to tolerate the protocol. For example, the initial fitness level of the client may not be sufficient to enable him to tolerate its rigors. The practitioner is then left to decide whether a modified version of the research protocol will be effective in improving blood cholesterol profiles. It is also possible that the protocol used in the scientific experiment will result in undertraining in some individuals; that is, in contrast to the previous scenario, the intensity of the stimulus may be insufficient to induce a training response. The exercise practitioner must then decide how to effectively alter the training loads in order to induce a similar response in a client or patient with a greater initial fitness level. In situations like these, it is often helpful to consult the discussion section of the research paper. Often the authors discuss in great detail the programmatic elements that they believe are responsible for the particular adaptations they observed; for instance, they may note that their subjects completed 10 intervals (with positive outcomes) in contrast to a previous study in the same population that used four intervals with negative findings. Mechanistic evidence, from either the same study or another, would further elucidate the cause(s) for the positive adaptations from a higher volume of exercise.
In medicine, one of the often cited criticisms of the evidence-based philosophy is that it leads to a cookbook approach to practice (Sackett, Rosenberg, Gray, Haynes, & Richardson, 1996). Opponents assert that evidence-based practitioners read scientific papers and then implement the protocols directly from the papers. The example we have presented illustrates that there really is no "recipe" for prescription; that is not the purpose of science. Because people are different, protocols may need to be altered to fit individual patient or client needs. Science influences the "ingredients" of the prescription. This hypothetical experiment demonstrates that interval exercise might be more effective than steady-state treadmill exercise in improving blood cholesterol of patients who are obese. It also provides some basic parameters for intensity, volume, mode, and so on for the implementation of a protocol. Practitioners must then decide whether to implement the protocol. They must also decide how they should implement interval exercise in a manner that is best suited to their client's, patient's, or athlete's individual needs and experience level.
Learn more about Evidence-Based Practice in Exercise Science.
Case Study 2: Vibration and Muscle Strength and Power
Charity is a university strength and conditioning coach. Recently, a professor in the school’s exercise physiology program acquired several vibration plates for a planned research study. The vibration plates are housed in the athletic training facility and are available to the athletes.
Charity is a university strength and conditioning coach. Recently, a professor in the school's exercise physiology program acquired several vibration plates for a planned research study. The vibration plates are housed in the athletic training facility and are available to the athletes. Charity heard about training with vibration plates at a national conference she attended recently; the presenter described a variety of upper and lower body exercises that could be performed on the plate and anecdotally claimed that such training results in noticeable performance improvements in athletes participating in a variety of sports. As an evidence-based practitioner, Charity realizes that although the vibration plate presentation was compelling, she needs to search the literature to determine what kind of scientific support exists for using vibration plate training as a modality to improve physiological and athletic performance.
Background
Vibration is thought to enhance acute neuromuscular performance via the stimulation of Ia afferent nerves, which effects a myotatic reflex contraction (Abercromby et al., 2007). Acutely, vibration improves maximal force and power output during concentric contractions; this facilitative effect is greater in elite athletes than in amateurs (Issurin & Tenenbaum, 1999; Liebermann & Issurin, 1997). However, vibration is ineffective when applied acutely to promote recovery or improve subsequent running performance after a strenuous exercise bout in highly fit runners (Edge, Mundel, Weir, & Cochrane, 2009). In competitive athletes, routine vibration training can increase strength, jump performance, and flexibility (Fagnani, Giombini, Di Cesare, Pigozzi, & Di Salvo, 2006), as well as improve proprioception and balance after anterior cruciate ligament reconstruction in comparison to a conventional rehabilitation program (Moezy, Olyaei, Hadian, Razi, & Faghihzadeh, 2008).
Charity currently employs evidence-based strength and conditioning programs with her athletes; these programs consist largely of resistance exercise - both traditional strength and explosive Olympic weightlifting exercises. Thus, to make a valid comparison in her athletic population, Charity should compare the effectiveness of vibration training to that of traditional resistance exercise. Given the limitations of vibration training (cost, availability, spatial restrictions), only if vibration training (either alone or in combination with traditional training) proves superior to traditional training would it be prudent to incorporate it on a large scale. Thus the evidence-based question is as follows.
In trained athletes, does vibration training, either alone or as an adjunct to resistance exercise, elicit improvements in muscle strength or power that are superior to those realized with traditional resistance training?
Search Strategy
Typing "vibration" into PubMed yields a list of MeSH subheadings; we select "vibration training." This returns 1141 studies. Activating the Age filter (Adult: 19-44 years) and Language filter (English) reduces this number to 377. Next, we add "AND athletes" to the search string ("vibration training AND athletes"), which returns 20 articles. Scanning these abstracts reveals 3 papers directly related to the chronic effects of vibration training (Delecluse et al., 2005; Issurin, Liebermann, & Tenenbaum, 1994; Preatoni et al., 2012). Of the 17 articles not included, most are acute studies and several others examine the effects of vibration on postworkout recovery and postsurgical rehabilitation outcomes; another study was excluded because it is not clear what exercise the control group performed.
Discussion of Results
The three articles reviewed are summarized in table 15.2. Preatoni and colleagues (2012) evaluated the effects of vibration training alone and in combination with traditional resistance training in 18 national-level female athletes (12 soccer and 6 softball athletes, with equal proportions in all groups). Subjects were randomized to one of three groups: (1) whole-body vibration training group, (2) traditional strength training group, and (3) combined whole-body vibration and strength training group. All training was performed during the winter preparatory period and in combination with other sport-specific field training such as speed drills, aerobic work, and technical and tactical skill practice. The periodized resistance training program was performed 2 days per week for 8 weeks; for the first week it consisted of six sets × six repetitions of squats performed at body weight with vibration (vibration group), at 60% 1RM (strength training group), or 30% 1RM with vibration (combined whole-body vibration and strength training group). Every 2 weeks, the external load was increased 6% (for the strength training group) and 3% (for the combined whole-body vibration and strength training group); greater intensity for the vibration group was achieved by increasing vibration frequency 5 Hz every 2 weeks (frequency was also increased for the combined group). Outcome measures included isometric strength (leg press); dynamic force, velocity, and power (explosive leg press with loads of 100% to 200% body weight in 20% increments); and power and power endurance (vertical jump and continuous 15-s vertical jumps, respectively). Training increased isometric strength (main effect, P = 0.02) with no differences between groups. No changes were observed for any parameter of the explosive leg press test. Performance on both vertical jump tests increased with training (main effect, P < 0.002), but there were no differences between groups. Maximum jump height (vertical jump test) and mean jump height and power (continuous 15-s vertical jump test) were increased only in the strength-trained group. The investigators also evaluated the characteristics of the vibration device (i.e., frequency, amplitude, and acceleration) and found variations up to 20% from the selected value; this was particularly true at higher frequencies. On the basis of other published data (Blottner et al., 2006; Mulder et al., 2008, 2007; Rittweger et al., 2006), the authors conclude that vibration exercise can elicit similar or improved outcomes compared to traditional strength training only when similar external loads are used; that is, they attribute the lack of an effect in their study to the lower external loads lifted by the combined vibration + strength training group (Preatoni et al., 2012).
Delecluse and colleagues (2005) examined the additive effect of a whole-body vibration training program over 5 weeks in 20 sprinters. Male and female sprinters (mean 100 m times: female = 12.46 ± 0.59 s, male = 11.45 ± 0.42 s) were randomly assigned to either a vibration or a control group. Both groups maintained their conventional training program, which consisted of intervals (10-60 s), speed training (two or three sessions per week with efforts near race pace), speed drills (two sessions per week), plyometric drills (one session per week), and explosive resistance training (three sessions per week) at 75% to 95% 1RM (three to five sets × two to five repetitions). In addition to their typical training, the vibration group completed three sessions per week of unloaded static and dynamic leg exercise on a vibration platform. The exercises employed were high squat, deep squat, wide stance squat, single-leg squat, lunge, and heel raise. The vibration program was implemented progressively through increases in the duration of vibration time and concomitant decreases in the rest periods; vibration amplitude (displacement) and frequency were also increased over the 5-week program. The study was conducted during the precompetitive phase of training. Outcome measures included strength (isometric and isokinetic knee extensor-flexor), maximal knee extension velocity (at 1%, 20%, 40%, and 60% of maximum isometric force), vertical jump, starting parameters (start time, horizontal start velocity, and horizontal start acceleration), and maximum velocity in a 30 m sprint. There were no changes in either group after the 5-week training program, nor were there any interaction effects or differences between groups posttraining.
Issurin, Liebermann, and Tenenbaum (1994) examined the effects of vibration training in 28 young male athletes who regularly participated in a wide cross section of club or varsity sports such as judo, swimming, volleyball, tennis, soccer, track and field, and cycling. Subjects were randomized to one of three groups: (1) upper body strength training with vibration and lower body flexibility training, (2) upper body strength training and lower body flexibility training with vibration, and (3) a calisthenics - basketball game control. The training program, which was conducted three times per week for 3 weeks, consisted of a ~10-min warm-up, a single upper body strength exercise (seated bench pull: six sets × six repetitions at 80% to 100% 1RM performed to failure), and ~20 min of specific static and ballistic stretching of the upper leg musculature. The program was performed by both experimental groups; vibration was added to either the upper or lower body activity according to group assignment. Outcome measures included strength (bench pull 1RM) and flexibility (two-leg split distance and sit and reach distance). Collectively, 1RM strength and both flexibility measures increased with training (main effects); there were also differences between groups for each outcome (group × time interaction effect). Unfortunately, the authors did not provide statistical contrasts between groups (e.g., strength training vs. strength training with vibration) to elucidate the between-group differences; because of the influence of the control group (which changed very little for any measure) on both main and interaction effects, it is difficult to interpret the study findings.
Luo, NcNamara, and Moran (2005) published a review evaluating the effects of vibration training on muscle strength and power, examining the effects of both chronic and acute vibration training. In 2005, only three papers had been published on the chronic adaptations to vibration training; of these, only one study employed trained athletes as subjects and has already been discussed (Issurin et al., 1994).
Conclusion and Strength of Evidence
There has been an explosion of literature regarding whole-body vibration in recent years. Some studies have been well conducted; others are poorly designed or uncontrolled, leading to erroneous or equivocal conclusions. There is still minimal understanding of the appropriate frequency, amplitude, direction, and length and mode of exercise needed for positive adaptations to vibration training. Despite the widespread use of vibration in athletic and private training settings, the evidence at the current time does not suggest that it is a strong tool to improve strength in athletically trained populations, although there is evidence for use in other populations.
There is level B evidence to refute the use of vibration training as a stand-alone or adjunct training method to increase muscle strength or power in athletes, as it is not demonstrably superior to traditional resistance exercise.
Program Recommendations
Although evidence supports vibration as a tool to improve strength and power in untrained populations, the data do not support its use to improve performance in athletes versus traditional strength methods. There is some evidence to support its use as a tool to acutely potentiate a power response; thus if Charity chooses to implement vibration, based on the literature it should be used as a postexcitatory potentiation tool. In general, Charity should continue training her athletes using traditional strength and conditioning programs but continue to watch the literature for emergent studies and protocols.
Save
Learn more about Evidence-Based Practice in Exercise Science.
Evidence-Based Practice in Action
On September 9, 2007, the second week of the 2007-2008 National Football League (NFL) season, the Buffalo Bills were at home for a game with the Denver Broncos. On a routine kickoff, third-year tight end Kevin Everett sprinted down the field and approached the kick returner, Domenik Hixon (Carchidi, 2008).
On September 9, 2007, the second week of the 2007-2008 National Football League (NFL) season, the Buffalo Bills were at home for a game with the Denver Broncos. On a routine kickoff, third-year tight end Kevin Everett sprinted down the field and approached the kick returner, Domenik Hixon (Carchidi, 2008). Everett dropped his center of gravity and extended into Hixon for the tackle - a motor skill that he had presumably performed thousands of times previously. Everett led with the crown of his helmet, contacting the helmet of Hixon at a high velocity, inadvertently violating a common but too often disregarded fundamental of tackling. The consequences of the collision were devastating and nearly fatal for Everett.
Immediately upon impact, Everett fell to the ground and lay face down, motionless. The collision resulted in a fracture dislocation of his third and fourth cervical vertebrae, injuring the spinal cord and instantly paralyzing Everett (Cappuccino et al., 2010; Carchidi, 2008). The sports medicine staff reacted quickly to the injury, clearing the scene to ensure that Everett was not injured further. With an injury such as Everett's, the standard-of-care protocol provides that the helmet remain on, the player be placed on a board, the face mask removed, and the player carefully moved to a stretcher and then transported by ambulance directly to the hospital. The sports medicine staff appeared to perfectly execute the protocol, and Everett was carefully transported to Millard Fillmore Gates Hospital (Carchidi, 2008).
In the ambulance ride en route to the hospital, the neurosurgery team used an experimental therapy that they hoped would improve Everett's prognosis. Infusing a cold saline solution into Everett's veins, the medical team induced a mild hypothermic state (Cappuccino et al., 2010). The use of ice to treat an injury is not novel - ice is used acutely for virtually every orthopedic injury. The principle of inducing systemic hypothermia is similar. The cold saline solution acutely controls systemic inflammation, and the medical team apparently believed that the therapy would reduce inflammation surrounding the spinal cord injury, preventing further damage (Cappuccino et al., 2010; Mummaneni, 2010). After evaluation by the medical staff, the neurosurgeon performed an emergency surgery in an attempt to save Everett's life (Cappuccino et al., 2010). After the surgery, Everett was placed on a respirator; it was believed that if he lived, he was unlikely to ever walk again (Carchidi, 2008).
Two days after the injury, Everett was removed from the respirator; he was reported to have minimal voluntary movements in his lower extremities, suggesting a theoretical possibility that he could regain the ability to walk (Cappuccino et al., 2010). On the basis on previous cases, the medical team believed that Everett had a small chance of regaining full control of his extremities (Carchidi, 2008). In the weeks and months that followed, Everett made remarkable progress, recovering at a rate far greater than expected. He was transferred to a top rehabilitation center for neurologic injuries in Houston, Texas, that implemented a comprehensive rehabilitation program. On December 23, 2007, Kevin Everett walked onto the field of Ralph Wilson Stadium - a remarkable feat that a few short months earlier had seemed impossible.
Kevin Everett's recovery was remarkable and a testament to the professional competence and readiness of the integrated sports medicine team, who made numerous decisions improving the chances that he might walk. Everett's story is also a demonstration of personal determination and perseverance that has inspired hope. For patients suffering severe spinal cord injuries, the story validates that dramatic recovery is possible. Medical personnel are encouraged in that Everett's case shows that diligent medical and rehabilitative therapy facilitates recovery. However, there is one overriding question that surrounds Kevin Everett's case: Why did he recover and why so fast? There are a number of possible explanations:
- Everett's recovery was simply a statistical improbability - he was an outlier and his recovery a chance occurrence.
- It was the result of sheer human determination and will in an athlete who simply would not accept his prognosis and would give everything to ensure he had the best chance to walk.
- It was the result of the sports medicine team's careful execution of the standard-of-care practice to prevent further injury immediately post-accident.
- Everett's recovery was the result of the precise execution of the neurosurgery team.
- The recovery was a result of the rehabilitation protocol implemented by a leading neurorehabilitation center.
- The rapid recovery was the result of cryotherapy, an experimental method that dramatically improved his prognosis.
The case of Kevin Everett highlights an important concept, that knowledge is a dynamic phenomenon (Amonette et al., 2010). The team of doctors, physical therapists, athletic trainers, and exercise specialists involved in the acute and postacute treatment of Everett's injury made numerous decisions that positively or negatively affected his outcome. The athletic trainers and sports medicine staff identified a possible injury to the spine and ensured that the athlete was quickly transported to the hospital. A careful procedure was used to move him to avoid further injury. The physicians made a decision to use the hypothermic technique to reduce spinal swelling. The neurosurgeon decided to perform surgery, and at some point, a physician determined that it was safe to remove Everett from the ventilator. In the rehabilitative process, physical therapists along with the medical team decided which therapeutic interventions were best suited to the stage of injury and made daily decisions on when to increase, decrease, or hold parameters like the intensity, volume, and duration of the rehabilitation program.
How did the sports medicine team determine the appropriate treatment?
Learn more about Evidence-Based Practice in Exercise Science.
Steps to Reading Research Critically
Reading and interpreting research may be one of the most important tasks of an evidence-based practitioner. It is important to develop the skills necessary to identify the key findings and to disregard the superfluous information.
Reading and interpreting research may be one of the most important tasks of an evidence-based practitioner. It is important to develop the skills necessary to identify the key findings and to disregard the superfluous information. Although critical appraisal is a topic left to a later chapter, next we present some practical guidelines for reading research evidence.
1-2. Read the Title and Abstract
The title of a research article can provide an important clue to the most important findings in the manuscript. But you should never read only the title and abstract. Some journal titles explicitly state the major finding of the paper. In a 1989 publication in Archives of Neurology, an article titled "Focused Stroke Rehabilitation Programs Improve Outcome" appears on pages 700-701 (Reding & McDowell, 1989) (figure 5.7). From the title alone, without reading the paper or the abstract, the reader learns that the investigators determined that a stroke rehabilitation program was effective in improving clinical outcomes. However, the very next article in the same volume of Archives of Neurology is titled "Focused Stroke Rehabilitation Programs Do Not Improve Outcome" (Dobkin, 1989) (figure 5.7). Which article is correct?
Two studies with directly contradictory titles that appeared consecutively in 1989 in Archives of Neurology.
Reprinted from PubMed.gov.
When the evidence-based practitioner relies on the title or abstract alone, he can make significant mistakes in the interpretation of research evidence. Also, examples such as the one just presented clearly show that research can be contradictory. The practitioner should read the title and abstract to determine whether the paper is relevant to the evidence-based question. If it is, he should proceed to a more careful reading and analysis to determine if the study methods and results support the findings stated in the abstract and title.
3. Read the Purpose, Construct, Theory, or Hypothesis Statement
After reading the title and abstract to determine the relevance of the study to the evidence-based question, the practitioner can skip to the final statement in the introduction that presents the study purpose, construct, theory, or hypothesis statement. This should provide the information needed to determine how the study should be designed to best answer the research question.
4. Read the Methods and Look for Flaws
The methods section is the most important part of a paper to read carefully and critically. It is from the methods section that an evidence-based practitioner can determine many of the potential biases and confounding factors associated with the study. This is also the section of the paper that determines the level or strength of evidence (chapter 8) provided by the research. As authors critically appraise their own research, they should carefully consider the study design, testing protocols, devices used, training and intervention protocols, statistical analyses, and study group allocations. If the authors are unclear in their presentation of any component of the methods, this should be a "red flag" to the reader and could potentially be a fatal flaw in the design.
Additional steps found inside Evidence-Based Practice in Exercise Science.
Translating Research Into Practice
As discussed earlier in this book, research design is a critical element to answering questions relevant to mechanistic, practical, and clinical science. One of the key aspects of research design is control of all potential confounding factors to eliminate the possibility that the outcomes arising from the intervention (independent variable) were influenced by an external factor.
As discussed earlier in this book, research design is a critical element to answering questions relevant to mechanistic, practical, and clinical science. One of the key aspects of research design is control of all potential confounding factors to eliminate the possibility that the outcomes arising from the intervention (independent variable) were influenced by an external factor. Although experimental control is a strength of research, and in particular of randomized control trials, it can also create problems when one is implementing research evidence in client, athlete, or patient populations. Suppose a clinical scientist is interested in studying the effect of interval exercise compared to steady-state exercise on hypercholesterolemia in adults who are obese. A logical study design to address such a question would be a randomized controlled trial. Consider the following hypothetical study:
One hundred participants who were obese were selected at random and then randomly assigned to one of four groups: interval exercise, short-duration steady-state exercise, long-duration steady-state exercise, and control with no exercise. In order to eliminate potential confounding factors, the participants were free from comorbidities including hypertension, insulin resistance, diabetes, overt cardiovascular disease, and recent orthopedic injuries. Before the intervention, all groups completed a treadmill
On the surface, this appears to be a sound single-blind randomized controlled trial. It is in fact well-designed and controlled, but there are some potential problems when a practitioner considers implementation. Because the scientists were interested in studying training responses to an intervention in obesity alone, they eliminated subjects with diabetes, hypertension, and other common comorbidities. This was a good decision for internal validity, but not for external validity; practitioners rarely treat individuals who are obese without any of these companion conditions (Castro, Kolka, Kim, & Bergman, 2014; Despres et al., 2008). Thus, practitioners are left to wonder whether the evidence is truly applicable to their patients or clients.
A second possible problem with the evidence is the elimination of secondary interventions. Strengths of a scientific experiment may actually be perceived as weaknesses with regard to practical implementation. In practice, multiple interventions are often implemented in concert with one another. This hypothetical experiment evaluated the effectiveness of interval versus steady-state treadmill exercise alone. An exercise practitioner is unlikely to implement the interval training protocol in isolation; instead, the protocol may be combined with resistance training, a healthy diet, and other behavioral modifications. Implementation of such multifaceted protocols may enhance the effectiveness of either of the interventions. Conversely, the addition of such interventions may also reduce the effectiveness of the protocol. Obviously, it is not scientifically plausible that resistance exercise would cause an increase in cholesterol or biologically negate the effects of the interval training protocol. However, it is possible that implementation of the secondary intervention will lead to overtraining, injury, soreness, and perhaps poor adherence to the protocol due to each of these secondary results of the combined protocol. Again, this is not likely, but it is certainly something the practitioner must consider.
Another potential problem with the implementation of scientific evidence is the possibility that a client may not be able to tolerate the protocol. For example, the initial fitness level of the client may not be sufficient to enable him to tolerate its rigors. The practitioner is then left to decide whether a modified version of the research protocol will be effective in improving blood cholesterol profiles. It is also possible that the protocol used in the scientific experiment will result in undertraining in some individuals; that is, in contrast to the previous scenario, the intensity of the stimulus may be insufficient to induce a training response. The exercise practitioner must then decide how to effectively alter the training loads in order to induce a similar response in a client or patient with a greater initial fitness level. In situations like these, it is often helpful to consult the discussion section of the research paper. Often the authors discuss in great detail the programmatic elements that they believe are responsible for the particular adaptations they observed; for instance, they may note that their subjects completed 10 intervals (with positive outcomes) in contrast to a previous study in the same population that used four intervals with negative findings. Mechanistic evidence, from either the same study or another, would further elucidate the cause(s) for the positive adaptations from a higher volume of exercise.
In medicine, one of the often cited criticisms of the evidence-based philosophy is that it leads to a cookbook approach to practice (Sackett, Rosenberg, Gray, Haynes, & Richardson, 1996). Opponents assert that evidence-based practitioners read scientific papers and then implement the protocols directly from the papers. The example we have presented illustrates that there really is no "recipe" for prescription; that is not the purpose of science. Because people are different, protocols may need to be altered to fit individual patient or client needs. Science influences the "ingredients" of the prescription. This hypothetical experiment demonstrates that interval exercise might be more effective than steady-state treadmill exercise in improving blood cholesterol of patients who are obese. It also provides some basic parameters for intensity, volume, mode, and so on for the implementation of a protocol. Practitioners must then decide whether to implement the protocol. They must also decide how they should implement interval exercise in a manner that is best suited to their client's, patient's, or athlete's individual needs and experience level.
Learn more about Evidence-Based Practice in Exercise Science.
Case Study 2: Vibration and Muscle Strength and Power
Charity is a university strength and conditioning coach. Recently, a professor in the school’s exercise physiology program acquired several vibration plates for a planned research study. The vibration plates are housed in the athletic training facility and are available to the athletes.
Charity is a university strength and conditioning coach. Recently, a professor in the school's exercise physiology program acquired several vibration plates for a planned research study. The vibration plates are housed in the athletic training facility and are available to the athletes. Charity heard about training with vibration plates at a national conference she attended recently; the presenter described a variety of upper and lower body exercises that could be performed on the plate and anecdotally claimed that such training results in noticeable performance improvements in athletes participating in a variety of sports. As an evidence-based practitioner, Charity realizes that although the vibration plate presentation was compelling, she needs to search the literature to determine what kind of scientific support exists for using vibration plate training as a modality to improve physiological and athletic performance.
Background
Vibration is thought to enhance acute neuromuscular performance via the stimulation of Ia afferent nerves, which effects a myotatic reflex contraction (Abercromby et al., 2007). Acutely, vibration improves maximal force and power output during concentric contractions; this facilitative effect is greater in elite athletes than in amateurs (Issurin & Tenenbaum, 1999; Liebermann & Issurin, 1997). However, vibration is ineffective when applied acutely to promote recovery or improve subsequent running performance after a strenuous exercise bout in highly fit runners (Edge, Mundel, Weir, & Cochrane, 2009). In competitive athletes, routine vibration training can increase strength, jump performance, and flexibility (Fagnani, Giombini, Di Cesare, Pigozzi, & Di Salvo, 2006), as well as improve proprioception and balance after anterior cruciate ligament reconstruction in comparison to a conventional rehabilitation program (Moezy, Olyaei, Hadian, Razi, & Faghihzadeh, 2008).
Charity currently employs evidence-based strength and conditioning programs with her athletes; these programs consist largely of resistance exercise - both traditional strength and explosive Olympic weightlifting exercises. Thus, to make a valid comparison in her athletic population, Charity should compare the effectiveness of vibration training to that of traditional resistance exercise. Given the limitations of vibration training (cost, availability, spatial restrictions), only if vibration training (either alone or in combination with traditional training) proves superior to traditional training would it be prudent to incorporate it on a large scale. Thus the evidence-based question is as follows.
In trained athletes, does vibration training, either alone or as an adjunct to resistance exercise, elicit improvements in muscle strength or power that are superior to those realized with traditional resistance training?
Search Strategy
Typing "vibration" into PubMed yields a list of MeSH subheadings; we select "vibration training." This returns 1141 studies. Activating the Age filter (Adult: 19-44 years) and Language filter (English) reduces this number to 377. Next, we add "AND athletes" to the search string ("vibration training AND athletes"), which returns 20 articles. Scanning these abstracts reveals 3 papers directly related to the chronic effects of vibration training (Delecluse et al., 2005; Issurin, Liebermann, & Tenenbaum, 1994; Preatoni et al., 2012). Of the 17 articles not included, most are acute studies and several others examine the effects of vibration on postworkout recovery and postsurgical rehabilitation outcomes; another study was excluded because it is not clear what exercise the control group performed.
Discussion of Results
The three articles reviewed are summarized in table 15.2. Preatoni and colleagues (2012) evaluated the effects of vibration training alone and in combination with traditional resistance training in 18 national-level female athletes (12 soccer and 6 softball athletes, with equal proportions in all groups). Subjects were randomized to one of three groups: (1) whole-body vibration training group, (2) traditional strength training group, and (3) combined whole-body vibration and strength training group. All training was performed during the winter preparatory period and in combination with other sport-specific field training such as speed drills, aerobic work, and technical and tactical skill practice. The periodized resistance training program was performed 2 days per week for 8 weeks; for the first week it consisted of six sets × six repetitions of squats performed at body weight with vibration (vibration group), at 60% 1RM (strength training group), or 30% 1RM with vibration (combined whole-body vibration and strength training group). Every 2 weeks, the external load was increased 6% (for the strength training group) and 3% (for the combined whole-body vibration and strength training group); greater intensity for the vibration group was achieved by increasing vibration frequency 5 Hz every 2 weeks (frequency was also increased for the combined group). Outcome measures included isometric strength (leg press); dynamic force, velocity, and power (explosive leg press with loads of 100% to 200% body weight in 20% increments); and power and power endurance (vertical jump and continuous 15-s vertical jumps, respectively). Training increased isometric strength (main effect, P = 0.02) with no differences between groups. No changes were observed for any parameter of the explosive leg press test. Performance on both vertical jump tests increased with training (main effect, P < 0.002), but there were no differences between groups. Maximum jump height (vertical jump test) and mean jump height and power (continuous 15-s vertical jump test) were increased only in the strength-trained group. The investigators also evaluated the characteristics of the vibration device (i.e., frequency, amplitude, and acceleration) and found variations up to 20% from the selected value; this was particularly true at higher frequencies. On the basis of other published data (Blottner et al., 2006; Mulder et al., 2008, 2007; Rittweger et al., 2006), the authors conclude that vibration exercise can elicit similar or improved outcomes compared to traditional strength training only when similar external loads are used; that is, they attribute the lack of an effect in their study to the lower external loads lifted by the combined vibration + strength training group (Preatoni et al., 2012).
Delecluse and colleagues (2005) examined the additive effect of a whole-body vibration training program over 5 weeks in 20 sprinters. Male and female sprinters (mean 100 m times: female = 12.46 ± 0.59 s, male = 11.45 ± 0.42 s) were randomly assigned to either a vibration or a control group. Both groups maintained their conventional training program, which consisted of intervals (10-60 s), speed training (two or three sessions per week with efforts near race pace), speed drills (two sessions per week), plyometric drills (one session per week), and explosive resistance training (three sessions per week) at 75% to 95% 1RM (three to five sets × two to five repetitions). In addition to their typical training, the vibration group completed three sessions per week of unloaded static and dynamic leg exercise on a vibration platform. The exercises employed were high squat, deep squat, wide stance squat, single-leg squat, lunge, and heel raise. The vibration program was implemented progressively through increases in the duration of vibration time and concomitant decreases in the rest periods; vibration amplitude (displacement) and frequency were also increased over the 5-week program. The study was conducted during the precompetitive phase of training. Outcome measures included strength (isometric and isokinetic knee extensor-flexor), maximal knee extension velocity (at 1%, 20%, 40%, and 60% of maximum isometric force), vertical jump, starting parameters (start time, horizontal start velocity, and horizontal start acceleration), and maximum velocity in a 30 m sprint. There were no changes in either group after the 5-week training program, nor were there any interaction effects or differences between groups posttraining.
Issurin, Liebermann, and Tenenbaum (1994) examined the effects of vibration training in 28 young male athletes who regularly participated in a wide cross section of club or varsity sports such as judo, swimming, volleyball, tennis, soccer, track and field, and cycling. Subjects were randomized to one of three groups: (1) upper body strength training with vibration and lower body flexibility training, (2) upper body strength training and lower body flexibility training with vibration, and (3) a calisthenics - basketball game control. The training program, which was conducted three times per week for 3 weeks, consisted of a ~10-min warm-up, a single upper body strength exercise (seated bench pull: six sets × six repetitions at 80% to 100% 1RM performed to failure), and ~20 min of specific static and ballistic stretching of the upper leg musculature. The program was performed by both experimental groups; vibration was added to either the upper or lower body activity according to group assignment. Outcome measures included strength (bench pull 1RM) and flexibility (two-leg split distance and sit and reach distance). Collectively, 1RM strength and both flexibility measures increased with training (main effects); there were also differences between groups for each outcome (group × time interaction effect). Unfortunately, the authors did not provide statistical contrasts between groups (e.g., strength training vs. strength training with vibration) to elucidate the between-group differences; because of the influence of the control group (which changed very little for any measure) on both main and interaction effects, it is difficult to interpret the study findings.
Luo, NcNamara, and Moran (2005) published a review evaluating the effects of vibration training on muscle strength and power, examining the effects of both chronic and acute vibration training. In 2005, only three papers had been published on the chronic adaptations to vibration training; of these, only one study employed trained athletes as subjects and has already been discussed (Issurin et al., 1994).
Conclusion and Strength of Evidence
There has been an explosion of literature regarding whole-body vibration in recent years. Some studies have been well conducted; others are poorly designed or uncontrolled, leading to erroneous or equivocal conclusions. There is still minimal understanding of the appropriate frequency, amplitude, direction, and length and mode of exercise needed for positive adaptations to vibration training. Despite the widespread use of vibration in athletic and private training settings, the evidence at the current time does not suggest that it is a strong tool to improve strength in athletically trained populations, although there is evidence for use in other populations.
There is level B evidence to refute the use of vibration training as a stand-alone or adjunct training method to increase muscle strength or power in athletes, as it is not demonstrably superior to traditional resistance exercise.
Program Recommendations
Although evidence supports vibration as a tool to improve strength and power in untrained populations, the data do not support its use to improve performance in athletes versus traditional strength methods. There is some evidence to support its use as a tool to acutely potentiate a power response; thus if Charity chooses to implement vibration, based on the literature it should be used as a postexcitatory potentiation tool. In general, Charity should continue training her athletes using traditional strength and conditioning programs but continue to watch the literature for emergent studies and protocols.
Save
Learn more about Evidence-Based Practice in Exercise Science.
Evidence-Based Practice in Action
On September 9, 2007, the second week of the 2007-2008 National Football League (NFL) season, the Buffalo Bills were at home for a game with the Denver Broncos. On a routine kickoff, third-year tight end Kevin Everett sprinted down the field and approached the kick returner, Domenik Hixon (Carchidi, 2008).
On September 9, 2007, the second week of the 2007-2008 National Football League (NFL) season, the Buffalo Bills were at home for a game with the Denver Broncos. On a routine kickoff, third-year tight end Kevin Everett sprinted down the field and approached the kick returner, Domenik Hixon (Carchidi, 2008). Everett dropped his center of gravity and extended into Hixon for the tackle - a motor skill that he had presumably performed thousands of times previously. Everett led with the crown of his helmet, contacting the helmet of Hixon at a high velocity, inadvertently violating a common but too often disregarded fundamental of tackling. The consequences of the collision were devastating and nearly fatal for Everett.
Immediately upon impact, Everett fell to the ground and lay face down, motionless. The collision resulted in a fracture dislocation of his third and fourth cervical vertebrae, injuring the spinal cord and instantly paralyzing Everett (Cappuccino et al., 2010; Carchidi, 2008). The sports medicine staff reacted quickly to the injury, clearing the scene to ensure that Everett was not injured further. With an injury such as Everett's, the standard-of-care protocol provides that the helmet remain on, the player be placed on a board, the face mask removed, and the player carefully moved to a stretcher and then transported by ambulance directly to the hospital. The sports medicine staff appeared to perfectly execute the protocol, and Everett was carefully transported to Millard Fillmore Gates Hospital (Carchidi, 2008).
In the ambulance ride en route to the hospital, the neurosurgery team used an experimental therapy that they hoped would improve Everett's prognosis. Infusing a cold saline solution into Everett's veins, the medical team induced a mild hypothermic state (Cappuccino et al., 2010). The use of ice to treat an injury is not novel - ice is used acutely for virtually every orthopedic injury. The principle of inducing systemic hypothermia is similar. The cold saline solution acutely controls systemic inflammation, and the medical team apparently believed that the therapy would reduce inflammation surrounding the spinal cord injury, preventing further damage (Cappuccino et al., 2010; Mummaneni, 2010). After evaluation by the medical staff, the neurosurgeon performed an emergency surgery in an attempt to save Everett's life (Cappuccino et al., 2010). After the surgery, Everett was placed on a respirator; it was believed that if he lived, he was unlikely to ever walk again (Carchidi, 2008).
Two days after the injury, Everett was removed from the respirator; he was reported to have minimal voluntary movements in his lower extremities, suggesting a theoretical possibility that he could regain the ability to walk (Cappuccino et al., 2010). On the basis on previous cases, the medical team believed that Everett had a small chance of regaining full control of his extremities (Carchidi, 2008). In the weeks and months that followed, Everett made remarkable progress, recovering at a rate far greater than expected. He was transferred to a top rehabilitation center for neurologic injuries in Houston, Texas, that implemented a comprehensive rehabilitation program. On December 23, 2007, Kevin Everett walked onto the field of Ralph Wilson Stadium - a remarkable feat that a few short months earlier had seemed impossible.
Kevin Everett's recovery was remarkable and a testament to the professional competence and readiness of the integrated sports medicine team, who made numerous decisions improving the chances that he might walk. Everett's story is also a demonstration of personal determination and perseverance that has inspired hope. For patients suffering severe spinal cord injuries, the story validates that dramatic recovery is possible. Medical personnel are encouraged in that Everett's case shows that diligent medical and rehabilitative therapy facilitates recovery. However, there is one overriding question that surrounds Kevin Everett's case: Why did he recover and why so fast? There are a number of possible explanations:
- Everett's recovery was simply a statistical improbability - he was an outlier and his recovery a chance occurrence.
- It was the result of sheer human determination and will in an athlete who simply would not accept his prognosis and would give everything to ensure he had the best chance to walk.
- It was the result of the sports medicine team's careful execution of the standard-of-care practice to prevent further injury immediately post-accident.
- Everett's recovery was the result of the precise execution of the neurosurgery team.
- The recovery was a result of the rehabilitation protocol implemented by a leading neurorehabilitation center.
- The rapid recovery was the result of cryotherapy, an experimental method that dramatically improved his prognosis.
The case of Kevin Everett highlights an important concept, that knowledge is a dynamic phenomenon (Amonette et al., 2010). The team of doctors, physical therapists, athletic trainers, and exercise specialists involved in the acute and postacute treatment of Everett's injury made numerous decisions that positively or negatively affected his outcome. The athletic trainers and sports medicine staff identified a possible injury to the spine and ensured that the athlete was quickly transported to the hospital. A careful procedure was used to move him to avoid further injury. The physicians made a decision to use the hypothermic technique to reduce spinal swelling. The neurosurgeon decided to perform surgery, and at some point, a physician determined that it was safe to remove Everett from the ventilator. In the rehabilitative process, physical therapists along with the medical team decided which therapeutic interventions were best suited to the stage of injury and made daily decisions on when to increase, decrease, or hold parameters like the intensity, volume, and duration of the rehabilitation program.
How did the sports medicine team determine the appropriate treatment?
Learn more about Evidence-Based Practice in Exercise Science.
Steps to Reading Research Critically
Reading and interpreting research may be one of the most important tasks of an evidence-based practitioner. It is important to develop the skills necessary to identify the key findings and to disregard the superfluous information.
Reading and interpreting research may be one of the most important tasks of an evidence-based practitioner. It is important to develop the skills necessary to identify the key findings and to disregard the superfluous information. Although critical appraisal is a topic left to a later chapter, next we present some practical guidelines for reading research evidence.
1-2. Read the Title and Abstract
The title of a research article can provide an important clue to the most important findings in the manuscript. But you should never read only the title and abstract. Some journal titles explicitly state the major finding of the paper. In a 1989 publication in Archives of Neurology, an article titled "Focused Stroke Rehabilitation Programs Improve Outcome" appears on pages 700-701 (Reding & McDowell, 1989) (figure 5.7). From the title alone, without reading the paper or the abstract, the reader learns that the investigators determined that a stroke rehabilitation program was effective in improving clinical outcomes. However, the very next article in the same volume of Archives of Neurology is titled "Focused Stroke Rehabilitation Programs Do Not Improve Outcome" (Dobkin, 1989) (figure 5.7). Which article is correct?
Two studies with directly contradictory titles that appeared consecutively in 1989 in Archives of Neurology.
Reprinted from PubMed.gov.
When the evidence-based practitioner relies on the title or abstract alone, he can make significant mistakes in the interpretation of research evidence. Also, examples such as the one just presented clearly show that research can be contradictory. The practitioner should read the title and abstract to determine whether the paper is relevant to the evidence-based question. If it is, he should proceed to a more careful reading and analysis to determine if the study methods and results support the findings stated in the abstract and title.
3. Read the Purpose, Construct, Theory, or Hypothesis Statement
After reading the title and abstract to determine the relevance of the study to the evidence-based question, the practitioner can skip to the final statement in the introduction that presents the study purpose, construct, theory, or hypothesis statement. This should provide the information needed to determine how the study should be designed to best answer the research question.
4. Read the Methods and Look for Flaws
The methods section is the most important part of a paper to read carefully and critically. It is from the methods section that an evidence-based practitioner can determine many of the potential biases and confounding factors associated with the study. This is also the section of the paper that determines the level or strength of evidence (chapter 8) provided by the research. As authors critically appraise their own research, they should carefully consider the study design, testing protocols, devices used, training and intervention protocols, statistical analyses, and study group allocations. If the authors are unclear in their presentation of any component of the methods, this should be a "red flag" to the reader and could potentially be a fatal flaw in the design.
Additional steps found inside Evidence-Based Practice in Exercise Science.
Translating Research Into Practice
As discussed earlier in this book, research design is a critical element to answering questions relevant to mechanistic, practical, and clinical science. One of the key aspects of research design is control of all potential confounding factors to eliminate the possibility that the outcomes arising from the intervention (independent variable) were influenced by an external factor.
As discussed earlier in this book, research design is a critical element to answering questions relevant to mechanistic, practical, and clinical science. One of the key aspects of research design is control of all potential confounding factors to eliminate the possibility that the outcomes arising from the intervention (independent variable) were influenced by an external factor. Although experimental control is a strength of research, and in particular of randomized control trials, it can also create problems when one is implementing research evidence in client, athlete, or patient populations. Suppose a clinical scientist is interested in studying the effect of interval exercise compared to steady-state exercise on hypercholesterolemia in adults who are obese. A logical study design to address such a question would be a randomized controlled trial. Consider the following hypothetical study:
One hundred participants who were obese were selected at random and then randomly assigned to one of four groups: interval exercise, short-duration steady-state exercise, long-duration steady-state exercise, and control with no exercise. In order to eliminate potential confounding factors, the participants were free from comorbidities including hypertension, insulin resistance, diabetes, overt cardiovascular disease, and recent orthopedic injuries. Before the intervention, all groups completed a treadmill
On the surface, this appears to be a sound single-blind randomized controlled trial. It is in fact well-designed and controlled, but there are some potential problems when a practitioner considers implementation. Because the scientists were interested in studying training responses to an intervention in obesity alone, they eliminated subjects with diabetes, hypertension, and other common comorbidities. This was a good decision for internal validity, but not for external validity; practitioners rarely treat individuals who are obese without any of these companion conditions (Castro, Kolka, Kim, & Bergman, 2014; Despres et al., 2008). Thus, practitioners are left to wonder whether the evidence is truly applicable to their patients or clients.
A second possible problem with the evidence is the elimination of secondary interventions. Strengths of a scientific experiment may actually be perceived as weaknesses with regard to practical implementation. In practice, multiple interventions are often implemented in concert with one another. This hypothetical experiment evaluated the effectiveness of interval versus steady-state treadmill exercise alone. An exercise practitioner is unlikely to implement the interval training protocol in isolation; instead, the protocol may be combined with resistance training, a healthy diet, and other behavioral modifications. Implementation of such multifaceted protocols may enhance the effectiveness of either of the interventions. Conversely, the addition of such interventions may also reduce the effectiveness of the protocol. Obviously, it is not scientifically plausible that resistance exercise would cause an increase in cholesterol or biologically negate the effects of the interval training protocol. However, it is possible that implementation of the secondary intervention will lead to overtraining, injury, soreness, and perhaps poor adherence to the protocol due to each of these secondary results of the combined protocol. Again, this is not likely, but it is certainly something the practitioner must consider.
Another potential problem with the implementation of scientific evidence is the possibility that a client may not be able to tolerate the protocol. For example, the initial fitness level of the client may not be sufficient to enable him to tolerate its rigors. The practitioner is then left to decide whether a modified version of the research protocol will be effective in improving blood cholesterol profiles. It is also possible that the protocol used in the scientific experiment will result in undertraining in some individuals; that is, in contrast to the previous scenario, the intensity of the stimulus may be insufficient to induce a training response. The exercise practitioner must then decide how to effectively alter the training loads in order to induce a similar response in a client or patient with a greater initial fitness level. In situations like these, it is often helpful to consult the discussion section of the research paper. Often the authors discuss in great detail the programmatic elements that they believe are responsible for the particular adaptations they observed; for instance, they may note that their subjects completed 10 intervals (with positive outcomes) in contrast to a previous study in the same population that used four intervals with negative findings. Mechanistic evidence, from either the same study or another, would further elucidate the cause(s) for the positive adaptations from a higher volume of exercise.
In medicine, one of the often cited criticisms of the evidence-based philosophy is that it leads to a cookbook approach to practice (Sackett, Rosenberg, Gray, Haynes, & Richardson, 1996). Opponents assert that evidence-based practitioners read scientific papers and then implement the protocols directly from the papers. The example we have presented illustrates that there really is no "recipe" for prescription; that is not the purpose of science. Because people are different, protocols may need to be altered to fit individual patient or client needs. Science influences the "ingredients" of the prescription. This hypothetical experiment demonstrates that interval exercise might be more effective than steady-state treadmill exercise in improving blood cholesterol of patients who are obese. It also provides some basic parameters for intensity, volume, mode, and so on for the implementation of a protocol. Practitioners must then decide whether to implement the protocol. They must also decide how they should implement interval exercise in a manner that is best suited to their client's, patient's, or athlete's individual needs and experience level.
Learn more about Evidence-Based Practice in Exercise Science.
Case Study 2: Vibration and Muscle Strength and Power
Charity is a university strength and conditioning coach. Recently, a professor in the school’s exercise physiology program acquired several vibration plates for a planned research study. The vibration plates are housed in the athletic training facility and are available to the athletes.
Charity is a university strength and conditioning coach. Recently, a professor in the school's exercise physiology program acquired several vibration plates for a planned research study. The vibration plates are housed in the athletic training facility and are available to the athletes. Charity heard about training with vibration plates at a national conference she attended recently; the presenter described a variety of upper and lower body exercises that could be performed on the plate and anecdotally claimed that such training results in noticeable performance improvements in athletes participating in a variety of sports. As an evidence-based practitioner, Charity realizes that although the vibration plate presentation was compelling, she needs to search the literature to determine what kind of scientific support exists for using vibration plate training as a modality to improve physiological and athletic performance.
Background
Vibration is thought to enhance acute neuromuscular performance via the stimulation of Ia afferent nerves, which effects a myotatic reflex contraction (Abercromby et al., 2007). Acutely, vibration improves maximal force and power output during concentric contractions; this facilitative effect is greater in elite athletes than in amateurs (Issurin & Tenenbaum, 1999; Liebermann & Issurin, 1997). However, vibration is ineffective when applied acutely to promote recovery or improve subsequent running performance after a strenuous exercise bout in highly fit runners (Edge, Mundel, Weir, & Cochrane, 2009). In competitive athletes, routine vibration training can increase strength, jump performance, and flexibility (Fagnani, Giombini, Di Cesare, Pigozzi, & Di Salvo, 2006), as well as improve proprioception and balance after anterior cruciate ligament reconstruction in comparison to a conventional rehabilitation program (Moezy, Olyaei, Hadian, Razi, & Faghihzadeh, 2008).
Charity currently employs evidence-based strength and conditioning programs with her athletes; these programs consist largely of resistance exercise - both traditional strength and explosive Olympic weightlifting exercises. Thus, to make a valid comparison in her athletic population, Charity should compare the effectiveness of vibration training to that of traditional resistance exercise. Given the limitations of vibration training (cost, availability, spatial restrictions), only if vibration training (either alone or in combination with traditional training) proves superior to traditional training would it be prudent to incorporate it on a large scale. Thus the evidence-based question is as follows.
In trained athletes, does vibration training, either alone or as an adjunct to resistance exercise, elicit improvements in muscle strength or power that are superior to those realized with traditional resistance training?
Search Strategy
Typing "vibration" into PubMed yields a list of MeSH subheadings; we select "vibration training." This returns 1141 studies. Activating the Age filter (Adult: 19-44 years) and Language filter (English) reduces this number to 377. Next, we add "AND athletes" to the search string ("vibration training AND athletes"), which returns 20 articles. Scanning these abstracts reveals 3 papers directly related to the chronic effects of vibration training (Delecluse et al., 2005; Issurin, Liebermann, & Tenenbaum, 1994; Preatoni et al., 2012). Of the 17 articles not included, most are acute studies and several others examine the effects of vibration on postworkout recovery and postsurgical rehabilitation outcomes; another study was excluded because it is not clear what exercise the control group performed.
Discussion of Results
The three articles reviewed are summarized in table 15.2. Preatoni and colleagues (2012) evaluated the effects of vibration training alone and in combination with traditional resistance training in 18 national-level female athletes (12 soccer and 6 softball athletes, with equal proportions in all groups). Subjects were randomized to one of three groups: (1) whole-body vibration training group, (2) traditional strength training group, and (3) combined whole-body vibration and strength training group. All training was performed during the winter preparatory period and in combination with other sport-specific field training such as speed drills, aerobic work, and technical and tactical skill practice. The periodized resistance training program was performed 2 days per week for 8 weeks; for the first week it consisted of six sets × six repetitions of squats performed at body weight with vibration (vibration group), at 60% 1RM (strength training group), or 30% 1RM with vibration (combined whole-body vibration and strength training group). Every 2 weeks, the external load was increased 6% (for the strength training group) and 3% (for the combined whole-body vibration and strength training group); greater intensity for the vibration group was achieved by increasing vibration frequency 5 Hz every 2 weeks (frequency was also increased for the combined group). Outcome measures included isometric strength (leg press); dynamic force, velocity, and power (explosive leg press with loads of 100% to 200% body weight in 20% increments); and power and power endurance (vertical jump and continuous 15-s vertical jumps, respectively). Training increased isometric strength (main effect, P = 0.02) with no differences between groups. No changes were observed for any parameter of the explosive leg press test. Performance on both vertical jump tests increased with training (main effect, P < 0.002), but there were no differences between groups. Maximum jump height (vertical jump test) and mean jump height and power (continuous 15-s vertical jump test) were increased only in the strength-trained group. The investigators also evaluated the characteristics of the vibration device (i.e., frequency, amplitude, and acceleration) and found variations up to 20% from the selected value; this was particularly true at higher frequencies. On the basis of other published data (Blottner et al., 2006; Mulder et al., 2008, 2007; Rittweger et al., 2006), the authors conclude that vibration exercise can elicit similar or improved outcomes compared to traditional strength training only when similar external loads are used; that is, they attribute the lack of an effect in their study to the lower external loads lifted by the combined vibration + strength training group (Preatoni et al., 2012).
Delecluse and colleagues (2005) examined the additive effect of a whole-body vibration training program over 5 weeks in 20 sprinters. Male and female sprinters (mean 100 m times: female = 12.46 ± 0.59 s, male = 11.45 ± 0.42 s) were randomly assigned to either a vibration or a control group. Both groups maintained their conventional training program, which consisted of intervals (10-60 s), speed training (two or three sessions per week with efforts near race pace), speed drills (two sessions per week), plyometric drills (one session per week), and explosive resistance training (three sessions per week) at 75% to 95% 1RM (three to five sets × two to five repetitions). In addition to their typical training, the vibration group completed three sessions per week of unloaded static and dynamic leg exercise on a vibration platform. The exercises employed were high squat, deep squat, wide stance squat, single-leg squat, lunge, and heel raise. The vibration program was implemented progressively through increases in the duration of vibration time and concomitant decreases in the rest periods; vibration amplitude (displacement) and frequency were also increased over the 5-week program. The study was conducted during the precompetitive phase of training. Outcome measures included strength (isometric and isokinetic knee extensor-flexor), maximal knee extension velocity (at 1%, 20%, 40%, and 60% of maximum isometric force), vertical jump, starting parameters (start time, horizontal start velocity, and horizontal start acceleration), and maximum velocity in a 30 m sprint. There were no changes in either group after the 5-week training program, nor were there any interaction effects or differences between groups posttraining.
Issurin, Liebermann, and Tenenbaum (1994) examined the effects of vibration training in 28 young male athletes who regularly participated in a wide cross section of club or varsity sports such as judo, swimming, volleyball, tennis, soccer, track and field, and cycling. Subjects were randomized to one of three groups: (1) upper body strength training with vibration and lower body flexibility training, (2) upper body strength training and lower body flexibility training with vibration, and (3) a calisthenics - basketball game control. The training program, which was conducted three times per week for 3 weeks, consisted of a ~10-min warm-up, a single upper body strength exercise (seated bench pull: six sets × six repetitions at 80% to 100% 1RM performed to failure), and ~20 min of specific static and ballistic stretching of the upper leg musculature. The program was performed by both experimental groups; vibration was added to either the upper or lower body activity according to group assignment. Outcome measures included strength (bench pull 1RM) and flexibility (two-leg split distance and sit and reach distance). Collectively, 1RM strength and both flexibility measures increased with training (main effects); there were also differences between groups for each outcome (group × time interaction effect). Unfortunately, the authors did not provide statistical contrasts between groups (e.g., strength training vs. strength training with vibration) to elucidate the between-group differences; because of the influence of the control group (which changed very little for any measure) on both main and interaction effects, it is difficult to interpret the study findings.
Luo, NcNamara, and Moran (2005) published a review evaluating the effects of vibration training on muscle strength and power, examining the effects of both chronic and acute vibration training. In 2005, only three papers had been published on the chronic adaptations to vibration training; of these, only one study employed trained athletes as subjects and has already been discussed (Issurin et al., 1994).
Conclusion and Strength of Evidence
There has been an explosion of literature regarding whole-body vibration in recent years. Some studies have been well conducted; others are poorly designed or uncontrolled, leading to erroneous or equivocal conclusions. There is still minimal understanding of the appropriate frequency, amplitude, direction, and length and mode of exercise needed for positive adaptations to vibration training. Despite the widespread use of vibration in athletic and private training settings, the evidence at the current time does not suggest that it is a strong tool to improve strength in athletically trained populations, although there is evidence for use in other populations.
There is level B evidence to refute the use of vibration training as a stand-alone or adjunct training method to increase muscle strength or power in athletes, as it is not demonstrably superior to traditional resistance exercise.
Program Recommendations
Although evidence supports vibration as a tool to improve strength and power in untrained populations, the data do not support its use to improve performance in athletes versus traditional strength methods. There is some evidence to support its use as a tool to acutely potentiate a power response; thus if Charity chooses to implement vibration, based on the literature it should be used as a postexcitatory potentiation tool. In general, Charity should continue training her athletes using traditional strength and conditioning programs but continue to watch the literature for emergent studies and protocols.
Save
Learn more about Evidence-Based Practice in Exercise Science.
Evidence-Based Practice in Action
On September 9, 2007, the second week of the 2007-2008 National Football League (NFL) season, the Buffalo Bills were at home for a game with the Denver Broncos. On a routine kickoff, third-year tight end Kevin Everett sprinted down the field and approached the kick returner, Domenik Hixon (Carchidi, 2008).
On September 9, 2007, the second week of the 2007-2008 National Football League (NFL) season, the Buffalo Bills were at home for a game with the Denver Broncos. On a routine kickoff, third-year tight end Kevin Everett sprinted down the field and approached the kick returner, Domenik Hixon (Carchidi, 2008). Everett dropped his center of gravity and extended into Hixon for the tackle - a motor skill that he had presumably performed thousands of times previously. Everett led with the crown of his helmet, contacting the helmet of Hixon at a high velocity, inadvertently violating a common but too often disregarded fundamental of tackling. The consequences of the collision were devastating and nearly fatal for Everett.
Immediately upon impact, Everett fell to the ground and lay face down, motionless. The collision resulted in a fracture dislocation of his third and fourth cervical vertebrae, injuring the spinal cord and instantly paralyzing Everett (Cappuccino et al., 2010; Carchidi, 2008). The sports medicine staff reacted quickly to the injury, clearing the scene to ensure that Everett was not injured further. With an injury such as Everett's, the standard-of-care protocol provides that the helmet remain on, the player be placed on a board, the face mask removed, and the player carefully moved to a stretcher and then transported by ambulance directly to the hospital. The sports medicine staff appeared to perfectly execute the protocol, and Everett was carefully transported to Millard Fillmore Gates Hospital (Carchidi, 2008).
In the ambulance ride en route to the hospital, the neurosurgery team used an experimental therapy that they hoped would improve Everett's prognosis. Infusing a cold saline solution into Everett's veins, the medical team induced a mild hypothermic state (Cappuccino et al., 2010). The use of ice to treat an injury is not novel - ice is used acutely for virtually every orthopedic injury. The principle of inducing systemic hypothermia is similar. The cold saline solution acutely controls systemic inflammation, and the medical team apparently believed that the therapy would reduce inflammation surrounding the spinal cord injury, preventing further damage (Cappuccino et al., 2010; Mummaneni, 2010). After evaluation by the medical staff, the neurosurgeon performed an emergency surgery in an attempt to save Everett's life (Cappuccino et al., 2010). After the surgery, Everett was placed on a respirator; it was believed that if he lived, he was unlikely to ever walk again (Carchidi, 2008).
Two days after the injury, Everett was removed from the respirator; he was reported to have minimal voluntary movements in his lower extremities, suggesting a theoretical possibility that he could regain the ability to walk (Cappuccino et al., 2010). On the basis on previous cases, the medical team believed that Everett had a small chance of regaining full control of his extremities (Carchidi, 2008). In the weeks and months that followed, Everett made remarkable progress, recovering at a rate far greater than expected. He was transferred to a top rehabilitation center for neurologic injuries in Houston, Texas, that implemented a comprehensive rehabilitation program. On December 23, 2007, Kevin Everett walked onto the field of Ralph Wilson Stadium - a remarkable feat that a few short months earlier had seemed impossible.
Kevin Everett's recovery was remarkable and a testament to the professional competence and readiness of the integrated sports medicine team, who made numerous decisions improving the chances that he might walk. Everett's story is also a demonstration of personal determination and perseverance that has inspired hope. For patients suffering severe spinal cord injuries, the story validates that dramatic recovery is possible. Medical personnel are encouraged in that Everett's case shows that diligent medical and rehabilitative therapy facilitates recovery. However, there is one overriding question that surrounds Kevin Everett's case: Why did he recover and why so fast? There are a number of possible explanations:
- Everett's recovery was simply a statistical improbability - he was an outlier and his recovery a chance occurrence.
- It was the result of sheer human determination and will in an athlete who simply would not accept his prognosis and would give everything to ensure he had the best chance to walk.
- It was the result of the sports medicine team's careful execution of the standard-of-care practice to prevent further injury immediately post-accident.
- Everett's recovery was the result of the precise execution of the neurosurgery team.
- The recovery was a result of the rehabilitation protocol implemented by a leading neurorehabilitation center.
- The rapid recovery was the result of cryotherapy, an experimental method that dramatically improved his prognosis.
The case of Kevin Everett highlights an important concept, that knowledge is a dynamic phenomenon (Amonette et al., 2010). The team of doctors, physical therapists, athletic trainers, and exercise specialists involved in the acute and postacute treatment of Everett's injury made numerous decisions that positively or negatively affected his outcome. The athletic trainers and sports medicine staff identified a possible injury to the spine and ensured that the athlete was quickly transported to the hospital. A careful procedure was used to move him to avoid further injury. The physicians made a decision to use the hypothermic technique to reduce spinal swelling. The neurosurgeon decided to perform surgery, and at some point, a physician determined that it was safe to remove Everett from the ventilator. In the rehabilitative process, physical therapists along with the medical team decided which therapeutic interventions were best suited to the stage of injury and made daily decisions on when to increase, decrease, or hold parameters like the intensity, volume, and duration of the rehabilitation program.
How did the sports medicine team determine the appropriate treatment?
Learn more about Evidence-Based Practice in Exercise Science.
Steps to Reading Research Critically
Reading and interpreting research may be one of the most important tasks of an evidence-based practitioner. It is important to develop the skills necessary to identify the key findings and to disregard the superfluous information.
Reading and interpreting research may be one of the most important tasks of an evidence-based practitioner. It is important to develop the skills necessary to identify the key findings and to disregard the superfluous information. Although critical appraisal is a topic left to a later chapter, next we present some practical guidelines for reading research evidence.
1-2. Read the Title and Abstract
The title of a research article can provide an important clue to the most important findings in the manuscript. But you should never read only the title and abstract. Some journal titles explicitly state the major finding of the paper. In a 1989 publication in Archives of Neurology, an article titled "Focused Stroke Rehabilitation Programs Improve Outcome" appears on pages 700-701 (Reding & McDowell, 1989) (figure 5.7). From the title alone, without reading the paper or the abstract, the reader learns that the investigators determined that a stroke rehabilitation program was effective in improving clinical outcomes. However, the very next article in the same volume of Archives of Neurology is titled "Focused Stroke Rehabilitation Programs Do Not Improve Outcome" (Dobkin, 1989) (figure 5.7). Which article is correct?
Two studies with directly contradictory titles that appeared consecutively in 1989 in Archives of Neurology.
Reprinted from PubMed.gov.
When the evidence-based practitioner relies on the title or abstract alone, he can make significant mistakes in the interpretation of research evidence. Also, examples such as the one just presented clearly show that research can be contradictory. The practitioner should read the title and abstract to determine whether the paper is relevant to the evidence-based question. If it is, he should proceed to a more careful reading and analysis to determine if the study methods and results support the findings stated in the abstract and title.
3. Read the Purpose, Construct, Theory, or Hypothesis Statement
After reading the title and abstract to determine the relevance of the study to the evidence-based question, the practitioner can skip to the final statement in the introduction that presents the study purpose, construct, theory, or hypothesis statement. This should provide the information needed to determine how the study should be designed to best answer the research question.
4. Read the Methods and Look for Flaws
The methods section is the most important part of a paper to read carefully and critically. It is from the methods section that an evidence-based practitioner can determine many of the potential biases and confounding factors associated with the study. This is also the section of the paper that determines the level or strength of evidence (chapter 8) provided by the research. As authors critically appraise their own research, they should carefully consider the study design, testing protocols, devices used, training and intervention protocols, statistical analyses, and study group allocations. If the authors are unclear in their presentation of any component of the methods, this should be a "red flag" to the reader and could potentially be a fatal flaw in the design.
Additional steps found inside Evidence-Based Practice in Exercise Science.
Translating Research Into Practice
As discussed earlier in this book, research design is a critical element to answering questions relevant to mechanistic, practical, and clinical science. One of the key aspects of research design is control of all potential confounding factors to eliminate the possibility that the outcomes arising from the intervention (independent variable) were influenced by an external factor.
As discussed earlier in this book, research design is a critical element to answering questions relevant to mechanistic, practical, and clinical science. One of the key aspects of research design is control of all potential confounding factors to eliminate the possibility that the outcomes arising from the intervention (independent variable) were influenced by an external factor. Although experimental control is a strength of research, and in particular of randomized control trials, it can also create problems when one is implementing research evidence in client, athlete, or patient populations. Suppose a clinical scientist is interested in studying the effect of interval exercise compared to steady-state exercise on hypercholesterolemia in adults who are obese. A logical study design to address such a question would be a randomized controlled trial. Consider the following hypothetical study:
One hundred participants who were obese were selected at random and then randomly assigned to one of four groups: interval exercise, short-duration steady-state exercise, long-duration steady-state exercise, and control with no exercise. In order to eliminate potential confounding factors, the participants were free from comorbidities including hypertension, insulin resistance, diabetes, overt cardiovascular disease, and recent orthopedic injuries. Before the intervention, all groups completed a treadmill
On the surface, this appears to be a sound single-blind randomized controlled trial. It is in fact well-designed and controlled, but there are some potential problems when a practitioner considers implementation. Because the scientists were interested in studying training responses to an intervention in obesity alone, they eliminated subjects with diabetes, hypertension, and other common comorbidities. This was a good decision for internal validity, but not for external validity; practitioners rarely treat individuals who are obese without any of these companion conditions (Castro, Kolka, Kim, & Bergman, 2014; Despres et al., 2008). Thus, practitioners are left to wonder whether the evidence is truly applicable to their patients or clients.
A second possible problem with the evidence is the elimination of secondary interventions. Strengths of a scientific experiment may actually be perceived as weaknesses with regard to practical implementation. In practice, multiple interventions are often implemented in concert with one another. This hypothetical experiment evaluated the effectiveness of interval versus steady-state treadmill exercise alone. An exercise practitioner is unlikely to implement the interval training protocol in isolation; instead, the protocol may be combined with resistance training, a healthy diet, and other behavioral modifications. Implementation of such multifaceted protocols may enhance the effectiveness of either of the interventions. Conversely, the addition of such interventions may also reduce the effectiveness of the protocol. Obviously, it is not scientifically plausible that resistance exercise would cause an increase in cholesterol or biologically negate the effects of the interval training protocol. However, it is possible that implementation of the secondary intervention will lead to overtraining, injury, soreness, and perhaps poor adherence to the protocol due to each of these secondary results of the combined protocol. Again, this is not likely, but it is certainly something the practitioner must consider.
Another potential problem with the implementation of scientific evidence is the possibility that a client may not be able to tolerate the protocol. For example, the initial fitness level of the client may not be sufficient to enable him to tolerate its rigors. The practitioner is then left to decide whether a modified version of the research protocol will be effective in improving blood cholesterol profiles. It is also possible that the protocol used in the scientific experiment will result in undertraining in some individuals; that is, in contrast to the previous scenario, the intensity of the stimulus may be insufficient to induce a training response. The exercise practitioner must then decide how to effectively alter the training loads in order to induce a similar response in a client or patient with a greater initial fitness level. In situations like these, it is often helpful to consult the discussion section of the research paper. Often the authors discuss in great detail the programmatic elements that they believe are responsible for the particular adaptations they observed; for instance, they may note that their subjects completed 10 intervals (with positive outcomes) in contrast to a previous study in the same population that used four intervals with negative findings. Mechanistic evidence, from either the same study or another, would further elucidate the cause(s) for the positive adaptations from a higher volume of exercise.
In medicine, one of the often cited criticisms of the evidence-based philosophy is that it leads to a cookbook approach to practice (Sackett, Rosenberg, Gray, Haynes, & Richardson, 1996). Opponents assert that evidence-based practitioners read scientific papers and then implement the protocols directly from the papers. The example we have presented illustrates that there really is no "recipe" for prescription; that is not the purpose of science. Because people are different, protocols may need to be altered to fit individual patient or client needs. Science influences the "ingredients" of the prescription. This hypothetical experiment demonstrates that interval exercise might be more effective than steady-state treadmill exercise in improving blood cholesterol of patients who are obese. It also provides some basic parameters for intensity, volume, mode, and so on for the implementation of a protocol. Practitioners must then decide whether to implement the protocol. They must also decide how they should implement interval exercise in a manner that is best suited to their client's, patient's, or athlete's individual needs and experience level.
Learn more about Evidence-Based Practice in Exercise Science.
Case Study 2: Vibration and Muscle Strength and Power
Charity is a university strength and conditioning coach. Recently, a professor in the school’s exercise physiology program acquired several vibration plates for a planned research study. The vibration plates are housed in the athletic training facility and are available to the athletes.
Charity is a university strength and conditioning coach. Recently, a professor in the school's exercise physiology program acquired several vibration plates for a planned research study. The vibration plates are housed in the athletic training facility and are available to the athletes. Charity heard about training with vibration plates at a national conference she attended recently; the presenter described a variety of upper and lower body exercises that could be performed on the plate and anecdotally claimed that such training results in noticeable performance improvements in athletes participating in a variety of sports. As an evidence-based practitioner, Charity realizes that although the vibration plate presentation was compelling, she needs to search the literature to determine what kind of scientific support exists for using vibration plate training as a modality to improve physiological and athletic performance.
Background
Vibration is thought to enhance acute neuromuscular performance via the stimulation of Ia afferent nerves, which effects a myotatic reflex contraction (Abercromby et al., 2007). Acutely, vibration improves maximal force and power output during concentric contractions; this facilitative effect is greater in elite athletes than in amateurs (Issurin & Tenenbaum, 1999; Liebermann & Issurin, 1997). However, vibration is ineffective when applied acutely to promote recovery or improve subsequent running performance after a strenuous exercise bout in highly fit runners (Edge, Mundel, Weir, & Cochrane, 2009). In competitive athletes, routine vibration training can increase strength, jump performance, and flexibility (Fagnani, Giombini, Di Cesare, Pigozzi, & Di Salvo, 2006), as well as improve proprioception and balance after anterior cruciate ligament reconstruction in comparison to a conventional rehabilitation program (Moezy, Olyaei, Hadian, Razi, & Faghihzadeh, 2008).
Charity currently employs evidence-based strength and conditioning programs with her athletes; these programs consist largely of resistance exercise - both traditional strength and explosive Olympic weightlifting exercises. Thus, to make a valid comparison in her athletic population, Charity should compare the effectiveness of vibration training to that of traditional resistance exercise. Given the limitations of vibration training (cost, availability, spatial restrictions), only if vibration training (either alone or in combination with traditional training) proves superior to traditional training would it be prudent to incorporate it on a large scale. Thus the evidence-based question is as follows.
In trained athletes, does vibration training, either alone or as an adjunct to resistance exercise, elicit improvements in muscle strength or power that are superior to those realized with traditional resistance training?
Search Strategy
Typing "vibration" into PubMed yields a list of MeSH subheadings; we select "vibration training." This returns 1141 studies. Activating the Age filter (Adult: 19-44 years) and Language filter (English) reduces this number to 377. Next, we add "AND athletes" to the search string ("vibration training AND athletes"), which returns 20 articles. Scanning these abstracts reveals 3 papers directly related to the chronic effects of vibration training (Delecluse et al., 2005; Issurin, Liebermann, & Tenenbaum, 1994; Preatoni et al., 2012). Of the 17 articles not included, most are acute studies and several others examine the effects of vibration on postworkout recovery and postsurgical rehabilitation outcomes; another study was excluded because it is not clear what exercise the control group performed.
Discussion of Results
The three articles reviewed are summarized in table 15.2. Preatoni and colleagues (2012) evaluated the effects of vibration training alone and in combination with traditional resistance training in 18 national-level female athletes (12 soccer and 6 softball athletes, with equal proportions in all groups). Subjects were randomized to one of three groups: (1) whole-body vibration training group, (2) traditional strength training group, and (3) combined whole-body vibration and strength training group. All training was performed during the winter preparatory period and in combination with other sport-specific field training such as speed drills, aerobic work, and technical and tactical skill practice. The periodized resistance training program was performed 2 days per week for 8 weeks; for the first week it consisted of six sets × six repetitions of squats performed at body weight with vibration (vibration group), at 60% 1RM (strength training group), or 30% 1RM with vibration (combined whole-body vibration and strength training group). Every 2 weeks, the external load was increased 6% (for the strength training group) and 3% (for the combined whole-body vibration and strength training group); greater intensity for the vibration group was achieved by increasing vibration frequency 5 Hz every 2 weeks (frequency was also increased for the combined group). Outcome measures included isometric strength (leg press); dynamic force, velocity, and power (explosive leg press with loads of 100% to 200% body weight in 20% increments); and power and power endurance (vertical jump and continuous 15-s vertical jumps, respectively). Training increased isometric strength (main effect, P = 0.02) with no differences between groups. No changes were observed for any parameter of the explosive leg press test. Performance on both vertical jump tests increased with training (main effect, P < 0.002), but there were no differences between groups. Maximum jump height (vertical jump test) and mean jump height and power (continuous 15-s vertical jump test) were increased only in the strength-trained group. The investigators also evaluated the characteristics of the vibration device (i.e., frequency, amplitude, and acceleration) and found variations up to 20% from the selected value; this was particularly true at higher frequencies. On the basis of other published data (Blottner et al., 2006; Mulder et al., 2008, 2007; Rittweger et al., 2006), the authors conclude that vibration exercise can elicit similar or improved outcomes compared to traditional strength training only when similar external loads are used; that is, they attribute the lack of an effect in their study to the lower external loads lifted by the combined vibration + strength training group (Preatoni et al., 2012).
Delecluse and colleagues (2005) examined the additive effect of a whole-body vibration training program over 5 weeks in 20 sprinters. Male and female sprinters (mean 100 m times: female = 12.46 ± 0.59 s, male = 11.45 ± 0.42 s) were randomly assigned to either a vibration or a control group. Both groups maintained their conventional training program, which consisted of intervals (10-60 s), speed training (two or three sessions per week with efforts near race pace), speed drills (two sessions per week), plyometric drills (one session per week), and explosive resistance training (three sessions per week) at 75% to 95% 1RM (three to five sets × two to five repetitions). In addition to their typical training, the vibration group completed three sessions per week of unloaded static and dynamic leg exercise on a vibration platform. The exercises employed were high squat, deep squat, wide stance squat, single-leg squat, lunge, and heel raise. The vibration program was implemented progressively through increases in the duration of vibration time and concomitant decreases in the rest periods; vibration amplitude (displacement) and frequency were also increased over the 5-week program. The study was conducted during the precompetitive phase of training. Outcome measures included strength (isometric and isokinetic knee extensor-flexor), maximal knee extension velocity (at 1%, 20%, 40%, and 60% of maximum isometric force), vertical jump, starting parameters (start time, horizontal start velocity, and horizontal start acceleration), and maximum velocity in a 30 m sprint. There were no changes in either group after the 5-week training program, nor were there any interaction effects or differences between groups posttraining.
Issurin, Liebermann, and Tenenbaum (1994) examined the effects of vibration training in 28 young male athletes who regularly participated in a wide cross section of club or varsity sports such as judo, swimming, volleyball, tennis, soccer, track and field, and cycling. Subjects were randomized to one of three groups: (1) upper body strength training with vibration and lower body flexibility training, (2) upper body strength training and lower body flexibility training with vibration, and (3) a calisthenics - basketball game control. The training program, which was conducted three times per week for 3 weeks, consisted of a ~10-min warm-up, a single upper body strength exercise (seated bench pull: six sets × six repetitions at 80% to 100% 1RM performed to failure), and ~20 min of specific static and ballistic stretching of the upper leg musculature. The program was performed by both experimental groups; vibration was added to either the upper or lower body activity according to group assignment. Outcome measures included strength (bench pull 1RM) and flexibility (two-leg split distance and sit and reach distance). Collectively, 1RM strength and both flexibility measures increased with training (main effects); there were also differences between groups for each outcome (group × time interaction effect). Unfortunately, the authors did not provide statistical contrasts between groups (e.g., strength training vs. strength training with vibration) to elucidate the between-group differences; because of the influence of the control group (which changed very little for any measure) on both main and interaction effects, it is difficult to interpret the study findings.
Luo, NcNamara, and Moran (2005) published a review evaluating the effects of vibration training on muscle strength and power, examining the effects of both chronic and acute vibration training. In 2005, only three papers had been published on the chronic adaptations to vibration training; of these, only one study employed trained athletes as subjects and has already been discussed (Issurin et al., 1994).
Conclusion and Strength of Evidence
There has been an explosion of literature regarding whole-body vibration in recent years. Some studies have been well conducted; others are poorly designed or uncontrolled, leading to erroneous or equivocal conclusions. There is still minimal understanding of the appropriate frequency, amplitude, direction, and length and mode of exercise needed for positive adaptations to vibration training. Despite the widespread use of vibration in athletic and private training settings, the evidence at the current time does not suggest that it is a strong tool to improve strength in athletically trained populations, although there is evidence for use in other populations.
There is level B evidence to refute the use of vibration training as a stand-alone or adjunct training method to increase muscle strength or power in athletes, as it is not demonstrably superior to traditional resistance exercise.
Program Recommendations
Although evidence supports vibration as a tool to improve strength and power in untrained populations, the data do not support its use to improve performance in athletes versus traditional strength methods. There is some evidence to support its use as a tool to acutely potentiate a power response; thus if Charity chooses to implement vibration, based on the literature it should be used as a postexcitatory potentiation tool. In general, Charity should continue training her athletes using traditional strength and conditioning programs but continue to watch the literature for emergent studies and protocols.
Save
Learn more about Evidence-Based Practice in Exercise Science.
Evidence-Based Practice in Action
On September 9, 2007, the second week of the 2007-2008 National Football League (NFL) season, the Buffalo Bills were at home for a game with the Denver Broncos. On a routine kickoff, third-year tight end Kevin Everett sprinted down the field and approached the kick returner, Domenik Hixon (Carchidi, 2008).
On September 9, 2007, the second week of the 2007-2008 National Football League (NFL) season, the Buffalo Bills were at home for a game with the Denver Broncos. On a routine kickoff, third-year tight end Kevin Everett sprinted down the field and approached the kick returner, Domenik Hixon (Carchidi, 2008). Everett dropped his center of gravity and extended into Hixon for the tackle - a motor skill that he had presumably performed thousands of times previously. Everett led with the crown of his helmet, contacting the helmet of Hixon at a high velocity, inadvertently violating a common but too often disregarded fundamental of tackling. The consequences of the collision were devastating and nearly fatal for Everett.
Immediately upon impact, Everett fell to the ground and lay face down, motionless. The collision resulted in a fracture dislocation of his third and fourth cervical vertebrae, injuring the spinal cord and instantly paralyzing Everett (Cappuccino et al., 2010; Carchidi, 2008). The sports medicine staff reacted quickly to the injury, clearing the scene to ensure that Everett was not injured further. With an injury such as Everett's, the standard-of-care protocol provides that the helmet remain on, the player be placed on a board, the face mask removed, and the player carefully moved to a stretcher and then transported by ambulance directly to the hospital. The sports medicine staff appeared to perfectly execute the protocol, and Everett was carefully transported to Millard Fillmore Gates Hospital (Carchidi, 2008).
In the ambulance ride en route to the hospital, the neurosurgery team used an experimental therapy that they hoped would improve Everett's prognosis. Infusing a cold saline solution into Everett's veins, the medical team induced a mild hypothermic state (Cappuccino et al., 2010). The use of ice to treat an injury is not novel - ice is used acutely for virtually every orthopedic injury. The principle of inducing systemic hypothermia is similar. The cold saline solution acutely controls systemic inflammation, and the medical team apparently believed that the therapy would reduce inflammation surrounding the spinal cord injury, preventing further damage (Cappuccino et al., 2010; Mummaneni, 2010). After evaluation by the medical staff, the neurosurgeon performed an emergency surgery in an attempt to save Everett's life (Cappuccino et al., 2010). After the surgery, Everett was placed on a respirator; it was believed that if he lived, he was unlikely to ever walk again (Carchidi, 2008).
Two days after the injury, Everett was removed from the respirator; he was reported to have minimal voluntary movements in his lower extremities, suggesting a theoretical possibility that he could regain the ability to walk (Cappuccino et al., 2010). On the basis on previous cases, the medical team believed that Everett had a small chance of regaining full control of his extremities (Carchidi, 2008). In the weeks and months that followed, Everett made remarkable progress, recovering at a rate far greater than expected. He was transferred to a top rehabilitation center for neurologic injuries in Houston, Texas, that implemented a comprehensive rehabilitation program. On December 23, 2007, Kevin Everett walked onto the field of Ralph Wilson Stadium - a remarkable feat that a few short months earlier had seemed impossible.
Kevin Everett's recovery was remarkable and a testament to the professional competence and readiness of the integrated sports medicine team, who made numerous decisions improving the chances that he might walk. Everett's story is also a demonstration of personal determination and perseverance that has inspired hope. For patients suffering severe spinal cord injuries, the story validates that dramatic recovery is possible. Medical personnel are encouraged in that Everett's case shows that diligent medical and rehabilitative therapy facilitates recovery. However, there is one overriding question that surrounds Kevin Everett's case: Why did he recover and why so fast? There are a number of possible explanations:
- Everett's recovery was simply a statistical improbability - he was an outlier and his recovery a chance occurrence.
- It was the result of sheer human determination and will in an athlete who simply would not accept his prognosis and would give everything to ensure he had the best chance to walk.
- It was the result of the sports medicine team's careful execution of the standard-of-care practice to prevent further injury immediately post-accident.
- Everett's recovery was the result of the precise execution of the neurosurgery team.
- The recovery was a result of the rehabilitation protocol implemented by a leading neurorehabilitation center.
- The rapid recovery was the result of cryotherapy, an experimental method that dramatically improved his prognosis.
The case of Kevin Everett highlights an important concept, that knowledge is a dynamic phenomenon (Amonette et al., 2010). The team of doctors, physical therapists, athletic trainers, and exercise specialists involved in the acute and postacute treatment of Everett's injury made numerous decisions that positively or negatively affected his outcome. The athletic trainers and sports medicine staff identified a possible injury to the spine and ensured that the athlete was quickly transported to the hospital. A careful procedure was used to move him to avoid further injury. The physicians made a decision to use the hypothermic technique to reduce spinal swelling. The neurosurgeon decided to perform surgery, and at some point, a physician determined that it was safe to remove Everett from the ventilator. In the rehabilitative process, physical therapists along with the medical team decided which therapeutic interventions were best suited to the stage of injury and made daily decisions on when to increase, decrease, or hold parameters like the intensity, volume, and duration of the rehabilitation program.
How did the sports medicine team determine the appropriate treatment?
Learn more about Evidence-Based Practice in Exercise Science.
Steps to Reading Research Critically
Reading and interpreting research may be one of the most important tasks of an evidence-based practitioner. It is important to develop the skills necessary to identify the key findings and to disregard the superfluous information.
Reading and interpreting research may be one of the most important tasks of an evidence-based practitioner. It is important to develop the skills necessary to identify the key findings and to disregard the superfluous information. Although critical appraisal is a topic left to a later chapter, next we present some practical guidelines for reading research evidence.
1-2. Read the Title and Abstract
The title of a research article can provide an important clue to the most important findings in the manuscript. But you should never read only the title and abstract. Some journal titles explicitly state the major finding of the paper. In a 1989 publication in Archives of Neurology, an article titled "Focused Stroke Rehabilitation Programs Improve Outcome" appears on pages 700-701 (Reding & McDowell, 1989) (figure 5.7). From the title alone, without reading the paper or the abstract, the reader learns that the investigators determined that a stroke rehabilitation program was effective in improving clinical outcomes. However, the very next article in the same volume of Archives of Neurology is titled "Focused Stroke Rehabilitation Programs Do Not Improve Outcome" (Dobkin, 1989) (figure 5.7). Which article is correct?
Two studies with directly contradictory titles that appeared consecutively in 1989 in Archives of Neurology.
Reprinted from PubMed.gov.
When the evidence-based practitioner relies on the title or abstract alone, he can make significant mistakes in the interpretation of research evidence. Also, examples such as the one just presented clearly show that research can be contradictory. The practitioner should read the title and abstract to determine whether the paper is relevant to the evidence-based question. If it is, he should proceed to a more careful reading and analysis to determine if the study methods and results support the findings stated in the abstract and title.
3. Read the Purpose, Construct, Theory, or Hypothesis Statement
After reading the title and abstract to determine the relevance of the study to the evidence-based question, the practitioner can skip to the final statement in the introduction that presents the study purpose, construct, theory, or hypothesis statement. This should provide the information needed to determine how the study should be designed to best answer the research question.
4. Read the Methods and Look for Flaws
The methods section is the most important part of a paper to read carefully and critically. It is from the methods section that an evidence-based practitioner can determine many of the potential biases and confounding factors associated with the study. This is also the section of the paper that determines the level or strength of evidence (chapter 8) provided by the research. As authors critically appraise their own research, they should carefully consider the study design, testing protocols, devices used, training and intervention protocols, statistical analyses, and study group allocations. If the authors are unclear in their presentation of any component of the methods, this should be a "red flag" to the reader and could potentially be a fatal flaw in the design.
Additional steps found inside Evidence-Based Practice in Exercise Science.
Translating Research Into Practice
As discussed earlier in this book, research design is a critical element to answering questions relevant to mechanistic, practical, and clinical science. One of the key aspects of research design is control of all potential confounding factors to eliminate the possibility that the outcomes arising from the intervention (independent variable) were influenced by an external factor.
As discussed earlier in this book, research design is a critical element to answering questions relevant to mechanistic, practical, and clinical science. One of the key aspects of research design is control of all potential confounding factors to eliminate the possibility that the outcomes arising from the intervention (independent variable) were influenced by an external factor. Although experimental control is a strength of research, and in particular of randomized control trials, it can also create problems when one is implementing research evidence in client, athlete, or patient populations. Suppose a clinical scientist is interested in studying the effect of interval exercise compared to steady-state exercise on hypercholesterolemia in adults who are obese. A logical study design to address such a question would be a randomized controlled trial. Consider the following hypothetical study:
One hundred participants who were obese were selected at random and then randomly assigned to one of four groups: interval exercise, short-duration steady-state exercise, long-duration steady-state exercise, and control with no exercise. In order to eliminate potential confounding factors, the participants were free from comorbidities including hypertension, insulin resistance, diabetes, overt cardiovascular disease, and recent orthopedic injuries. Before the intervention, all groups completed a treadmill
On the surface, this appears to be a sound single-blind randomized controlled trial. It is in fact well-designed and controlled, but there are some potential problems when a practitioner considers implementation. Because the scientists were interested in studying training responses to an intervention in obesity alone, they eliminated subjects with diabetes, hypertension, and other common comorbidities. This was a good decision for internal validity, but not for external validity; practitioners rarely treat individuals who are obese without any of these companion conditions (Castro, Kolka, Kim, & Bergman, 2014; Despres et al., 2008). Thus, practitioners are left to wonder whether the evidence is truly applicable to their patients or clients.
A second possible problem with the evidence is the elimination of secondary interventions. Strengths of a scientific experiment may actually be perceived as weaknesses with regard to practical implementation. In practice, multiple interventions are often implemented in concert with one another. This hypothetical experiment evaluated the effectiveness of interval versus steady-state treadmill exercise alone. An exercise practitioner is unlikely to implement the interval training protocol in isolation; instead, the protocol may be combined with resistance training, a healthy diet, and other behavioral modifications. Implementation of such multifaceted protocols may enhance the effectiveness of either of the interventions. Conversely, the addition of such interventions may also reduce the effectiveness of the protocol. Obviously, it is not scientifically plausible that resistance exercise would cause an increase in cholesterol or biologically negate the effects of the interval training protocol. However, it is possible that implementation of the secondary intervention will lead to overtraining, injury, soreness, and perhaps poor adherence to the protocol due to each of these secondary results of the combined protocol. Again, this is not likely, but it is certainly something the practitioner must consider.
Another potential problem with the implementation of scientific evidence is the possibility that a client may not be able to tolerate the protocol. For example, the initial fitness level of the client may not be sufficient to enable him to tolerate its rigors. The practitioner is then left to decide whether a modified version of the research protocol will be effective in improving blood cholesterol profiles. It is also possible that the protocol used in the scientific experiment will result in undertraining in some individuals; that is, in contrast to the previous scenario, the intensity of the stimulus may be insufficient to induce a training response. The exercise practitioner must then decide how to effectively alter the training loads in order to induce a similar response in a client or patient with a greater initial fitness level. In situations like these, it is often helpful to consult the discussion section of the research paper. Often the authors discuss in great detail the programmatic elements that they believe are responsible for the particular adaptations they observed; for instance, they may note that their subjects completed 10 intervals (with positive outcomes) in contrast to a previous study in the same population that used four intervals with negative findings. Mechanistic evidence, from either the same study or another, would further elucidate the cause(s) for the positive adaptations from a higher volume of exercise.
In medicine, one of the often cited criticisms of the evidence-based philosophy is that it leads to a cookbook approach to practice (Sackett, Rosenberg, Gray, Haynes, & Richardson, 1996). Opponents assert that evidence-based practitioners read scientific papers and then implement the protocols directly from the papers. The example we have presented illustrates that there really is no "recipe" for prescription; that is not the purpose of science. Because people are different, protocols may need to be altered to fit individual patient or client needs. Science influences the "ingredients" of the prescription. This hypothetical experiment demonstrates that interval exercise might be more effective than steady-state treadmill exercise in improving blood cholesterol of patients who are obese. It also provides some basic parameters for intensity, volume, mode, and so on for the implementation of a protocol. Practitioners must then decide whether to implement the protocol. They must also decide how they should implement interval exercise in a manner that is best suited to their client's, patient's, or athlete's individual needs and experience level.
Learn more about Evidence-Based Practice in Exercise Science.
Case Study 2: Vibration and Muscle Strength and Power
Charity is a university strength and conditioning coach. Recently, a professor in the school’s exercise physiology program acquired several vibration plates for a planned research study. The vibration plates are housed in the athletic training facility and are available to the athletes.
Charity is a university strength and conditioning coach. Recently, a professor in the school's exercise physiology program acquired several vibration plates for a planned research study. The vibration plates are housed in the athletic training facility and are available to the athletes. Charity heard about training with vibration plates at a national conference she attended recently; the presenter described a variety of upper and lower body exercises that could be performed on the plate and anecdotally claimed that such training results in noticeable performance improvements in athletes participating in a variety of sports. As an evidence-based practitioner, Charity realizes that although the vibration plate presentation was compelling, she needs to search the literature to determine what kind of scientific support exists for using vibration plate training as a modality to improve physiological and athletic performance.
Background
Vibration is thought to enhance acute neuromuscular performance via the stimulation of Ia afferent nerves, which effects a myotatic reflex contraction (Abercromby et al., 2007). Acutely, vibration improves maximal force and power output during concentric contractions; this facilitative effect is greater in elite athletes than in amateurs (Issurin & Tenenbaum, 1999; Liebermann & Issurin, 1997). However, vibration is ineffective when applied acutely to promote recovery or improve subsequent running performance after a strenuous exercise bout in highly fit runners (Edge, Mundel, Weir, & Cochrane, 2009). In competitive athletes, routine vibration training can increase strength, jump performance, and flexibility (Fagnani, Giombini, Di Cesare, Pigozzi, & Di Salvo, 2006), as well as improve proprioception and balance after anterior cruciate ligament reconstruction in comparison to a conventional rehabilitation program (Moezy, Olyaei, Hadian, Razi, & Faghihzadeh, 2008).
Charity currently employs evidence-based strength and conditioning programs with her athletes; these programs consist largely of resistance exercise - both traditional strength and explosive Olympic weightlifting exercises. Thus, to make a valid comparison in her athletic population, Charity should compare the effectiveness of vibration training to that of traditional resistance exercise. Given the limitations of vibration training (cost, availability, spatial restrictions), only if vibration training (either alone or in combination with traditional training) proves superior to traditional training would it be prudent to incorporate it on a large scale. Thus the evidence-based question is as follows.
In trained athletes, does vibration training, either alone or as an adjunct to resistance exercise, elicit improvements in muscle strength or power that are superior to those realized with traditional resistance training?
Search Strategy
Typing "vibration" into PubMed yields a list of MeSH subheadings; we select "vibration training." This returns 1141 studies. Activating the Age filter (Adult: 19-44 years) and Language filter (English) reduces this number to 377. Next, we add "AND athletes" to the search string ("vibration training AND athletes"), which returns 20 articles. Scanning these abstracts reveals 3 papers directly related to the chronic effects of vibration training (Delecluse et al., 2005; Issurin, Liebermann, & Tenenbaum, 1994; Preatoni et al., 2012). Of the 17 articles not included, most are acute studies and several others examine the effects of vibration on postworkout recovery and postsurgical rehabilitation outcomes; another study was excluded because it is not clear what exercise the control group performed.
Discussion of Results
The three articles reviewed are summarized in table 15.2. Preatoni and colleagues (2012) evaluated the effects of vibration training alone and in combination with traditional resistance training in 18 national-level female athletes (12 soccer and 6 softball athletes, with equal proportions in all groups). Subjects were randomized to one of three groups: (1) whole-body vibration training group, (2) traditional strength training group, and (3) combined whole-body vibration and strength training group. All training was performed during the winter preparatory period and in combination with other sport-specific field training such as speed drills, aerobic work, and technical and tactical skill practice. The periodized resistance training program was performed 2 days per week for 8 weeks; for the first week it consisted of six sets × six repetitions of squats performed at body weight with vibration (vibration group), at 60% 1RM (strength training group), or 30% 1RM with vibration (combined whole-body vibration and strength training group). Every 2 weeks, the external load was increased 6% (for the strength training group) and 3% (for the combined whole-body vibration and strength training group); greater intensity for the vibration group was achieved by increasing vibration frequency 5 Hz every 2 weeks (frequency was also increased for the combined group). Outcome measures included isometric strength (leg press); dynamic force, velocity, and power (explosive leg press with loads of 100% to 200% body weight in 20% increments); and power and power endurance (vertical jump and continuous 15-s vertical jumps, respectively). Training increased isometric strength (main effect, P = 0.02) with no differences between groups. No changes were observed for any parameter of the explosive leg press test. Performance on both vertical jump tests increased with training (main effect, P < 0.002), but there were no differences between groups. Maximum jump height (vertical jump test) and mean jump height and power (continuous 15-s vertical jump test) were increased only in the strength-trained group. The investigators also evaluated the characteristics of the vibration device (i.e., frequency, amplitude, and acceleration) and found variations up to 20% from the selected value; this was particularly true at higher frequencies. On the basis of other published data (Blottner et al., 2006; Mulder et al., 2008, 2007; Rittweger et al., 2006), the authors conclude that vibration exercise can elicit similar or improved outcomes compared to traditional strength training only when similar external loads are used; that is, they attribute the lack of an effect in their study to the lower external loads lifted by the combined vibration + strength training group (Preatoni et al., 2012).
Delecluse and colleagues (2005) examined the additive effect of a whole-body vibration training program over 5 weeks in 20 sprinters. Male and female sprinters (mean 100 m times: female = 12.46 ± 0.59 s, male = 11.45 ± 0.42 s) were randomly assigned to either a vibration or a control group. Both groups maintained their conventional training program, which consisted of intervals (10-60 s), speed training (two or three sessions per week with efforts near race pace), speed drills (two sessions per week), plyometric drills (one session per week), and explosive resistance training (three sessions per week) at 75% to 95% 1RM (three to five sets × two to five repetitions). In addition to their typical training, the vibration group completed three sessions per week of unloaded static and dynamic leg exercise on a vibration platform. The exercises employed were high squat, deep squat, wide stance squat, single-leg squat, lunge, and heel raise. The vibration program was implemented progressively through increases in the duration of vibration time and concomitant decreases in the rest periods; vibration amplitude (displacement) and frequency were also increased over the 5-week program. The study was conducted during the precompetitive phase of training. Outcome measures included strength (isometric and isokinetic knee extensor-flexor), maximal knee extension velocity (at 1%, 20%, 40%, and 60% of maximum isometric force), vertical jump, starting parameters (start time, horizontal start velocity, and horizontal start acceleration), and maximum velocity in a 30 m sprint. There were no changes in either group after the 5-week training program, nor were there any interaction effects or differences between groups posttraining.
Issurin, Liebermann, and Tenenbaum (1994) examined the effects of vibration training in 28 young male athletes who regularly participated in a wide cross section of club or varsity sports such as judo, swimming, volleyball, tennis, soccer, track and field, and cycling. Subjects were randomized to one of three groups: (1) upper body strength training with vibration and lower body flexibility training, (2) upper body strength training and lower body flexibility training with vibration, and (3) a calisthenics - basketball game control. The training program, which was conducted three times per week for 3 weeks, consisted of a ~10-min warm-up, a single upper body strength exercise (seated bench pull: six sets × six repetitions at 80% to 100% 1RM performed to failure), and ~20 min of specific static and ballistic stretching of the upper leg musculature. The program was performed by both experimental groups; vibration was added to either the upper or lower body activity according to group assignment. Outcome measures included strength (bench pull 1RM) and flexibility (two-leg split distance and sit and reach distance). Collectively, 1RM strength and both flexibility measures increased with training (main effects); there were also differences between groups for each outcome (group × time interaction effect). Unfortunately, the authors did not provide statistical contrasts between groups (e.g., strength training vs. strength training with vibration) to elucidate the between-group differences; because of the influence of the control group (which changed very little for any measure) on both main and interaction effects, it is difficult to interpret the study findings.
Luo, NcNamara, and Moran (2005) published a review evaluating the effects of vibration training on muscle strength and power, examining the effects of both chronic and acute vibration training. In 2005, only three papers had been published on the chronic adaptations to vibration training; of these, only one study employed trained athletes as subjects and has already been discussed (Issurin et al., 1994).
Conclusion and Strength of Evidence
There has been an explosion of literature regarding whole-body vibration in recent years. Some studies have been well conducted; others are poorly designed or uncontrolled, leading to erroneous or equivocal conclusions. There is still minimal understanding of the appropriate frequency, amplitude, direction, and length and mode of exercise needed for positive adaptations to vibration training. Despite the widespread use of vibration in athletic and private training settings, the evidence at the current time does not suggest that it is a strong tool to improve strength in athletically trained populations, although there is evidence for use in other populations.
There is level B evidence to refute the use of vibration training as a stand-alone or adjunct training method to increase muscle strength or power in athletes, as it is not demonstrably superior to traditional resistance exercise.
Program Recommendations
Although evidence supports vibration as a tool to improve strength and power in untrained populations, the data do not support its use to improve performance in athletes versus traditional strength methods. There is some evidence to support its use as a tool to acutely potentiate a power response; thus if Charity chooses to implement vibration, based on the literature it should be used as a postexcitatory potentiation tool. In general, Charity should continue training her athletes using traditional strength and conditioning programs but continue to watch the literature for emergent studies and protocols.
Save
Learn more about Evidence-Based Practice in Exercise Science.
Evidence-Based Practice in Action
On September 9, 2007, the second week of the 2007-2008 National Football League (NFL) season, the Buffalo Bills were at home for a game with the Denver Broncos. On a routine kickoff, third-year tight end Kevin Everett sprinted down the field and approached the kick returner, Domenik Hixon (Carchidi, 2008).
On September 9, 2007, the second week of the 2007-2008 National Football League (NFL) season, the Buffalo Bills were at home for a game with the Denver Broncos. On a routine kickoff, third-year tight end Kevin Everett sprinted down the field and approached the kick returner, Domenik Hixon (Carchidi, 2008). Everett dropped his center of gravity and extended into Hixon for the tackle - a motor skill that he had presumably performed thousands of times previously. Everett led with the crown of his helmet, contacting the helmet of Hixon at a high velocity, inadvertently violating a common but too often disregarded fundamental of tackling. The consequences of the collision were devastating and nearly fatal for Everett.
Immediately upon impact, Everett fell to the ground and lay face down, motionless. The collision resulted in a fracture dislocation of his third and fourth cervical vertebrae, injuring the spinal cord and instantly paralyzing Everett (Cappuccino et al., 2010; Carchidi, 2008). The sports medicine staff reacted quickly to the injury, clearing the scene to ensure that Everett was not injured further. With an injury such as Everett's, the standard-of-care protocol provides that the helmet remain on, the player be placed on a board, the face mask removed, and the player carefully moved to a stretcher and then transported by ambulance directly to the hospital. The sports medicine staff appeared to perfectly execute the protocol, and Everett was carefully transported to Millard Fillmore Gates Hospital (Carchidi, 2008).
In the ambulance ride en route to the hospital, the neurosurgery team used an experimental therapy that they hoped would improve Everett's prognosis. Infusing a cold saline solution into Everett's veins, the medical team induced a mild hypothermic state (Cappuccino et al., 2010). The use of ice to treat an injury is not novel - ice is used acutely for virtually every orthopedic injury. The principle of inducing systemic hypothermia is similar. The cold saline solution acutely controls systemic inflammation, and the medical team apparently believed that the therapy would reduce inflammation surrounding the spinal cord injury, preventing further damage (Cappuccino et al., 2010; Mummaneni, 2010). After evaluation by the medical staff, the neurosurgeon performed an emergency surgery in an attempt to save Everett's life (Cappuccino et al., 2010). After the surgery, Everett was placed on a respirator; it was believed that if he lived, he was unlikely to ever walk again (Carchidi, 2008).
Two days after the injury, Everett was removed from the respirator; he was reported to have minimal voluntary movements in his lower extremities, suggesting a theoretical possibility that he could regain the ability to walk (Cappuccino et al., 2010). On the basis on previous cases, the medical team believed that Everett had a small chance of regaining full control of his extremities (Carchidi, 2008). In the weeks and months that followed, Everett made remarkable progress, recovering at a rate far greater than expected. He was transferred to a top rehabilitation center for neurologic injuries in Houston, Texas, that implemented a comprehensive rehabilitation program. On December 23, 2007, Kevin Everett walked onto the field of Ralph Wilson Stadium - a remarkable feat that a few short months earlier had seemed impossible.
Kevin Everett's recovery was remarkable and a testament to the professional competence and readiness of the integrated sports medicine team, who made numerous decisions improving the chances that he might walk. Everett's story is also a demonstration of personal determination and perseverance that has inspired hope. For patients suffering severe spinal cord injuries, the story validates that dramatic recovery is possible. Medical personnel are encouraged in that Everett's case shows that diligent medical and rehabilitative therapy facilitates recovery. However, there is one overriding question that surrounds Kevin Everett's case: Why did he recover and why so fast? There are a number of possible explanations:
- Everett's recovery was simply a statistical improbability - he was an outlier and his recovery a chance occurrence.
- It was the result of sheer human determination and will in an athlete who simply would not accept his prognosis and would give everything to ensure he had the best chance to walk.
- It was the result of the sports medicine team's careful execution of the standard-of-care practice to prevent further injury immediately post-accident.
- Everett's recovery was the result of the precise execution of the neurosurgery team.
- The recovery was a result of the rehabilitation protocol implemented by a leading neurorehabilitation center.
- The rapid recovery was the result of cryotherapy, an experimental method that dramatically improved his prognosis.
The case of Kevin Everett highlights an important concept, that knowledge is a dynamic phenomenon (Amonette et al., 2010). The team of doctors, physical therapists, athletic trainers, and exercise specialists involved in the acute and postacute treatment of Everett's injury made numerous decisions that positively or negatively affected his outcome. The athletic trainers and sports medicine staff identified a possible injury to the spine and ensured that the athlete was quickly transported to the hospital. A careful procedure was used to move him to avoid further injury. The physicians made a decision to use the hypothermic technique to reduce spinal swelling. The neurosurgeon decided to perform surgery, and at some point, a physician determined that it was safe to remove Everett from the ventilator. In the rehabilitative process, physical therapists along with the medical team decided which therapeutic interventions were best suited to the stage of injury and made daily decisions on when to increase, decrease, or hold parameters like the intensity, volume, and duration of the rehabilitation program.
How did the sports medicine team determine the appropriate treatment?
Learn more about Evidence-Based Practice in Exercise Science.
Steps to Reading Research Critically
Reading and interpreting research may be one of the most important tasks of an evidence-based practitioner. It is important to develop the skills necessary to identify the key findings and to disregard the superfluous information.
Reading and interpreting research may be one of the most important tasks of an evidence-based practitioner. It is important to develop the skills necessary to identify the key findings and to disregard the superfluous information. Although critical appraisal is a topic left to a later chapter, next we present some practical guidelines for reading research evidence.
1-2. Read the Title and Abstract
The title of a research article can provide an important clue to the most important findings in the manuscript. But you should never read only the title and abstract. Some journal titles explicitly state the major finding of the paper. In a 1989 publication in Archives of Neurology, an article titled "Focused Stroke Rehabilitation Programs Improve Outcome" appears on pages 700-701 (Reding & McDowell, 1989) (figure 5.7). From the title alone, without reading the paper or the abstract, the reader learns that the investigators determined that a stroke rehabilitation program was effective in improving clinical outcomes. However, the very next article in the same volume of Archives of Neurology is titled "Focused Stroke Rehabilitation Programs Do Not Improve Outcome" (Dobkin, 1989) (figure 5.7). Which article is correct?
Two studies with directly contradictory titles that appeared consecutively in 1989 in Archives of Neurology.
Reprinted from PubMed.gov.
When the evidence-based practitioner relies on the title or abstract alone, he can make significant mistakes in the interpretation of research evidence. Also, examples such as the one just presented clearly show that research can be contradictory. The practitioner should read the title and abstract to determine whether the paper is relevant to the evidence-based question. If it is, he should proceed to a more careful reading and analysis to determine if the study methods and results support the findings stated in the abstract and title.
3. Read the Purpose, Construct, Theory, or Hypothesis Statement
After reading the title and abstract to determine the relevance of the study to the evidence-based question, the practitioner can skip to the final statement in the introduction that presents the study purpose, construct, theory, or hypothesis statement. This should provide the information needed to determine how the study should be designed to best answer the research question.
4. Read the Methods and Look for Flaws
The methods section is the most important part of a paper to read carefully and critically. It is from the methods section that an evidence-based practitioner can determine many of the potential biases and confounding factors associated with the study. This is also the section of the paper that determines the level or strength of evidence (chapter 8) provided by the research. As authors critically appraise their own research, they should carefully consider the study design, testing protocols, devices used, training and intervention protocols, statistical analyses, and study group allocations. If the authors are unclear in their presentation of any component of the methods, this should be a "red flag" to the reader and could potentially be a fatal flaw in the design.
Additional steps found inside Evidence-Based Practice in Exercise Science.
Related Books